




1 Center for Coronary Artery Disease (CCAD), Beijing Anzhen Hospital, and Beijing Institute of Heart, Lung and Blood Vessel Diseases, Capital Medical University, 100029 Beijing, China
†These authors contributed equally.
Academic Editor: Carlo Briguori
Abstract
Background: Several complications can contribute to the risk of shock during the chronic total occlusion (CTO) percutaneous coronary intervention (PCI) procedure. However, some patients that develop shock do not exhibit any apparent complications, and few studies to date have discussed the risk of unexplained perioperative shock in patients undergoing CTO PCI. Accordingly, this study was designed with the goal of defining perioperative risk factors linked to the odds of unexplained shock during CTO PCI. Methods: In total, this study analyzed data from 924 patients that underwent CTO PCI without any in-hospital complications from January 2016–August 2021. Cardiologists collected data pertaining to patient clinical characteristics, laboratory findings, angiographic findings, and procedural characteristics. Patients were separated into two groups based upon whether or not they experienced perioperative shock. The relationship between specific variables and perioperative shock incidence was assessed via a multivariable stepwise logistic regression approach. A risk-scoring nomogram was then designed for use as a tool to guide patient risk assessment efforts during PCI procedural planning. Results: Overall, 4.8% of these patients (44/924) experienced unexplained perioperative shock. Independent predictors associated with unexplained shock during CTO PCI included baseline systolic pressure (odds ratio (OR) 0.968, 95% confidence interval (CI): 0.945–0.991), baseline heart rate (OR 1.055, 95% CI: 1.020–1.091), baseline hemoglobin (OR 0.970, 95% CI: 0.947–0.994), procedure duration (OR 1.008, 95% CI: 1.002–1.015), J-CTO score (OR 1.521, 95% CI: 1.021–2.267), and use of a retrograde approach (OR 3.252, 95% CI: 1.426–7.415). The unbiased C-index estimate was 0.859, and this model exhibited excellent calibration. Conclusions: The risk of unexplained shock is an important consideration for clinicians performing the CTO PCI procedure. These analyses revealed unexplained shock risk to be independently related to lower baseline systolic pressure, higher baseline heart rate, lower baseline hemoglobin, more procedure time, higher J-CTO score, and more use of a retrograde approach.
Keywords
- chronic total occlusion
- complication
- shock
- percutaneous coronary intervention
Several new techniques and pieces of equipment have been developed over the past 10 years to overcome to complexities inherent to the chronic total occlusion (CTO) percutaneous coronary intervention (PCI) procedure, thereby improving operative success rates [1, 2]. When successful, CTO PCI can contribute to the alleviation of patient symptoms and prolonged survival [3, 4]. However, the utility of the CTO PCI procedure is limited by the potential for serious complications that can negatively impact patient prognosis [5, 6]. In severe cases, patients may exhibit cardiac or non-cardiac complications that can contribute to the incidence of hypotension and potentially circulatory shock [7]. Despite these risks, hypotension and shock are often not included in lists of procedure-related complications in published studies [2] and scoring systems. In clinical settings, a subset of patients who experience shock do not exhibit any serious CTO PCI complications, and shock can even occur in a subset of patients who undergo successful CTO PCI treatment, necessitating the prolonged use of vasoactive drugs to maintain appropriate blood pressure. No reports to data have described this form of unexplained perioperative shock associated with the CTO PCI procedure. As such, this retrospective study was designed to survey the incidence of unexplained CTO PCI-related shock and to identify associated risk factors.
This retrospective analysis incorporated data from 1165 consecutive patients that underwent the CTO PCI procedure in Beijing Anzhen Hospital, Capital Medical University from January 2016 to August 2021. Of these patients, 924 were ultimately included in this study based on defined inclusion/exclusion criteria. These patients were separated into two groups based upon they did or did not develop perioperative shock (n = 44 and n = 880, respectively). The study flowchart is shown in Fig. 1, while in-hospital periprocedural complications are detailed in Table 1. The Institutional Review Board of our center approved this study. All CTO PCI procedures were performed by an experienced team of cardiologists.
