



 , Alessandro Lazzarin 1,2, Matteo Santoni 4, Francesca Trentini 1,2, Ugo De Giorgi 5, Nicole Brighi 5, Chiara Tommasi 1,2,3, Silvia Puglisi 6, Orazio Caffo 7, Stefania Kinspergher 7, Alessia Mennitto 8, Carlo Cattrini 8, Elena Verzoni 9, Alessandro Rametta 9, Marco Stellato 9, Andrea Malgeri 10, Giandomenico Roviello 11, Enrico Maria Silini 2,12, Pasquale Rescigno 13, Sara Elena Rebuzzi 14,15, Giuseppe Fornarini 6, Federico Quaini 2, Giulia Claire Giudice 1,2, Giuseppe Luigi Banna 16,†, Sebastiano Buti 1,2,3,*,†
, Alessandro Lazzarin 1,2, Matteo Santoni 4, Francesca Trentini 1,2, Ugo De Giorgi 5, Nicole Brighi 5, Chiara Tommasi 1,2,3, Silvia Puglisi 6, Orazio Caffo 7, Stefania Kinspergher 7, Alessia Mennitto 8, Carlo Cattrini 8, Elena Verzoni 9, Alessandro Rametta 9, Marco Stellato 9, Andrea Malgeri 10, Giandomenico Roviello 11, Enrico Maria Silini 2,12, Pasquale Rescigno 13, Sara Elena Rebuzzi 14,15, Giuseppe Fornarini 6, Federico Quaini 2, Giulia Claire Giudice 1,2, Giuseppe Luigi Banna 16,†, Sebastiano Buti 1,2,3,*,†
1 Medical Oncology Unit, University Hospital of Parma, 43126 Parma, Italy
2 Department of Medicine and Surgery, University of Parma, 43126 Parma, Italy
3 Gruppo Oncologico Italiano di Ricerca Clinica (GOIRC), 43126 Parma, Italy
4 Oncology Unit, Macerata Hospital, 62100 Macerata, Italy
5 Department of Medical Oncology, IRCCS Istituto Romagnolo per lo Studio dei Tumori (IRST) “Dino Amadori'', 47014 Meldola, Italy
6 Medical Oncology Unit 1, IRCCS Ospedale Policlinico San Martino, 16122 Genova, Italy
7 Department of Medical Oncology, Santa Chiara Hospital, 38100 Trento, Italy
8 Division of Oncology, University Hospital “Maggiore della Carità", 28100 Novara, Italy
9 Medical Oncology Department, Fondazione IRCCS Istituto Nazionale dei Tumori, 20133 Milan, Italy
10 Department of Medical Oncology, Fondazione Policlinico Campus Bio-Medico, 00161 Roma, Italy
11 Department of Health Sciences, University of Florence, 50139 Florence, Italy
12 Pathology Unit, University Hospital of Parma, 43126 Parma, Italy
13 Candiolo Cancer Institute, FPO-IRCCS, 10123 Turin, Italy
14 Medical Oncology Unit, Ospedale San Paolo, 17012 Savona, Italy
15 Department of Internal Medicine and Medical Specialties (Di.M.I.), University of Genova, 16166 Genova, Italy
16 Department of Oncology, Portsmouth Hospitals University NHS Trust, PO6 3LY Cosham, Portsmouth, UK
†These authors contributed equally.
Abstract
Background: The advent of immune checkpoint inhibitors (ICIs)
has revolutionized the metastatic renal cell carcinoma (mRCC) therapeutic
landscape. Nevertheless, tyrosine-kinase inhibitors (TKIs) targeting the vascular
endothelial growth factor (VEGF) axis still play a key role. The aim of the
present study was to explore the prognostic performance of an integrated blood
score, based on hemoglobin (Hb) concentration, mean corpuscular volume (MCV), and
red cell distribution width (RDW), in mRCC patients treated with anti-VEGF TKIs.
The primary endpoint was to correlate Hb, MCV, and RDW with progression-free
survival (PFS) and overall survival (OS). Materials and Methods: Our
multicenter retrospective observational study involved mRCC patients treated with
pazopanib or cabozantinib from January 2012 to December 2020 in nine Italian
centers. Clinical records and laboratory data, including Hb levels, MCV, and RDW,
were collected at baseline. Descriptive statistics and univariate and
multivariate analyses were performed. Results: We enrolled 301 mRCC
patients of which 179 (59%) underwent pazopanib, and 122 (41%) cabozantinib. We
considered baseline Hb
Graphical Abstract
Keywords
- metastatic renal cell carcinoma (mRCC)
- macrocytosis
- anisocytosis
- anemia
- HIF
- tyrosine-kinase inhibitors
- prognostic score
- MCV
- Hb
- RDW
The treatment landscape for metastatic clear cell renal cell carcinoma (mccRCC)
is constantly evolving. Despite the recent advent of immunotherapy-based
regimens, tyrosine kinase inhibitors (TKIs) still play a key role in mccRCC,
except for sarcomatoid-differentiated subtypes [1, 2], which are known to benefit
more from immune-checkpoint inhibitors (ICIs). As a matter of fact, the
combination of ICIs with TKIs represents a valid option for all intermediate and
poor-risk patients according to the International Metastatic Renal Cell Carcinoma
Database Consortium (IMDC) score, especially when a timely disease control is
needed [3]. Various combinations have gained U.S. Food and Drug Administration (FDA) and European Medicines Agency (EMA) approval for clinical
use in this setting: pembrolizumab plus axitinib (KEYNOTE 426 trial),
pembrolizumab plus lenvatinib (CLEAR trial), avelumab plus axitinib (JAVELIN
Renal 101 trial), and nivolumab plus cabozantinib (CheckMate 9ER trial) [4, 5, 6, 7].
