

 , Jeswant Dillon 3, Mohamed Ezani Md Taib 3, Alwi Mohamed Yunus 3, Abdul Rais Sanusi 3, Mohd Nazeri Nordin 3, Julian A. Smith 4,5
, Jeswant Dillon 3, Mohamed Ezani Md Taib 3, Alwi Mohamed Yunus 3, Abdul Rais Sanusi 3, Mohd Nazeri Nordin 3, Julian A. Smith 4,51 Jeffrey Cheah School of Medicine & Health Sciences, Monash University Malaysia, 47500 Subang Jaya, Selangor, Malaysia
2 Victorian Heart Institute, Monash University, 3168 Melbourne, Australia
3 Department of Cardiothoracic Surgery, National Heart Institute, 50400 Kuala Lumpur, Malaysia
4 Department of Surgery, School of Clinical Sciences at Monash Health, Monash University, 3168 Melbourne, Australia
5 Department of Cardiothoracic Surgery, Monash Health, 3168 Melbourne, Australia
Academic Editors: Giuseppe Santarpino and Giuseppe Nasso
Abstract
Objective: The objective of this study is to analyse the incidence of
postoperative atrial fibrillation (POAF), demography, post-operative outcomes
including morbidity and mortality, length of Cardiac Intensive Care Unit (CICU)
stay, High Dependency Unit (HDU) stay, and total hospital stay in patients
undergoing coronary bypass grafting (CABG) at Institut Jantung Negana (IJN).
Methods: We conducted a prospective, randomised, controlled trial. We
supplied the treatment group with Tocovid capsules and the control group with
placebo containing palm superolein. Results: Since January 2019, we have
recruited the target population of 250 patients. However, the result is still
blinded as we are still analysing blood samples for tocotrienol levels. 89.2% of
patients completed the study with a 3.6% mortality and a 7.6% attrition rate.
35.2% of the patients developed POAF, the mean time being 46.06
Keywords
- Tocovid
- postoperative atrial fibrillation (POAF)
- CABG
- CICU stay
- total hospital stay
- morbidity
- mortality
One of the commonest complications of cardiac surgery is postoperative atrial fibrillation (POAF). It occurs in about 20% to 40% [1] of patients after isolated coronary bypass grafting (CABG) and more often after combined CABG and valve surgery [2]. In an earlier retrospective study [3], we observed a prolonged Cardiac Intensive Care Unit (CICU) stay, High Dependency Unit (HDU) stay and total hospital stay among these patients, with a projected increase in resource utilisation. This was accompanied by a statistically significant increase in the incidence of stroke and death [3].
There is no single unifying mechanism in the development of POAF. It is generally agreed that both a susceptible substrate and a trigger factor are needed to initiate POAF [4, 5]. While multiple factors may initiate POAF, current data suggests that the postoperative inflammatory state after CABG plays a significant role in initiating POAF [6, 7]. More precisely, it is the shed mediastinal blood that serves as a notable source for this inflammation [8, 9, 10]. Recent data also showed that the incidence of POAF increased when the pericardium was opened. In contrast when the pericardium remained intact, as in transcatheter aortic valve replacement, a risk reduction of 82% was observed [11, 12].
It is currently believed that besides the inflammatory milieu, the presence of
oxidative stress also predisposes to POAF [13]. This happens when the reactive
oxygen species produced inundates the endogenous antioxidant defences [14]. When
the recruited leukocytes are activated to release O
In light of this pathogenesis, we postulate that using a potent anti-inflammatory antioxidant might mitigate POAF. We decided on tocotrienol, a compound that has not been commonly investigated, despite its much superior antioxidative and anti-inflammatory effect compared to its cousin, tocopherol [18]. We hypothesise that this may confer a therapeutic advantage in the safety endpoints post-CABG by reducing the incidence of POAF and its adverse sequelae.
To determine the incidence of POAF, demography, post-operative outcomes including morbidity and mortality, length of CICU stay, HDU stay, and total hospital stay.
We designed this study as a prospective, double-blind, randomised, controlled trial involving parallel groups. All patients who were admitted at the Institut Jantung Negana (IJN), Kuala Lumpur, for CABG, or CABG and valve surgery, were automatically recruited into the study.
Patients were divided into two arms using a computer-generated randomisation programme: (1) a Control group with placebo plus standard care, and (2) a Treatment group with Tocovid, plus standard care.
