

 , Yuka Kimura 1, Satoshi Kasagi 1,5, Takatoshi Kasai 1,3,4
, Yuka Kimura 1, Satoshi Kasagi 1,5, Takatoshi Kasai 1,3,41 Sleep Center, Toranomon Hospital, 105-8470 Tokyo, Japan
2 Cardiovascular Center, Toranomon Hospital, 105-8470 Tokyo, Japan
3 Department of Cardiovascular Medicine, Juntendo University Graduate School of Medicine, 113-8421 Tokyo, Japan
4 Cardiovascular Respiratory Sleep Medicine, Juntendo University Graduate School of Medicine, 113-8421 Tokyo, Japan
5 Okinaka Memorial Institute for Medical Research, 105-8470 Tokyo, Japan
Academic Editor: Matteo Bertini
Abstract
Background: Abnormal respiration during radiofrequency catheter
ablation (RFCA) with deep sedation in patients with atrial fibrillation (AF) can
affect the procedure’s success. However, the respiratory pattern during RFCA with
deep sedation remains unclear. This study aimed to investigate abnormal
respiration during RFCA and its relationship with sleep apnea in patients with
AF. Methods: We included patients with AF who underwent RFCA with
cardiorespiratory monitoring using a portable polygraph both at night and during
RFCA with deep sedation. The patients were divided based on the administered
sedative medicines. Results: We included 40 patients with AF. An
overnight sleep study revealed that 27 patients had sleep apnea; among them, 9
showed central predominance. During RFCA with deep sedation, 15 patients showed
an abnormal respiratory pattern, with 14 patients showing obstructive
predominance. Further, 17 and 23 patients were administered with propofol alone
and dexmedetomidine plus propofol, respectively. There was no significant
between-group difference in the respiratory event index (REI) at night (7.9 vs.
9.3, p = 0.744). However, compared with the group that received
dexmedetomidine plus propofol, the propofol-alone group showed a higher REI
during RFCA (5.4 vs. 2.6, p = 0.048), more frequent use of the airway
(47% vs. 13%, p = 0.030), and a higher dose of administered propofol
(3.9 mg/h/kg vs. 1.2 mg/h/kg, p
Keywords
- obstructive sleep apnea
- central sleep apnea
- atrial fibrillation
- radiofrequency catheter ablation
- sedation
Atrial fibrillation (AF) is often related to sleep apnea [1] and there is a need to elucidate their relationship. AF is a common disease that is recently frequently treated with radiofrequency catheter ablation (RFCA) therapy. The widespread use of ablation therapy could be attributed to improvements in treatment techniques and sedative use, which have shortened the treatment time, improved the success rate, and reduced complications [2]. Moreover, the presence of sleep apnea in patients with AF is associated with the success rate of ablation therapy [3]. Continuous positive airway pressure (CPAP) therapy is the gold standard for obstructive apnea; further, it reduces AF recurrence after ablation [4, 5].
Obesity and apnea are associated with the success rate of ablation [6]. The sudden cessation and resumption of breathing during ablation with sedation could prolong the treatment time and reduce the success rate. In Japan, some electrophysiology cardiologists prefer using adaptive servo-ventilation (ASV) to stabilize breathing during ablation [7].
Central and obstructive apneas are common sleep-related breathing disorders related to AF; however, there have been inconsistent reports regarding the frequency of central apnea [8]. The occurrence of central apnea during ablation compared with that during sleep, as well as the significance of using ASV during ablation, remain unclear. This study aimed to investigate sleep apnea in patients with AF undergoing ablation therapy and respiratory abnormalities during ablation with sedatives.
We included consecutive patients who were admitted to our hospital for RFCA from
January 2016 to May 2017. We excluded patients aged
Upon admission for ablation therapy, height and weight measurements, as well as responses to the Epworth Sleepiness Scale (ESS) questionnaire, were collected. For echocardiography, we used data obtained within six months before ablation therapy.
The patients underwent cardiorespiratory monitoring using a portable digital
polygraph (SAS-3200, Nihon Kohden, Tokyo, Japan) during the night before RFCA and
during the RFCA procedure with deep sedation. Arterial oxygen saturation
(SaO
The monitoring time during ablation was defined as the time from sedative
administration to the end of the ablation procedure unless the following
situations occurred: oxygen administration; mechanical airway clearance; and
other operations that interrupted cardiopulmonary recordings, including
pericardiocentesis for cardiac tamponade. The respiratory event index (REI) was
defined as the number of events during the monitoring time of each setting. We
defined sleep apnea as a nighttime REI
Before procedure commencement, cardiorespiratory monitoring equipment, as well as monitors required for the procedure, were placed. This was followed by the administration of sedatives; specifically, propofol alone or in combination with dexmedetomidine, to achieve deep sedation and reduce intraprocedural movement. The operator preoperatively determined the sedative choice. Concomitant administration of dexmedetomidine began after August 2016. Further, the operator who performed ablation operator was blinded to the presence or absence of apnea at night. In case of use of the nasopharyngeal airway during the ablation or starting of supplemental oxygen, respiratory events were calculated until the time for analysis.
