
 , Giovanni Miotti 2, Tamara Ius 3, Luca de Marco 2, Massimo Robiony 1, Pier Camillo Parodi 2, Pier Paolo Panciani 4, Marco Zeppieri 5,*
, Giovanni Miotti 2, Tamara Ius 3, Luca de Marco 2, Massimo Robiony 1, Pier Camillo Parodi 2, Pier Paolo Panciani 4, Marco Zeppieri 5,*
1 Clinic of Maxillofacial Surgery, Head-Neck and NeuroScience Department University Hospital of Udine, 33100 Udine, Italy
2 Department of Plastic Surgery, University Hospital of Udine, 33100 Udine, Italy
3 Neurosurgery Unit, Head-Neck and NeuroScience Department University Hospital of Udine, 33100 Udine, Italy
4 Division of Neurosurgery, Department of Medical and Surgical Specialties, Radiological Sciences and Public Health, University of Brescia, 25123 Brescia, Italy
5 Department of Ophthalmology, University Hospital of Udine, 33100 Udine, Italy
Abstract
Background: Facial reconstruction represents one of the main challenges for surgeons. Stem cells (SC) represent the most studied solution for tissue regeneration. This approach appears particularly promising in combination with bioengineered scaffolds and 3D bioprinting. The purpose of this systematic review is to define the main domains of current application of SC therapy within contemporary clinical workflows, evaluate indications and limitations, report current knowledge in this innovative field of research, and define the landscape of evidence for such approaches. Methods: A systematic review was performed on the pertinent literature regarding stem cell-based cell therapies currently available in the reconstruction of the face. The review used the main databases for scientific literature based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Results: A total of 15 papers were selected after an independent search was performed. The two major domains for current application of stem cells in clinical practice were bone and skin categories. Conclusions: Cell therapy in the field of facial reconstruction represents a promising approach. The evidence regarding the current clinical use, however, seems to show this option to be limited. Bioengineering advances and the parallel development of 3D bioprinting technology can potentially enhance the role of stem cells in the future.
Keywords
- stem cells
- facial reconstruction
- mesenchymal stem cells (MSC)
- adipose-derived stem cells (ACS)
- 3D bioprinting
- bioengineered scaffolds
The facial area represents one of the most challenging anatomical regions to manage. This is because the reconstruction of this district must satisfy requirements of aesthetic harmony and functionality, which makes it difficult to find the most appropriate techniques to achieve this purpose. There is a growing body of literature analyzing the role of mesenchymal stem cells (MSC) in regenerative therapies. This is due to their characteristics of differentiation into important lineages under defined conditions in laboratory settings and in limited circumstances, after implantation in a living organism [1]. MSCs can be easily isolated from bone marrow and the adipose tissue stromal fraction. All tissues embody cells with properties similar to MSC within the microvasculature [2]. In addition to the differentiation characteristics, MSCs have well recognized anti-inflammatory and immuno-modulatory properties (including their high proliferation and self-renewal). These cells have been either directly applied to damaged tissue as cell therapy or inserted in appropriate scaffolds to generate new “engineered” tissue [3].
The whole area of stem cell (SC) research has been growing over the past 20 years with an increasing number of types and qualities of cell lines being studied. SC are currently used in numerous medical branches, including neurology, cardiology, hematology, as well as plastic surgery, etc. [4, 5, 6].
In 2001, MSC initially reported to be obtained from bone marrow samples, were shown to also be capable of being isolated from adipose tissue stromal fraction [7]. In the past years, fat grafts have been used as autologous filler to contour deformities, posttraumatic defects, burn injuries, scar contractures, facial atrophy and rejuvenation. Since then, research has moved to the cellular and molecular characterization of properties of implanted fat tissue. Studies performed in the last two decades have revealed that fat tissue is not only repletive, but is an active tissue with complex functional and signalling properties. Moreover, several studies have found that the addition of adipose-derived mesenchymal stem cells (AD-MSCs) to fat grafts significantly improved the viability and engraftment, resulting in better aesthetic outcomes [8]. In addition, ADSCs seem to improve the survival of fat grafts and reduce the incidence of fat necrosis [9].
Several studies have shown that this approach could stimulate and accelerate
cell differentiation and survival as well as angiogenesis, and regulate immune
responses. AD-MSCs have been shown to promote angiogenesis by secreting
pro-angiogenic factors such as vascular endothelial growth factor (VEGF), basic
fibroblast growth factor (bFGF), and hepatocyte growth factor (HGF) [10]. In
addition to their role in angiogenesis, AD-MSCs have also been shown to play a
critical role in regulating immune responses. This is due to the immunomodulatory
properties that allow them to suppress inflammatory responses and regulate immune
cell function through the secretion of anti-inflammatory cytokines including
interleukin-10 (IL-10), transforming growth factor-beta (TGF-
AD-MSCs have shown a multitude of possible applications in clinical research, ranging from liver injury, myocardium and bone reconstruction, nerve regeneration to muscle-skeletal dysfunctions or diabetes [12].
Despite such a multitude of applications and the amount of scientific evidence, clinical applications are still underreported for a variety of reasons. The main problems lie in the fact that SC therapy and research is relatively recent, and that multidisciplinary clinical trials are needed to validate this type of therapy in humans for long-term safety and efficacy. Current research in this field, however, has shown that SC therapy represents the prerequisite for future regenerative approaches, including bioprinting, scaffold fabrication, etc. The aim of this systematic review was to assess the current reports of clinical uses of SC therapy for the facial area as well as cover bioprinting applications. In this manuscript, we define the main domains of current application of SC therapy within contemporary clinical workflows, evaluate indications and limitations, report current knowledge in this innovative field of research, and define the landscape of evidence for such approaches.