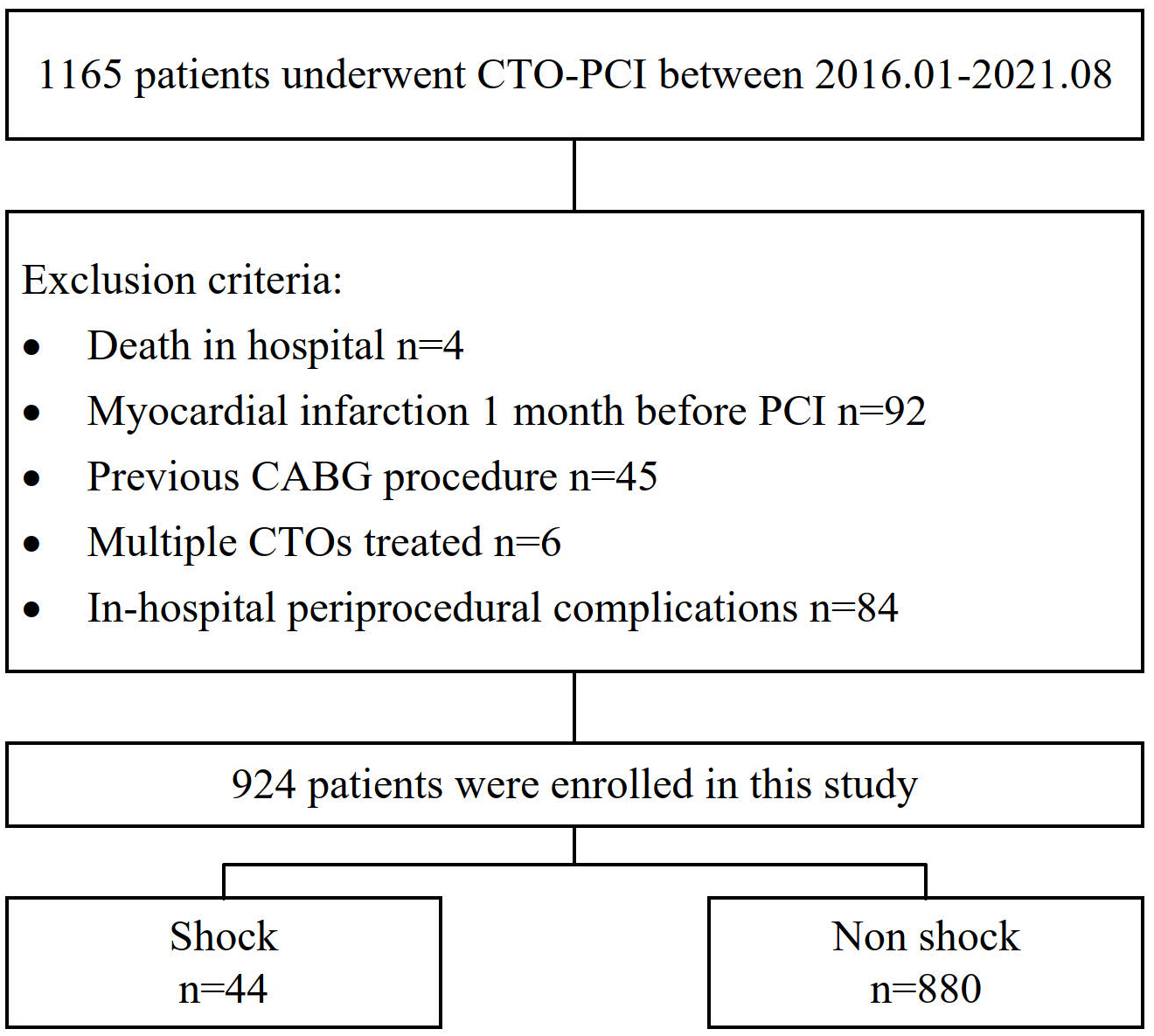 Fig. 1.
Fig. 1.Flow chart of this study.