At least two days prior to surgery, the blinded randomised patients were administered daily with either 400 mg Tocovid in two divided doses, or placebo, which was prepared by Hovid Berhad, a company based in Ipoh, Malaysia. Each 200 mg soft-gel Tocovid capsule contained a cocktail of tocotrienol (61.52 mg alpha-Tocotrienol, 112.80 mg gamma-Tocotrienol and 25.68 mg delta-Tocotrienol) and tocopherol (91.60 IU alpha-tocopherol). This regime was continued post-CABG until six weeks follow-up when the study was terminated.
We decided on giving 400 mg of Tocovid daily since many other clinical studies [19, 20] have used this regime without any adverse effects. We continued the treatment until the patient was discharged. The patients and the surgeons were blinded throughout the study, as were the research assistants. Only Clinical Research Nurses were not blinded. Onsite cardiothoracic ward nurses monitored and ensured compliance. Postoperatively all patients were observed for any electrocardiogram (ECG) changes via continuous ECG monitoring. All POAF episodes were treated according to the preference of the attending cardiothoracic surgeon.
For the study flow chart, refer to attachment: Fig. 1.
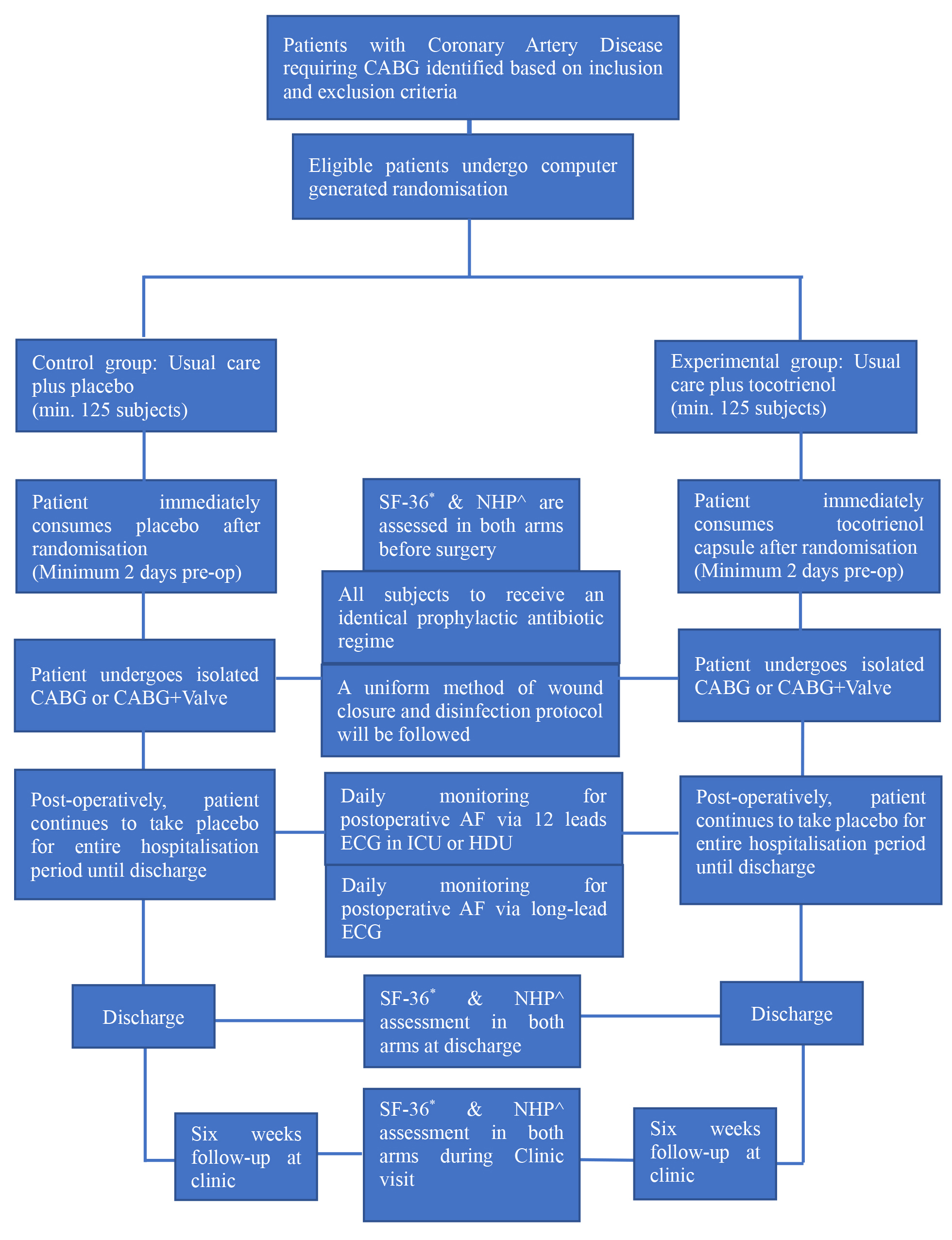 Fig. 1.
