1. Introduction
Ischaemic heart disease (IHD) is a major cause of morbidity and mortality
worldwide [1, 2]. Over the years major advances have been made in its overall
management, with exercise-based cardiac rehabilitation (EBCR) being central in
the current management of individuals with IHD [3, 4, 5]. Exercise has a broad impact
on the cardiovascular (CV) system, on both the heart and the peripheral
vasculature, being associated with several beneficial effects in terms of the CV
function (such as cardiac contractility and chronotropic reserve) and risk factor
control, as well as having several extra-CV actions such as effects on
inflammation and on metabolic pathways [6, 7, 8].
Cardiopulmonary exercise testing (CPET) can have a central role in the
assessment of individuals undergoing EBCR, as to provide integrative data on the
CV, pulmonary, and musculoskeletal systems, as well as their interactions [9, 10]. Indeed, beyond its role in risk stratification and exercise prescription,
several studies have highlighted the association between functional parameters
and CV events [11, 12, 13].
While there are currently extensive data on the beneficial effects of EBCR in
the setting of IHD, there are still some caveats related to its optimal
application [14, 15]. Notably, certain subgroups of individuals such as the
elderly tend to be underrepresented in different series [7, 14, 16]. Importantly,
this group of patients can have a worse prognosis after an acute myocardial
infarction (AMI) [4, 17, 18]. In this regard, some studies have suggested the
beneficial effects of EBCR among elderly individuals, in terms of functional
parameters such as the peak oxygen uptake (pVO) as well as events [14, 19, 20]. We have previously shown that, in a group of AMI survivors undergoing an
EBCR programme, the elderly had significant improvements in functional parameters
(as assessed by pVO and exercise duration), though these were smaller than
those presented by their younger counterparts [20]. Interestingly, differences in
terms of functional parameters between older and younger individuals have also
been reported in other studies [21]. As such, the overall effects of EBCR in the
elderly have been the focus of heightened interest [14, 22].
Beyond classical parameters such as the pVO, others have emerged as to try
to provide a broader view of the CV system [9]. Among these, peak circulatory
power (CP) has been reported as an interesting CPET parameter, being a
non-invasive surrogate of the peak exercise cardiac power [9, 23, 24]. This
parameter, which incorporates both pVO and systolic arterial blood pressure
(SBP), provides data on both central and peripheral components of cardiac work,
and can thus be of interest as to provide a more comprehensive and integrative
view on the CV response to exercise [23, 25]. While this parameter has previously
been studied in individuals with coronary artery disease (CAD) and in heart
failure (HF), data pertaining to the effect of EBCR (particularly in older
individuals) remains elusive [10, 23, 26, 27]. Given this background, in the
present study we aimed at assessing the effect of an EBCR programme on CP in AMI
survivors, and specifically to assess the impact of age on this parameter.
2. Methods
This was an observational, retrospective cohort study. The eligible population
comprised all patients discharged from the Cardiology Department of the
Gaia/Espinho Hospital Centre with the diagnosis of an AMI (according to the
International Classification of Diseases, 9th Eition), between November of 2012
and April of 2017. To be included in the study, patients had to have completed a
phase II EBCR programme (including at least two assessments in a consultation
with a physical medicine specialist and performance of a CPET at the beginning
and at the end of the programme) after discharge. The study was approved by the
local Institutional Ethics Committee.
2.1 EBCR protocol
The EBCR programme has been previously described [15, 28, 29]. Briefly, this
encompassed a predefined 8-week (three sessions per week) outpatient protocol.
Before starting, patients were clinically assessed and underwent a CPET [14].
Training intensity was individually prescribed by an expert in EBCR (taking into
consideration the heart rate obtained during CPET) [20, 28, 30].
2.1.1 Cardiopulmonary exercise testing
Patients underwent a symptom limited CPET on a treadmill (Mortara XScribe;
Mortara Instruments, Milwaukee, WI, USA) using either a modification of the Bruce
protocol or a variation of this protocol (in highly deconditioned patients) [15].
