

 , Cynthia F. Corbett 1,2, Robin M. Dawson 1,2, Michael D. Wirth 1, Bernardine M. Pinto 1,3
, Cynthia F. Corbett 1,2, Robin M. Dawson 1,2, Michael D. Wirth 1, Bernardine M. Pinto 1,31 College of Nursing, University of South Carolina, Columbia, SC 29208, USA
2 Advancing Chronic Care Outcomes through Research and iNnovation (ACORN) Center, College of Nursing, University of South Carolina, Columbia, SC 29208, USA
3 The Cancer Survivorship Research Center, College of Nursing, University of South Carolina, Columbia, SC 29208, USA
Abstract
Background: Fitness is a marker of physiological and mental health. The
purpose of this pilot study was to assess the feasibility of processes to recruit
women with polycystic ovary syndrome (PCOS) during the Covid pandemic and collect
their health and fitness data. Additionally, the data was used to explore
possible associations between anthropometrics, PCOS biomarkers, health-related
quality-of-life (HRQoL), and depressive symptoms with that of fitness and
self-reported physical activity levels among women with PCOS. Methods: A
convenience sample of women with PCOS (n = 15) were recruited via flyers and the
snowball method. Participants completed surveys, anthropometrics, a dual energy
x-ray absorptiometry scan, blood work, and a fitness assessment. Data were
statistically analyzed using Spearman correlations. Results: Feasibility
measures of recruitment and retention rates were 83% and 100%, respectively.
Fidelity measurement for process averaged 97%. Participants (age 25.9 (
Keywords
- polycystic ovary syndrome
- fitness testing
- fitness
- anthropometrics
- biomarkers
- aerobic capacity
- muscular endurance
Polycystic ovary syndrome (PCOS), the most common chronic endocrinopathy among women, has a prevalence that ranges between 15 and 20% [1]. Common signs/symptoms include subfertility, insulin resistance, dyslipidemia, hirsutism, and lethargy, placing women with PCOS at risk for comorbid conditions such as diabetes, cardiovascular disease, reproductive cancers, and depression and resulting in reduced health-related quality-of-life (HRQoL) [2]. Unfortunately, a PCOS diagnosis is often missed or delayed, as its presentation can widely vary, thus affecting treatment recommendations [3].
According to Rotterdam criteria, PCOS is diagnosed when two of three characteristics exist: clinical or biochemical hyperandrogenism, ovulatory dysfunction, and/or ultrasound evidence of polycystic ovaries [4]. Using all possible combinations, this heterogenous condition produces four phenotypes. For example, some women with PCOS may be obese, others lean and some women with PCOS may have hirsutism, while others may not. Such differences in physical presentation confound PCOS diagnosis and treatment. However, the risk for comorbid conditions holds constant regardless of phenotype due to factors such as central adiposity (affecting 50% of women) and dyslipidemia (affecting 70% of women), which are both independent of total bodyfat percentage [3, 5].
Lifestyle changes, such as exercise, are recommended as first-line treatment by the Endocrine Society Clinical Practice Guidelines for PCOS [4]. However, research indicates that less than 60% of women with PCOS engage in regular physical activity [5] and more than 25% are sedentary [6]. Fitness (the sum attributes of cardiorespiratory capacity, muscular strength and endurance, and flexibility), is a marker of physical and mental health and people who are fit have lower mortality from any cause as compared to those who are not fit [7]. To date, there are no research studies about fitness as an indicator of PCOS clinical features and health risk. As such, we conducted a pilot study to assess the feasibility of processes to recruit women with polycystic ovary syndrome (PCOS) and collect their health and fitness data. Additionally, the data was used to explore possible associations between anthropometrics, PCOS biomarkers, health-related quality-of-life (HRQoL), and depressive symptoms with that of fitness and self-reported physical activity levels among women with PCOS.