Fig. 1.Study Flow Chart. *SF-36, Short Form 36 Questionnaire; ^NHP, Nottingham Health Profile Questionnaire.
Inclusion Criteria:
Males or females over 18 years of age.
Elective, on-pump surgery of coronary artery revascularisation, either isolated or combined with valve surgery.
Exclusion criteria:
Urgent or emergency surgery as well as off-pump surgery.
Poor left ventricular (LV) function (ejection fraction (EF)
Allergy to palm oil or Vitamin E, or any form of arrhythmia pre-operatively.
Long-term treatment with corticosteroid.
Participation in other clinical trial within three months prior to the study.
Vitamin E or other potent antioxidant supplementation with within one month prior to randomisation.
The primary end point was POAF occurrence as confirmed on an ECG by the absence of p-wave and irregularly QRS complex of at least 30-second duration. For shorter ECGs, we diagnosed atrial fibrillation (AF)/atrial flutter (AFL) on the arrhythmia present at onset or termination [21]. The secondary end points were the length of hospital stay (LoHS) including both CICU and HDU stay.
For sample size calculation, we used the PS Power and Sample Size Calculation Software (Version 3.1.6, Developer: W.D. Dupont & W.D. Plummer. Licensed under a Creative Commons Attribution–NonCommercial-NoDerivs 3.0 United States License).
We estimated sample size based on findings from a prior study by Musa et
al. [3]. The researchers found POAF incidence at IJN to be 28.7%. Assuming the
true relative risk of AF for experimental subjects relative to controls is 0.45
[22], then if we use the PS Power and Sample Size Calculator [23, 24] with
For statistical analysis of the data, we used the SPSS software version 27.0 (IBM Inc., Chicago, IL, USA).
We conducted this study according to the Malaysian Good Clinical Practice Guideline while abiding by the Helsinki Declaration revised in 2013. Informed written consent was obtained from all subjects prior to their participation in this study.
We sought ethics approvals from three institutions: the Institut Jantung Negara Research Ethics Committee (IJNREC/201/2017), the Monash University Human Research Ethics Committee (MUHREC) (2017-9227-10263) and the National Pharmaceutical Regulatory Agency (NPRA) (CTX-180304). The study was registered with the National Medical Research Register (NMRR-17-1994-34963) and the US National Library of Medicine-Clinical Trials (NCT03807037).
Recruitment of patients started on 21 January, 2019 and we reached 250 patients on 30 June, 2021 from a total of 1128 patients screened within that period. The current results are based on patients’ data; these were retrieved from patients who have completed the study. The tabulated figures consist of data extracted from both the IJN computer system and physical records.
Our population sample consists of 223 patients (89.2%) who have completed the study. There were 11 withdrawals and another 7 were lost during follow-up. We recorded 9 deaths (3.6%) which was slightly lower compared to our earlier study [25] in 2018 where the mortality rate stood at 4.66%. Therefore, the attrition rate was 7.2%. Eighteen serious adverse events (SAE) were reported but none was related to the investigational product.
The statistical analyses on the results of our study below were on the non-unblinded dataset since we have not completed the collection of all the data. Hence, our analyses were between the POAF group against the non-POAF group–not Tocovid versus control. This final analysis will only be conducted at the end of the study; at that time, all the data would have been completed and the groups unblinded. We also wish to emphasize that our analyses were restricted to patients with complete data. Hence, there might be some variations with regard to the number of patients analysed in each section.