Moreover, TKIs may represent a monotherapy option in favorable-risk patients
presenting low tumor burden and indolent disease progression patterns, or in
selected cases who cannot receive ICIs [8]. Sunitinib, an oral TKI, which
inhibits different growth factors, such as vascular endothelial growth factor
receptor (VEGFR), platelet-derived growth factor receptor (PDGFR), and c-KIT, was
the first TKI to show a significant benefit in progression-free survival (PFS)
and overall survival (OS), compared to the current standard of care treatment
with interferon-
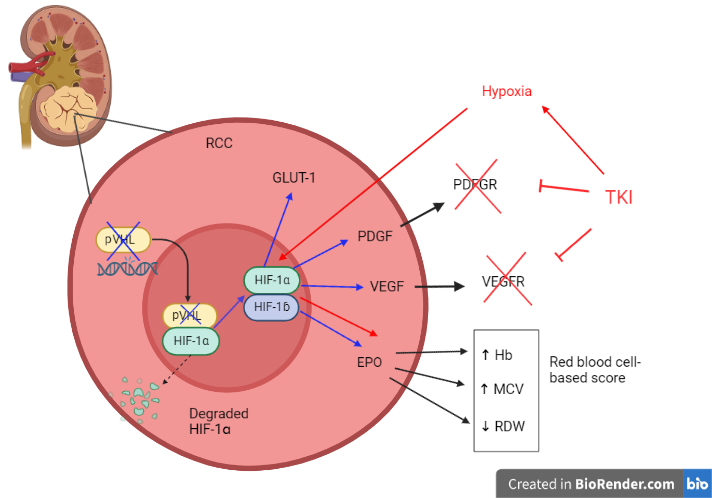
This class of drugs mainly works by blocking the hypoxia-inducible
factor-1-alpha (HIF-1
The loss of the VHL gene is an early tumorigenesis event that occurs in
approximately 90% of ccRCCs, which leads tumor cells to a state of
pseudohypoxia, and consequently, upregulates HIF-1
In addition to the VEGF axis, one of the main target genes of the HIF-1 complex is erythropoietin (EPO). This hormone, mostly synthesized in the renal cortex by peritubular fibroblasts, is responsible for keeping the blood hemoglobin (Hb) concentration within a normal range by promoting survival, proliferation, and differentiation of erythrocytic progenitors [17].
Moreover, according to both Memorial Sloan Kettering Cancer Center (MSKCC) and IMDC prognostic scores, anemia is negatively associated with mRCC survival [18, 19]. Interestingly, it is ranked amongst the adverse events related to anti-VEGF TKIs and it seems to be related to off-target effects, such as the inhibition of FLT-3 and c-KIT, especially during treatment with sunitinib [20]. Nonetheless, increases in Hb concentration and red blood cell counts in the blood have also been reported during treatment with these agents [21, 22, 23].
Interestingly, the elevation of the mean corpuscular volume (MCV), which reflects macrocytosis, is another phenomenon described during treatment with anti-VEGF TKIs [24, 25] and correlates with a survival benefit in mRCC patients treated with sunitinib [26, 27, 28].
Furthermore, among red blood cell-centered parameters, red cell distribution width (RDW)—an indirect measure of anisocytosis—has been proven to be clinically meaningful, being directly associated with the grading and staging of the disease in localized RCCs, in addition to cancer-specific mortality in mRCC patients who underwent partial or total nephrectomy [29, 30]. Of note is a study by Aktepe et al. [31], which revealed that a higher RDW level correlated with a shorter PFS and OS in mRCC patients treated with either sunitinib or pazopanib.
Our preliminary data revealed that a relevant proportion of patients with mRCC
treated with pazopanib or cabozantinib had baseline macrocytosis or anisocytosis.
Moreover, we demonstrated a significant increase in Hb, MCV, and RDW values
following TKI treatment. Baseline macrocytosis resulted in a positive correlation
with PFS in patients treated with pazopanib, while anisocytosis emerged as a
negative prognostic factor for all patients treated with pazopanib or
cabozantinib. The evidence provided by this study suggests that Hb, MCV, and RDW
may indirectly reflect the activation of the HIF-1
Thus, the aim of the present study was to delineate a new integrated prognostic
score in mRCCs treated with anti-VEGF TKIs, based on easily exploitable blood
parameters, such as Hb concentration, MCV (macrocytosis), and RDW (anisocytosis),
which may reflect an upregulation of the HIF-1
Our multicenter observational retrospective study was conducted on patients with mRCC who were undergoing TKI treatment with pazopanib or cabozantinib between January 2012 and December 2020 in nine Italian centers. The primary endpoint of the study was to assess the impact of our new integrated prognostic score, based on Hb concentration, MCV, and RDW, on PFS and OS.
Our study cohort involved patients with unresectable or metastatic RCCs, histologically confirmed, who had received pazopanib or cabozantinib at any time in their treatment.