This systematic review centered on the clinical applications of SC in facial regenerative surgery, reporting the evidence of the use of modern SC based therapies, as well as the various limitations. The assessment was carried out in accordance with the guidelines described in “Cochrane Handbook for Systematic Reviews of Interventions” (version 6.2.0) [13] and “Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)” statement [14]. The main search query for this study was performed according to the SPIDER structure [15] (Sample, Phenomenon of Interest, Design, Evaluation, Research type), which were synthesized with the following questions: “what are the available clinical applications of stem cells therapies in facial regeneration and in which field are they used?” (Table 1).
| S | Human subjects candidate to regenerative therapies in the facial area |
| PI | The use of stem cells for regenerative therapies in vivo |
| D | Only original and prospective studies (clinical trials, cohort studies, case series…) |
| E | Clinical outcomes, possibility of use |
| R | Qualitative or quantitative |
An extensive literature search was conducted through a comprehensive query to identify original reports describing the clinical application of stem cells in the facial area. The major databases for medical literature were searched (MEDLINE, Web of Science, Cochrane Library, Scopus, EMBASE). MEDLINE and EMBASE search was extended including the creation of search queries based on Medical Subject Headings (MeSH) terms and Emtree categories. Comprehensive queries were composed specifically for MEDLINE and EMBASE and are reported in Table 2.
| MEDLINE | EMBASE |
|---|---|
| QUERY 1 | QUERY #1 |
| (“facial” regeneration) AND (stem cell*) NOT(“review*”) | (‘facial regeneration’ OR (facial AND (‘regeneration’/exp OR regeneration))) AND (‘stem’/exp OR stem) AND cell? NOT review? |
| 106 results | |
| QUERY 2 | #2 |
| (“facial” regeneration) AND (stem cell*) AND bioprinting | #1 AND (2013:py OR 2014:py OR 2015:py OR 2016:py OR 2017:py OR 2018:py OR 2019:py OR 2020:py OR 2021:py OR 2022:py OR 2023:py) AND ‘human’/de |
| 2 results | |
| QUERY 3 (MeSH terms) | #3 - Emtree |
| ((stem cells[MeSH Terms]) AND (regeneration[MeSH Terms])) AND (face[MeSH Terms]) NOT(“review*”) | ‘bioprinting’/exp AND ‘face’/exp |
| 10 results |
Following the initial search, bibliography data in .nbib format were imported into Endnote v20.0 (Clarivate Analytics, London, UK) for duplicate removal. After this step, all articles were screened independently by two investigators (AT and GM) by evaluating titles and abstracts. In case of lack of consensus, disagreements were resolved by a third independent investigator (MZ). Following abstract selection, all full-text papers were retrieved, and carefully analyzed. All data collected were saved in an electronic spreadsheet.
According to the research enquiry formulated in the SPIDER scheme, the inclusion criteria were defined as follows: 10-year time range (2013 to 2023), only studies presenting clinically relevant applications of stem cells (including original research consisting of clinical trials), prospective cohort studies, and case series. Any study fulfilling such criteria and presenting a clinical application of stem cells within the facial area was selected.
With regards to exclusion criteria, systematic reviews, metanalyses and other non-original studies were excluded. We also excluded low evidence studies such as case reports, posters, abstracts, and conference papers. Animal research and in vitro research, as well as any kind of preclinical research without immediate translation into clinical applicability, were excluded from this study. We also excluded publications concerning laboratory procedures or conventional surgical techniques for regeneration (i.e., bone grafts and skin grafts, lipofilling and lipoaspiration). In addition, studies presenting clinical application of engineered scaffolds, but without any mention of stem cells, were not considered.
Two independent investigators (AT and GM) assessed each full text and extracted the following information: title of the paper, journal and year of publication, study design and methodology, number of patients, context of application of regenerative techniques, use of stem cells. Studies satisfying such criteria were further classified into the following categories of regeneration: bone, skin and soft tissue, nervous tissue, vascular networks, dental, or cartilage. In order to provide a more stringent and well defined assessment of this specific topic, studies regarding SC therapies in the field of ophthalmology were not considered in this analysis.
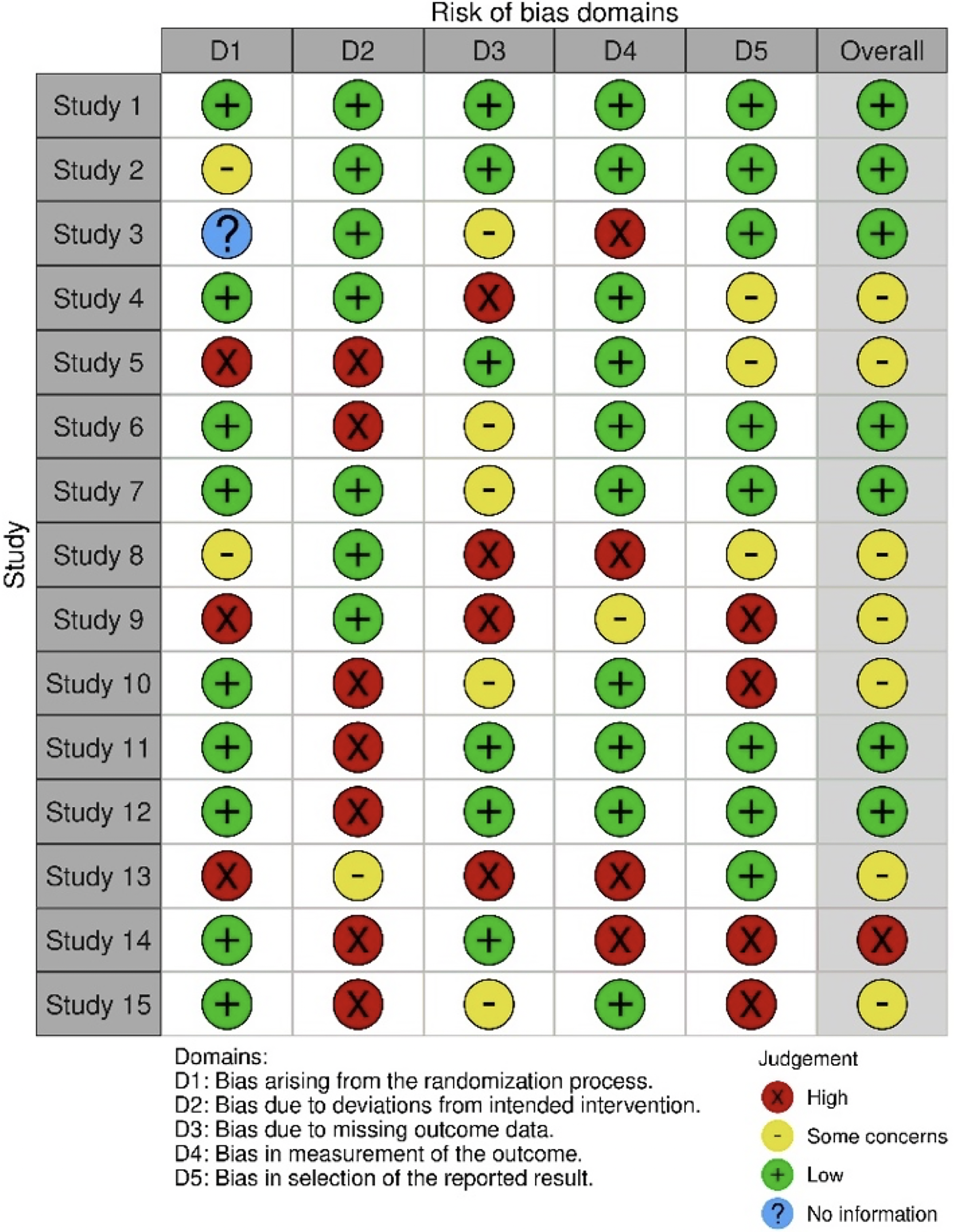
The two independent investigators separately assessed the risk of bias through the robvis visualization tool, importing an electronic spreadsheet with bias estimation formatted according to the RoB2.0 dataset model. Five main domains were analyzed to describe the risk of systematic errors that might impair the selected papers: “Bias arising from the randomization process; bias due to deviations from intended intervention; bias due to missing outcome data; bias in measurement of the outcome; bias in selection of the reported result”.