Table 1 below describes the characteristics of our study sample. The mean age
was 60.88
| Demographic | Total, mean |
Non-POAF group, mean |
POAF group, mean |
p-value | |
| Age (years) | 60.88 |
59.93 |
62.36 |
0.02* | |
| Range: 39 to 85 years old | |||||
| Gender: | 0.20 | ||||
| Male | 196 | 121 (61.7) | 75 (38.3) | ||
| Female | 46 | 33 (71.7) | 13 (28.3) | ||
| Population: | 0.40 | ||||
| Malay | 199 | 122 (61.3) | 77 (38.7) | ||
| Chinese | 8 | 6 (75.0) | 2 (25.0) | ||
| Indian | 34 | 25 (73.5) | 9 (26.5) | ||
| Other | 1 | 1 (100.0) | 0 (0.0) | ||
| EuroSCORE II: | 0.39 | ||||
| Low risk | 102 (42.7) | 66 (64.7) | 36 (40.9) | ||
| Medium risk | 108 (45.2) | 70 (64.8) | 38 (35.2) | ||
| High risk | 29 (12.1) | 15 (51.7) | 14 (48.3) | ||
| *p-value significant at 0.05 using independent T-test. | |||||
As a predictive factor of POAF, gender remains a contentious matter. While it is controversial to assume that male gender is a predictor of POAF, the effect of gender on POAF is definitely an interesting field of study. It has been shown that the female gender is shielded against POAF [32] but other studies have shown poorer outcomes among women after CABG [33, 34, 35, 36]. Meanwhile, Filardo et al. [37] attested to the poorer late survival in both women and men; however, they also showed that the early burden of POAF was less in women. While the debate continues, our results showed that there was no statistically significant difference between the sexes in developing POAF although the majority (80.9%) of our patients were males.
However, we found no statistically significant difference exists between the different ethnic groups in terms of POAF. However, this is a marked difference from our previous study [25] in which the Indian population had significantly lower odds of developing POAF compared to the other races. It also contrasts with a Singaporean study [38] that found that Malays and Chinese, as compared to Indians, had a higher likelihood of developing this phenomenon post-CABG. Western papers [39, 40, 41] showed that Caucasians were more prone to developing POAF compared to blacks, and genetic disparity between the races was thought to be the reason [39]. However, the survival rate of POAF patients after CABG showed that the black race was a significant predictor for decreased survival [40, 41]. This finding was definitely useful to both the surgeons and their patients.
Our study cohort showed that most of our patients (87.9%) were in the low and medium risk EuroSCORE II group. We observed no statistically significant difference in the development of POAF in between these groups. However, an earlier study by Chen-Scarabelli et al. [42] showed that higher EuroSCORE was associated with POAF though not with mortality after CABG surgery.
Table 2 below refers to the POAF (post-operative AF) characteristics of our study patients. 35.2% of patients developed POAF which is higher compared to our previous study [25] where 28.7% of the patients developed AF post CABG. However, it would be hasty to conclude that Tocovid has no effect in lowering the POAF rate since this is still a blinded analysis. Nevertheless, 35.2% falls within the POAF incidence range cited in the literature [43, 44, 45].
| Characteristics of AF | n (%), mean | |
| Occurrence of POAF | 88 (35.2) | |
| Time from surgery to POAF (minutes) | 2793.61 | |
| Range: 10 to 7044 minutes | ||
| Duration (hours): | ||
| 45 (52.9) | ||
| 40 (47.1) | ||
| Number of episodes: | ||
| Single | 45 (51.1) | |
| Multiple | 43 (48.9) | |
| Atrial fibrillation on discharge | 0 (0.0) | |
The mean time for POAF development of was 46.56
Malaysia has the highest rate of obesity and overweight among Asian countries according to World Health Organization (WHO) [50]. Table 3 below indicates that 52.22% of the study sample was overweight and 25.12% was obese according to the Asian guidelines [51]. However, no statistically significant difference was observed between the groups in terms of POAF occurrence. This finding contradicts some reports in the literature [52, 53, 54, 55] which suggest that, compared to their non-obese counterparts, obese patients are more prone to develop POAF. An earlier work of Sun X et al. [56] together with a most recent study by Vural Ü and Aglar A [57] have suggested that obesity is a predictor for POAF. However, a very recent meta-analysis [58] of 36 prospective studies which has yet to be peer-reviewed found that obesity might not increase the risk of developing POAF after CABG.
