


1 Department of Neurosurgery, University Medical Centre Ljubljana, 1000 Ljubljana, Slovenia
2 Department of Neurophysiology, University Medical Centre Ljubljana, 1000 Ljubljana, Slovenia
3 Department of Physical and Rehabilitation Medicine, University Medical Centre Ljubljana, 1000 Ljubljana, Slovenia
4 National Institute for Rehabilitation, 1000 Ljubljana, Slovenia
Academic Editor: Piero Pavone
Abstract
Background: Spasticity is characterised by an atypical increase of muscle tone, affecting normal movements and interfering with the patient quality of life. The medicines may limit the effects of the disease and selective dorsal rhizotomy (SDR) can be used for selected cases or cases refractory to medicine. We present the surgical technique and the short-term results of this newly established surgical treatment in Slovenia. Methods: A retrospective analysis was performed of all patients that underwent the SDR from 2017 to 2019. The median follow-up was of 10 months. The following data have been collected: aetiology of spasticity, age at SDR, number of sectioned lumbar rootlets L1–S2, intraoperative disappearance of the H-reflex and intraoperative preservation of the bulbocavernosus reflex. The motor functions of all children have been classified by the Gross Motor Function Classification System (GMFCS) and Gross Motor Function Measure (GMFM-88). Twelve children underwent SDR, the median age at surgery was 9.6 years (min 3.9–max 16 years). Results: A mean of 57.8% of dorsal rootlets L2–S1 have been cut, while at level L1 50% of the dorsal roots have been routinely sectioned. The median amount of S2 rootlets cut was 14.3%. Postoperatively, we observed a sudden decrease in muscle tone. In all patients, there was an improvement of the muscle tone and of the gait pattern. The GMFM improved from 187.8 to 208.3 after a follow-up of 6 months. Conclusions: There was no complication in terms of wound healing, cerebrospinal fluid fistula of neurological dysfunctions. Despite the relatively short follow-up, our early results confirm the efficacy of the SDR.
Keywords
- Cerebral palsy
- Spasticity
- Selective dorsal rhizotomy
- Children
- Paediatrics
Spasticity is a motor disorder characterized by an increase in muscle tone that interferes with the mobility and therefore affects the quality of life [1]. It is most commonly encountered in children with cerebral palsy (CP), although it can be a leading symptom of numerous neurological disorders. It results from a lesion of the upper motor neuron, which regulates muscle tone control. Therefore, there is an imbalance of the signals between the central nervous system and muscles, which leads to an abnormal increase of muscle tone and to hyperirritability of myotatic reflexes [1, 2]. According to the affected limbs, CP can be divided into a hemiplegic, diplegic and tetraplegic type [3, 4]. Spasticity is most commonly associated with CP [5], which has an estimated prevalence ranging from 2 to 3 per 1000 live births [2]. The spasticity in CP usually becomes pronounced only after the age of 6 months and is evident by the end of the first year of life [3].
The management of spasticity in CP is still a great challenge for clinicians, despite the advances in medical care, rehabilitation medicine and surgical techniques [6]. The treatment of spasticity is important to reduce the muscle tone, improve the quality of life and reduce pain and deformations. Treatment can be directed toward (1) increasing the inhibitory activity on the muscle tone (with the action of drugs such as baclofen) and (2) reducing the efferent impulses that stimulate muscles and rise the abnormal muscle tone (with application of botulinum toxin) or with surgical procedures such as selective dorsal rhizotomy (SDR) [3, 7].
SDR is one of most commonly indicated surgical procedures to reduce spasticity in children with CP [8]. Technical advancements over the last two decades helped to reduce the invasiveness of the procedure and to improve the intraoperative neuromonitoring (IONM) techniques [6, 9, 10]. The best candidates are young children, older than 3 years, which are able to walk alone or with aids and for whom there is a potential improvement of the gait pattern after SDR [11]. Recently some Authors underlined the efficacy of SDR even in patients classified as Gross Motor Function Classification System (GMFCS) 4 or 5, for which it constitutes an alternative to intrathecal baclofen [12]. Since SDR requires a complex multidisciplinary approach, it is performed in relatively few centres [6, 13]. At the University Medical Centre Ljubljana, the SDR has been established as a standard surgical technique in 2017 and is since then included in routine clinical practice for children with CP. In this article, we present the surgical technique and the short-term results of this surgical treatment at our institution.