Clinicopathological records, including Eastern Cooperative Oncology Group Performance Status (ECOG PS), prognostic score using the International mRCC Database Consortium (IMDC) criteria, metastatic involvement, histopathological characteristics, and hematological/biochemical parameters (MCV, RDW, and Hb levels), were collected at baseline, before starting TKI treatments. Exclusion criteria consisted of systemic treatment other than cabozantinib or pazopanib and an absence of medical records.
The study was conducted following the approval by the ethics committee of the coordinating Center (protocol number 208/2021/OSS/AOUPR MA.RE.CA.P., date of approval: September 1, 2021) and the obtainment of patient informed consent.
Descriptive statistics were employed to report on patient characteristics.
Receiver operating characteristics curves (ROC)-based cut-offs were used to
select the optimal values of MCV (
The PFS was intended as the time from the beginning of the TKI therapy to the disease progression or death, whichever occurred first. The OS was calculated from the start of treatment to death for any cause. Patients without progression or death at the last follow-up were considered censored. Median follow-up was calculated according to the so-termed “reverse Kaplan–Meier” (Kaplan–Meier estimate of potential follow-up) technique. PFS and OS were estimated using the Kaplan–Meier method, while the log-rank test (Mantel–Cox) was applied to evaluate statistical differences in PFS and OS between groups. Then, PFS and OS data were analyzed through Cox univariate and multivariate proportional hazards regression models and the results were expressed as hazard ratios (HR), 95% confidence intervals (95% CI), and p values. The multivariate models were fitted to include covariates which resulted significant in the univariate analysis. To minimize the risk of multiplicity, Holm–Bonferroni correction test was applied to all multi-variant comparisons. The threshold for statistical significance was set to a p value of 0.05. IBM SPSS Statistics v. 25.0 (IBM SPSS Statistics for Windows, Version 25.0, IBM Corp., Armonk, New York, USA) was used to perform all the computational analyses. JAMOVI version 2.3.21 (https://www.jamovi.org/) was used for drawing the survival curves.
The preplanned analyses were computed in the overall patient population and within each treatment group (pazopanib or cabozantinib).
During the study period, we enrolled 301 mRCC patients: 179 (59%) underwent
pazopanib, while 122 (41%) were treated with cabozantinib. Baseline
clinicopathological characteristics in the overall population and TKI subgroups
are reported in Table 1. The median age was 68 years, with a clear prevalence of
males over females (68% vs 32%). According to IMDC criteria, 53% of
patients belonged to the intermediate prognostic group, while 95% of patients
had an ECOG PS of 0 or 1. The vast majority of patients underwent a nephrectomy
(85%). In regard to the sites of the metastases, the lung was the most common
(64%), followed by nodes (42%), and bones (37%), while glands and liver
accounted for 19% each. Pazopanib was administered as the first-line treatment
in 97% of cases, while cabozantinib was mainly administered as second (42%) or
further-line therapy (44%). The mean Hb value was 12.5 g/dL, while about
two-thirds of patients presented baseline macrocytosis (MCV levels
| Number of patients (%) | Overall | Pazopanib group | Cabozantinib group | |
| 301 (100%) | 179 (59%) | 122 (41%) | ||
| Median age (range) | 68 (36–89) | 70 (42–89) | 65 (36–85) | |
| Sex (%) | ||||
| Male | 206 (68.4) | 126 (70.4) | 80 (65.6) | |
| Female | 95 (31.6) | 52 (29.4) | 42 (34.4) | |
| Histology (%) | ||||
| Clear cell | 250 (83.1) | 152 (84.9) | 98 (80.3) | |
| Papillary | 24 (8.0) | 11 (6.1) | 13 (10.7) | |
| Chromophobe | 8 (2.7) | 5 (2.8) | 3 (2.5) | |
| NOS | 19 (6.3) | 11 (6.1) | 8 (6.6) | |
| IMDC score (%) | ||||
| Good | 103 (34.2) | 65 (36.3) | 38 (31.1) | |
| Intermediate | 159 (52.8) | 92 (51.4) | 67 (54.9) | |
| Poor | 39 (13.0) | 22 (12.3) | 17 (13.9) | |
| ECOG PS (%) | ||||
| 0 | 183 (60.8) | 10 (61.5) | 73 (59.8) | |
| 1 | 102 (33.9) | 61 (34.1) | 41 (33.6) | |
| 2–3 | 16 (5.4) | 8 (4.5) | 8 (6.5) | |
| NLR (%) | ||||
| 183 (60.8) | 80 (44.7) | 43 (35.2) | ||
| 102 (33.9) | 75 (41.9) | 65 (53.3) | ||
| NA | 38 (12.6) | 24 (13.4) | 14 (11.5) | |
| Nephrectomy (%) | ||||
| Yes | 256 (85) | 149 (83.2) | 107 (87.7) | |
| No | 45 (15) | 30 (16.8) | 15 (12.3) | |
| Median number of metastatic sites (range) | 2 (1–8) | 2 (1–6) | 3 (1–8) | |
| Sites of metastasis (%) | ||||
| Lung | 194 (64.5) | 116 (64.8) | 78 (63.9) | |
| Liver | 58 (19.3) | 29 (16.2) | 29 (23.8) | |
| Nodes | 126 (41.9) | 58 (32.4) | 68 (55.7) | |
| Bone | 112 (37.2) | 53 (29.6) | 59 (48.4) | |
| Glands | 58 (19.3) | 30 (33.5) | 28 (23.0) | |
| Other | 114 (37.9) | 60 (33.5) | 54 (44.3) | |
| Use of PPI (%) | ||||
| Yes | 132 (43.9) | 69 (38.5) | 63 (51.6) | |
| No | 169 (56.1) | 110 (61.5) | 59 (48.4) | |
| Line of treatment (%) | ||||
| 1st | 192 (63.8) | 175 (97.8) | 17 (13.9) | |
| 2nd | 54 (17.9) | 3 (1.0) | 51 (41.8) | |
| 55 (18.3) | 1 (0.2) | 54 (44.2) | ||
| Hb values | ||||
| 121 (40.2) | 61 (34.1) | 60 (49.2) | ||
| 180 (59.8) | 118 (65.9) | 62 (50.8) | ||
| MCV | ||||
| 102 (33.9) | 68 (38.0) | 34 (27.9) | ||
| 199 (66.1) | 111 (62.0) | 88 (72.1) | ||
| RDW | ||||
| 164 (54.5) | 108 (60.3) | 57 (46.7) | ||
| 137 (45.5) | 71 (39.7) | 65 (53.3) | ||
Abbreviations: NOS, not otherwise specified; IMDC score, International Metastatic RCC Database Consortium Score; ECOG PS, Eastern Cooperative Oncology Group Performance Status; NLR, neutrophil-to-lymphocyte ratio; NA, not available; PPI, proton pump inhibitor; Hb, hemoglobin; MCV, mean corpuscular volume; RDW, red cell distribution width.