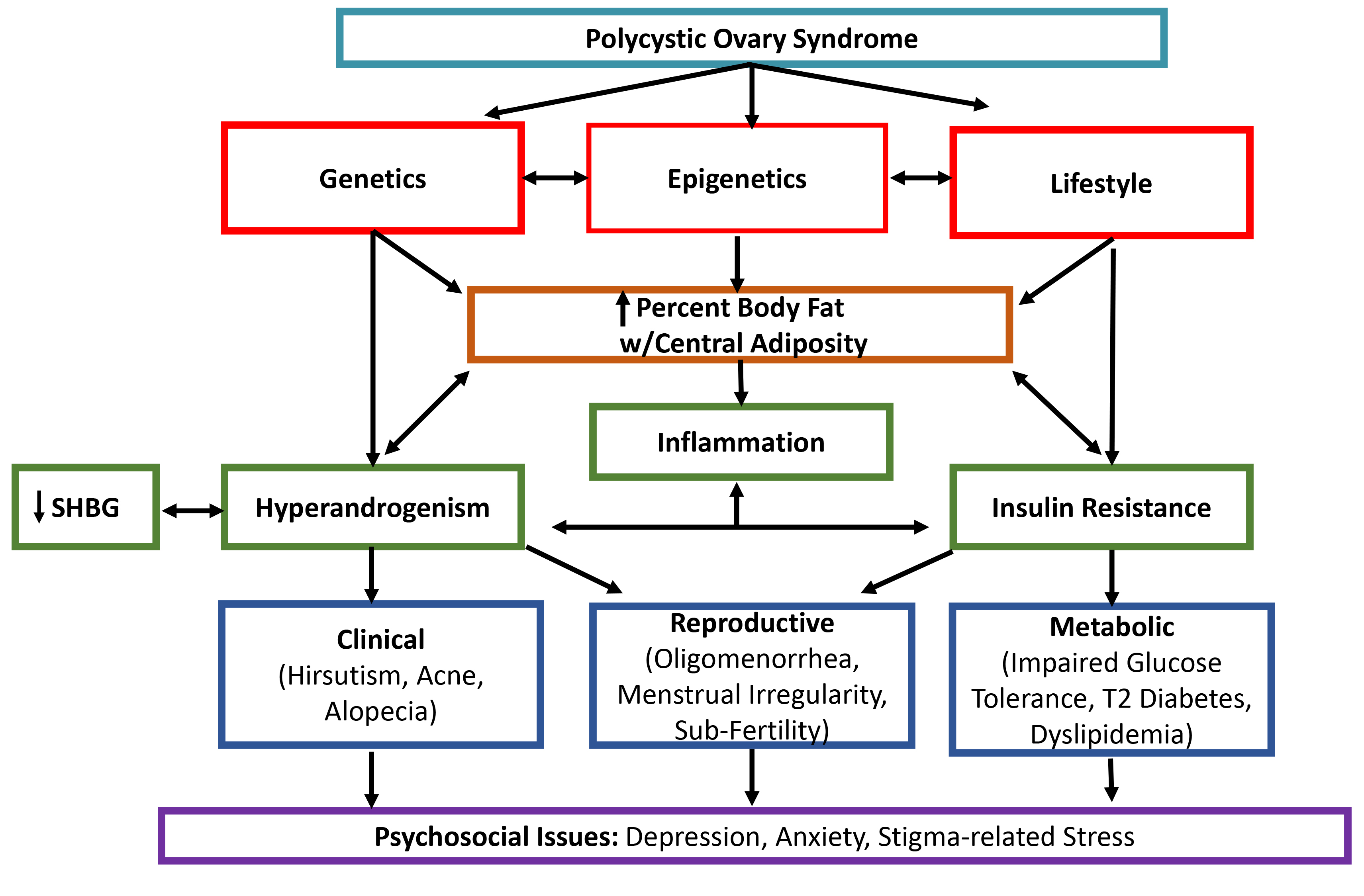
A theoretical PCOS physiological model guided this study (Fig. 1, Ref. [8]). PCOS is multifactorial, as genetic alterations, epigenetic modifications, and environmental factors contribute to development or worsening of the clinical manifestations [8]. Genetic origin of PCOS is confirmed by a hereditary factor observed in first-degree relatives, as women who have mothers or sisters with PCOS are at increased risk (35–40%) of developing the condition [9]. In addition to a genetic basis, epigenetic alterations (e.g., DNA methylation, noncoding RNA regulation) play a central role in PCOS outcomes, including phenotypic difference, by dynamically and reversibly controlling gene expression during childhood and into adulthood [8]. Environmental factors (e.g., nutrition, physical activity, smoking) combined with genetic predisposition can change the epigenome landscape leading to (epi)genetic susceptibility for developing PCOS throughout life [8].