We retrospectively analysed data of all patients that underwent the SDR in the period from September 2017 to December 2019. All children had a preoperative multidisciplinary assessment to plan the best treatment modality and to plan the best sequence of therapeutic events, comprising SDR, soft tissue orthopaedic surgery, botulinum injection, tenotomy, and physiotherapy. The following data have been collected: aetiology of the spastic diplegia, age at SDR, number of sectioned rootlets L1–S1, amount of sectioned S2 rootlets, intraoperative disappearance of the H-reflex and intraoperative preservation of the bulbocavernosus reflex. Patients and their parents have given their written informed consent to be included in the study. The institutional review board of the University Medical Centre Ljubljana stated that this retrospective archive study does not need ethics approval.
There are several scales adopted to classify spasticity and functionality in children with CP [6, 7, 8]. The most commonly used are:
(1) Gross Motor Function Classification System (GMFCS) [14] (Table 1): gives a description of a child’s motor function and of which mobility aids a child need.
| GMFCS level | Clinical characteristics |
| Level I | Walks well in all settings. Balance and speed may be limited compared with children developing normally. |
| Level II | Walks in most settings but may have difficulty walking long distances or with balance. May utilise personal or environmental mobility aids to climb stairs. |
| Level III | Walks with the use of hand-held mobility aids such as K-walkers in most indoor settings. Uses wheeled mobility for longer distance travel. |
| Level IV | Utilises wheeled mobility aids in most settings (either attendant-propelled or powered) and requires assistance to transfer. |
| Level V | Transported in wheelchairs in all settings and has limited to no antigravity head, trunk and limb control. |
(2) Modified Ashworth Scale (MAS) [14] (Table 2): measures the resistance during passive soft45 tissue stretching.
| Ashworth grade | Degree of spasticity- clinical signs |
| 0 | No increase in muscle tone |
| 1 | Slight increase in tone giving a catch when the limb was moved in flexion or extension |
| 2 | More marked increase in tone but limb easily flexed |
| 3 | Considerable increase in tone - passive movement difficult |
| 4 | Limb rigid in flexion or extension |
(3) Range of Motion (ROM) [15]: measures the movements around a specific joint or body part.
(4) Gross Motor Function Measure (GMFM-88) [15]: assesses the motor activities in lying and rolling, sitting, crawling and kneeling, standing and walking, running and jumping.
All children have been routinely assessed preoperatively, one month after surgery and six months after surgery. The motor functions of all children have been classified by using the GMFCS and GMFM-88. The spasticity was evaluated by MAS.
The SDR was indicated for all paediatric patients where a potential amelioration of the motor function of the lower limbs was recognized, independently from the preoperative GMFCS and other measures. Before the SDR, all patients had a brain and spine MRI scan to exclude other impairments that could cause spasticity or impede the SDR procedure. The SDR procedure and intraoperative neuromonitoring techniques All SDR procedures have been performed using the same technique. A laminotomy was performed at the level of the medullary conus (usually L1) and then the dura was opened with a 15–20 mm long durotomy. The lateral sulcus between motor and sensory roots and the sulcus between S1 and S2 root have been recognized. First, half of the sensory root L1 were sectioned at the exit from the neuroforamen. After that, all sensory roots from L2 to S1 have been stimulated and then divided in 3 to 6 rootlets. Each rootlet has been stimulated separately and only those rootlets that showed a spastic activity have been cut. The stimulation was done with current ranges from 0.5 to 10 mA, determining the threshold response of each dorsal rootlet. Once the threshold was determined, a 1-second 50 Hz train was administered with the response monitored by the observation of electrical activity from needle electrodes implanted in the muscles of the lower limbs. Finally, the S2 has been examined. It has been recognized for being the last larger single-bundle nerve root exiting from the conus, above the smaller roots S3–S5. The S2 root has been stimulated and examined for the detection of the pudendal nerve root action potential. Only a small part of the root has been section, specifically the one with the lowest of absent detection of pudendal afferents. After closing the dura, the lamina has been fixed with titanium plates and the wound closed in layers. After surgery, the patients followed a strict rehabilitation protocol and were discharged to the University Rehabilitation Institute after 10 days. Afterwards, children were included in a long-term rehabilitation program and follow-up, which was structured in 3 separate months of intensive rehabilitation program during the first year and two separate months per year during the next years. Out of these periods, all children were included in every day physiotherapeutic practise.