| Complication | n = 84 |
| No-reflow or slow-flow | n = 2 |
| Arrhythmia requiring treatment | n = 4 |
| Coronary perforation | n = 14 |
| Donor vessel injury | n = 8 |
| Acute thrombosis | n = 2 |
| Vascular access complications | n = 18 |
| Major bleeding* | n = 48 |
| Vascular access complications & bleeding | n = 6 |
| One patient was major bleeding with coronary perforation; one patient was major
bleeding with donor vessel injury. *A drop in the hemoglobin of | |
Shock was defined as systolic blood pressure (SBP)
CTO PCI technical success was defined by achieving a TIMI grade
Categorical variables are reported as percentages and were compared via Fisher’s
exact test or Pearson chi-square tests, whereas continuous variables are reported
as means
The majority of patients included in this study were male and of Asian
ethnicity. Of these patients 69.1% had hypertension, 48.9% had undergone prior
PCI, and 35.6% were diabetic. The mean ejection fraction for these patients was
60.1%
| Variable | Overall | Shock | p value | |
| (n = 924) | Yes (n = 44) | No (n = 880) | ||
| Gender (Female) | 168 (18.4%) | 9 (20.0%) | 159 (18.3%) | 0.689 |
| Age, y | 58.4 |
56.8 |
58.5 |
0.264 |
| BMI, kg/m |
26.4 |
25.3 |
26.5 |
0.049 |
| Baseline systolic pressure, mmHg | 127.9 |
122.8 |
128.1 |
0.029 |
| Baseline diastolic pressure, mmHg | 72.6 |
70.8 |
72.7 |
0.268 |
| Baseline heart rate, /min | 71.9 |
76.1 |
71.7 |
0.022 |
| Hypertension | 636 (69.1%) | 28 (63.6%) | 608 (69.1%) | 0.446 |
| Diabetes mellitus | 326 (35.3%) | 11 (25.0%) | 315 (35.8%) | 0.144 |
| Dyslipidemia | 766 (82.9%) | 34 (77.3%) | 732 (83.2%) | 0.310 |
| Prior stroke | 40 (4.3%) | 0 (0%) | 40 (4.5%) | 0.148 |
| Atrial fibrillation | 10 (1.1%) | 2 (4.5%) | 8 (0.9%) | 0.078 |
| Prior myocardial infarction | 246 (26.6%) | 15 (34.1%) | 231 (26.2%) | 0.251 |
| Prior PCI | 452 (48.9%) | 28 (63.6%) | 424 (48.2%) | 0.045 |
| Current tobacco use | 367 (39.7%) | 16 (36.4%) | 351 (39.9%) | 0.641 |
| Echocardiography | ||||
| Ejection fraction | 60.1 |
60.3 |
60.1 |
0.586 |
| Ejection fraction |
29 (3.1%) | 0 (0%) | 29 (3.3%) | 0.392 |
| Ejection fraction |
92 (10.0%) | 3 (6.8%) | 89 (10.1%) | 0.609 |
| LVEDD | 49.0 |
48.2 |
49.0 |
0.648 |
| LVESD | 32.8 |
32.8 |
32.8 |
0.263 |
| Ventricular aneurysm | 42 (4.5%) | 0 (0%) | 42 (4.8%) | 0.260 |
| Valvular regurgitation (moderate-severe) | 42 (4.5%) | 5 (11.4%) | 37 (4.2%) | 0.044 |
| Medication | ||||
| Aspirin | 924 (100%) | 44 (100%) | 880 (100%) | - |
| Clopidogrel | 679 (73.9%) | 30 (68.2%) | 649 (73.7%) | 0.414 |
| Ticagrelor | 245 (26.5%) | 14 (31.8%) | 231 (26.3%) | 0.414 |
| ACEI/ARB | 436 (47.2%) | 17 (38.6%) | 419 (47.6%) | 0.244 |
| 599 (64.8%) | 33 (75.0%) | 566 (63.2%) | 0.148 | |
| Nitrates | 713 (77.2%) | 35 (79.5%) | 678 (77.0%) | 0.700 |
| Calcium channel blocker | 274 (29.7%) | 12 (27.3%) | 262 (29.8%) | 0.723 |
| Loop diuretics | 108 (11.7%) | 5 (11.4%) | 103 (11.7%) | 0.945 |
| Statin | 898 (97.2%) | 44 (100%) | 854 (97.0%) | 0.247 |
| Aldosterone receptor antagonist | 58 (6.3%) | 4 (9.1%) | 54 (6.1%) | 0.350 |
| Oral anticoagulants | 12 (1.3%) | 2 (4.5%) | 10 (1.1%) | 0.108 |
| Low molecular heparin | 123 (13.3%) | 7 (15.9%) | 116 (13.2%) | 0.603 |
| BMI, body mass index; ACEI, angiotensin converting enzyme inhibitors; ARB, angiotensin receptor blocker; LVEDD, left ventricular end diastolic diameter; LVESD, left ventricular end systolic diameter; PCI, percutaneous coronary intervention. | ||||
Relative to patients that did not experience shock, those that did experience
shock exhibited lower baseline RBC levels (4.4
| Variable | Overall | Shock | p value | |
| (n = 924) | Yes (n = 44) | No (n = 880) | ||
| WBC, 10 |
6.9 |
6.8 |
6.9 |
0.319 |
| Baseline RBC, 10 |
4.6 |
4.4 |
4.6 |
0.021 |
| Post operation RBC, 10 |
4.4 |
3.9 |
4.4 |
0.000 |
| Baseline Hb, g/L | 140.5 |
135.8 |
140.8 |
0.030 |
| Post operation Hb, g/L | 132.4 |
120.0 |
133.2 |
0.000 |
| 8.0 |
15.6 |
7.6 |
0.000 | |
| PLT, 109/L | 217.9 |
217.0 |
217.9 |
0.736 |
| Creatinine, mg/mL | 0.83 |
0.81 |
0.84 |
0.646 |
| TC, mmol/L | 4.5 |
10.4 |
4.3 |
0.485 |
| TG, mmol/L | 1.8 |
1.5 |
1.8 |
0.050 |
| HDL-C, mmol/L | 1.0 |
0.9 |
1.0 |
0.357 |
| LDL-C, mmol/L | 2.2 |
2.0 |
2.2 |
0.040 |
| Hs-CRP, mg/L | 3.4 |
1.8 |
3.5 |
0.168 |
| D-dimer, ng/mL | 129.0 |
120.9 |
129.4 |
0.294 |
| BNP, pg/mL | 100.8 |
86.6 |
101.6 |
0.472 |
| WBC, white blood cell; RBC, red blood cell; Hb, hemoglobin; PLT, platelet; TC, total cholesterol; TG, triacylglycerol; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; Hs-CRP, hypersensitive C-reactive protein; BNP, B-type natriuretic peptide. | ||||
Patient angiographic and procedural characteristics are summarized in Table 4.