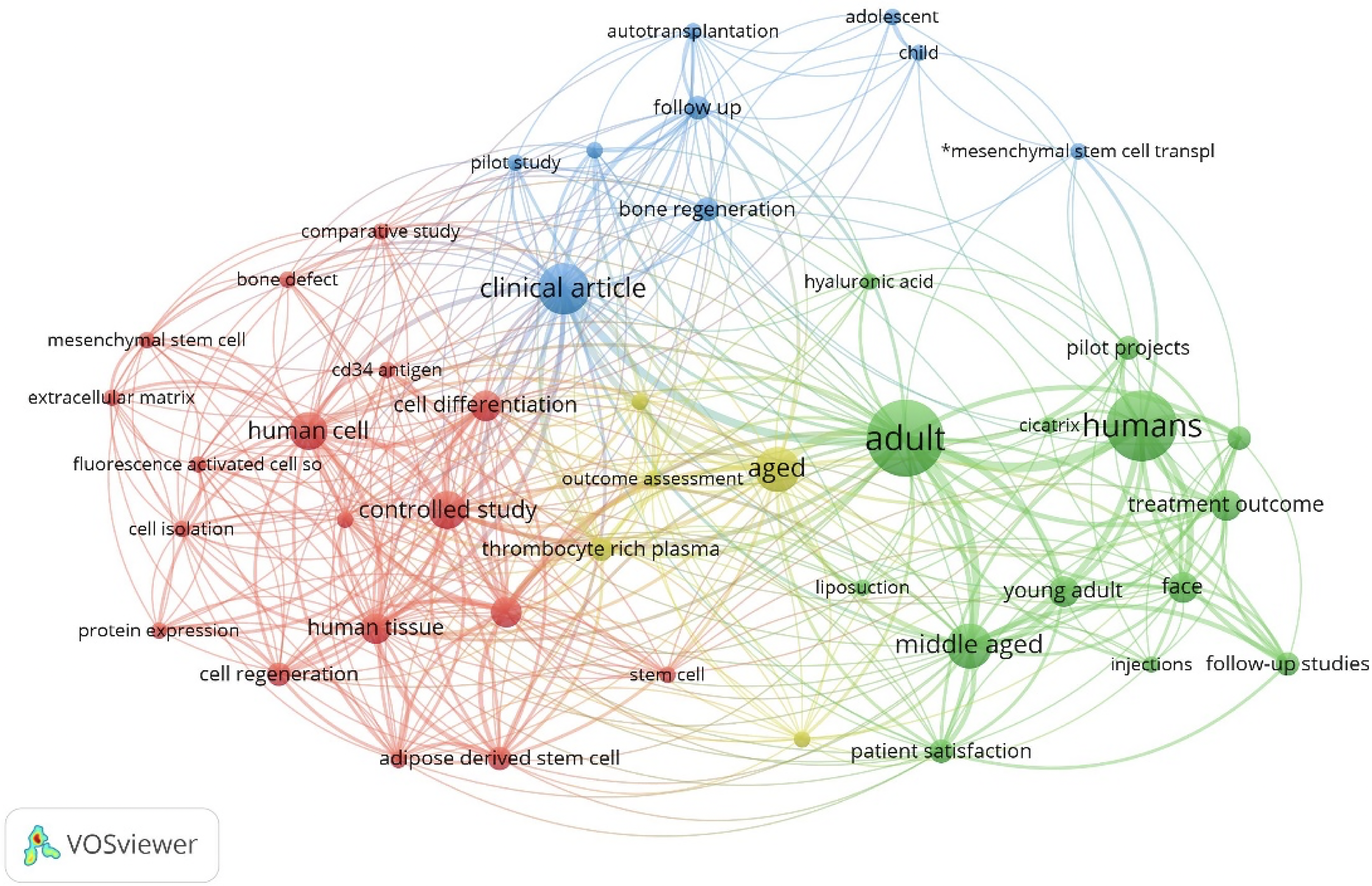
Data were collected in a Microsoft Excel spreadsheet for analysis and in an Endnote library for bibliography storage. To provide a graphical representation of connections between keywords of the selected studies, and to trace a map of relevant conceptual domains, a connection plot was generated using VOS viewer v1.6.18 (an open source software, which can generate a connection plot for bibliometric networks, based on co-occurrence of relevant keywords extracted from a collection of selected papers, Centre for Science and Technology Studies (CWTS), Leiden, Netherlands).