Between September 2017 and December 2019, 12 children underwent the SDR. The main demographic data are summarized in Table 3. The median follow up was 10 months (min 1 month–max 27 months). Three children did not reach a follow up of 6 months. Eight patients were male, four were female. The median age for the SDR treatment was 9.6 years (min 3.9–max 16 years). All children had a spasticity related to CP, 11 of them had a diplegic type and 2 two had a tetraplegic form of CP. All children had some early postnatal complications, mainly an intraventricular/parenchymal haemorrhage or an ischemic impairment, which led to a periventricular leukomalacia. Nine of them were born prematurely (25th to 34th week of gestation).
| Age | PREOP GMFCS | PREOP GMFM-88 | 3 months follow-up | 6 months follow-up | % sectioned L2–S1 | % sectioned S2 | |
| Patient 1 | 14 | 3 | 184 | 192 | 206 | 53.3 | 15 |
| Patient 2 | 16 | 3 | 180 | 194 | 200 | 41.6 | 0 |
| Patient 3 | 8 | 2 | 258 | 265 | 274 | 58 | 0 |
| Patient 4 | 10 | 2 | 253 | 245 | 253 | 59.7 | 0 |
| Patient 5 | 3 | 2 | 202 | 198 | 231 | 58.3 | 20.8 |
| Patient 6 | 8 | 4 | 107 | 114 | 124 | 53.9 | 16.5 |
| Patient 7 | 9 | 1 | 188 | 244 | 245 | 59.2 | 8.3 |
| Patient 8 | 14 | 3 | 180 | 200 | 204 | 64.7 | 22.5 |
| Patient 9 | 6 | 4 | 127 | 142 | 143 | 63.1 | 8.3 |
| Patient 10 | 6 | 3 | 193 | 194 | NA | 57.4 | 25 |
| Patient 11 | 8 | 2 | 185 | 186 | NA | 54.8 | 29 |
| Patient 12 | 8 | 4 | 197 | 198 | NA | 69.9 | 26.5 |
The children have been distributed in GMFCS levels as follows: level I. 1 patient; level II. 4 patients; level III. 4 patients; level IV. 3 patients. Preoperatively, seven children were assessed by GMFM; they had reached in average 187.8 total points (min 107–max 258). All had in some extent lowered ROM, mostly in hips and knees. Spasticity was pronounced, with average MAS scores from 2.4 in gastrocnemius muscle to 0.4 in hip flexors.
At surgery, a mean of 57.8% of dorsal rootlets L2–S1 (min 41.6%–max 69.9%) have been cut (Table 3), while at level L1 50% of the nerve root have been routinely sectioned without the use of IONM. The median amount of S2 rootlets being sectioned was 14.3% (min 0%–max 33%), since the detection of pudendal dorsal root action potentials impeded a more extensive rate of sectioning. Intraoperatively, the H-reflex has disappeared and BCR have been preserved in all cases.
Postoperatively, we observed a sudden decrease in muscle tone. All children reported transitory paraesthesias along the lower limbs, which resolved within few weeks. Some needed lower doses of gabapentin in early weeks of postoperative rehabilitation. None of the patients had urinary control problems. The wounds were healing by primary intention and no signs of CSF leak were present. In the first weeks after surgery, the lower limb function and gait worsened, due to paraesthesias, loss of rigidity and postoperative pain. Children were routinely transferred to the rehabilitation hospital 10 days after surgery.