In the overall population, the median PFS (mPFS) and OS (mOS) were 12.0 (95% CI 9.5–14.6) and 25.8 months (95% CI 21.3–30.2), respectively.
Based on our preliminary data, which strongly suggested positive prognostic
values of Hb
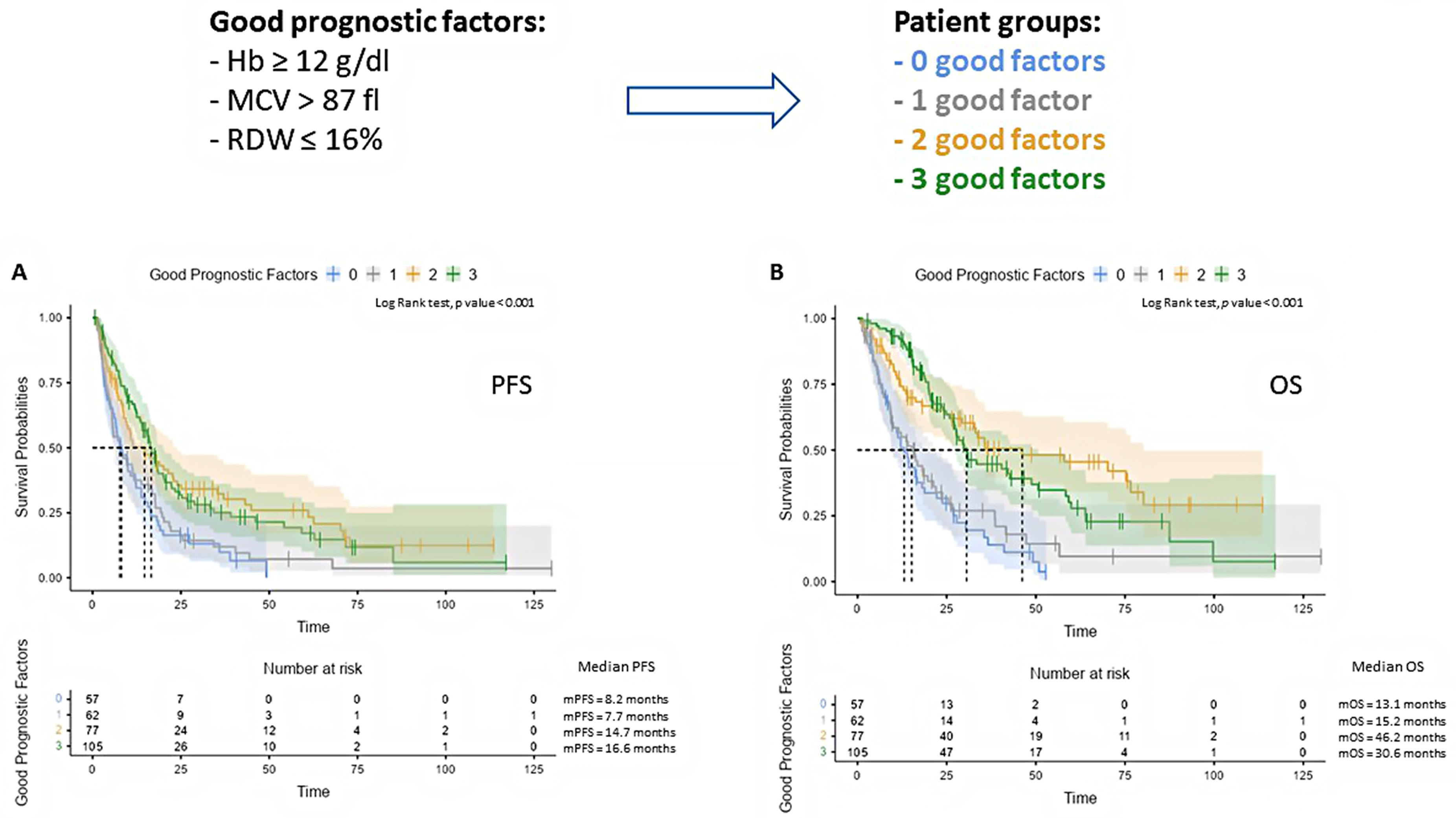 Fig. 1.
