

1 Department of Cardiac Surgical Care Unit, Affiliated Hospital of Qingdao University, 266003 Qingdao, Shandong, China
2 Department of Thoracic Surgery, Affiliated Hospital of Qingdao University, 266003 Qingdao, Shandong, China
Abstract
Background: There are six widely used equations to calculate the
estimated glomerular filtration rate (eGFR) of patients. We aimed to assess the
predictive power of preoperative eGFR calculated by these equations for the
occurrence of postoperative acute kidney injury (AKI). Methods: Patients
who underwent isolated coronary surgery from January 2016 to January 2021 were
continuously enrolled. Serum creatinine and cystatin C used to calculate eGFR
were both measured within 1 week before surgery. The eGFR was calculated using
six equations: Cockcroft Gault (CG) equation, Chinese abbreviated modification of
diet in renal disease (MDRD) equation, chronic kidney disease-epidemiology
(CKD-EPI) equation, and full age spectrum (FAS) equation. Postoperative AKI was
diagnosed by Kidney Disease Improving Global Outcomes criteria (KDIGO)
(① urine volume
Keywords
- estimated glomerular filtration rate
- chronic kidney disease-epidemiology equation
- full age spectrum equation
- acute kidney injury
- coronary artery bypass grafting
Postoperative acute kidney injury (AKI) is a common complication after heart surgery, with an incidence of between 5% and 42%. Postoperative AKI is associated with a variety of adverse events, such as prolonged intensive care unit (ICU) stay and increased mortality [1, 2]. The development of AKI is influenced by many clinical factors, such as advanced age, congestive heart failure, hyperglycemia, pre-existing kidney disease, and emergency surgery [1, 2]. Therefore, adequate assessment of preoperative renal function is particularly important for identifying high-risk patients and predicting postoperative AKI.
Estimated glomerular filtration rate (eGFR) is a convenient tool for assessing renal function in patients. In addition to the commonly used Cockcroft Gault (CG) equation [3], the modification of diet in renal disease (MDRD) equation [4], and chronic kidney disease-epidemiology (CKD-EPI) equation [5], there are also the Schwartz equation [6] for children and the Berlin Initiative Study (BIS) equation [7] for people over 70 years of age. Recently, Hans Pottel [8, 9] proposed a full age spectrum (FAS) equation that could cover all ages. Studies have shown that the FAS equation is also suitable for the Chinese general population [10, 11, 12]. Besides assessing renal function, the above-mentioned equations are also widely used to assess the risk of death, AKI, and other adverse events [13, 14, 15, 16, 17].
Xiaoyun Wu et al. [17] study demonstrated that the CKD-EPI equation, which was based on serum creatinine, has a better predictive power than the CG and MDRD equations on the incidence of postoperative AKI in on-pump heart surgery. However, their study did not include eGFR calculated by cystatin C. Cystatin C, a 13-kDa cysteine proteinase inhibitor protein, is freely filtered by the kidney with near-complete reabsorption and catabolism in the proximal tubule and no significant urinary excretion. Serum cystatin C is much less affected by patient characteristics such as gender, age, nutritional status, and sarcopenia than serum creatinine [18, 19, 20]. Therefore, equations developed based on cystatin may have a wide range of applications. It is therefore necessary to evaluate the prediction value of eGFR calculated by cystatin C.