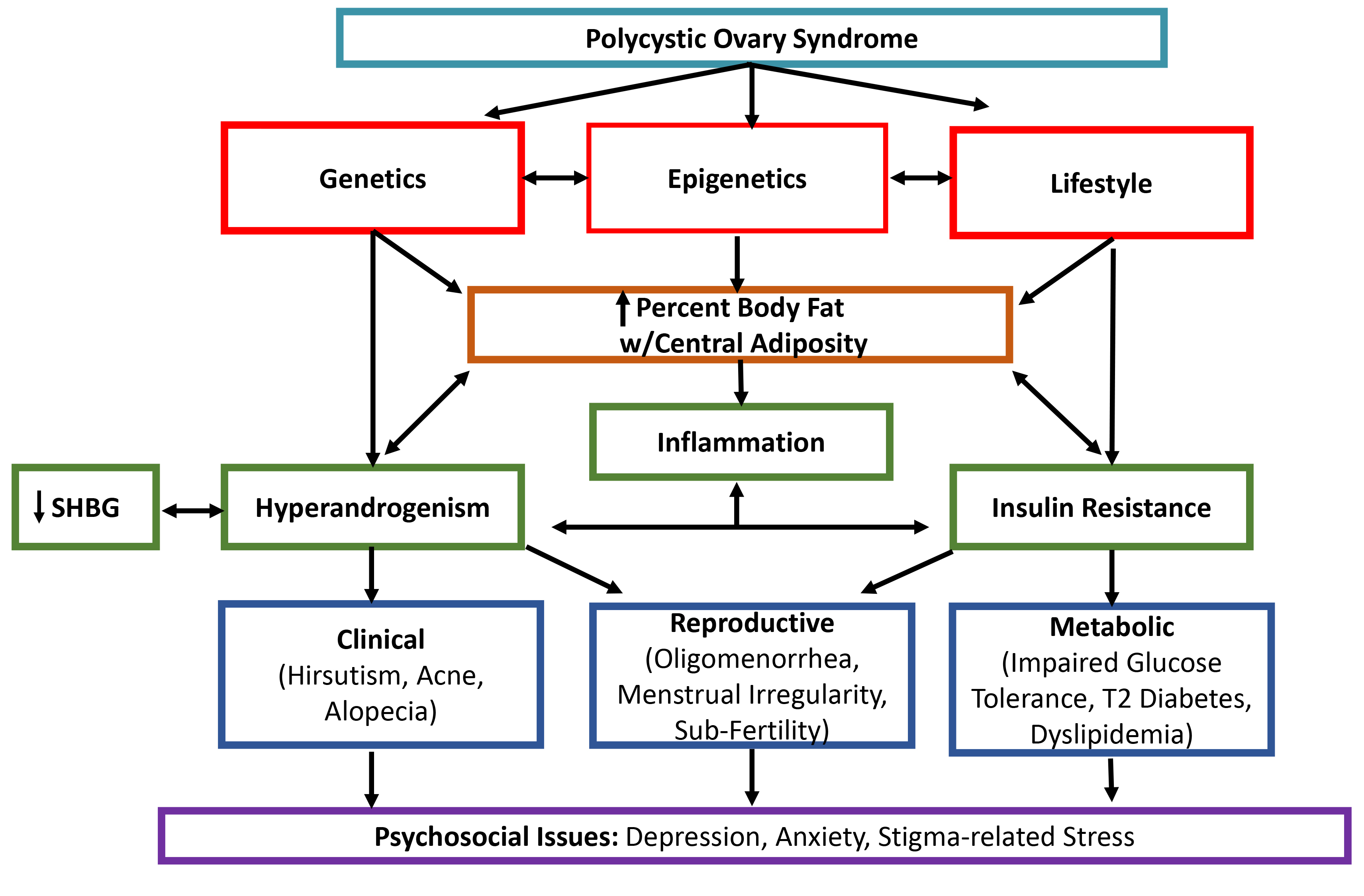 Fig. 1.
Fig. 1.Adapted (with permission) physiological model of polycystic ovary syndrome [8]. This model illustrates the interrelationships and outcomes of etiological factors and PCOS symptoms.
Obesity is a common characteristic of women with PCOS, and affects clinical manifestations such as hyperandrogenism, insulin resistance, and dyslipidemia [4]. Visceral fat, bodyfat located within the abdominal cavity, is a storage site for circulating androgen. Androgen is also present in plasma as free or unbound testosterone [4]. Further, hyperinsulinemia due to insulin resistance also contributes to excess androgen, as hyperinsulinemia decreases the total amount of sex hormone binding globulin (SHBG) [10], a glycoprotein that binds with androgen. Androgen is also produced in excess by the adrenal glands in most women with PCOS [4].
The investigator’s apriori target goal for sample size was based on a small
effect size and p
Feasibility measures included recruitment and retention rates and participant feedback. The recruitment rate was calculated by dividing the total number of participants who entered the study by the number of participants who answered the call for participants, and then multiplying by 100%. The retention rate was calculated by dividing by the number of participants completing all phases of the study by the number of participants entering the study, and then multiplying by 100%. Fidelity to process was measured using an apriori checklist, with results calculated by dividing the number of missed steps by the number of defined actions and multiplying by 100%. At the end of each fitness assessment, participants were asked three open-ended questions to obtain their feedback about the research process. A future full-scale study will be based on the feasibility of this pilot trial.