Fig. 1.Representative Kaplan–Meier curves illustrating the impact of the number of good prognostic factors on patient PFS (A) and OS (B). Number at risk is reported at the bottom of the curve. Hb, hemoglobin; MCV, mean corpuscolar volume; RDW, red cell distribution width; OS, overall survival; PFS, progression-free survival.
Significance was preserved for both PFS and OS in pazopanib-treated patients (Supplementary Fig. 1Ai and Aii), while only for OS in cabozantinib-treated mRCC (Supplementary Fig. 2Ai and Aii), after stratifying patients by TKI agents
In view of this preliminary finding, we developed a red cell-based “blood score” that allowed us to split our patient population into two categories: favorable (2–3 good factors) and unfavorable (0–1 good factors). Thereafter, the impact on PFS and OS was even more remarkable (mPFS 16.3 (95% CI 13.4–19.1) vs 7.9 (95% CI 5.3–10.4) months; mOS 33.7 (95% CI 23.9–43.4) vs 14.1 (95% CI 10.3–17.9) months), as clearly highlighted in Fig. 2A,B.
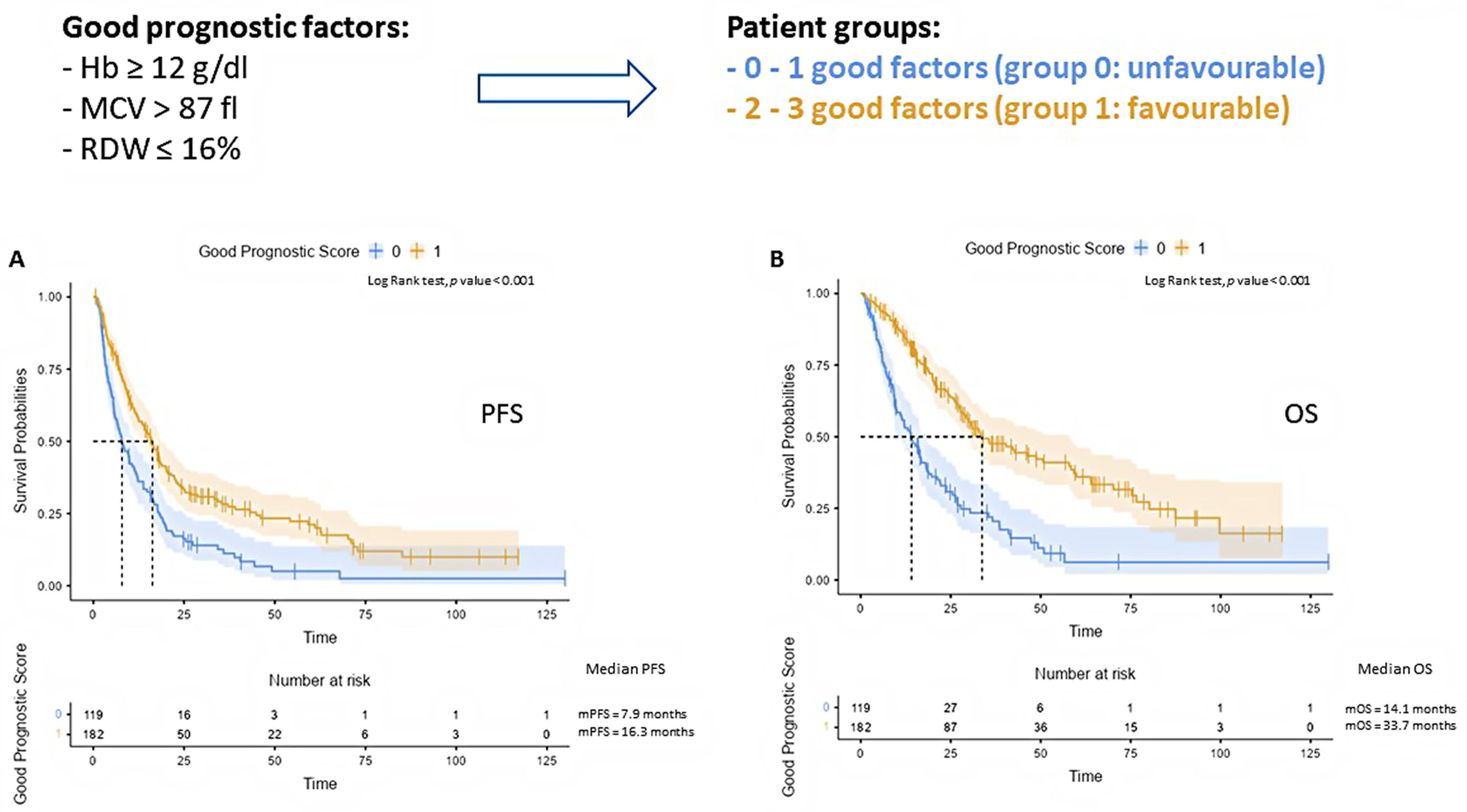 Fig. 2.