| Pre-operative characteristic | Total, mean |
Non-POAF group, mean |
POAF group, mean |
p-value | |
| Body Mass Index (kg/m |
27.15 |
27.25 |
26.86 |
0.29 | |
| 2 (0.8) | 0 (0.0) | 2 (100.0) | |||
| 18.5–22.9 | 57 (23.6) | 38 (66.7) | 19 (33.3) | ||
| 23–29.9 | 124 (51.2) | 79 (63.7) | 45 (36.3) | ||
| 59 (24.4) | 37 (62.7) | 22 (37.3) | |||
| Range: 17.6 to 42.47 | |||||
| New York Heart Functional Class: | 0.89 | ||||
| NYHA I | 145 (60.2) | 92 (63.4) | 53 (36.6) | ||
| NYHA II | 94 (39.0) | 61 (64.9) | 33 (35.1) | ||
| NYHA III | 2 (0.8) | 1 (50.0) | 1 (50.0) | ||
| NYHA IV | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Left ventricular ejection fraction | 51.45 |
51.92 |
50.67 |
0.29 | |
| Range: 9 to 67 | |||||
| Left atrial size (mm) | 18.09 |
17.63 |
18.74 |
0.09 | |
| Range: 9 to 46 | |||||
| Right atrial size (mm) | 13.88 |
13.43 |
14.51 |
0.007* | |
| Range: 7.7 to 31 | |||||
| *p-value significant at 0.05 using independent T-test. | |||||
We have excluded poor EF (
The pre-morbid history of our patients is illustrated in Table 4 below. As expected, the majority were afflicted with hypertension (81%), diabetes mellitus (62%) and hypercholesterolaemia (90.1%) but we noticed no statistically significant difference between the groups. Similarly, our analysis on chronic kidney disease which is normally linked to POAF [64, 65], showed no significant difference in between the two groups.
| Medical condition | Total, n (%) | Non-POAF group, n (%) | POAF group, n (%) | p-value | ||
| COPD: | - | 0.7 | ||||
| Yes | 3 (1.2) | 2 (66.7) | 1 (33.3) | |||
| No | 239 (98.8) | 152 (63.6) | 87 (36.4) | |||
| Asthma: | - | 0.64 | ||||
| Yes | 1 (0.4) | 1 (100.0) | 0 (0.0) | |||
| No | 241 (99.6) | 153 (63.5) | 88 (36.5) | |||
| Hypertension: | 0.35 | 0.56 | ||||
| Yes | 196 (81.0) | 123 (62.8) | 73 (37.2) | |||
| No | 46 (19.0) | 31 (67.4) | 15 (32.6) | |||
| Diabetes mellitus: | 0.46 | 0.49 | ||||
| Yes | 150 (62.0) | 93 (62.0) | 57 (38.0) | |||
| No | 92 (38.0) | 61 (66.3) | 31 (33.7) | |||
| Hypercholesterolemia: | 0.32 | 0.57 | ||||
| Yes | 218 (90.1) | 140 (64.2) | 78 (35.8) | |||
| No | 24 (9.9) | 14 (58.3) | 10 (41.7) | |||
| Chronic kidney disease: | 0.08 | 0.77 | ||||
| Yes | 23 (9.5) | 14 (60.9) | 9 (39.1) | |||
| No | 219 (90.5) | 140 (63.9) | 79 (36.1) | |||
| Current or ex-smoker: | 0.08 | 0.77 | ||||
| Yes | 127 (54.3) | 83 (65.4) | 44 (34.6) | |||
| No | 107 (45.7) | 68 (63.6) | 39 (36.4) | |||
| Alcohol intake: | - | 0.18 | ||||
| Yes | 9 (3.9) | 4 (44.4) | 5 (55.6) | |||
| No | 219 (96.1) | 142 (64.8) | 77 (35.2) | |||
When we compared current or ex-smokers with non-smokers to analyse the
relationship between smoking habits and POAF incidence, we observed no
statistically significant difference between them (p = 0.77). In
contrast, a previous study [66] showed smokers tend to have a lower incidence of
POAF (p
We performed isolated CABG in 92.5% and CABG combined with valve surgery in 7.5% in our study population as shown in Table 5 below. Mitral valve replacement surgery accounts for almost 60% of cases of the combined surgery group; only one case involved mitral valve repair. Aortic valve replacement was performed in the remaining 40% of cases. However, no statistically significant difference was observed between these groups in terms of developing POAF. This contradicts the general belief that a combined valve with CABG would result in a higher occurrence of POAF [70, 71] besides the use of heart-lung bypass machine [72, 73]. In a recent multicentre prospective study [74] involving a total of 28 centres, it was reconfirmed that combined valve and CABG was significantly correlated with the occurrence of POAF.