CP (expressed in mmHg mL/kg/min) was defined as the product of pVO
(mL/kg/min) and peak SBP (mmHg) [9, 23]; the VE/VCO slope (a measure of
ventilatory efficiency, incorporating minute ventilation and VCO) was
derived by automatic linear regression from values obtained during the CPET [9, 10]. Data related to pVO and the respiratory exchange ratio (RER) have been
previously reported [20]. Patients were not asked to discontinue beta-blockers
before the test.
2.1.2 Clinical and analytical variables
As previously detailed, patients were categorized according to age: 65
years-old (younger group) or 65 years-old (elderly group) [20].
Data were collected for clinical, analytical, and echocardiographic variables
according to the electronic health records (EHR). Arterial hypertension was
defined according to the presence of this diagnosis in clinical files.
Dyslipidaemia was defined according to previous diagnosis, or the use of
antidyslipidaemic medication prior to admission, or by having a low-density
lipoprotein cholesterol 190 mg/dL [3]. Diabetes mellitus was defined
according to previous diagnosis, or the use of antidiabetic agents prior to
admission, or by having a glycated haemoglobin 6.5% [30]. Arterial
hypertension, dyslipidaemia and diabetes mellitus were categorized as present or
absent, in accordance with these criteria. Left ventricular ejection fraction was
evaluated by the biplane Simpson’s method, according to pre-discharge assessment.
2.2 Statistical analysis
Continuous variables were presented as mean standard deviation or as
median [percentile 25–75, interquartile range (IQR)] according to the
distribution. Categorical variables were expressed as absolute count (as well as
percentage). Continuous variables were compared using unpaired or paired
t test for those with normal distribution, or with the Mann-Whitney or
Wilcoxon tests (for unmatched and matched data, respectively). The comparison of
categorical variables was performed with the test. The normality
of the distribution was analysed with the Kolmogorov-Smirnov test. The Spearman
correlation was used to assess the relationship between CP and the VE/VCO
slope. Linear regression analysis was used to assess if age (being 65
years-old) was a significant predictor of the change in CP irrespective of
potential confounders. Sex, prior history of CAD, number of EBCR sessions, Killip
classification, the presence of arterial hypertension, the presence of
dyslipidaemia, the presence of diabetes mellitus, smoking status, and the
baseline CP were forced into the model. Given that, as previously reported, RER
values differed between age groups (as detailed in the Discussion), baseline RER
was also included in the model [20]. Results were two-sided, and a p value below
0.05 was considered as significant. Statistical analysis was done using Stata 14
(Stata Corp, College Station, TX, USA).
3. Results
The overall study population and baseline characteristics have been previously
described [20]. Briefly, a total of 379 patients (81% male gender, mean age 58.8
10.6 years-old, 67% after a ST-segment elevation MI) were included in
this study, of whom 30% were 65 years-old upon discharge (Table 1).
Table 1.Study population characteristics.