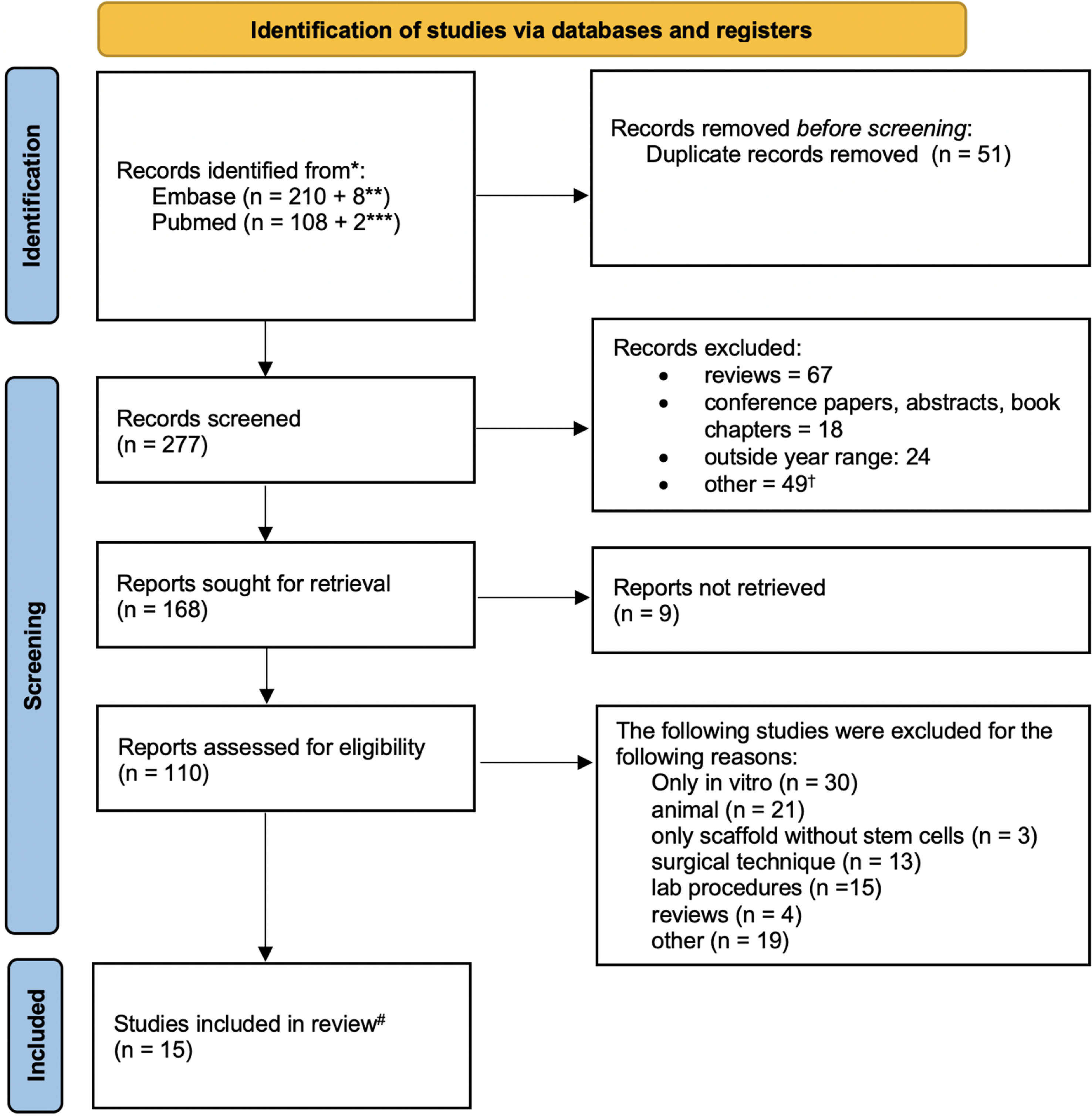
Fig. 1 depicts the PRISMA flowchart describing the process of study selection. Using a combination of keywords, MeSH and Emtree hierarchical terms, the investigators found 328 articles, which were saved in a unique Pubmed (.nbib) file, which was then imported into Endnote for to identify possible duplicates. After duplicate removal, 51 studies were deleted. The remaining 168 studies were screened by title and subsequently by abstract, which led to exclusion of 9 more studies (Cohen’s k coefficient = 0.96). Studies candidate for full-text reading were 110, of which 85 were removed according to exclusion criteria (Cohen’s k coefficient = 0.91). The remaining 25 studies underwent a further selection process by strict application of inclusion criteria that led to only 15 studies being examined in this review (Table 3).
| Authors and year | Category | Type of stem cells used | Clinical setting | Number of patients | Measured outcome | |
| 1 | (Bordin et al. 2019) | Dental | Dentapulp stem cells | Type 2 diabetic patients | 8 | Decreased stem cells clonogenesis |
| 2 | (Khojasteh et al. 2017) | Bone | Buccal fat pad derived mesenchymal stem cells | Alveolar cleft osteoplasty | 10 | Bone formation measured with CBCT |
| 3 | (Castillo-Cardiel et al. 2016) | Bone | Autologous mesenchymal stem cells from adipose tissue | Mandibular fractures | 20 | Bone quality evaluated using CT |
| 4 | (Al-Ahmady et al. 2018) | Bone | autologous bone marrow mononuclear cells combined with platelet-rich fibrin and nanohydroxyapatite | Alveolar cleft defects | 20 | Clinical and Bergland’s radiographic scale |
| 5 | (Akhlaghi et al. 2019) | Bone | Human amniotic membranes loaded with buccal fat pad-derived stem cells | Jaw bone defects | 9 | Radiomorphometric analysis with CBCT |
| 6 | (Redondo et al. 2018) (Solakoglu et al. 2019) | Bone | Autologous bone-derived mesenchymal stem cells | Oral surgery (bone regeneration) | 9 | CT density of the cyst interior |
| 7 | (Philippart et al. 2014) | Bone | Autologous mesenchymal stromal cell | Using the iliac crest as bioreactor for mesenchymal stromal cell (preosteoblasts) | 13 | Hematopoietic colony assay |
| 8 | (De Riu et al. 2018) | Cartilage | Bone marrow nucleated cells | Temporomandibular joint disorders | 30 | Clinical and MR |
| 9 | (Solakoglu et al. 2019) (Virzì et al. 2017) | Skin and soft tissue | Adipose-derived mesenchymal stem cells | Scleroderma patients | 6 | Clinical and histological |
| 10 | (Ibrahim et al. 2015) | Skin and soft tissue | Autologus bone marrow stem cells | Acne scars | 14 | Clinical (CADI score) |
| 11 | (Charles-de-Sá et al. 2020) | Skin and soft tissue | autologous adipose mesenchymal stem cells | Solar elastosis | 20 | Immunohistochemical features |
| 12 | (Gentile et al. 2014) | Skin and soft tissue | Adipose-Derived Stromal Vascular Fraction Cells | Facial scars | 10 | Clinical |
| 13 | (Svolacchia et al. 2022) | Skin and soft tissue | Autologous adipose mesenchymal stem cells | Aesthetics (antiaging) | 14 | Clinical |
| 14 | (Xu et al. 2016) | Skin and soft tissue | Autologous adipose mesenchymal stem cells | Aesthetics (antiaging) | 18 | Secretory cell pattern |
| 15 | (Rigotti et al. 2016) | Skin and soft tissue | Expanded adipose-derived stem cells | Facelift | 13 | Histological features |
MR, mitral regurgitation; CT, computed tomography; CBCT, cone beam computed tomograhpy; CADI, Cardiff acne Disability Index.