| Operative details | Total, mean |
Non-POAF group, mean |
POAF group, mean |
p-value | ||
| Surgery type: | ||||||
| CABG alone | 222 (92.5) | 143 (64.4) | 79 (35.6) | 1.49 | 0.22 | |
| CABG + valve | 18 (7.5) | 9 (50.0) | 9 (50.0) | |||
| Bypass time (in minutes) | 97.00 |
95.98 |
98.91 |
0.54 | ||
| Range: 42 to 304 minutes | ||||||
| Cross-clamp time (in mins) | 75.84 |
75.86 |
75.81 |
0.22 | 0.99 | |
| Range: 17 to 244 minutes | ||||||
| Number of anastomoses: | ||||||
| Single | 6 (2.5) | 2 (33.3) | 4 (66.7) | - | 0.13 | |
| Multiple | 234 (97.5) | 150 (64.1) | 84 (35.9) | |||
The mean cross-clamp time in our study was 75.84
Adverse outcomes such as stroke, reoperation, infection, renal failure, respiratory complications and other cerebral insults, besides a twofold increase in mortality [80, 81, 82] were always associated with POAF. Admittedly, while this correlation might not be direct, it does contribute to the increase in morbidity and mortality post-CABG. In Table 6 below, although more POAF patients developed stroke as compared to non-POAF, it was not statistically significant. While the mortality rate in our study population was 3.6% as compared to the mortality rate in our earlier publication (4.66%) [25] this was definitely much lower. But we saw a statistically significant difference with a threefold increase in death among patients that developed POAF post-CABG. Our finding concurs with a recent paper by Emma Thorén et al. [83] where POAF was associated with mortality with a more recent paper from Taiwan which also concluded that in the Asian population, POAF is significantly correlated with an overall mortality [84].
| Post-operative outcomes | Total, n (%) | Non-POAF group, n (%) | POAF group, n (%) | p-value | ||
| Stroke: | - | 0.14 | ||||
| Yes | 4 (1.7) | 1 (25.0) | 3 (75.0) | |||
| No | 232 (98.3) | 148 (63.8) | 84 (36.2) | |||
| Sternal infection: | - | 0.6 | ||||
| Yes | 6 (2.5) | 4 (66.7) | 2 (33.33) | |||
| No | 232 (97.5) | 146 (62.9) | 86 (37.1) | |||
| Respiratory problems: | - | 0.2 | ||||
| Yes | 9 (3.8) | 4 (44.4) | 5 (55.6) | |||
| No | 229 (96.2) | 146 (63.8) | 83 (36.2) | |||
| Renal failure requiring dialysis: | - | 0.007** | ||||
| Yes | 12 (5.0) | 3 (25.0) | 9 (75.0) | |||
| No | 226 (95.0) | 147 (65.0) | 79 (35.0) | |||
| Endocrine problems: | - | 0.63 | ||||
| Yes | 1 (0.4) | 1 (100.0) | 0 (0.0) | |||
| No | 237 (99.6) | 149 (62.9) | 88 (37.1) | |||
| Pleural effusion: | 4.79 | 0.03* | ||||
| Yes | 18 (7.6) | 7 (38.9) | 11 (61.1) | |||
| No | 219 (92.4) | 142 (64.8) | 77 (35.2) | |||
| Cardiac Tamponade: | 0.16 | 0.69 | ||||
| Yes | 22 (9.2) | 13 (59.1) | 9 (40.9) | |||
| No | 216 (90.8) | 137 (63.4) | 79 (36.6) | |||
| Fever: | - | 0.10 | ||||
| Yes | 12 (5.0) | 5 (41.7) | 7 (58.3) | |||
| No | 226 (95.0) | 145 (64.2) | 81 (35.8) | |||
| Hyperkalaemia: | - | 0.15 | ||||
| Yes | 4 (1.7) | 1 (25.0) | 3 (75.0) | |||
| No | 233 (98.3) | 148 (63.5) | 85 (36.5) | |||
| Others: | - | 0.06 | ||||
| Yes | 7 (2.9) | 2 (28.6) | 5 (71.4) | |||
| No | 231 (97.1) | 148 (64.1) | 83 (35.9) | |||
| Death: | - | 0.01* | ||||
| Yes | 9 (3.75) | 2 (22.2) | 7 (77.8) | |||
| No | 231 (96.25) | 150 (64.9) | 81 (35.1) | |||
| *p-value significant at 0.05 using Chi Square Test. **p-value significant at 0.05 using Fisher exact Test. | ||||||
We also assessed other common complications as depicted in Table 6 but none of them, except pleural effusion, were significantly correlated with POAF. This is consistent with the finding by Brookes et al. [85] who found a link between new onset atrial fibrillation and pleural effusion. Similarly, Anderson [86] also showed that self-clearing chest tubes may reduce POAF although a randomized data is still needed to prove this claim. Interestingly a systematic review by Gozdek et al. [87] showed that posterior pericardial drainage to minimize any possibility of pericardial tamponade could reduce the odds of POAF by 58% indicating that POAF is possibly associated with pericardial collections. In our study cohort as well, we noticed that statistically significant number of patients with renal failure developed POAF. Similarly, the correlation between renal dysfunction and POAF has been established by Chua et al. [88]. While the mechanism was not fully understood, it was thought to be related to fluid overload and activation of renin-angiotensin-aldosterone cascade which would then lead to myocardial fibrosis [89].