|
Younger group (n = 266) |
Elderly group (n = 113) |
p-value |
| Age (years) |
53.5 7.0 |
71.5 5.7 |
0.001 |
| Male sex |
209 (79%) |
98 (87%) |
0.064 |
| STEMI |
187 (70%) |
68 (60%) |
0.055 |
| Revascularisation |
239 (90%) |
96 (85%) |
0.174 |
| Killip classification |
|
|
0.001 |
|
1 |
230 (87%) |
79 (70%) |
|
|
2 |
27 (10%) |
23 (20%) |
|
|
3 |
2 (1%) |
9 (8%) |
|
|
4 |
5 (2%) |
2 (2%) |
|
| History of CAD |
32 (12%) |
28 (25%) |
0.002 |
| Arterial hypertension |
120 (45%) |
83 (73%) |
0.001 |
| Dyslipidaemia |
151 (57%) |
82 (73%) |
0.004 |
| Diabetes mellitus |
59 (22%) |
41 (36%) |
0.004 |
| Smoking status |
|
|
0.001 |
|
- Current smoker |
150 (56%) |
23 (20%) |
|
|
- Former smoker |
44 (17%) |
30 (27%) |
|
| Body mass index |
26.8 3.6 |
26.6 3.1 |
0.569 |
| Ejection fraction (%) |
52 (44–56) |
51 (45–57) |
0.956 |
|
- Acetylsalicylic acid |
263 (99%) |
113 (100%) |
0.257 |
|
- Clopidogrel |
151 (57%) |
75 (66%) |
0.081 |
|
- Ticagrelor |
111 (42%) |
34 (30%) |
0.033 |
|
- Anticoagulants |
12 (5%) |
15 (13%) |
0.002 |
|
- ACEi/ARA |
258 (97%) |
107 (95%) |
0.277 |
|
- BB |
252 (95%) |
101 (89%) |
0.059 |
|
- Spironolactone |
31 (12%) |
19 (17%) |
0.174 |
|
- Diuretics |
32 (12%) |
38 (34%) |
0.001 |
|
- CCB |
11 (4%) |
22 (19%) |
0.001 |
|
- Nitrates |
16 (6%) |
30 (27%) |
0.001 |
|
- Nicorandil |
2 (1%) |
5 (4%) |
0.015 |
|
- Ivabradine |
1 (1%) |
1 (1%) |
0.532 |
|
- Anti-diabetic agents |
52 (20%) |
35 (31%) |
0.016 |
|
- Insulin |
11 (4%) |
4 (4%) |
0.786 |
|
- Statins |
264 (99%) |
113 (100%) |
0.355 |
| Number of EBCR sessions |
24 (17–26) |
20 (16–24) |
0.057 |
| Legend: ACEi, angiotensin-converting enzyme inhibitors; ARA, angiotensin II
receptor blockers; BB, beta-blockers; CAD, coronary artery disease; CCB,
calcium-channel blockers; EBCR, exercise-based cardiac rehabilitation; n, number
of subjects; STEMI, ST-segment elevation acute myocardial infarction.
Excluding insulin. |
Patients completed a median of 22 (IQR 16–25) ECBR sessions, with older
individuals attending an inferior number [20 (16–24) vs 24 (17-26), p =
0.057]. As previously reported, pVO differed between groups at both the
beginning and the end of the programme (19.68 5.63 vs 24.15 5.72 mL/kg/min and 20.47 5.61 vs 25.75
5.93 mL/kg/min, respectively, p 0.001 for both comparisons)
[20]. Peak SBP did not differ between groups at the beginning [150
(140–160) vs 150 (140–160) mmHg, p = 0.289] or the end of the
programme [150 (140–165) vs 150 (140–160) mmHg, p = 0.408], nor did
its variation (p = 0.341).
Overall, CP significantly improved after the EBCR programme (all patients: 3676
1120 vs 3434 1066 mmHg mL/kg/min, p 0.001; younger
group: 3911 1084 vs 3619 1034 mmHg mL/kg/min, p
0.001; older group: 3120 1006 vs 2999 1018 mmHg mL/kg/min,
p = 0.018). Older individuals, however, presented lower levels of CP at
both the beginning and the end of the programme (Table 2, Fig. 1). In addition,
this subgroup had a smaller improvement (delta) in CP when compared to younger
individuals (Table 2). The VE/VCO slope differed between groups at both the
beginning [30.0 (27.3–32.9) vs 28.3 (25.8–30.9), p 0.001] and the
end of the programme [29.8 (27.9–31.9) vs 28.2 (25.9–30.8), p 0.001] though no difference was present in terms of its variation (delta)
between groups (p = 0.367). No correlation was found between the
variation (delta) in CP and in the VE/VCO slope (Spearman’s =
-0.022; p = 0.680).