Continuous variables are expressed as mean and standard deviation or median and interquartile range, while categorical variables are presented as numbers and percentages.
Two groups of patients were compared based on the presence or absence of sleep
apnea and sedative medication. Between-group comparisons of categorical and
continuous variables were performed using the chi-squared test or Fisher’s exact
test and the t-test or Mann-Whitney U-test, respectively. A multivariate
regression model was used to identify predictors of REI values during ablation.
In this model, the explanatory variables included age, sex, body mass index
(BMI), REI value during the day, and propofol administration rate. Statistical
analyses were performed using R software, version 3.4.3 (R Core Team, Vienna, Austria).
Two-sided p values
We included 40 patients (85% men; mean age: 60 years; mean BMI: 23.7). The median time since AF diagnosis was 18 months; further, 30% of the patients had chronic AF and the median ESS score was 6 points. In the nocturnal sleep study, the mean recording time was 435 minutes. The median REI was 9.0. Further, 27 patients had sleep apnea, with 18 and 9 patients showing obstructive and central respiratory events, respectively. There were no significant differences in age, sex, and BMI between patients with or without apnea (cut-off REI value of 5/h). There was no significant difference in the median ESS score between patients with and without apnea (5.5 vs. 9.0, p = 0.743). Additionally, there were no significant between-group differences in the rate of chronicity and duration of AF. Data obtained from echocardiography, including the left ventricular ejection fraction and left atrial diameter, were not significantly associated with the presence of sleep apnea (Table 1).
| Sleep apnea (n = 27) | No sleep apnea (n = 13) | p value | |
| Age, years | 61 |
57 |
0.331 |
| Male, n (%) | 25 (93%) | 9 (69%) | 0.053 |
| BMI, kg/m |
24.0 |
23.1 |
0.485 |
| ESS | 5.5 (3.0–7.8) | 9.0 (4.5–12.0) | 0.743 |
| Persistent AF, n (%) | 18 (67%) | 10 (77%) | 0.507 |
| History of AF, months | 16 (4.5–66) | 22 (6.0–72) | 0.675 |
| LVEF, % | 64.4 |
67.7 |
0.196 |
| LAD, mm | 39.9 |
36.4 |
0.073 |
| BMI, body mass index; ESS, Epworth Sleepiness Scale; AF, atrial fibrillation; LVEF, left ventricular ejection fraction; LAD, left atrial dimension. | |||
Comparison according to the sedatives used during ablation revealed that the combination group was significantly older than the propofol alone group. However, there were no significant between-group differences in other background factors, nighttime REI values, and event type (obstructive or central) (Table 2). Regarding cardiorespiratory monitoring during ablation, the mean recording time was 173 minutes and the median REI was 3.5. Additionally, 15 patients developed abnormal breathing during ablation, with 14 and 1 patient showing obstructive and central respiratory events, respectively. Compared with the combination group, the propofol-alone group showed significantly higher REI values and use of the nasopharyngeal airway. There was no between-group difference in supplemental oxygen use. Contrastingly, the combination group showed a significantly higher propofol administration rate than the propofol-alone group (Table 3).