With regards to the selected manuscripts, only one study represented the field of stem cell use for the regeneration of dental elements. Likewise, only one study presented the use of stem cells for joint regeneration in the facial area. The majority of papers reported the use of stem cells of different origins to attain regeneration of bone tissue in the facial area (40%) and their application in the context of skin and soft tissue (46.7%). With regards to the clinical scenarios in which stem cells were used for regenerative therapies, all papers reporting skin and soft tissue regeneration referred to aesthetical procedures, whereas bone regeneration was usually considered in cases of alveolar cleft defects, jaw cysts and posttraumatic sequelae. With regards to the type of stem cells used, 9 papers used MSCs derived from adipose tissue and SVF; 5 papers reported the use of MSCs derived from bone marrow; 1 paper reported MSCs isolated from dental pulp.
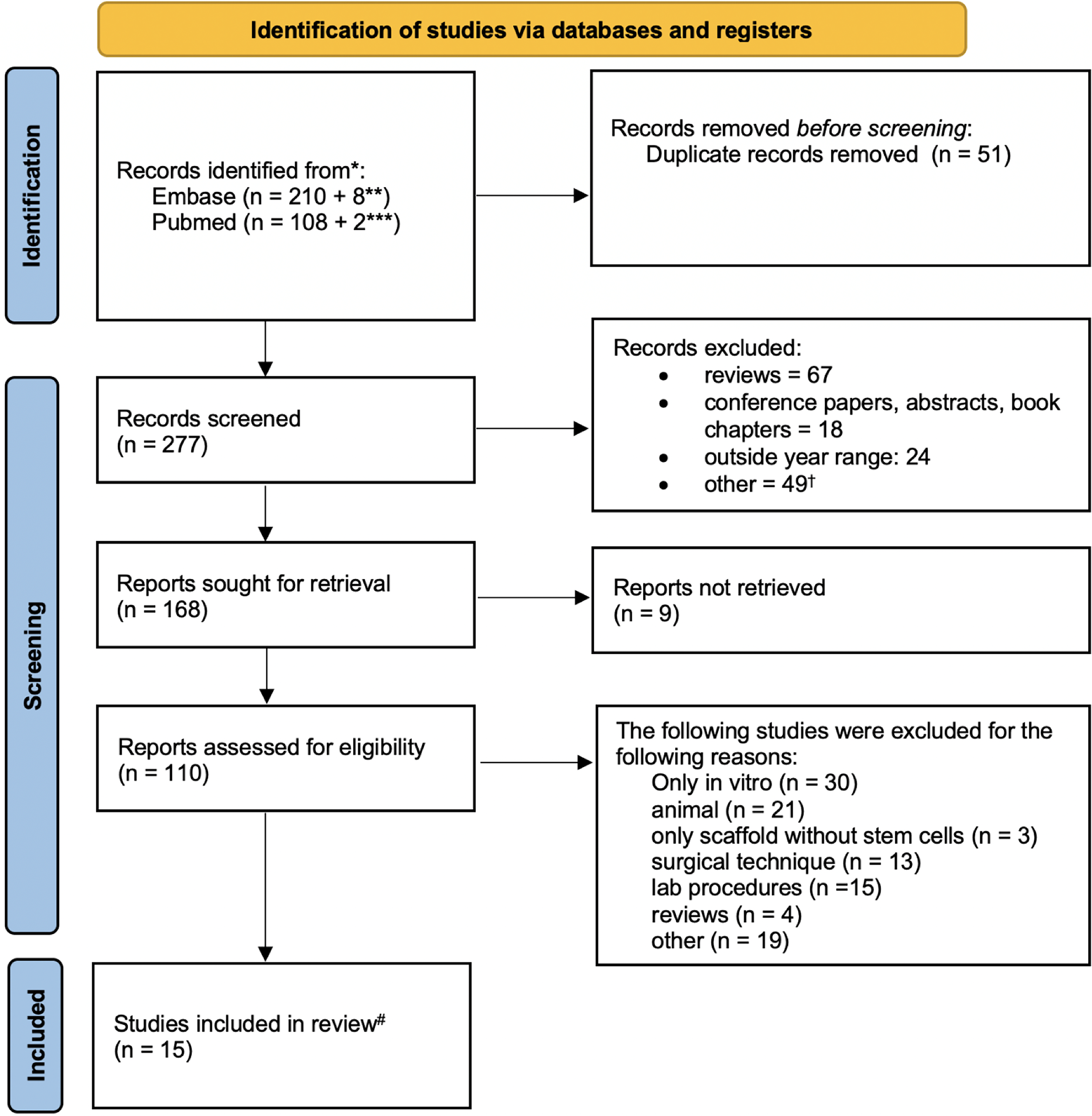 Fig. 1.