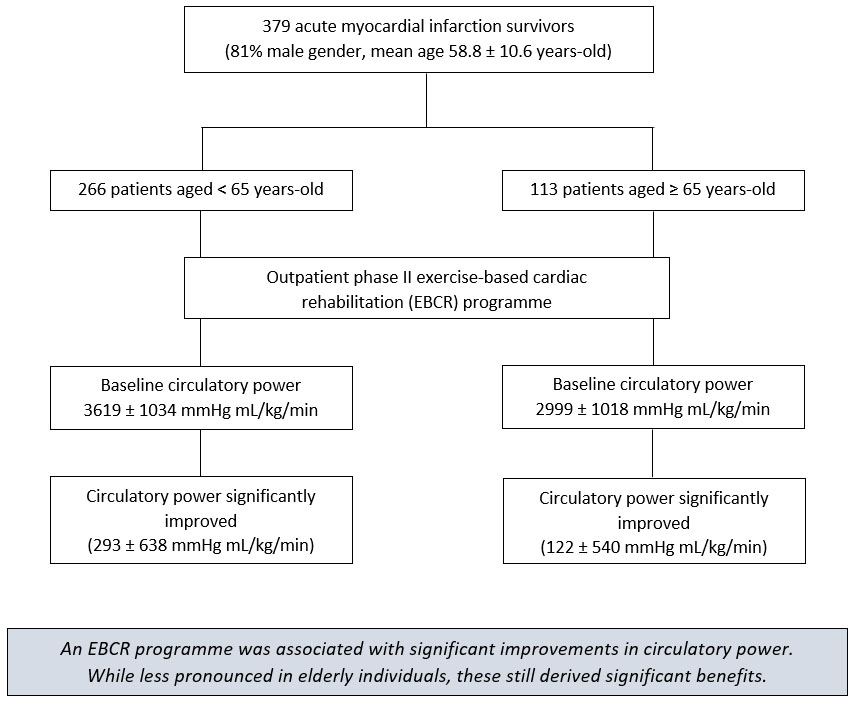 Fig. 1.
Fig. 1.
A contemporary EBCR programme was associated with significant
improvements in circulatory power (CP) among a group of AMI survivors. While the
elderly had lower CP levels at the beginning and the end of the program, and had
a smaller increase than younger patients, these still presented significant
improvements. These results highlight the relevance of these programmes among
these individuals.
Being aged 65 years-old was associated with a smaller improvement in CP
irrespective of sex, prior history of CAD, Killip classification, ejection
fraction, presence of arterial hypertension, dyslipidaemia, diabetes mellitus,
smoking status (current or former smoking), number of EBCR sessions and baseline
CP (Table 3). This result was maintained after inclusion of the baseline RER
(p 0.001). This was also maintained after inclusion in the model of
differences in medications at discharge (with an effect on blood pressure)
between groups, and after including all medications potentially influencing blood
pressure (i.e., angiotensin-converting enzyme inhibitors/angiotensin II receptor
blockers, beta-blockers, spironolactone, diuretics, calcium-channel blockers,
nitrates, nicorandil, ivabradine; p 0.001 for both models).
Table 2.Comparison between peak circulatory power among younger and
older patient groups at different stages of the exercise-based cardiac
rehabilitation programme.
|
CPET1 (younger group) |
CPET1 (elderly group) |
p-value |
| CP (mmHg mL/kg/min) |
3619 1034 |
2999 1018 |
0.001 |
|
CPET2 (younger group) |
CPET2 (elderly group) |
p-value |
| CP (mmHg mL/kg/min) |
3911 1084 |
3120 1006 |
0.001 |
|
Delta (younger group) |
Delta (elderly group) |
p-value |
| CP (mmHg mL/kg/min) |
293 638 |
122 540 |
0.013 |
| Legend: CPET1, cardiopulmonary exercise test at the beginning of the EBCR
programme; CPET2, cardiopulmonary exercise test at the end of the EBCR programme;
CP, peak circulatory power. |
Table 3.Multivariable linear regression analysis for the evaluation of
older age as a predictor of the change in peak circulatory power after an
exercise-based cardiac rehabilitation programme.