With the improvement of surgical techniques, more and more patients are
receiving off-pump coronary artery bypass grafting. Since the conclusions of the
previous study were based on patients who underwent on-pump surgery [17, 21], it
is necessary to explore the predictive power of each of the eGFR equations after
off-pump surgery. The aim of our study was to compare the predictive power of
preoperative eGFR calculated by each equation (including CG, MDRD,
CKD-EPI
This study was a single center, retrospective case-control study, of consecutively reviewed patients who underwent isolated coronary artery bypass grafting (CABG) at the Affiliated Hospital of Qingdao University. The study protocol was approved by the Ethics Committee of the Affiliated Hospital of Qingdao University, and informed consent was waived. The clinical data of all patients were derived from the medical scientific research data system (YIDUYUN System) of the Affiliated Hospital of Qingdao University, and the data did not contain privacy information. Laboratory samples were collected 7 days prior to surgery. Patients who met the following conditions were included: ① underwent isolated of-pump CABG in our cardiac center from January 1, 2016, to January 1, 2021; ② patients were older than 18 years. Patients with the following characteristics were excluded: ① patients with ventricular arrhythmias or cardiogenic shock before surgery (n = 11); ② underwent minimally invasive surgery (n = 41); ③ underwent cardiopulmonary bypass (n = 120); ④ emergency surgery (n = 23); ⑤ body mass index less than 18.5 (n = 11); ⑥ patients with missing data (n = 328). To avoid the effects of sarcopenia on serum creatinine levels, we excluded patients with a lower BMI. The patient enrollment process is shown in Fig. 1.
 Fig. 1.
Fig. 1.Process of patient enrollment. CABG, coronary artery bypass grafting; KDIGO, Kidney Disease Improving Global Outcomes; AKI, acute kidney injury.
Six equations [3, 4, 5, 8, 9] are shown in Table 1. Postoperative AKI was diagnosed
according to Kidney Disease Improving Global Outcomes (KDIGO) criteria
(① urine volume
| Names | Levels | Equations |
| Cockcroft Gault | (140 – Age) × Weight / (72 × Cr) × 0.85 (if female) | |
| MDRD | 175 × Cr^ – 1.234 × Age^ – 0.179 × 0.79 (if female) | |
| CKD-EPI |
||
| Female Cr |
144 × (Cr/0.7)^ – 0.329 × 0.993^Age | |
| Female Cr |
144 × (Cr/0.7)^ – 1.209 × 0.993^Age | |
| Male Cr |
141 × (Cr/0.9)^ – 0.411 × 0.993^Age | |
| Male Cr |
141 × (Cr/0.9)^ – 1.209 × 0.993^Age | |
| CKD-EPI |
||
| Cys |
133 × (Cys/0.8)^ – 0.499 × 0.996^Age × 0.932 (if female) | |
| Cys |
133 × (Cys/0.8)^ – 1.328 × 0.996^Age × 0.932 (if female) | |
| FAS |
||
| 2 |
107.3/(Cr/Q1) | |
| Age |
107.3/(Cr/Q1) × 0.988^(Age – 40) | |
| FAS |
||
| 2 |
107.3/(Cys/Q2) | |
| Age |
107.3/(Cys/Q2) × 0.988^(Age – 40) |
Note: Weight (Kg); Cr, creatinine (mg/dL), Cys, cystatin C (mg/L); Q1 = 0.70
(mg/dL) for females and Q1 = 0.90 (mg/dL) for males; Q2 = 0.82 mg/L for ages
Oxygen inhalation and breathing training were given to all patients after admission. Anti-platelet therapy, myocardial nutrition (such as CoenzyMe Q10, Trimetazidine and Potassium Magnesium Aspartate Tablets), and other treatments were given according to the patient’s condition. All patients underwent a sternotomy, and received heparin (1 mg/kg). During surgery, the left anterior descending artery was grafted first, followed by the diagonal artery or obtuse marginal artery, and finally the posterior descending artery and the right posterior lateral artery.