Fig. 1.PRISMA flowchart. *The following filters were applied directly to the main search query: only humans and only English, no reviews and case reports. Only studies with a clinical application in patients were eligible, animal studies and studies done in vitro were not considered. Study range was set between 2013 and 2023. **The first number refers to records identified via keywords; the second refers to records identified via MeSH. ***The first number refers to records identified via keywords; the second refers to records identified via Emtree. †Not related, only in vitro, animal, without abstract, embryology studies, surgical technique studies. Reports classified into 5 classes (bone, nerve, cartilage, dental, skin and soft tissue). # Studies subject to full data extraction.
The average number of patients sampled by selected papers was 14 individuals. Literature mapping based on the connection plot generated using VOS viewer revealed that the most connected nodes were the keywords “humans”; “adult”; “clinical article”; “aged”; “human cell” (Fig. 2). Bias assessment was conducted across all domains according to Cochrane guidelines [8] revealing a low risk of bias in 7 papers, some concerns in 7 papers, and a high risk in only one paper (Fig. 3).
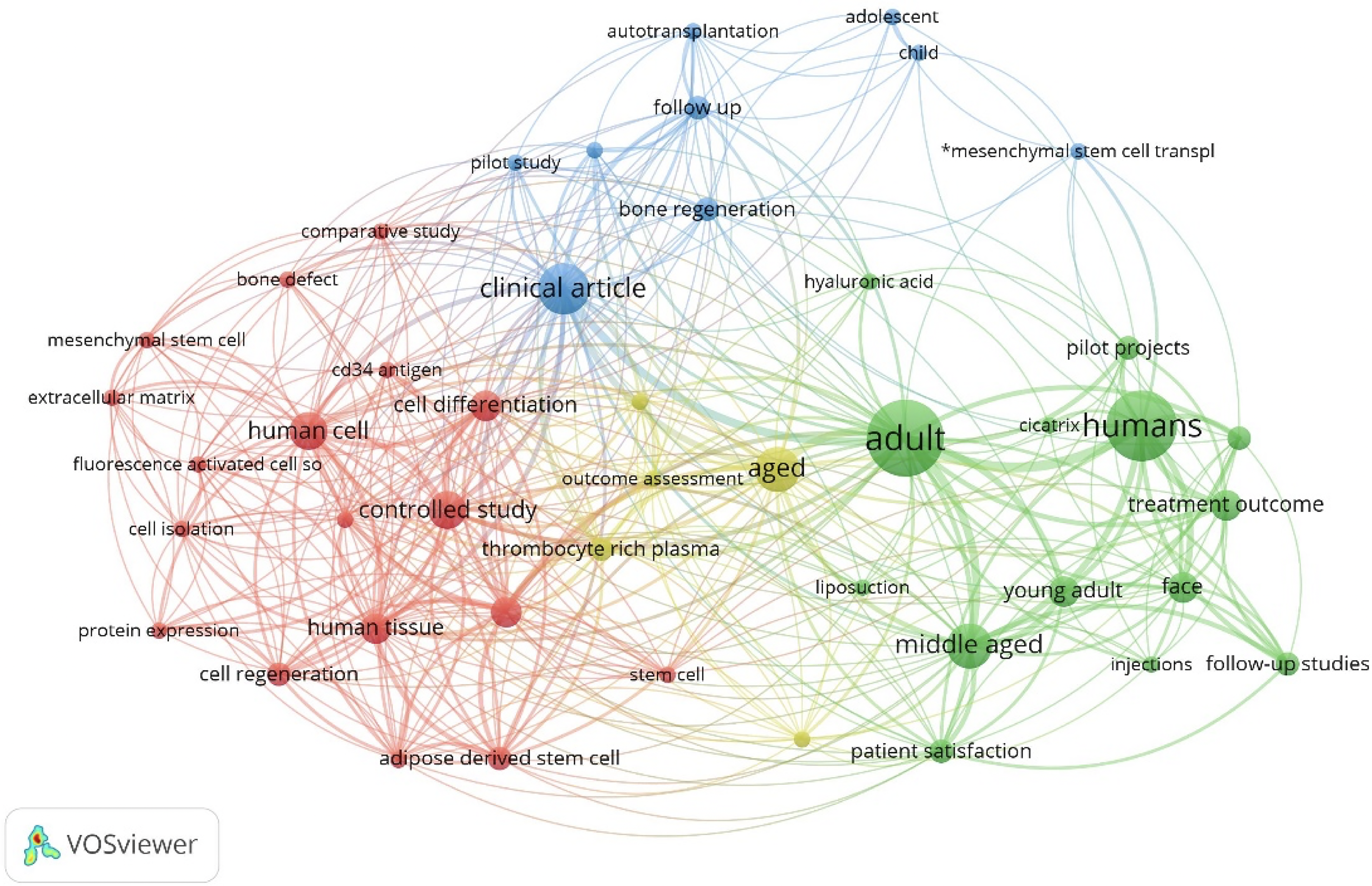 Fig. 2.
Fig. 2.Connection plot depicting literature mapping generated in VOS viewer.