The average operative duration was higher among patients that experienced shock
relative to patients that did not (144.4
| Variable | Overall | Shock | p value | |
| (n = 924) | Yes (n = 44) | No (n = 880) | ||
| Procedure time, minute | 91.2 |
144.4 |
88.6 |
0.000 |
| Coronary artery dominance | ||||
| Left dominant | 56 (6.1%) | 1 (2.3%) | 55 (6.3%) | 0.512 |
| Right dominant | 753 (81.5%) | 39 (88.6%) | 714 (81.1%) | 0.211 |
| Codominant | 115 (12.4%) | 4 (9.4%) | 111 (12.6%) | 0.490 |
| Multivessel lesions | 702 (76.0%) | 34 (77.3%) | 668 (75.9%) | 0.836 |
| Multiple CTO lesions | 59 (6.4%) | 1 (2.3%) | 58 (6.6%) | 0.355 |
| ISR CTO | 86 (9.3%) | 6 (13.6%) | 80 (9.1%) | 0.289 |
| Target vessel | ||||
| LAD | 374 (40.5%) | 18 (40.9%) | 356 (40.5%) | 0.952 |
| LCX | 143 (15.1%) | 1 (1.4%) | 142 (16.1%) | 0.013 |
| RCA | 392 (42.4%) | 25 (56.8%) | 367 (41.7%) | 0.048 |
| Side branch at proximal cap | 448 (48.5%) | 24 (54.5%) | 424 (48.2%) | 0.410 |
| Distal cap at bifurcation | 241 (26.1%) | 19 (43.2%) | 222 (25.2%) | 0.008 |
| Proximal segment target | 343 (37.1%) | 23 (52.3%) | 320 (36.4%) | 0.033 |
| Blunt/no stump | 666 (72.1%) | 37 (84.1%) | 624 (70.7%) | 0.069 |
| Moderate/severe tortuosity | 291 (31.5%) | 19 (43.2%) | 272 (30.9%) | 0.087 |
| CTO Length |
648 (70.1%) | 38 (86.4%) | 610 (69.4%) | 0.016 |
| Moderate/severe calcification | 72 (7.8%) | 4 (9.4%) | 68 (7.8%) | 0.770 |
| Prior CTO PCI attempt | 79 (8.5%) | 11 (25.0%) | 68 (7.8%) | 0.001 |
| No interventional collaterals | 48 (5.2%) | 0 (0%) | 48 (5.5%) | 0.162 |
| Bad distal landing zone | 30 (3.2%) | 1 (1.4%) | 29 (3.2%) | 1.000 |
| J-CTO score | 1.9 |
2.5 |
1.9 |
0.000 |
| J-CTO score |
631 (68.3%) | 36 (81.8%) | 595 (67.6%) | 0.048 |
| Use of femoral access | 447 (48.4%) | 30 (68.2%) | 417 (47.4%) | 0.007 |
| Retrograde approach | 136 (14.7%) | 25 (56.8%) | 111 (12.6%) | 0.000 |
| Knuckle technique | 29 (3.1%) | 4 (9.4%) | 25 (2.8%) | 0.044 |
| Externalization technique | 69 (7.5%) | 16 (36.4%) | 53 (6.0%) | 0.000 |
| Reverse-CART technique | 16 (1.7%) | 1 (1.4%) | 15 (1.7%) | 0.545 |
| ADR(Stingray) technique | 11 (1.2%) | 1 (1.4%) | 10 (1.1%) | 0.417 |
| Procedural success | 789 (85.4%) | 39 (88.6%) | 750 (85.2%) | 0.532 |
| CTO, chronic total occlusion; ISR, in-stent restenosis; LAD, left anterior descending artery; LCX, left circumflex artery; RCA, right coronary artery; PCI, percutaneous coronary intervention; ADR, anterograde dissection reentry. | ||||
A multivariate stepwise logistic regression analysis identified six independent predictors of unexplained shock (Table 5), including baseline SBP (OR 0.968, 95% CI: 0.945–0.991), baseline heart rate (OR 1.055, 95% CI: 1.020–1.091), baseline Hb levels (OR 0.970, 95% CI: 0.947–0.994), operative duration (OR 1.008, 95% CI: 1.002–1.015), J-CTO score (OR 1.521, 95% CI: 1.021–2.267), and use of retrograde approach (OR 3.252, 95% CI: 1.426–7.415). Correspondnig adjusted odds ratios are shown in Table 6.