All continuous variables were described by the mean
In the total cohort of 1428 patients, the mean age was 63.7 years, and 74.4%
were male. The prevalence of hypertension, diabetes and shrunken pore syndrome
was 72.8%, 39.5% and 13.3%, respectively. In this cohort, 25.5% (319/1428) of
patients developed postoperative AKI. The mean eGFR for the entire study are CG
(84.0
| Variables | Overall | Non-AKI | AKI | p value |
| n = 1428 | n = 1109 | n = 319 | ||
| Age (year, mean |
63.7 (8.3) | 63.0 (8.2) | 66.2 (7.9) | |
| Sex (male, %) | 1063 (74.4) | 828 (74.7) | 235 (73.7) | 0.775 |
| High (cm, mean |
167.0 (7.5) | 167.1 (7.3) | 166.4 (7.8) | 0.119 |
| Weight (Kg, mean |
71.8 (11.1) | 71.9 (11.2) | 71.2 (10.5) | 0.291 |
| Body mass index (Kg/m |
25.7 (3.1) | 25.7 (3.2) | 25.7 (3.1) | 0.949 |
| Smoking (%) | 631 (44.2) | 489 (44.1) | 142 (44.5) | 0.945 |
| Acute coronary syndrome (%) | 221 (15.5) | 172 (15.5) | 49 (15.4) | 1 |
| Heart failure (%) | 57 (4.0) | 34 (3.1) | 23 (7.2) | 0.002 |
| Coronary stent (%) | 182 (12.7) | 141 (12.7) | 41 (12.9) | 1 |
| Hypertensions (%) | 1040 (72.8) | 787 (71.0) | 253 (79.3) | 0.004 |
| Diabetes mellitus (%) | 564 (39.5) | 431 (38.9) | 133 (41.7) | 0.398 |
| Stroke (%) | 222 (15.5) | 166 (15.0) | 56 (17.6) | 0.256 |
| Peripheral vascular disease (%) | 42 (2.9) | 32 (2.9) | 10 (3.1) | 0.851 |
| Chronic obstructive pulmonary disease (%) | 28 (2.0) | 21 (1.9) | 7 (2.2) | 0.818 |
| Chronic kidney disease (%) | 13 (0.9) | 7 (0.6) | 6 (1.9) | 0.049 |
| Shrunken pore syndrome (%) | 190 (13.3) | 113 (10.2) | 77 (24.1) | |
| Creatinine (mg/L, mean |
79.9 (36.1) | 75.4 (18.8) | 95.6 (65.5) | |
| Cystatin C (mg/L, mean |
1.0 (0.4) | 0.9 (0.2) | 1.3 (0.6) | |
| Triglyceride (mmol/L, mean |
1.7 (1.3) | 1.7 (1.2) | 1.8 (1.6) | 0.266 |
| Cholesterol (mmol/L, mean |
4.2 (1.3) | 4.3 (1.3) | 4.1 (1.4) | 0.016 |
| High-density lipoproteins (mmol/L, mean |
1.1 (0.3) | 1.2 (0.3) | 1.1 (0.3) | 0.014 |
| Low-density lipoproteins (mmol/L, mean |
2.5 (0.9) | 2.6 (1.0) | 2.5 (0.9) | 0.32 |
| Lipoprotein a (mg/L, median IQR) | 208.4 [110.0, 406.1] | 208.2 [110.0, 402.0] | 211.0 [110.7, 427.0] | 0.849 |
| Apolipoprotein AI (g/L, mean |
1.2 (0.2) | 1.2 (0.2) | 1.2 (0.2) | 0.094 |
| Apolipoprotein B (g/L, mean |
0.9 (0.3) | 0.9 (0.3) | 0.8 (0.3) | 0.226 |
| Fasting blood glucose (mmol/L, mean |
6.3 (2.5) | 6.2 (2.4) | 6.5 (2.7) | 0.144 |
| Uric acid (µmol/L, mean |
335.8 (92.8) | 330.8 (87.5) | 353.4 (107.5) | |
| Hemoglobin (g/L, mean |
131.7 (17.4) | 132.5 (17.0) | 129.0 (18.3) | 0.002 |
| Platelet (10 |
219.2 (63.0) | 218.8 (63.3) | 220.5 (61.9) | 0.667 |
| High-sensitivity troponin I (ng/mL, median IQR) | 0.014 (0.008, 0.029) | 0.014 (0.008, 0.027) | 0.017 (0.010, 0.041) | |
| Ejection Fraction (%, mean |
57.5 (7.1) | 57.9 (6.9) | 56.2 (7.5) | |
| Angiotensin converting enzyme inhibitor (%) | 271 (19.0) | 203 (18.3) | 68 (21.3) | 0.259 |
| Angiotensin receptor blocker (%) | 494 (34.6) | 378 (34.1) | 116 (36.4) | 0.492 |