| Propofol-alone group (n = 17) | Combination group (n = 23) | p value | |
| Age, years | 55 |
63 |
0.016 |
| Male, n (%) | 15 (88%) | 19 (83%) | 0.999 |
| BMI, kg/m |
24.0 |
23.4 |
0.594 |
| ESS | 5 (3.5–5.5) | 6 (3–8.8) | 0.180 |
| Persistent AF, n (%) | 4 (24%) | 8 (35%) | 0.505 |
| History of AF, months | 24 (8–72) | 13 (4–62.5) | 0.933 |
| LVEF, % | 65.8 |
65.2 |
0.789 |
| LAD, mm | 38.9 |
38.7 |
0.929 |
| Recording time, min | 493 |
431 |
0.797 |
| REI, /h | 7.9 (4.0–13.3) | 9.3 (2.7–12.4) | 0.744 |
| Lowest SaO |
88% (86–93%) | 90% (85–91%) | 0.865 |
| BMI, body mass index; ESS, Epworth Sleepiness Scale; AF, atrial fibrillation;
LVEF, left ventricular ejection fraction; LAD, left atrial dimension; REI,
respiratory index; SaO | |||
| Propofol-alone group (n = 17) | Combination group (n = 23) | p value | |
| Recording time, min | 135 |
200 |
0.028 |
| REI, /h | 5.4 (2.0–11.4) | 2.6 (1.5–4.8) | 0.048 |
| Lowest SaO |
88% (84–90%) | 90% (87–95%) | 0.347 |
| Supplemental oxygen | 17 (100%) | 19 (83%) | 0.123 |
| Nasopharyngeal airway | 8 (47%) | 3 (13%) | 0.030 |
| Propofol, mg/h/kg | 3.9 |
1.2 |
|
| REI, respiratory index; SaO | |||
There was no significant correlation between the nighttime REI and the REI during ablation (r = 0.06, p = 0.689, Fig. 1). The multivariate model revealed that only the rate of propofol administration was a significant predictor of REI during ablation (Table 4).
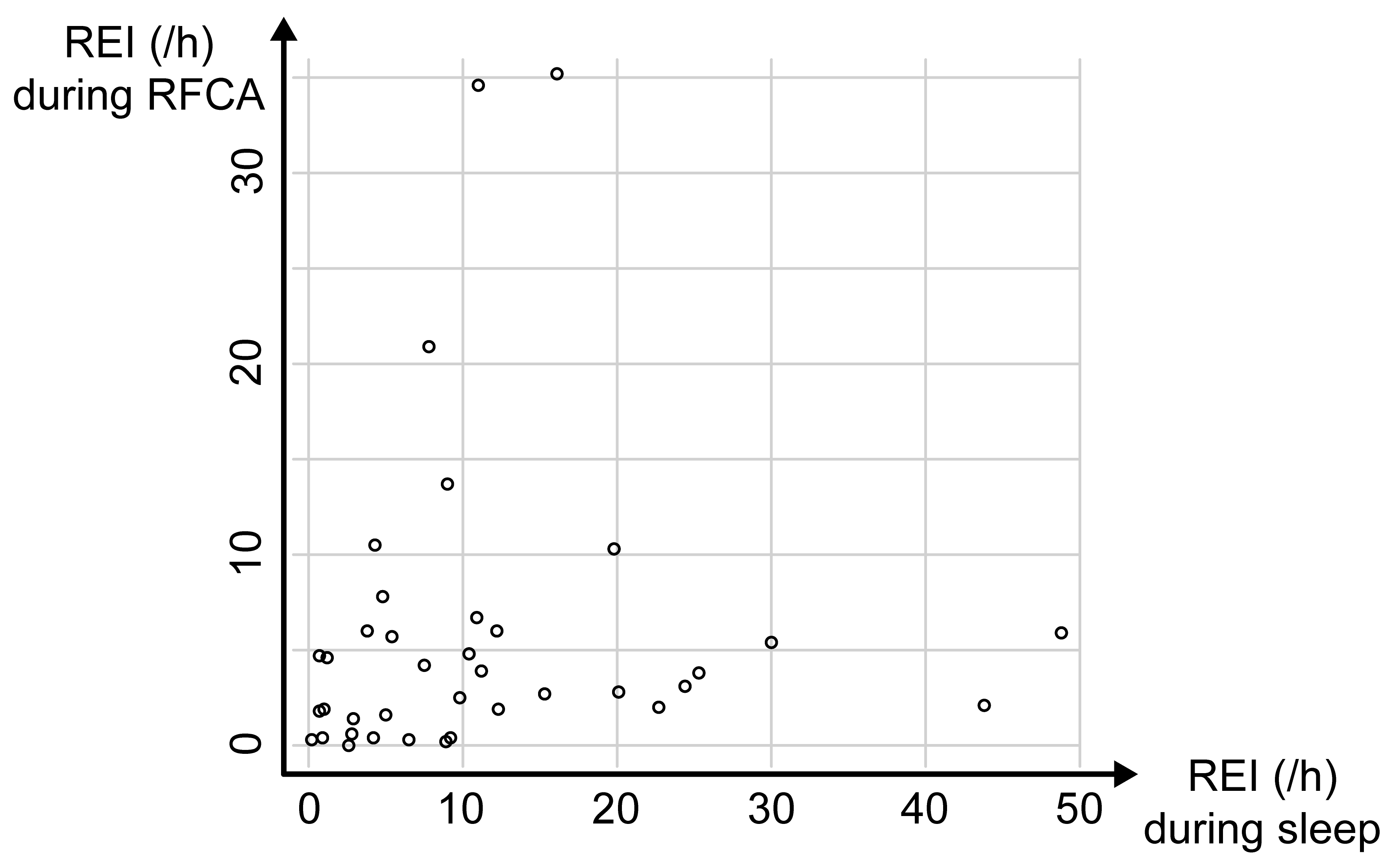 Fig. 1.