At three months of follow-up, there was already an improvement of the GMFM score, which was in average 197.6 (min 110–max 248). At six months follow-up, average scores of MAS were 0 for all evaluated muscles. All children had improved their gross motor functioning and in average achieved 208.3 points (min 147–max 249) in GMFM test (Fig. 1). All GMFCS grades improved in terms of GMFM testing, also children classified preoperatively as grades 4. Due to the small number of patients and due to the short follow-up, no statistical examination was done. We were also not able to confirm, if amelioration in grade 4 patients was comparable to patients with grades 2 and 3. In terms of improvement, we observed no changes in GMFCS during the follow up period.
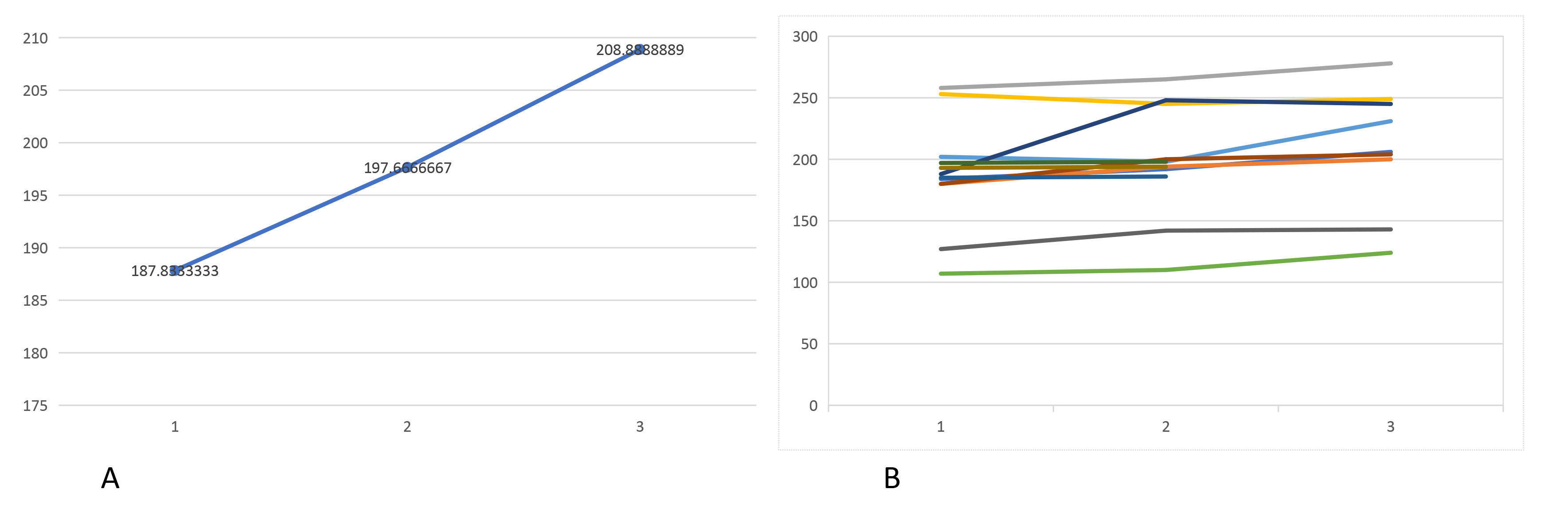 Fig. 1.
Fig. 1.Graphic presentation of the improvement of GMFM between the preoperative evaluation, and after 3 and 6 months of follow-up. The values in A are represented as a median range of GMFM, while graphic B shows the values of each patient separately. Note that three patients did not reach a 6 months follow-up.
Multiple evidences suggest that SDR reduces spasticity and improves ambulation in children affected by spastic diplegia. The technique is not new and it was first described in 1908 by Sherrington and Foerster [16]. Despite favourable results on muscle tone, they reported a significant postoperative morbidity because of sensory loss and ataxia, which resulted from total section of lumbar sensory roots. This has led to a temporary omission of the technique for several decades, until in 1978, Fasano described the selective section of the lumbar sensory roots [17], known as SDR. He disconnected only those fascicles that were causing a permanent and pathological contraction of the muscle during the IONM. Later, Peacock better defined the significance of the pathological response to the electrophysiological stimulation [18]. Since then, various modifications of the original surgical technique have been described [6, 9]. In particular, the one-level approach through a single level laminotomy allowed a much smaller skin incision, a less invasive procedure and decreased the rate of spinal deformities, that can occur after a L1–L5 laminectomy [19].