| Variables |
Coefficient |
Standard error |
p value |
| Sex |
267.474 |
88.706 |
0.003 |
| Age 65 years-old |
−309.428 |
77.935 |
0.001 |
| Ejection fraction |
41.403 |
70.281 |
0.556 |
| Arterial hypertension |
−72.074 |
67.512 |
0.286 |
| Dyslipidaemia |
131.219 |
68.217 |
0.055 |
| Diabetes mellitus |
−23.197 |
73.631 |
0.753 |
| Smoking status |
−28.980 |
38.881 |
0.457 |
| Number of EBCR sessions |
−0.658 |
4.716 |
0.889 |
| Killip class |
−87.193 |
55.904 |
0.120 |
| Previous history of CAD |
−119.542 |
95.022 |
0.209 |
| Baseline CP |
−0.209 |
0.036 |
0.001 |
| Legend: CAD, coronary artery disease; EBCR, exercise-based cardiac
rehabilitation; CP, peak circulatory power. |
4. Discussion
In the current study, AMI survivors submitted to contemporary EBCR (encompassing
aerobic and resistance training, in a background of optimal therapy) presented
significant improvements in CP. Though older patients had lower levels of CP and
had smaller increases across the programme, these still presented significant
improvements.
We have previously assessed the differential impact of an EBCR programme among
elderly individuals in terms of classical CPET parameters such as the pVO,
exercise test duration and the RER [20]. The current results on CP concur with
our previous observations, by depicting an overall gap between age strata, while
also reinforcing the beneficial effects of a contemporary EBCR programme among
both subgroups of patients [20]. Briefly, our prior data showed that although
older individuals had lower functional capacity (namely a lower pVO and
exercise duration), these also derived significant benefits from this
intervention [20]. In this analysis, we have focused on CP, a parameter which
could reflect the overall performance of the cardiac pump, and thus provide a
non-invasive estimate of the cardiac power [23, 31, 32]. Given the data reporting
the relationship between CP and CV events, we believe these results are of
relevance to the current literature on this topic. This parameter, first
described in 2002 by Cohen-Solal et al., has been mainly explored in the
setting of HF, where it has emerged as a potentially important component of the
overall CPET prognostic assessment [9, 23, 31, 32, 33]. Indeed, while the central role
of pVO in the assessment of CV disease is consensual [11, 14], CP has been
reported as being able to provide additional ancillary data, namely among
individuals with HF under beta-blocker therapy [34]. Interestingly, a recent
report by Lala et al. [32] on advanced HF patients found that
CP was a strong predictor of a composite outcome encompassing death, durable
mechanical circulatory support implantation or cardiac transplantation (at 1
year). Notably, whilst its assessment in the setting of HF has expanded over the
years, data on the impact of EBCR on CP remains to be further ascertained,
specifically in terms of data among elderly individuals [27, 35, 36].