To date, no study in Malaysia has assessed the economic impact of managing POAF patients post cardiac surgery. The closest regional study was conducted in Thailand [90] where it was shown that there was a statistically significant high economic burden in managing POAF patients. Studies conducted elsewhere have demonstrated that POAF was associated with prolonged CICU stay and total hospital stay [91, 92]. This would of course be translated into an increased cost of hospitalisation. For instance, US patients who developed POAF would incur additional hospital treatment costs in the range of USD10,000 to USD20,000 [93]. Furthermore, US healthcare expenditures related to POAF management were approximately 1 billion USD per year [94]. Another study [95] demonstrated that POAF led to an increase in the utilisation of hospital resources, with an increase in the direct costs of managing affected patients. No such studies have been conducted locally regarding the financial burden in managing POAF patients. However, it would not be surprising if it yields similar results.
Based on the outcomes tabulated in Table 7 above, there was a statistically significant difference between the two groups with regard in to the mean duration of CICU stay (p = 0.005) and HDU stay (p = 0.02). Similarly, there was also a significant difference in total duration of hospital stay (p = 0.001). Our findings concur with one study [73] that collected data from 28 centres which showed that POAF occurrence was significantly correlated to the length of stay in CICU and total hospital stay with a resultant increase in resource utilisation.
| Duration | Total, median |
Non-POAF group, median |
POAF group, median |
p-value | |
| Duration in CICU (minute) | 1722 |
1632 |
2872 |
0.005* | |
| Range: 640 to 67740 minutes | |||||
| Duration in HDU (minute) | 1640 |
1545 |
2700 |
0.02* | |
| Range: 190 to 14760 minutes | |||||
| Duration of ventilation (minute) | 1134 |
1110 |
1190 |
0.06 | |
| Range: 350 to 17120 minutes | |||||
| Duration of hosp. stay (day) | 7.0 |
7.0 |
8.0 |
0.001* | |
| Range: 5 to 86 days | |||||
| Reintubation: | 0.12 | ||||
| Yes | 8 (3.4) | 3 (37.5) | 5 (62.5) | ||
| No | 230 (96.6) | 148 (64.3) | 82 (35.7) | ||
| *p-value significant at | |||||
35.2% of our study population exhibited POAF. This was slightly higher compared to our previous study [2] of about 28.7%. We should note that despite advances in the perioperative cardiac surgery care, the length of stay in the CICU, HDU, and the total hospital stay have remained unchanged over the years [96, 97]. At the moment we are unsure whether our prophylactic intervention using Tocovid would reduce the incidence of POAF in the study arm. Despite this uncertainty, we take comfort in the words of Sir William Ramsay, the Chemist Nobel Laureate, who reminds us that progress is made by trial and failure. Therefore, we shall endure until the study is unblinded.
As we outlined earlier, oxidative stress and inflammation from the shed mediastinal blood within the pericardium are now thought to be responsible for the pathogenesis of POAF. Cardiac surgery itself inflicts a trauma on the heart, and this is compounded by the use of cardiopulmonary bypass that produces ischaemic injury. Oxidative stress and the production of pro-inflammatory molecules from reperfusion injury after cardioplegic arrest activateds the production of leucocytes, nitrous oxide and reactive oxygen species [79, 98]. Human studies have demonstrated that a correlation exists between the development of POAF with systemic inflammation and oxidative stress [99, 100].
Studies have shown that longer CICU and hospital stay, and a higher rate of readmission were associated with POAF [95, 101]. These outcomes translate into approximately USD 2 billion out of more than USD 6 billion per year related to POAF care in the US [102, 103]. Unfortunately, no financial data from IJN of Kuala Lumpur or any other cardiac centres in Malaysia are available with regard to the total cost in managing patients with POAF. Nonetheless, there is no doubt that managing such patients entails higher costs. Therefore, reducing POAF incidence among post-CABG patients would benefit not only patients or hospitals but to the national economy itself.