| Beta receptor blocker (%) | 1044 (73.1) | 805 (72.6) | 239 (74.9) | 0.449 |
| Calcium channel blocker (%) | 521 (36.5) | 389 (35.1) | 132 (41.4) | 0.046 |
| Statin (%) | 1134 (79.4) | 893 (80.5) | 241 (75.5) | 0.063 |
| Digoxin (%) | 65 (4.6) | 47 (4.2) | 18 (5.6) | 0.288 |
| Diuretics (%) | 525 (36.8) | 368 (33.2) | 157 (49.2) | |
| Surgical time (min, mean |
261.5 (78.4) | 261.3 (79.9) | 262.2 (73.1) | 0.86 |
| Left internal thoracic artery (%) | 1290 (90.3) | 1004 (90.5) | 286 (89.7) | 0.719 |
| Incomplete revascularization (%) | 34 (2.4) | 25 (2.3) | 9 (2.8) | 0.535 |
| eGFR (mL/min/1.73 m |
||||
| Cockcroft Gault | 84.0 (22.7) | 86.4 (21.3) | 75.5 (25.6) | |
| MDRD | 95.5 (26.1) | 98.1 (24.0) | 86.3 (30.7) | |
| CKD-EPI |
84.9 (18.7) | 88.7 (15.9) | 71.8 (21.7) | |
| CKD-EPI |
80.0 (21.7) | 84.4 (19.4) | 64.8 (22.3) | |
| FAS |
82.9 (23.7) | 85.7 (22.8) | 72.9 (24.3) | |
| FAS |
72.6 (18.4) | 76.2 (17.1) | 60.2 (17.3) |
AKI, acute kidney injury; SD, standard deviation; eGFR, estimated glomerular filtration rate; MDRD, modification of diet in renal disease; CKD-EPI, chronic kidney disease-epidemiology; FAS, full age spectrum; IQR, inter-quartile range.
Patients with AKI were more likely to be older, and had an increased incidence of heart failure, hypertension, and chronic kidney disease. Patients in the AKI group were more likely to have received diuretics, to have a lower left ventricular ejection fraction and eGFR. The AKI group had a higher prevalence of SPS than the non-AKI group. The distribution of eGFR levels in AKI and non-AKI groups are shown in Fig. 2. These values were calculated by six equations.
 Fig. 2.
Fig. 2.The distribution of eGFR levels in AKI and non-AKI groups. AKI, acute kidney injury; eGFR, estimated glomerular filtration rate; MDRD, modification of diet in renal disease; CKD-EPI, chronic kidney disease-epidemiology; FAS, full age spectrum; CG, Cockcroft Gault.
The odds ratios (ORs) and 95% confidence interval (CI) of each eGFRs are presented in Table 3. The results of
Univariate logistic regression analyses indicated that all eGFR equations were
significantly correlated with postoperative AKI (all p
| Equations | Model 1 | Model 2 | Model 3 | |||
| OR (95% CI) | p value | OR (95% CI) | p value | OR (95% CI) | p value | |
| Cockcroft Gault | 0.979 (0.973–0.984) | 0.982 (0.976–0.988) | 0.983 (0.977–0.99) | |||
| MDRD | 0.982 (0.977–0.987) | 0.983 (0.978–0.988) | 0.983 (0.978–0.989) | |||
| CKD-EPI |
0.969 (0.962–0.975) | 0.971 (0.964–0.978) | 0.97 (0.962–0.978) | |||
| CKD-EPI |
0.953 (0.947–0.96) | 0.955 (0.948–0.962) | 0.955 (0.946–0.963) | |||
| FAS |
0.975 (0.969–0.981) | 0.978 (0.972–0.984) | 0.978 (0.971–0.985) | |||
| FAS |
0.94 (0.931–0.949) | 0.94 (0.931–0.95) | 0.941 (0.93–0.953) | |||
MDRD, modification of diet in renal disease; CKD-EPI, chronic kidney disease-epidemiology; FAS, full age spectrum; OR, odds ratio; CI, confidence interval.
 Fig. 3.