Anthropometric measurements included height (measured to nearest 0.1 cm
using a wall-mounted stadiometer), weight (measured twice and to nearest 0.1 kg
using an electronic scale), and waist and hip circumferences (measured
twice to nearest 0.1 cm using a measuring tape). Body mass index (BMI) was
calculated with the formula [BMI = weight (kg)/height (m)
After fasting for at least eight hours before the appointment, participants received venipuncture for a laboratory panel including free testosterone, SHBG, and lipid profile. Trained personnel followed standard protocol for venipuncture to collect approximately 10 mL of blood. The specimens were processed at Lexington Medical Center (West Columbia, SC, USA). Results were confidentially sent to the principal investigator’s university office. Free testosterone is used to diagnose androgen excess not due to other rare disorders [3]. SHBG is a PCOS and insulin resistance biomarker [10]. A lipid profile was collected to assess for dyslipidemia.
The demographic questionnaire included age, race, educational attainment, marital status, number of children, employment, insurance, geographic residence, and comorbid conditions.
PCOS-specific HRQoL was measured using the Polycystic Ovary Syndrome Questionnaire (PCOSQ-50). The PCOSQ-50 has been reported to have a construct validity of 0.92 and test-retest reliability of 0.91 [13]. It includes 50 items in six domains: psychosocial/emotional, fertility, sexual function, obesity/menstrual disorders, hirsutism, and coping. Answers are given on a 5-point Likert scale ranging from 1 = always (worst condition) to 5 = never (best condition). A score for each domain was calculated as the sum of all answered items in the domain divided by the number of answered items. The total PCOSQ-50 score was calculated as the sum of all answered items divided by the number of answered items. Lower scores indicate poor HRQoL [13].
The Rapid Assessment of Physical Activity (RAPA) was used to determine participants’ physical activity levels. The RAPA includes seven yes/no questions. The sum of “yes” responses indicates physical activity frequency, and intensity. The second section of the RAPA includes questions about the performance of resistance training and flexibility exercise. The RAPA has been reported to have good sensitivity (100%) and specificity (75%) for determining physical activity level [14]. Positive and negative predictive value for determining physical activity levels were 94.4% and 100% respectively [14].
The Personal Health Questionnaire (PHQ-8) was used to assess prevalence and
severity of depressive symptoms occurring within the past two weeks. The scale
consists of 8 items with a 4-point rating ranging from 0 (not at all) to 3
(nearly every day). A score of
The modified Bruce treadmill test was used to estimate maximal oxygen
consumption (VO
Using the American College of Sports Medicine (ACSM) protocol, the modified push-up test was used to estimate upper body muscular fitness. This test was chosen as a safer alternative than one-rep-max tests for sedentary or physically inactive participants and due to the availability of normative data. The test involves performing push-ups in a modified position (knees bent with lower legs in contact with the mat). The score is the total number of modified push-ups performed with proper form in one minute. The score was compared to gender- and age-based normative data. The norm-referenced test-retest reliability estimate using intraclass correlations from one-way analysis of variance (ANOVA) was R = 0.99 [16].
Using ACSM protocol, the curl-up test was used to estimate abdominal muscular fitness. This test was chosen as a safer alternative than one-rep-max tests for sedentary or physically inactive participants and due to the availability of normative data. In a supine position, the participant repetitively lifts and lowers the upper body to a metronome set at 40 beats/minute. The score is the number of curl-ups performed with proper form to cadence. The score was compared to gender- and age-based normative data. Psychometric findings included high test-retest reliability (r = 0.98), moderately high inter-apparatus reliability (r = 0.71), and moderately high inter-tester reliability (r = 0.76) [16].
Using ACSM protocol, the sit-and-reach test was used to assess hamstring flexibility. The test was chosen because it assesses the flexibility of several muscle groups with one movement and due to the availability of normative data. This measure was chosen because hamstring flexibility is related to low back and knee joint health. Participants sat against a wall with feet placed at the 15-inch mark on a measuring tape. Keeping knees straight and feet plantarflexed, participants reached forward with both hands. The score was the farthest distance reached of three trials. The score was compared to gender-and age-based normative data. The sit-and-reach test has shown a moderate mean criterion-related validity for estimating hamstring extensibility (r = 0.46–0.67) [16].