| Variable | Univariable analysis | Stepwise logistic regression | ||||
| Shock | No shock | p value | Odds ratio | 95% CI | p value | |
| (n = 44) | (n = 880) | |||||
| BMI, kg/m |
25.3 |
26.5 |
0.049 | |||
| Baseline systolic pressure, mmHg | 122.8 |
128.1 |
0.029 | 0.968 | 0.945–0.991 | 0.007 |
| Baseline heart rate, /min | 76.1 |
71.7 |
0.022 | 1.055 | 1.020–1.091 | 0.002 |
| Baseline Hb, g/L | 135.8 |
140.8 |
0.030 | 0.970 | 0.947–0.994 | 0.015 |
| LDL-C, mmol/L | 2.0 |
2.2 |
0.040 | |||
| Distal cap at bifurcation | 19 (43.2%) | 222 (25.2%) | 0.008 | |||
| Proximal segment target | 23 (52.3%) | 320 (36.4%) | 0.033 | |||
| Prior PCI | 28 (63.6%) | 424 (48.2%) | 0.045 | |||
| Valvular regurgitation (moderate-severe) | 5 (11.4%) | 37 (4.2%) | 0.044 | |||
| Procedure time, minute | 144.4 |
88.6 |
0.000 | 1.008 | 1.002–1.015 | 0.008 |
| J-CTO score | 2.5 |
1.9 |
0.000 | 1.521 | 1.021–2.267 | 0.039 |
| Use of femoral access | 30 (68.2%) | 417 (47.4%) | 0.007 | |||
| Knuckle technique | 4 (9.4%) | 25 (2.8%) | 0.044 | |||
| Retrograde approach | 25 (56.8%) | 111 (12.6%) | 0.000 | 3.252 | 1.426–7.415 | 0.005 |
| LCX target | 1 (1.4%) | 142 (16.1%) | 0.013 | |||
| RCA target | 25 (56.8%) | 367 (41.7%) | 0.048 | |||
| BMI, body mass index; LDL-C, low-density lipoprotein cholesterol; RBC, red blood cell; Hb, hemoglobin; LCX, left circumflex artery; RCA, right coronary artery; PCI, percutaneous coronary intervention. | ||||||
| Variable | Odds Ratio | 95% CI | p value |
| Baseline systolic pressure (per + 10 mmHg) | 0.721 | 0.568–0.915 | 0.007 |
| Baseline heart rate (per + 10 /min) | 1.704 | 1.219–2.381 | 0.002 |
| Baseline Hb (per + 10 g/L) | 0.741 | 0.583–0.943 | 0.015 |
| Procedure time (per + 30 mins) | 1.286 | 1.069–1.548 | 0.008 |
| J-CTO score (per + 1 point) | 1.521 | 1.021–2.267 | 0.039 |
| Use of retrograde approach | 3.252 | 1.426–7.415 | 0.005 |
| Hb, hemoglobin. | |||
These perioperative predictors were then used to design a nomogram capable of quantifying a given individual’s risk of experiencing unexplained shock (Fig. 2). ROC curves for the final model are shown in Fig. 3, with discrimination having been assessed based on an unbiased C-index estimate of 0.859.