Fig. 3.The correlation between OR and eGFR levels. CKD-EPI, chronic kidney disease-epidemiology; FAS, full age spectrum; OR, odds ratio; eGFR, estimated glomerular filtration rate; CI, confidence interval.
ROC analysis and subgroup analysis of six eGFR equations are demonstrated in
Table 4. The ROC curve of the total cohort is shown in Fig. 4. In the ability to
predict postoperative AKI, FAS
| Equations | AUC | 95% CI | p value | |
| Total cohort | n = 1428 | |||
| Cockcroft Gault | 0.621 | 0.584–0.657 | ||
| MDRD | 0.614 | 0.576–0.652 | ||
| CKD-EPI |
0.643 | 0.608–0.678 | ||
| CKD-EPI |
0.739 | 0.708–0.771 | ||
| FAS |
0.643 | 0.607–0.678 | ||
| FAS |
0.744 | 0.713–0.774 | ||
| Male | n = 1063 | |||
| Cockcroft Gault | 0.638 | 0.596–0.68 | ||
| MDRD | 0.629 | 0.585–0.673 | ||
| CKD-EPI |
0.661 | 0.62–0.701 | ||
| CKD-EPI |
0.742 | 0.705–0.779 | ||
| FAS |
0.66 | 0.619–0.701 | ||
| FAS |
0.752 | 0.716–0.788 | ||
| Female | n = 365 | |||
| Cockcroft Gault | 0.575 | 0.501–0.649 | 0.037 | |
| MDRD | 0.569 | 0.495–0.642 | 0.057 | |
| CKD-EPI |
0.588 | 0.517–0.659 | 0.014 | |
| CKD-EPI |
0.728 | 0.668–0.787 | ||
| FAS |
0.591 | 0.518–0.663 | 0.012 | |
| FAS |
0.72 | 0.661–0.78 | ||
| Age |
n = 698 | |||
| Cockcroft Gault | 0.565 | 0.517–0.613 | 0.006 | |
| MDRD | 0.568 | 0.519–0.618 | 0.004 | |
| CKD-EPI |
0.577 | 0.528–0.625 | 0.001 | |
| CKD-EPI |
0.674 | 0.628–0.72 | ||
| FAS |
0.578 | 0.53–0.627 | 0.001 | |
| FAS |
0.675 | 0.629–0.72 | ||
| Age |
n = 730 | |||
| Cockcroft Gault | 0.627 | 0.565–0.69 | ||
| MDRD | 0.675 | 0.616–0.734 | ||
| CKD-EPI |
0.683 | 0.627–0.74 | ||
| CKD-EPI |
0.784 | 0.738–0.83 | ||
| FAS |
0.68 | 0.623–0.737 | ||
| FAS |
0.783 | 0.737–0.83 |
ROC, receiver operating characteristic; AUC, area under the receiver operating characteristic curve; CI, confidence interval; MDRD, modification of diet in renal disease; CKD-EPI, chronic kidney disease-epidemiology; FAS, full age spectrum.