In the first months of life, the muscles are still loose and the typical signs of cerebral palsy may not be evident [2, 13]. Spasticity occurs later, usually after six months of age. The symptoms become more and more evident with child’s growth and may be diverse, ranging from almost undetectable clumsiness to severe disability. Typical symptoms, regardless of type, include abnormal muscle tone, balance disorders and abnormally lively tendon reflexes, often accompanied by involuntary movements [2, 4, 10]. The walk is unstable, usually patients walk on their toes or present a typical scissor pattern of walking. Because of the increased muscle tone, the deformation of bones and joints may also occur, progressively affecting the mobility [7, 20].
All these symptoms were observed also in our patients and were differing on severity among them. Postoperatively, subjective and clinical improvements were observed early after the surgery. Paraesthesias appearing in the form of tingling disappeared after a few days or weeks and with the help of intensive physiotherapy the joints range of motion and the gait pattern improved. We observed at 6 months follow up a GMFM improvement from 187.8 to 208.3. The aims of the SDR treatment include: improvement of child’s functional state (especially the pattern of walking), facilitation of the everyday care, prevention of the onset of contractures, deformations and pain [8, 9]. All these goals were achieved after the SDR in our series of patients.
The best prognostic factor for patients that undergo SDR is a good patient selection. The SDR is mostly suitable for children with spastic diplegia classified with GMFCS 2 or 3. These children are able to walk, or, at least, they have a potential for improvement of the lower limb motility [21, 22, 23]. In low degrees of spasticity (GMFCS 1), the daily activities are not disturbed to such degree, that the operation would bring any relevant relief, as with higher grades. Accordingly to these principles, the majority of our patients were classified as GMFCS 2 and 3. Additionally, age of the child is a very important prognostic factor [24, 25]. The SDR is ideal procedure from 4 to 8 years, as the growth and brain myelination are almost complete during this time. Rarely, the indication for SDR is justified after 15 years of age, when even with by means of intensive physiotherapy, strengthening the muscles and altering the pattern of walking appears difficult [19, 21].
We observed no early surgical complication, no CSF leak and no spine deformity. Furthermore, by using the detection of the dorsal root action potential at the level S2, we observed no permanent, nor transitory sphincter dysfunction. Future efforts will be directed toward a more detailed mapping of the pudendal afferents, by adopting not only penile and clitoridal electrodes, but also anal and intraurethral electrodes. Beyond this, the ideal amount of sectioned rootlets is far from being known. Sectioning less rootlets could better preserve the sensorial function, but whether it would also result in a less effective reduction of spasticity, remains a topic of discussion.
SDR has been started in 2017 at our Institution, which is the only one performing this surgical treatment in Slovenia, a country with 2 million people and around 40000 birth/year. Before 2017, children who needed SDR were addressed abroad. In this sense, the possibility of having the procedure performed in their own country and in a mother-language environment is of paramount importance for children and their families. SDR is part of national health insurance plan and is completely funded by the National health system of Slovenia.
A limitation of our study is the lack of a longer follow up. SDR results are usually more defined after a follow up of 2 years. Despite this, our early results show that SDR is efficacious and safe and this data will serve as a basic set of data for future case series.
SDR is an effective surgical treatment for spasticity in children with CP. Our early results confirm the efficacy of the procedure, as demonstrated by the improvement of the GMFM from 187.8 to 208.3. We observed no surgical complications.
CP, Cerebral palsy; SDR, Selective dorsal rhizotomy; IONM, Intraoperative neuromonitoring; GMFCS, Gross Motor Function Classification System; MAS, Modified Ashworth Scale; ROM, Range of Motion; GMFM, Gross Motor Function Measure.
All authors contributed equally. PS, TV and KG analysed the data; PS, ZR, RB and NK wrote the paper.
The consent to participate in the study was obtained with the informed consent of all participants. The institutional review board of the University Medical Centre Ljubljana stated that this retrospective archive study does not need ethics approval.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest. TV is serving as one of the Guest Editors of this journal. We declare that TV had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to PP.