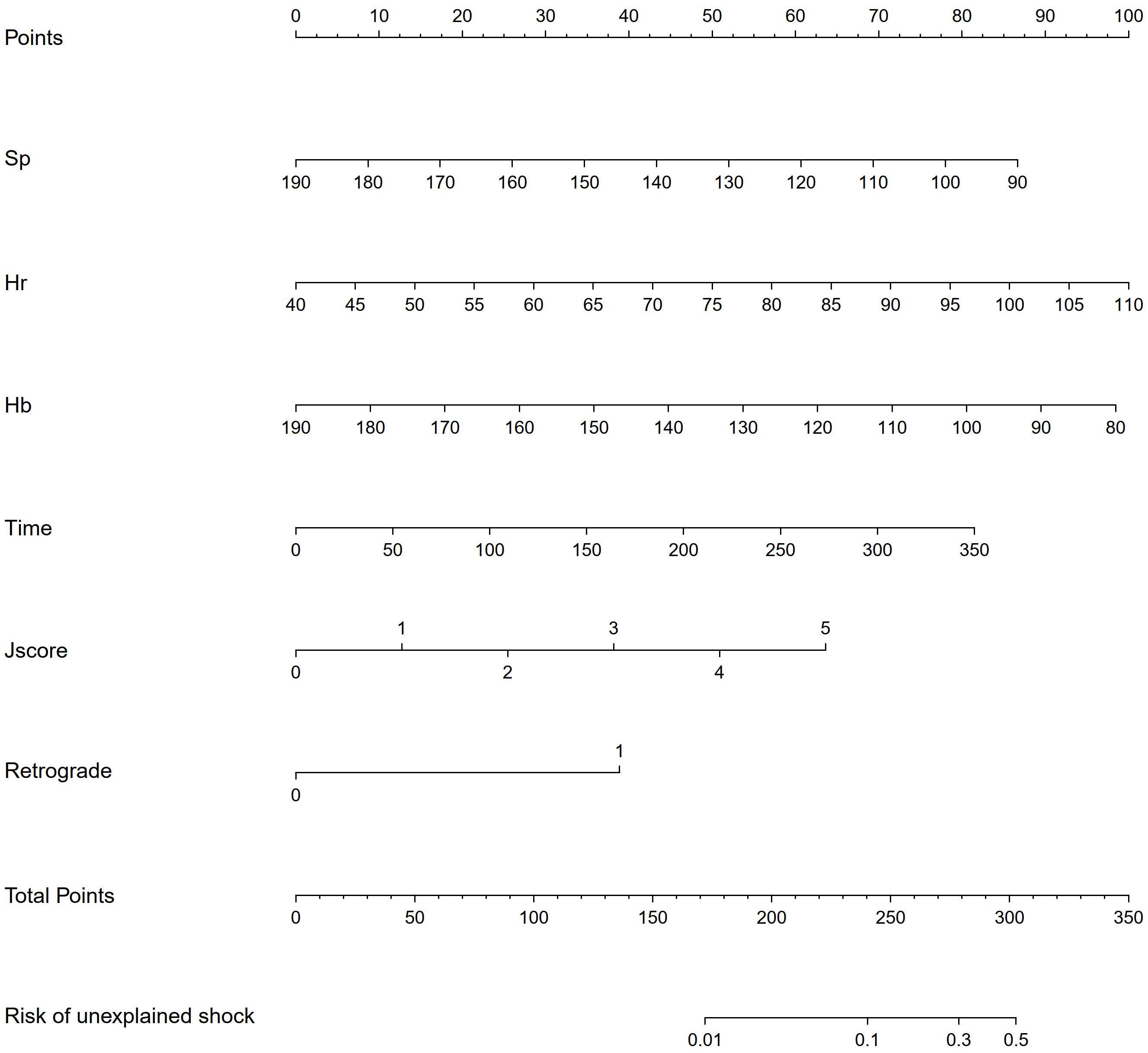 Fig. 2.
Fig. 2.Nomogram predicting the risk of unexplained shock based on dependent factors identified from multivariate logistic regression. Sp, systolic pressure, mmHg (baseline); Hr, heart rate, /min (baseline); HB, hemoglobin, g/L (baseline); Time, Procedure time, minute.