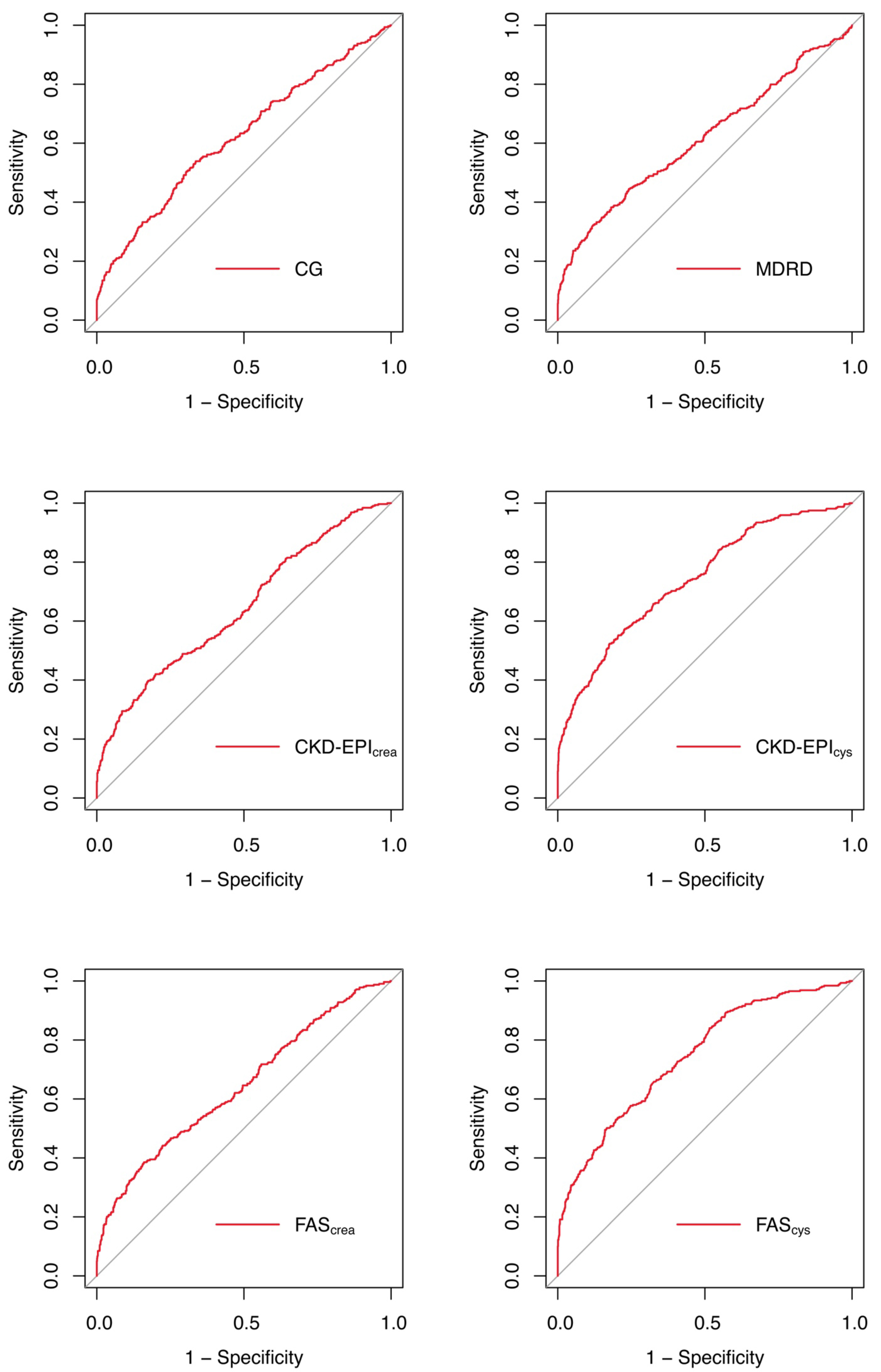 Fig. 4.
Fig. 4.ROC curves of each equations in the total cohort. ROC, receiver operating characteristic; CG, Cockcroft Gault; MDRD, modification of diet in renal disease; CKD-EPI, chronic kidney disease-epidemiology; FAS, full age spectrum.