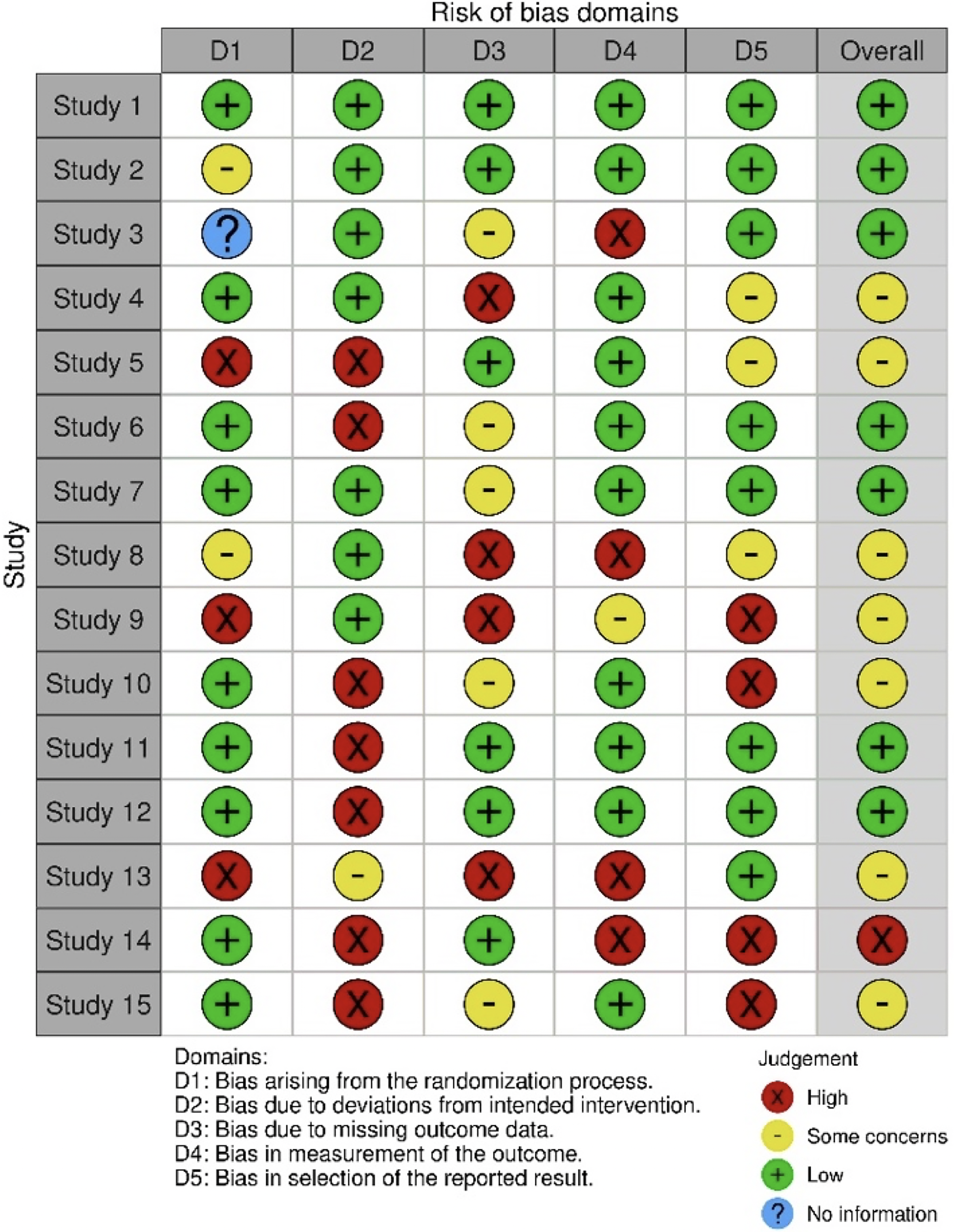 Fig. 3.
Fig. 3.Risk of bias estimation for the selected papers according to the robvis tool.
Regenerative medicine is currently one of the fastest growing fields worldwide. Cell therapies based on SC can offer potentially innovative and possible solutions in cases in which it is necessary to repair or regenerate damaged tissues by trauma or degenerative processes. The facial area is one of the most important elements of our body from an aesthetic and functional perspective. The idea of being able to regenerate and restore this region has led to the development of multiple studies based on SC therapy. The rationale for the use of SC for tissue regeneration is linked to the stimuli and mediators that they determine in damaged tissues. It is well established in the literature and in other branches of medicine, that the mechanisms underlying this type of treatment involve neo-angiogenesis, cell migration, inflammation control, and cellular/extracellular modifications.
The use of stem cells differs based on the intended application and the availability of different types of stem cells. Embryonic stem cells (ESCs), for example, have been extensively used in research due to their totipotency, but their use in clinical applications is limited due to ethical concerns and the possible hazard of immune rejection [16]. Induced pluripotent stem cells (iPSCs), consisting of reprogrammed adult cells to a pluripotent state, seem to be promising in both research and clinical applications, but their use is still in the early stages [17].
MSCs, on the other hand, have been studied extensively for their potential therapeutic applications and relative ease of harvest. Multiple clinical trials testing their safety and efficacy have been conducted [18]. What makes them highly attractive is the fact that they are easy to obtain from various sources, including bone marrow, adipose tissue, and umbilical cord tissue. The application of MSCs in the field of regenerative medicine has been widely discussed in literature. These cells are characterized by multipotency, self-renewal and high proliferative rate [4]. Moreover, they possess a paracrine activity, which is central in stimulating cell differentiation, cell replacement and anti-apoptosis [5].
AD-MSCs are one of the most commonly used types of mesenchymal stem cells in both research and clinical trials, which is due to a variety of reasons, including: their abundance and ease of isolation [19], given that adipose tissue is a rich source of stem cells, and AD-MSCs can be easily obtained through minimally invasive procedures such as lipoaspiration; versatility and differentiation potential [20], as AD-MSCs have the potential to differentiate into a variety of cell types, including bone, cartilage, fat, muscle, and nerve cells; immunomodulatory properties [21]; and, safety and low risk of rejection [22], since AD-MSCs are isolated from the patient’s own adipose tissue and the risk of rejection or adverse reactions is low.
In the last years it has become evident that AD-MSCs play an important role in cell therapy because they are an easily accessible source and maintain all the features of MSCs. One consolidated way to transfer fat for tissue regeneration and augmentation is lipofilling. AD-MSCs are often used in conjunction with lipofilling as they can be isolated from the lipoaspirate to achieve a better retention rate of the transferred fat and improved outcomes in terms of volume, contour, and texture; moreover, AD-MSCs are present in the adipose tissue and can be isolated during the liposuction process [23, 24].
The stromal vascular cell fraction (SVF) of adipose tissue and the platelet-rich
plasma (PRP) are two options capable of enhancing the activity of ASCs. However,
according to recent literature [25], SVF, which is commonly obtained by washing,
enzymatic digestion, and centrifugation, or by commercially available mechanical
methods, contains only slight amounts of AD-MSCs, as the percentage of ADSCs in
SVF ranges between
Platelet-rich plasma (PRP) is another product with regenerative potential. It is rich in growth factors and cytokines which activate cell proliferation, wound healing, matrix formation and increase blood supply [27]. Studies have shown how PRP acts both at the microenvironment level, by stimulating the growth and differentiation of adipocytes from ASCs, and at the microcirculation level, by stimulating neoangiogenesis essential for cellular nourishment. Similarly, SVF stimulates neoangiogenesis and ensures the maintenance of tissue architecture [28, 29].