Fig. 2.Representative Kaplan–Meier curves illustrating the impact of our red blood cell-based score on patient PFS (A) and OS (B). Number at risk is reported at the bottom of the curve.
When we separately analyzed the outcome of the pazopanib and cabozantinib
populations, the prognostic value of our integrated score was maintained in both
subgroups. Specifically, in the pazopanib-treated subgroup presenting 2–3 good
factors (favorable group), where the median PFS (17.7 months, 95% CI
13.8–21.6), and OS (46.2 months 95% CI 10.4–17.8) were significantly longer
compared to the unfavorable group (p
To further confirm the prognostic impact of our integrated score, we applied
univariable and multivariable regression models that, in addition to our
multiparametric score, encompassed predetermined key covariates: sex (male
vs female), ECOG-PS (0 vs
As reported in Table 2, in the univariate analysis, ECOG PS
| PFS | Univariate | Multivariate | |||||
| HR | 95% CI | Adj. p value | HR | 95% CI | Adj. p value | ||
| Sex | p = 0.073 | ||||||
| Male | ref | ||||||
| Female | 0.77 | 0.59–1.02 | |||||
| ECOG PS | p = 0.014 | p = 0.904 | |||||
| 0 | ref | ref | |||||
| 1.48 | 1.08–1.85 | 1.06 | 0.76–1.48 | ||||
| Histology | p = 0.028 | p = 0.016 | |||||
| Clear Cell | ref | ref | |||||
| Papillary | 1.58 | 0.98–2.55 | 1.58 | 0.93–2.68 | |||
| Chromophobe | 2.53 | 1.24–5.14 | 2.81 | 1.34–5.89 | |||
| Other | 0.67 | 0.38–1.17 | 0.88 | 0.48–1.64 | |||
| IMDC | p = 0.01 | p | |||||
| Good | ref | ref | |||||
| Intermediate | 1.08 | 0.81–1.43 | 0.93 | 0.68–1.28 | |||
| Poor | 2.95 | 1.99–4.37 | 2.25 | 1.44–3.52 | |||
| NLR | p = 0.014 | p = 0.028 | |||||
| ref | ref | ||||||
| 1.55 | 1.18–2.04 | 1.38 | 1.03–1.83 | ||||
| Liver metastasis | p = 0.042 | p = 0.043 | |||||
| No | ref | ref | |||||
| Yes | 1.45 | 1.06–1.99 | 1.43 | 1.01–2.02 | |||
| Bone metastasis | p = 0.028 | p = 0.060 | |||||
| No | ref | ref | |||||
| Yes | 1.43 | 1.10–1.85 | 1.32 | 0.99–1.77 | |||
| Use of PPIs | p = 0.01 | p = 0.018 | |||||
| No | ref | ref | |||||
| Yes | 1.55 | 1.20–2.205 | 1.42 | 1.06–1.89 | |||
| Nephrectomy | p = 0.014 | p = 0.939 | |||||
| No | ref | ref | |||||
| Yes | 0.59 | 0.42–0.82 | 1.02 | 0.67–1.54 | |||
| Red blood cell-based score | p = 0.01 | p = 0.069 | |||||
| 0–1 factors (unfavorable group) | ref | ref | |||||
| 2–3 factors (favorable group) | 0.56 | 0.43–0.72 | 0.74 | 0.55–1.02 | |||
Abbreviations: 95% CI, 95% confidence intervals; PFS, progression-free survival; ECOG PS, Eastern Cooperative Oncology Group Performance Status. IMDC, International mRCC Database Consortium criteria; NLR, neutrophil-to-lymphocyte ratio; PPIs, proton pump inhibitors.
Adjusted p values following Holm–Bonferroni post-hoc test. HR, Hazard ratio; ref, reference.
| OS | Univariate | Multivariate | |||||
| HR | CI (95%) | Adj. p value | HR | CI (95%) | Adj. p value | ||
| Sex | p = 0.192 | ||||||
| Male | ref | ||||||
| Female | 0.74 | 0.53–1.02 | |||||
| ECOG PS | p = 0.01 | p = 0.725 | |||||
| 0 | ref | ref | |||||
| 1.68 | 1.26–2.24 | 1.04 | 0.77–1.40 | ||||
| Histology | p = 0.192 | ||||||
| Clear Cell | ref | ||||||
| Papillary | 1.70 | 1.02–2.82 | |||||
| Chromophobe | 1.67 | 0.78–3.56 | |||||
| Other | 0.73 | 0.38–1.39 | |||||
| IMDC | p = 0.01 | p | |||||
| Good | ref | ref | |||||
| Intermediate | 1.61 | 1.14–2.25 | 0.12 | 1.35–0.92 | |||
| Poor | 5.78 | 3.72–8.99 | 4.14 | 2.50–6.88 | |||
| NLR | p = 0.01 | p = 0.014 | |||||
| ref | ref | ||||||
| 1.73 | 1.26–2.36 | ||||||
| Liver metastasis | p = 0.192 | ||||||
| No | ref | ||||||
| Yes | 1.30 | 0.91–1.86 | |||||
| Bone metastasis | p = 0.06 | ||||||
| No | ref | ||||||
| Yes | 1.44 | 1.07–1.93 | |||||
| Use of PPIs | p = 0.01 | p = 0.005 | |||||
| No | ref | ref | |||||
| Yes | 1.67 | 1.25–2.22 | 1.58 | 1.51–2.16 | |||
| Nephrectomy | p = 0.01 | p = 0.920 | |||||
| No | ref | ref | |||||
| Yes | 0.46 | 0.32–0.65 | 0.97 | 0.62–1.53 | |||
| Red blood cell-based score | p = 0.01 | p | |||||
| 0–1 factors (unfavorable group) | ref | ref | |||||
| 2–3 factors (favorable group) | 0.38 | 0.29–0.51 | 0.53 | 0.39–0.75 | |||
Abbreviations: 95% CI, 95% confidence intervals; PFS, progression-free survival; ECOG PS, Eastern Cooperative Oncology Group Performance Status. IMDC, International mRCC Database Consortium criteria; NLR, neutrophil-to-lymphocyte ratio; PPIs, proton pump inhibitors.