In the age and sex subgroups, we found that FAS
The calibration curves showed that there is a good agreement between the
predicted probability by two equations (FAS
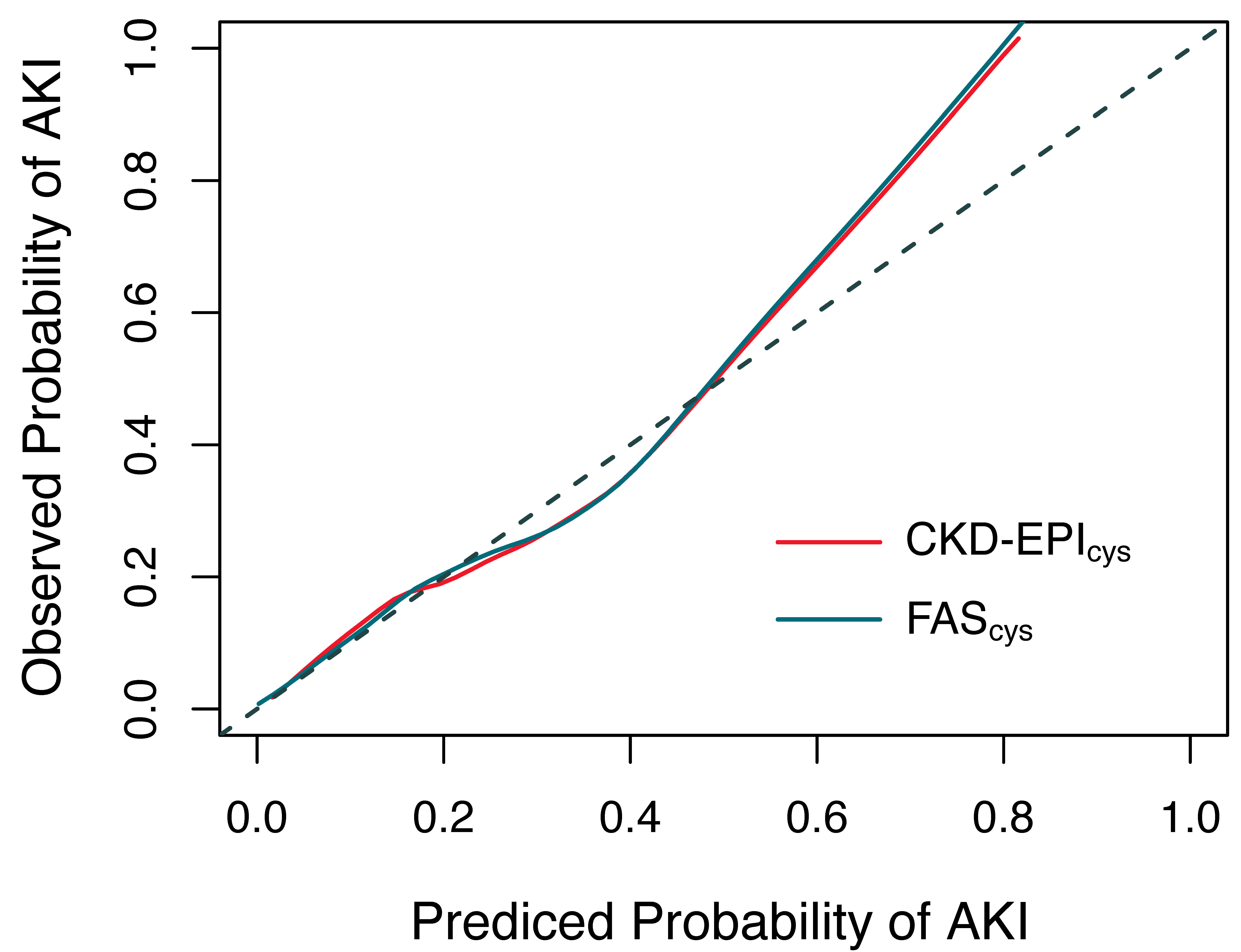 Fig. 5.
Fig. 5.The calibration curves of FAS
This study found that preoperative eGFRs calculated based on cystatin C have more accurate predictive power for AKI after off-pump CABG. Moreover, in patients younger than 65 years, all equations had better performance than patients over 65 years. Compared with each eGFR, we also found that the average value of eGFR calculated by the FAS equation based on cystatin C was the lowest, while the average value of the MDRD equation was the highest. The predictive power of preoperative eGFR based on cystatin C was better than creatinine. This phenomenon may be related to the following two reasons: ① cystatin C is better than creatinine in evaluating renal function. It was much less affected by patient characteristics, such as gender, age, body size and composition, and nutritional status [18, 19, 20]. ② Due to SPS, eGFRs calculated by the creatinine could be overestimated. In this study, the incidence of SPS was significantly higher in the AKI group than in the non-AKI group. Therefore, we suggest using equations based on cystatin C to calculate eGFR [22, 23].