Ageing is associated with several changes in both the CV system and other sites,
with decreases in overall functional capacity being described in different
clinical settings [37, 38]. This concept has been particularly studied in terms
of pVO, being also described in CP (which incorporates the former in its
calculation) [37, 39]. The fact that similarly to the results concerning
pVO[20], the differences in CP were maintained even after adjusting for
several potential confounders highlights the concept that these could (at least
partially) be attributed to differences in terms of the overall physiologic
response between groups. Furthermore, a higher CV burden in the background of
imbalances in terms of CV risk factors (such as arterial hypertension,
dyslipidaemia, and diabetes, significantly more prevalent in older individuals)
as well as of prior CAD could also be related to these findings. As reviewed by
Fleg et al. a plethora of CV changes (potentially modulated by risk
factor exposure) could be associated with pathological imbalances in the elderly,
whereas extra-CV adaptations should also be kept in mind [40, 41]. As elegantly
reviewed by Giallauria et al., ageing is a risk factor for frailty, a
multifactorial condition involving different mechanistic pathways and having
numerous manifestations, being associated with impaired quality of life, lower
functional capacity, and worse outcomes [18, 41, 42, 43, 44]. In this regard, data from
the SILVER-AMI study, assessing 3041 individuals aged 75 years-old with
an AMI, reinforced this notion by reporting that mobility impairment was able to
modulate the association between age and outcomes [18]. One analysis from this
study also showed that in-hospital mobility was an important predictor of
functional decline in this population [43]. Interestingly, a prior study on
elderly individuals, addressing the potential role of pre-infarction angina, also
showed that among patients with this clinical manifestation prior physical
activity could affect in-hospital CV outcomes [45]. Notably, and in accordance
with the current results, EBCR has been shown to be able to lead to significant
improvements in functional capacity among elderly individuals, reinforcing its
pivotal role in this higher risk subset of patients [20, 21, 36].
The current study assessed CP by a CPET, as a product of pVO and SBP, as
described in the current recommendations [9, 23]. Though the use of mean
arterial blood pressure has also been described, given the concordance between
measurements described by Hulkkonen et al. [24], we believe this should
not limit the interpretation of the current data. Differences in the RER should
also be taken into consideration [20]. However, while this differed between
groups, the mean values obtained (1.09 0.10 vs 1.09 0.13 in the
younger group; 1.05 0.11 vs 1.03 0.11 in the older group) as well
as the incorporation of this parameter in the regression model should not hinder
the overall assessment of the data on CP. Another point which should be
acknowledged relates to the lack of data on musculoskeletal parameters, which
could have influenced test termination and as such overall assessment. Given the
differences in terms of muscle mass and function associated with ageing, as well
as the potential role of exercise in mitigating these changes, further studies
should focus on these parameters, as to provide a broader overview on the
adaptations leading to functional impairment [14, 41, 46, 47]. In addition,
though the programme comprised 24 sessions, elderly patients completed a shorter
number (as shown in Table 1). This is in accordance with previous reports and
highlights the need for further strategies to promote both referral and overall
uptake of EBCR programmes in the elderly [16, 48, 49]. Though this point should be
acknowledged, given the lack of significant differences between groups and the
inclusion of this parameter in the regression model, this should not preclude the
interpretation of the overall results.
Interestingly, a seminal study reported on a correlation between CP and the
VE/VCO slope [50]. While differences in terms of overall patient
characteristics (particularly when considering functional capacity and ejection
fraction) should be taken into consideration, the current findings concerning the
VE/VCO slope reinforce the complexity of responses, while also reinforcing
the need for further data on the overall determinants of functional capacity in
this patient population. Finally, given the recently reported findings by
Anand et al. [51] on peak stress cardiac power (as assessed by
stress echocardiography) in terms of mortality and HF development among
individuals with an ejection fraction above 50%, it would be interesting to have
data on stress echocardiography. Given the morphological and functional changes
associated with ageing, additional echocardiographic parameters (encompassing
both left ventricular size and potential hypertrophy as well as diastolic
function) could also be of interest [28, 38, 40]. While these points should be
acknowledged and pondered with, the current results provide a pragmatic
assessment on the impact of a contemporary EBCR programme on CP among elderly
individuals, showcasing the relevance of this intervention among this challenging
group of patients.