Adjusted p values following Holm–Bonferroni post-hoc test. HR, Hazard ratio; ref, reference.
When challenged in the multivariate model, the prognostic value of histology,
IMDC, NLR, liver metastases, and proton pump inhibitor (PPI) use was confirmed, in terms of PFS (Table 2), while only IMDC, NLR, and PPI use reached statistical significance for OS
(Table 3). Of note, the blood score retained its highly significant impact on OS
(HR 0.53, 95% CI 0.39–0.75, p
TKIs are currently recommended both as first-line (alone or in combination with ICIs) and further lines of treatment in mRCC; however, only a portion of mRCC patients are able to gain a meaningful benefit, meaning the prediction of any long-term responses to these treatments remains a challenging and unsolved issue [32, 33]. Therefore, effective and easily exploitable predictive markers are required for individual clinical trial design and patient management. Thus, we aimed to unveil the potential prognostic role of a multiparametric blood score, which accounts for predetermined features, such as baseline Hb concentration, MCV, and RDW, in mRCC patients treated with anti-VEGF TKIs.
Among tumor- and patient-specific parameters, the reliability of anemia, a
well-established risk factor in the MSKCC score developed during the cytokine era
[18], has been extensively investigated in the context of the TKI-driven
therapeutic landscape. Indeed, evidence has been presented numerous times
indicating that serum hemoglobin below the lower limit of normal (LLN) was a
meaningful predictor for shorter OS and PFS [34, 35, 36, 37]. Conversely, the prognostic
significance of hemoglobin changes following TKI treatments is still debated and
under intense scrutiny. A number of studies reported a transient increase in
hemoglobin levels in 23.8% to 90% of mRCC patients, which peaked at 4–9 weeks
after the onset of treatment [38, 39]. Similarly, our preliminary
observations on 301 mRCC patients undergoing TKIs confirmed a significant rise in
blood Hb concentrations, with a mean increase of 1 g/dL, as early as day 15. The
underlying mechanism might reside in the reinforcement of the HIF-1
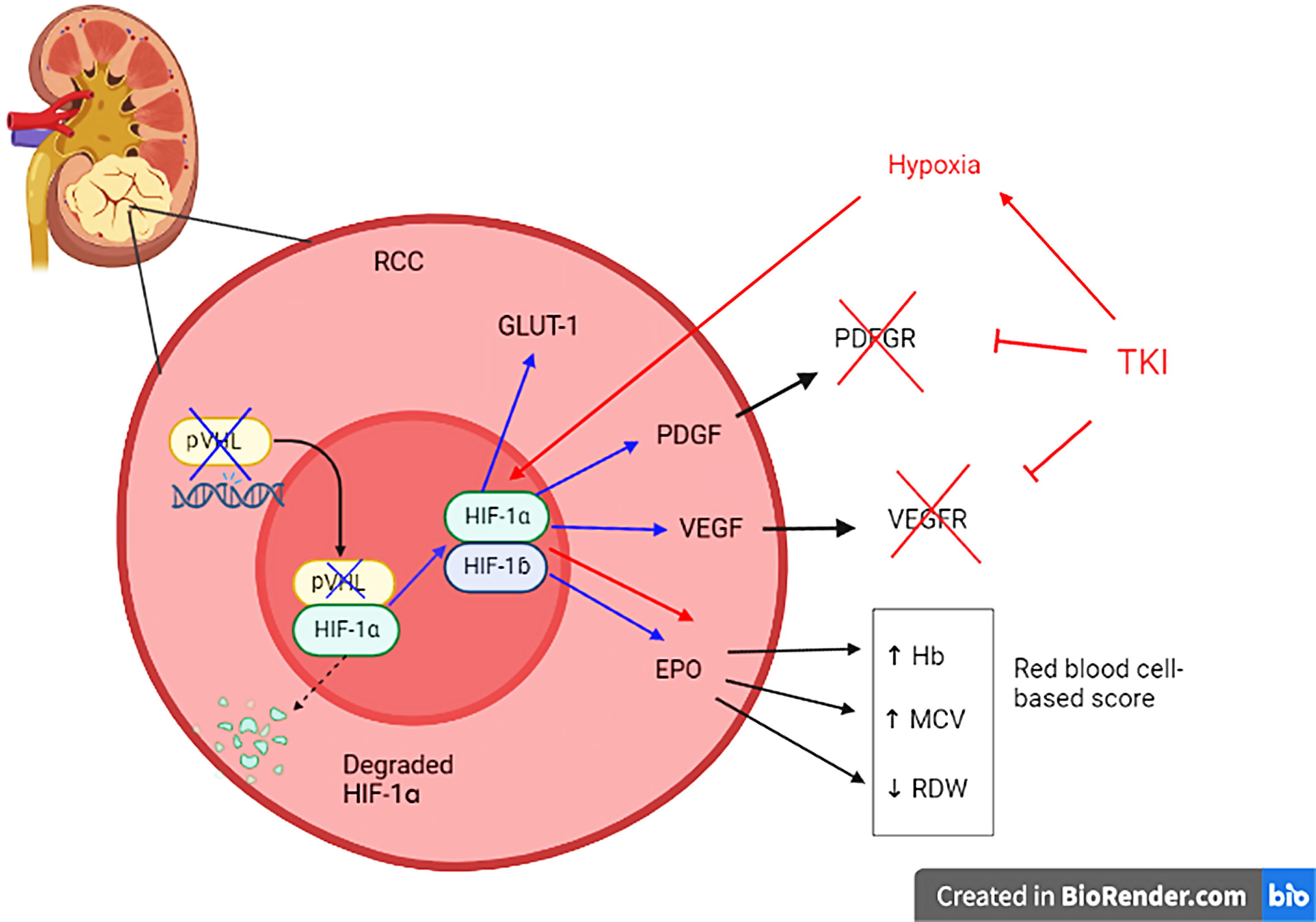 Fig. 3.