Xiaoyun Wu et al. [17] compared the predictive value of eGFRs after cardiac surgery. The main conclusion of their paper is that the CKD-EPI equation has a better predictive effect than the CG and MDRD equations. Additionally, the body surface area adjusted CG equation performed better in their cohort. In the comparison of the predictive power of CKD-EPI, CG, and MDRD equations, the results of our study are consistent with their conclusions. It is important to note that the decrease in perfusion pressure during on-pump surgery can alter renal function. Hence, the occurrence of postoperative AKI, in their study, is more than 2-fold of our cohort. Differences were also seen in sample size, average age, and the incidence of males/females. Wu’s study also explored the predictive effect of eGFR within 2 days after surgery. Patients were being treated in the cardiac intensive care unit at this time. Hence, AKI can be directly and conveniently diagnosed based on urine volume or creatinine levels. Therefore, it is not necessary to calculate eGFR to predict AKI alone. In summary, Wu’s conclusion cannot be directly applied to all cardiac surgery patients.
In the subgroup analysis, we also found that the predictive effect of the eGFR equations was enhanced in patients less than 65 years. This phenomenon may be related to the patient’s condition when the equation was established. Younger patients have a lower incidence of heart failure, atrial fibrillation, and other co-morbidities. Therefore, renal function may have a greater impact on postoperative AKI in younger patients. In other studies, the equations were more accuracy for the diagnosis and stratification in patients with advanced kidney disease or older age [24, 25]. But none of the patients in these studies underwent cardiac surgery.
Notably, in our study, eGFR based cystatin C had better predictive power in the diabetic population. Studies have also demonstrated that serum cystatin C has better predictive power for adverse outcomes in diabetic patients. Kati Jarvela et al.’s [26] study prospectively enrolled 200 patients who underwent elective CABG, and measured their serum creatinine and cystatin C levels. Study point out that cystatin C and cystatin C-based estimation of GFR may be useful and more sensitive than creatinine in detecting mild acute renal insufficiency in diabetic patients. In addition, Caroline Pereira Domingueti and colleagues [27] also demonstrated that cystatin C-based equations present the best accuracy to detect macroalbuminuria in Cystatin type 1 diabetes mellitus patients. This phenomenon may be related to the fact that diabetes not only increases serum cystatin levels, but also significantly increases the risk of postoperative AKI [26, 28].
By comparing each equations, we identified two equations that were suitable for preoperative assessment of renal function. Accurate assessment of preoperative renal function not only could predict the risk of postoperative AKI, but also be used to guide preoperative clinical strategy to avoid AKI. In addition, AKI is influenced by multiple perioperative risk factors, which may explain the limited predictive power of eGFR. Despite improvement in bias compared with equations based on creatinine, some studies suggest that a few biases remain in equations based on cystatin C, especially in patients who are chronically ill. Among them, measured GFR may be necessary for the accurate assessment of GFR in these populations [20, 29]. On the other hand, some studies found that further modification and the addition of the Chinese racial factor could improve the predictive and stratification ability of preoperative eGFR [12, 30]. Hence, further research is needed.
This study was a single-center, retrospective, cohort study. Therefore, various biases in retrospective studies also exist in this study. Due to the limitations of the study design, measurement of GFR, a gold standard, could not be performed, so the results need to be further verified in large-scale, multi-center prospective studies.
Preoperative eGFR calculated by FAS
The data analyzed in this study are available from the corresponding author or first author upon reasonable request.
WQ and JT were responsible for the conception and design of the work. JT and CZ were responsible for data collection and article drafting. WQ, JT, WH were responsible for data analysis and substantial revision. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The Ethics Committee of the Affiliated Hospital of Qingdao University approved the study [QYFY WZLL 28075]. All procedures performed in this study involving human participants were by the Declaration of Helsinki. The need for consent was waived by the Ethics Committee of the Affiliated Hospital of Qingdao University due to the retrospective nature of the study. Patient data confidentiality was protected.
Thanks to Dr. Yangyan Wei from Wuhan Asia General Hospital for his help in study design and statistics.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.