We are aware that other compounds have been used in research to prevent POAF; for instance, polyunsaturated fatty acids (PUFAs), vitamin C, or a combination of vitamins C and E [104]. PUFAs have been demonstrated to reduce cardiovascular morbidity in animal models [105]. In a study by Rubanenko O and Rubanenko A [106], patients treated with PUFAs not only displayed reduced in inflammation and oxidative stress after CABG, but also exhibited a reduction in POAF after CABG. A meta-analysis [107] of 19 randomised controlled trials (RCTs) conducted in 2017 and a meta-analysis [108] in 2018 that included 14 RCTs also showed that CABG patients treated with PUFAs displayed a significant reduction of POAF compared to controls. In all these cases, an antioxidant prevented POAF, and the results were very promising the more so since our study is based on the same presumption.
Similarly, vitamin C, a known antioxidant, has been studied. A 2016 meta-analysis [109] of 7 RCTs showed that vitamin C treatment reduces the incidence of POAF. However, a more recent RCT [110] in 2018 found no significant difference. But to date, there are no guidelines on the use of vitamin C for POAF prophylaxis. A 2013 study [111] used combined antioxidants with vitamin C, vitamin E and PUFAs, demonstrated a significant reduction in the incidence of POAF among patients receiving these cocktails as compared to controls. However, to date, there are no guidelines regarding this protocol.
With the aforementioned studies and the postulated inflammatory and oxidative pathways in the promotion of POAF, we anticipate that using Tocovid, a strong antioxidant and anti-inflammatory agent, might be useful in mitigating the occurrence of POAF. We understand that it is still too early to make any definite claim. Nonetheless, this study has a scientific rationale, and once completed, it will be unblended for analysis.
Our main limitation was the patients’ recruitment. This is due to the current COVID-19 pandemic which reduced the number of patients that could be enrolled in our study as a result of the limited availability of ICU beds. Similarly, the rate of tracing the patients’ medical records at the IJN Record Office dampened the pace of the study since only limited records were available for tracing each week. Not all the required data points were available on the track care, making reference to patients’ medical records unavoidable.
As a preliminary conclusion, we would like to reiterate that POAF after cardiac surgery was the most common complication after CABG; it occurred in 35.2% of our study population. There was a statistically significant difference among POAF patients with regard to the occurrence of renal failure and death; we observed a three-fold increase in both. Both CICU and HDU time, and also the total hospital stay, were significantly longer among POAF patients. This translates to a heavier economic burden on the patient, the hospital, and the economy, although we have not conducted any cost analysis in this study.
All authors of this paper have read and approved the final version submitted.
Harvard Dataverse: Replication Data for: A mid-cycle analysis on the role of Tocovid, a tocotrienol-rich vitamin E, in preventing atrial fibrillation after coronary artery bypass grafting (CABG) surgery.
Link: https://doi.org/10.7910/DVN/BZBHGX.
This project contains the following underlying data:
Set 1: Raw Data.
Set 2: Output Data.
CONSORT Checklist.
AFM—conceptualization, data curation, formal analysis, investigation, methodology, project administration, visualization, writing-original draft preparation, writing-review and editing; JD, MEMT, AMY, ARS, MNN—provided significant input into the study protocol, performed the bypass surgery on the study patients, and provided the post-operative care; JAS—administration, supervision, validation, writing-review and editing.
The study protocol was approved by the Institut Jantung Negara Ethics Committee (IJNREC/201/2017), Monash University Human Research Ethics Committee (MUHREC/2017-9227-10263). and the National Pharmaceutical Regulatory Agency (NPRA/CTX-180304). IJNREC also served as the data safety committee.
We registered the study with the National Medical Research Registry (NMRR-17-1994-34963) and the US National Library of Medicine-Clinical Trials (NCT03807037).
Link: https://clinicaltrials.gov/ct2/show/NCT03807037.
Written informed consent was obtained from all subjects prior to commencement of the study. A copy of the written consent form is available for review by the Editorial office/Chief Editor/Editorial Board members of this journal.
The authors would like to thank the following people for their contribution to this study: Mohd Zahid Kamaruddin, Cardiothoracic trainee at Institut Jantung Negara (IJN) for his tireless effort, Madam Irni Yusnida Mohd Rashid, Senior Study Coordinator, Clinical Research Department, IJN; the Clinical Research nurses at IJN; and our dedicated research assistants namely Mohd Ikhmal Othman, Anisah Zahirah Nor Aripin and Ahmad Muziru Idham Adnan.
HOVID Berhad: MMRD-MS-1801 and Malaysian Palm Oil Berhad (MPOB): MMRD-MS-2001 funded this project. However, the funders were involved neither in the design of the project nor in the preparation of this manuscript.
The authors declare no conflict of interest.