Fig. 3.Explanatory figure illustrating the HIF-
A few investigations have also demonstrated that increased hemoglobin may be associated with longer survival [38, 40, 41, 42]. Conversely, despite the limitation of including small sample size and lack of correction for well-known clinical prognostic factors, a retrospective analysis by Tripathi et al. [43] documented significantly shorter time to treatment failure (TTTF) and PFS in patients displaying an increase in Hb levels.
Concerning the role of macrocytosis in mRCC patients, it has been repeatedly reported that its onset following TKI treatment correlated to a better survival outcome [26, 27, 28]. This evidence may be linked with the role of c-KIT-mediated signaling which, upon TKI inhibition, could determine an impaired maturation of blood elements derived from c-KIT expressing hematopoietic stem cells, and the consequent release of larger erythrocytes into the bloodstream [25].
Finally, among red blood cell-centered features, the presence of anisocytosis was negatively associated with mRCC survival, as effectively demonstrated in a retrospective observational study that included patients treated with sunitinib or pazopanib [31].
In the current investigation, we first revealed the clinical impact of combining
Hb levels, MCV, and RDW on mRCC patient outcomes. Thereafter, we developed a
multiparametric blood score integrating all the above-mentioned factors and
delineating two prognostic categories. Specifically, patients carrying at least 2
good prognostic factors (Hb
Based on these findings, we hypothesized that elevated Hb, macrocytosis, and low
anisocytosis may be sustained by EPO stimulation depending on HIF-1
In spite of the intrinsic limitation of a retrospective nature, the multicenter involvement, the adequate median follow-up, the balanced TKI type, and the treatment line, represent strengths in our study. Moreover, the high prognostic performance of our red blood cell score likely resided in its multiparametric nature, is independent of the TKI drugs and might be effectively exploitable in clinical practice since the proposed circulating parameters could be easily obtained by a “simple” blood sample.
To the best of our knowledge, the present work is the first retrospective observational investigation to provide evidence on the clinical relevance and applicability of a multiparametric blood score based on hemoglobin levels, MCV, and RDW values and can be used to identify mRCC patients who might gain benefit from TKI therapy (cabozantinib or pazopanib).
In-depth analyses aimed at assessing circulating EPO and erythroblasts that will corroborate our hypothesis are currently ongoing.
Future studies are warranted to prospectively test the validity of our score in mRCC patients treated with immune combinations.
All data generated or analyzed during this study are included in this published article.
GM: conceptualization, project administration, visualization, writing – original draft, writing: review & editing; AL: data curation, writing – original draft; MSa: data curation, review, editing; FT: data curation, writing – original draft; UDG: data curation, review, editing; NB: data curation, review, editing; CT: data curation, review, editing; SP: data curation, review, editing; OC: data curation, review, editing; SK: data curation, review, editing; AMe: data curation, review, editing; CC: data curation, review, editing; EV: data curation, review, editing; AR: data curation, review, editing; MSt: data curation, review, editing; AMa: data curation, review, editing; GR: data curation, review, editing; EMS: data curation, review, editing; PR: data curation, review, editing; SER: data curation, review, editing; GF: data curation, review, editing; GCG: visualization, data curation, review, editing; GLB: data curation, critical review, editing; FQ: data curation, review, editing; SB: conceptualization, data curation, formal analysis, methodology, project administration, visualization, writing – original draft, writing: review & editing. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was conducted following the approval by the ethics committee of the coordinating Center (protocol number 208/2021/OSS/AOUPR MA.RE.CA.P., date of approval: September 1, 2021) and the obtainment of patient informed consent.
Not applicable.
This research received no external funding.
Sebastiano Buti received honoraria as a speaker at scientific events and advisory role by Bristol-Myers Squibb (BMS), Pfizer; MSD, Ipsen, AstraZeneca and Novartis; he also received research funding from Novartis, but we can confirm that these grants do not interfere at all with this manuscript and the presented data. The other authors have no conflicts of interest to disclose.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.