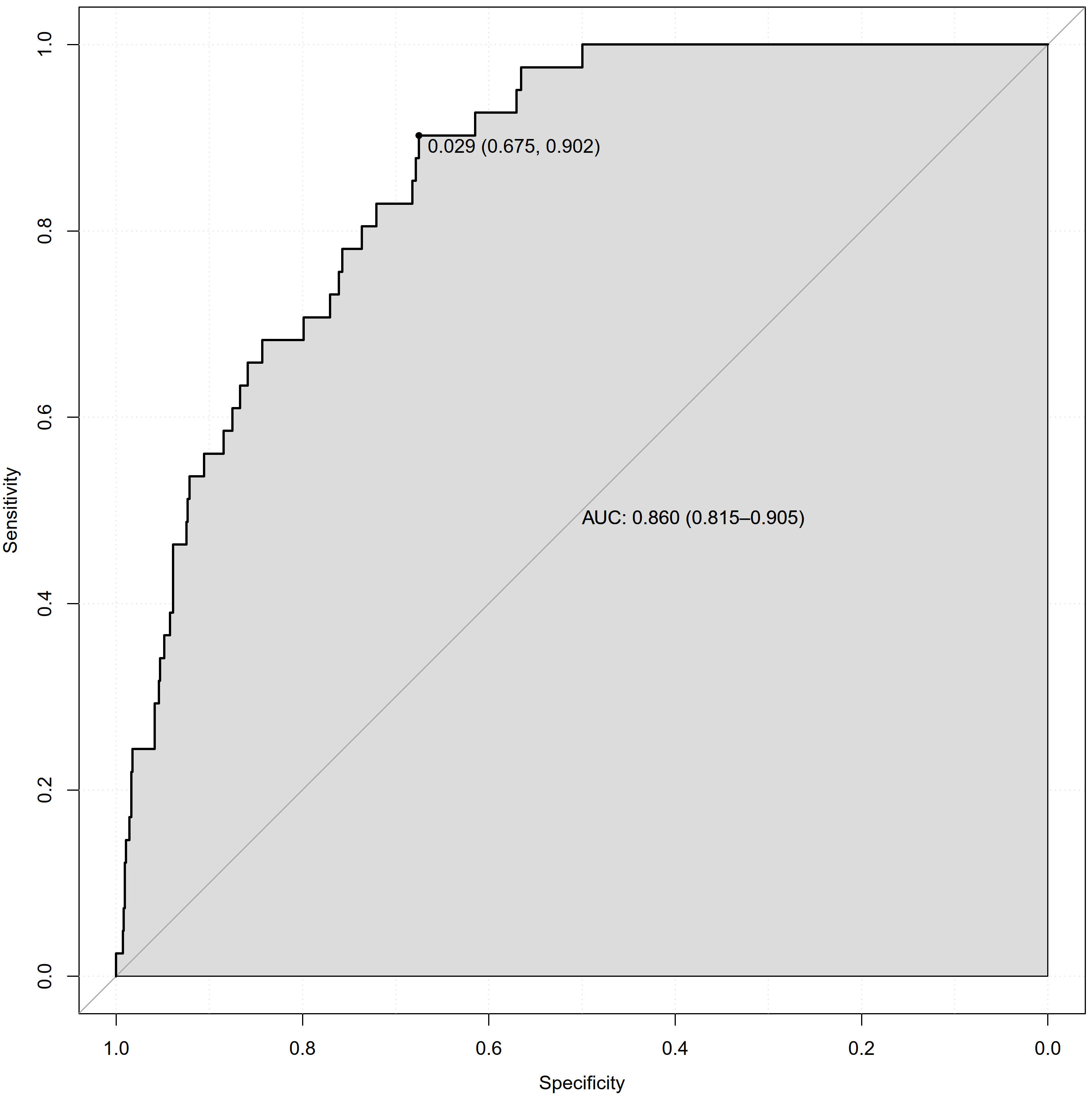 Fig. 3.
Fig. 3.ROC curve based on predicted probabilities obtained from the model. AUC, area-under-the-curve; ROC, receiver operating characteristic.
Unexplained shock is a potential CTO PCI procedural complication that has been the focus of insufficient study to date. The results of this study indicate that unexplained shock affected ~4.8% of CTO PCI patients, in addition to revealing 6 simple clinical indicators can be used to predict unexplained shock risk. This study is the first to our knowledge to have developed a model for the prediction of unexplained shock during CTO PCI, and these findings may be invaluable for future procedural planning efforts.
In a prior meta-analysis, a 3.1% pooled complication rate was reported for 18,061 cases [2], while a 2.8% complication rate was reported for 1569 hybrid CTO procedures in the PROGRESS registry [11]. The unexplained shock incidence rate for the 924 cases in this study (4.8%) was in line with the CTO complication rates reported previously [2]. This emphasizes the need for CTO operators to take this complication into consideration, given that shock-related data have not been reported for large CTO-related clinical studies such as the OPEN CTO study [12], EXPLORE study [13], and the EuroCTO study [14].