Fig. 1.Relationship between the respiratory event index (REI) during sleep and the REI during ablation. There was no significant correlation between nighttime REI and REI during radiofrequency catheter ablation (RFCA).
| p value | ||
| Age | 0.07 | 0.586 |
| Sex | 1.92 | 0.571 |
| BMI | 0.01 | 0.993 |
| REI during sleep | 0.07 | 0.579 |
| Propofol | 2.6 | 0.002 |
|
BMI, body mass index; REI, respiratory index; | ||
In our study, among 40 participants scheduled for AF ablation, two-thirds had sleep apnea; among them, one-third showed predominantly central sleep apnea (CSA). Moreover, approximately one-third of the patients with respiratory events scored as apneas or hypopneas under sedation during ablation, with most being obstructive events. Nocturnal REI was not a predictor of the severity of apneic events during ablation; instead, the amount of propofol used for sedation was a significant predictor.
AF is associated with a high incidence of apnea (21%–74%) [1]. However, few studies have described the association of AF with obstructive and central apnea separately. AF is an established risk factor for CSA, which is considered independent of the presence or absence of HF. However, the rate of CSA complications and their pathogeneses remain unclear [8]. In our study, one-third of the patients with nocturnal apneas showed predominantly central apneas. Future studies on the predictive factors for the development of central events are warranted. It remains unclear whether CPAP therapy for apnea in patients with AF who underwent ablation reduces AF recurrence. However, it is known that patients with AF have poor adherence to CPAP, which could be partly attributed to the fact that they are not sleepy even though they have sleep apnea [9]. In our study, approximately one-third of the patients with AF had CSA, which may result in poor adherence to CPAP treatment. We believe that evaluation of residual apnea and, if necessary, use of ASV may be a treatment option.
Propofol or midazolam may be used for deep sedation during ablation therapy; furthermore, respiratory support, including airway or mask-supported positive pressure breathing, may be required [7]. Moreover, dexmedetomidine is a sedative with low respiratory depression that has been used for non-intubated patients requiring sedation for surgical and diagnostic procedures [10]. We found that respiratory events, especially obstructive events, appeared during sedation in a manner dependent on the propofol dose. Since the propofol amount can be reduced by the concomitant use of dexmedetomidine, this combination strategy can allow decreased respiratory events during sedation.
Several studies have shown that ASV is helpful as a respiratory aid during ablation procedures for AF. However, in our study, the respiratory events during ablation were mainly obstructive; therefore, CPAP may be acceptable rather than ASV. It may be desirable to use a nasal airway or similar device to avoid obstruction. Since many patients present with central apnea at night, periodic breathing after block release should be considered.
This study has several limitations. First, we performed cardiorespiratory
monitoring using a portable monitor rather than full polysomnography. We used the
same device at night and during the ablation in order to obtain similar
parameters for both periods. Therefore, hypopnea could only be scored for events
with desaturation, which may result in underestimation. Nevertheless, obstructive
and central events were differentiated by monitoring the respiratory effort and
snoring sounds. Second, recordings during ablation were short (mean
In conclusion, AF-related sleep apnea was frequent; additionally, one-third of the patients with sleep apnea predominantly showed central events. Given the variety of AF-related respiratory events, appropriate evaluation is necessary before interventions for sleep apnea in patients with AF.
YT and TK designed the research study. YT performed the research. YK and SK provided help and advice on the data analysis and interpretation. YT and YK analyzed the polygraph data. YT, SK and TK wrote the manuscript. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript.
The Toranomon Hospital Ethics Committee approved the study (No. 1273), and informed consent to participate was obtained from all the participants.
The authors are grateful to Haruo Mitani, who was the main operator for catheter ablations performed during the period of the study.
This work was supported by the Okinaka Memorial Institute for Medical Research Foundation (100012832). The funding source has no other role in this study.
The authors declare no conflict of interest. Takatoshi Kasai is serving as one of the Editorial Board members/Guest editors of this journal. We declare that Takatoshi Kasai had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Matteo Bertini.