5. Limitations
Several points should be taken into consideration when interpreting the present
results. As previously mentioned, this was a retrospective single-centre study,
including only those individuals who completed the EBCR programme, with no
control group [20]. While this should be acknowledged, prior data from randomized
controlled trials in the field should be considered in the face of this caveat
[27, 28]. Furthermore, patients were under optimized medical therapy (as shown in
Table 1), with most being submitted to revascularization. As such, generalization
of these findings to other settings should be done cautiously. Secondly, data
concerning parameters such as the presence of atrial fibrillation, renal
function, and haematological parameters (namely haemoglobin) were not available
for the current analysis [52]. Of note, measures of frailty could also be of
interest, as this syndrome could lead to limitations in terms of functional
assessments as well as EBCR uptake [42, 43]. In this regard, methodologies such
as the 5-meter gait speed test and the Timed Up and Go test have been proposed as
potential ancillary tools in the evaluation of these individuals [43, 44]. Given
these points, further studies focusing on these parameters could allow additional
tailoring of EBCR programmes among the elderly [14, 41, 44, 47]. Arterial
hypertension was defined (as described in the Methods section) according to the
presence of this diagnosis in the EHR. As such, some individuals under medication
due to left ventricular systolic dysfunction or angina could have been missed in
this categorization, whereas the lack of ambulatory blood pressure monitoring
could also have been of relevance, as to appraise the potential presence of
“white-coat” hypertension [4, 53]. Albeit these issues, the maintenance of the
present results after inclusion of different medications (which could affect
blood pressure) on the model should be considered, as further reinforcing the
current findings. Thirdly, we dichotomized patients as below or 65
years-old. As previously discussed [20], though several definitions have been
used to define elderly individuals, this cut-off was chosen given its utilization
in different studies [21, 36, 45, 53], with data reporting on its importance in
terms of events [54]. Whilst this, the fact that only 3.7% of individuals were
aged 80 years-old should be considered, as further studies should
specifically focus on addressing different responses according to age substrata.
Finally, data on CV outcomes was not present, as our aim was to assess the impact
of an EBCR programme on functional capacity, as expressed by CP. This
information, along with the incorporation of serial echocardiographic assessments
(namely stress echocardiography, as explored in the Discussion) should be the
focus of future research, as to refine the role of CP in this setting. We
believe, however, that while these hindrances should be pondered with, the
current study provides novel and relevant data on the CV response to a
contemporary EBCR programme among AMI survivors, with a special focus on elderly
individuals, thus providing a useful framework for further studies exploring the
relationship between CP improvements, potential EBCR programme design
personalization and overall CV events.
6. Conclusions
A contemporary ECBR programme was associated with significant improvements in CP
among AMI survivors. Patients aged 65 years-old presented significant
improvements in CP, though these were less pronounced than those among younger
individuals, even after adjustment for several potential confounding factors.
These results highlight the importance of EBCR among elderly individuals, given
its physiological and functional benefits, in this challenging higher risk group
of individuals.
Author contributions
EMV, AJ, ST, JR, LC, FM, MT were involved in the study’s conceptualization and methodology. EMV, MT were involved in the data collection. EMV, RLL, JPN were involved in the statistical analysis. EMV, RLL, MT were involved in the writing of the first draft. EMV, MT, JPN, RFC were involved in the review and editing of the study. All authors read and approved the final manuscript.
Ethics approval and consent to participate
All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the local Ethics Committee (approval number: 229/2017-1).
Acknowledgment
Not applicable.
Funding
This study received no external funding.
Conflict of interest
The authors declare no conflict of interest.
Availability of datasets
The datasets generated and/or analysed during the current study are not publicly
available.


 , Ricardo Ladeiras-Lopes 1,2, Ana João 1, Susana Torres 1, José Ribeiro 1, Lilibeth Campos 3, Fátima Miranda 3, José Pedro Nunes 4, Madalena Teixeira 1, Ricardo Fontes-Carvalho 1,2
, Ricardo Ladeiras-Lopes 1,2, Ana João 1, Susana Torres 1, José Ribeiro 1, Lilibeth Campos 3, Fátima Miranda 3, José Pedro Nunes 4, Madalena Teixeira 1, Ricardo Fontes-Carvalho 1,2