Shock is a clinical state wherein patients exhibit circulatory failure resulting in insufficient cellular oxygen utilization [15]. Shock is diagnosed based on a combination of hemodynamic, biochemical, and clinical findings [15]. Hypotension, which is common in the context of CTO PCI and can arise in response to many different factors, precedes shock [16, 17]. Certain causes of hypotension such as allergic reactions, vasovagal syndrome, guide interference with the aortic valve, or deep guide engagement can be alleviated through basic investigation and appropriate intervention [17]. Severe shock, however, is often caused by complications, and the differential diagnosis for complication-related shock is complex. Hypovolemic shock can arise due to access site complications and bleeding, while coronary complications such as donor vessel injury or perforation can exhibit a sudden and severe onset. When complication-related hypotension develops, it is vital that the underlying complications be rapidly treated to prevent progression to shock [18]. Most such complications are the result of the use of particular intraoperative procedures and techniques. Many different factors can contribute to the incidence of complications, and PROGRESS CTO complications scores offer value in the prediction of CTO PCI procedure-related complications [11]. Many patients suffering from shock, however, do not exhibit any apparent serious complications, with these cases being designated as instances of unexplained shock. Few studies to date have mentioned unexplained or complication-related shock when discussing CTO PCI-related procedural outcomes. As these two forms of shock may be driven by distinct underlying mechanisms, further efforts to differentiate between the two are warranted.
When comparing the two patient groups in this study, significant differences in
base-line SBP, heart rate, BMI, and prior PCI were observed. The association
between BP control and long-term PCI patient prognosis remains a matter of
controversy [19]. However, prior evidence has revealed a link between lower BP at
admission and in-hospital prognosis. Shiraish et al. [20] studied a
population of Japanese acute MI patients undergoing PCI, and found an SBP
As CTO PCI necessitates the utilization of large sheaths and is associated with
a high frequency of dual access, it is associated with a high risk of blood loss
[26]. Procedure-associated blood loss may represent an important cause of
unexplained shock incidence. Here, all cases exhibited a mean decrease in
hemoglobin levels of ~8 g/L (140.5
The risk of ischemia is higher for the CTO PCI procedure as compared to conventional PCI [16], in part owing to the use of additional contrast agents and a guiding catheter with a larger diameter. Certain techniques including retrograde PCI can contribute to donor artery or collateral channel ischemia [17]. While these events may not result in serious complications, they do decrease cardiac output. The extent to which these is- chemic risks are impacted following CTO opening remains to be established.
Several studies have identified severe cardiac insufficiency or low LV function
(LVEF
J-CTO scores are correlated with CTO complexity, with CTOs exhibiting a J-CTO
score
Overall, these findings suggest that a combination of ischemia and blood loss due to a variety of reasons can contribute to the incidence of unexplained shock among patients undergoing the CTO PCI procedure. While these patients may not experience complications in the traditional sense that are directly related to procedural success, efforts to mitigate CTO PCI-related blood loss and ischemia may protect against the incidence of unexplained shock. The risk scoring system developed herein has the potential to aid clinicians performing the CTO PCI procedure by enabling appropriate preoperative planning, arrangement, and strategy adjustment as necessary. The risk of shock for high-risk patients can be mitigated by reducing the operative duration to the greatest extent possible, employing retrograde techniques, and allowing more skilled operators to perform the procedure.
There are some limitations to this analysis. For one, this was a single-center retrospective study, and the results may thus not be representative of findings for other centers or operators. In addition, the mechanisms underlying unexplained shock were not clarified through this study, and further efforts to delineate these mechanisms may be critical to the treatment or prevention of this potentially serious clinical outcome. Moreover, these results do not offer any insight regarding long-term patient prognosis. Accordingly, we plan to perform future studies examining the mechanisms governing the incidence of unexplained shock and the long-term prognosis of these patients.
In summary, these results suggest that baseline systolic pressure, baseline heart rate, baseline hemoglobin levels, operative duration, J-CTO score, and the use of a retrograde approach can be used to predict the incidence of non-complication-related shock in patients undergoing CTO PCI procedures. These findings can be used to facilitate the preoperative evaluation of high-risk patients and corresponding strategy adjustment efforts.
ZC, YLiu, SH, YZ, YS and YLi—Data curation; ZC, WJ and HL—Formal analysis; HP, ZC—Conceptualization; ZC—Writing - original draft; JL, HP—Writing - review and editing, Resources; ALL—read and agreed to the published version of the manuscript.
Not applicable.
Not applicable.
This research was funded by National Natural Science Fund of China, grant number 81970291 and 82170344.
The authors declare no conflict of interest.
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.