Adipose tissue, however, is not the only source of MSCs. Bone marrow derived mesenchymal stem cells (BM-MSCs) have similar classification and comparable characteristics to ASCs. Although BM-MSCs and AD-MSCs have been proved to differentiate into multiple cell lineages, recent studies have suggested that AD-MSCs may have an advantage over BM-MSCs in terms of their differentiation potential. A greater adipogenic potential [30], AD-MSCs also have an improved chondrogenic potential compared to BM-MSCs [31]. The authors suggest that this may be due to the fact that AD-MSCs express higher levels of chondrogenic markers and produce more extracellular matrix than BM-MSCs.
Facial regenerative surgery has relied on a variety of techniques, including the addition of fat and bone grafts to bring volume and structure in smaller defects, and largely resorting to various options of free flap techniques to reconstruct wide tissue defects. Over the last decade, free flap techniques have been further improved by modern computer-aided technology. This has allowed tailoring of flap design to a patient-specific condition thanks to a meticulous presurgical study conducted on virtual models. A further improvement was provided by advances in 3D-printing, which enabled companies to provide customized facial implants made of a variety of materials including titanium, polyether ether ketone, and ceramics. However, regenerative therapies based on stem cells are still underreported and the evidence for their usefulness is inconclusive.
The focus of this paper was to assess the literature regarding the current adoption of stem cell therapy in clinical settings that deal with the facial area. The evaluation of a timespan of 10 years allowed us to collect only the most recent literature that covered the documented advances in this field. Overall, the results of this systematic review show that there is limited evidence for SC clinical treatment. Most of the studies still involve preclinical work in vitro or animal testing. The most frequently reported categories for stem cell application can be ascribed to bone and skin/soft tissue regeneration. Intuitively, SC treatment of functionally demanding tissue, such as nerves or muscles, as well as architecturally complex structures, like vascular networks, are still far from being implemented within real clinical scenarios. Our systematic review found no studies that reported the clinical use of SC on patients.
Concerning bone tissue regeneration, facial surgery provides a substantial number of conditions that require SC, including craniofacial malformations, pre-prosthetic surgery, and post-traumatic sequelae. An interesting study [27] reported the application of ASCs to enhance mandibular fracture healing after internal rigid fixation. Other studies tended to use the regenerative potential offered by SC to improve alveolar process regeneration, especially in cases of long-standing edentulism with jaw atrophy [32, 33]. Other interesting perspectives in bone regeneration are related to the formation of new bone in the area of maxillary clefts, which are currently treated by positioning bone grafts [34, 35]. For this area, stem cells might play an increasingly important role in the future. MSCs use was reported by De Riu et al. [36] as the first paper describing joint regeneration in temporomandibular joint. A similar experience was repeated a few years later by Sembronio, Tel and colleagues [37].
With regards to skin and soft tissue, current applications are mainly directed in aesthetic fields, especially concerning ageing signs. For instance, Charles-de-Sá et al. [6] tested mesenchymal stem cells in the treatment of photoaged skin. They treated 20 patients affected by solar elastosis with subdermal ASCs injections using analysis of skin histopathology before and after treatment. They demonstrated a significant increase of new elastic fibres and a removal of the elastotic material in the deep dermis. This study shows how transplanted ASCs appear to be able to involve all the pathways described above and to produce a long-term activation of the resident MSC pool.
Regarding MSCs use in skin regeneration, these cells have also been used in
combination with fractional CO
It is evident that many of the approaches used to harvest and seed stem cells do not involve culture in vitro, but only surgical or lab techniques to isolate cells from adipose tissue or SVF. Future research and clinical treatment will probably move towards a lab-cultured and expanded stem cell population approach. In that case, cells are obtained from a few progenitors collected from autologous sources. Laboratory manipulation of SC might be interesting for conditioning differentiation to specific cell lineagesto maximize the effect on the receiving site.
It is interesting to note that although the search query included a specific heading for bioprinting processes, no paper was found fulfilling the inclusion criteria and presenting bioprinting applications. Bioprinting, a potentially promising field in the future, is still confined to mere laboratory research and not applied in clinical settings. SC knowledge and clinical application will undoubtedly represent a possibility to facilitate the advent of 3D bioprinting. Bioprinters inks can be enriched by cultured stem cells, seeded along the coordinates of a CAD model to satisfy the computer-generated geometry, which will allow 3D print customized biological components. The simplest currently available applications of bioprinting concern the fabrication of skin grafts. In this approach, the tissue thinness does not require printing a vascular network to nourish the it. Although keratinocytes have already been 3D-printed [39, 40], there is no scientific evidence to date supporting the use of printed skin graft to replace traditionally harvested ones.
In conclusion, this systematic review aimed to map the current scenario for the clinical application of SCs in regenerative therapies in the facial area. Report numbers are still limiting. The majority of research is still performed in vitro or in animal testing. Clinical applications tend to consider surgically harvested or laboratory processed tissue containing stem cells, not cultivating progenitors and controlling the differentiation. It is foreseeable that 3D bioprinting will provide the technological solution for the widespread adoption of stem cells within bioinks. Technological innovations could potentially allow for the manufacturing of patient-specific biological parts. This can start from autologous progenitors for specific defects in the facial area, which avoids flap harvesting and other invasive approaches. The review focused mostly on preliminary work done in vitro and on animal studies, which represent the fundamentals of SC-based regenerative approaches in the facial area.
Data and Materials pertinent to the study are all provided in the manuscript.
AT did the research, wrote the paper, prepared the figures and provided the final approval of the version of the article; GM did some of the research, wrote portions of the paper, and provided the final approval of the version of the article; TI, LM, MR, PCP, PPP, and MZ assisted in the research, edited the paper, and provided the final approval of the version of the article; MZ assisted in the conception and design of the study, writing, outline, final approval of the version of the article to be published and completed the English and scientific editing (a native English speaking MD, Ph.D.). All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.