Analyses were conducted using IBM SPSS Statistics for Windows, version 27.0 (IBM
Corp., Armonk, NY, USA). Descriptive statistics (frequencies or mean
The feasibility of conducting health and fitness assessments of women with PCOS
was measured using recruitment and retention rates and participant feedback.
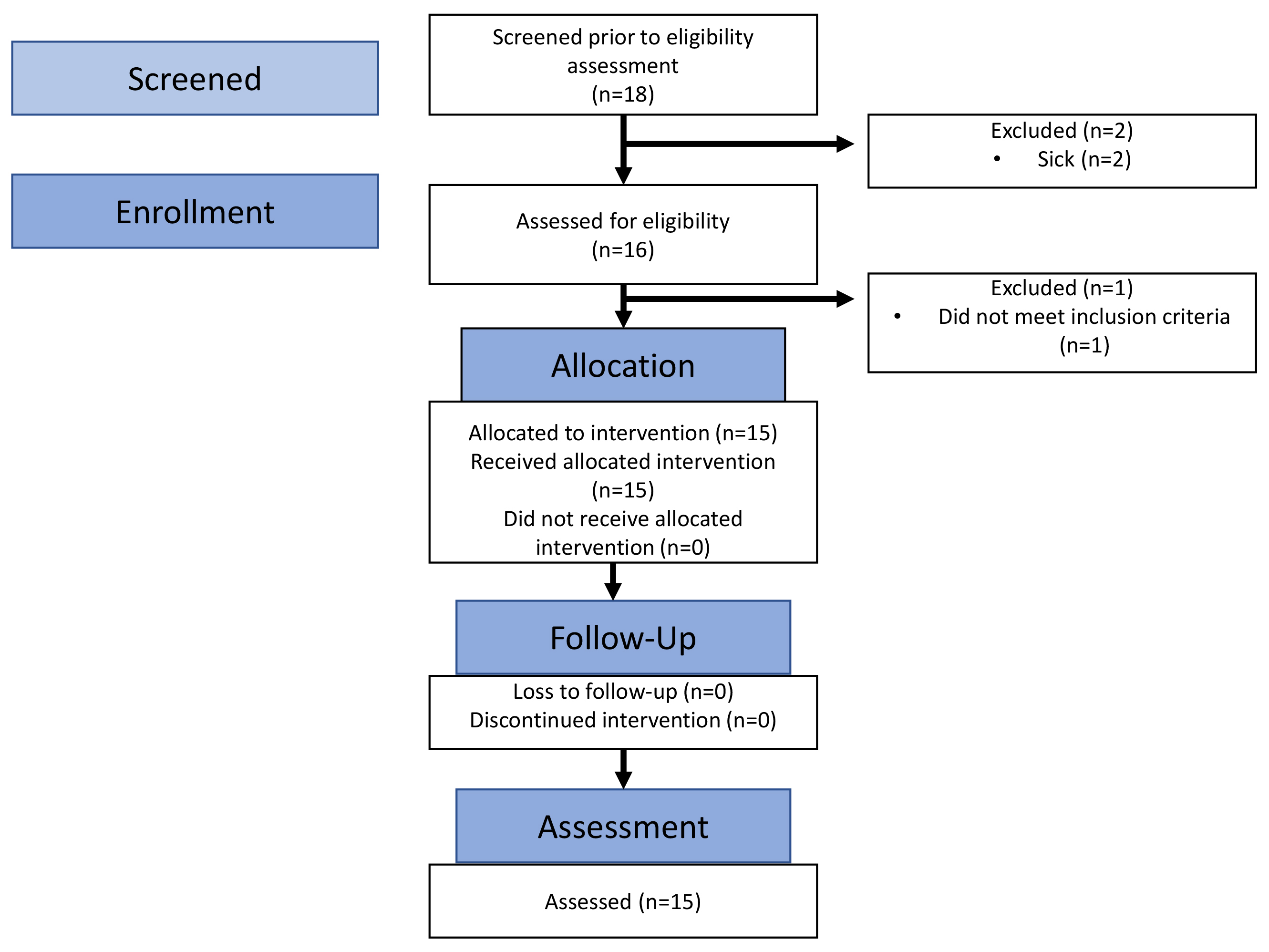
Eighteen women answered the call for participants, with 15 meeting eligibility
requirements for a recruitment rate of 83%. Fifteen women entered the study and
successfully completed all phases for a retention rate of 100% (Fig. 2). Using a
level of confidence at 95%, the margin of error for recruitment was 2%.
Anything between 0.61% and 1.00% (0.81
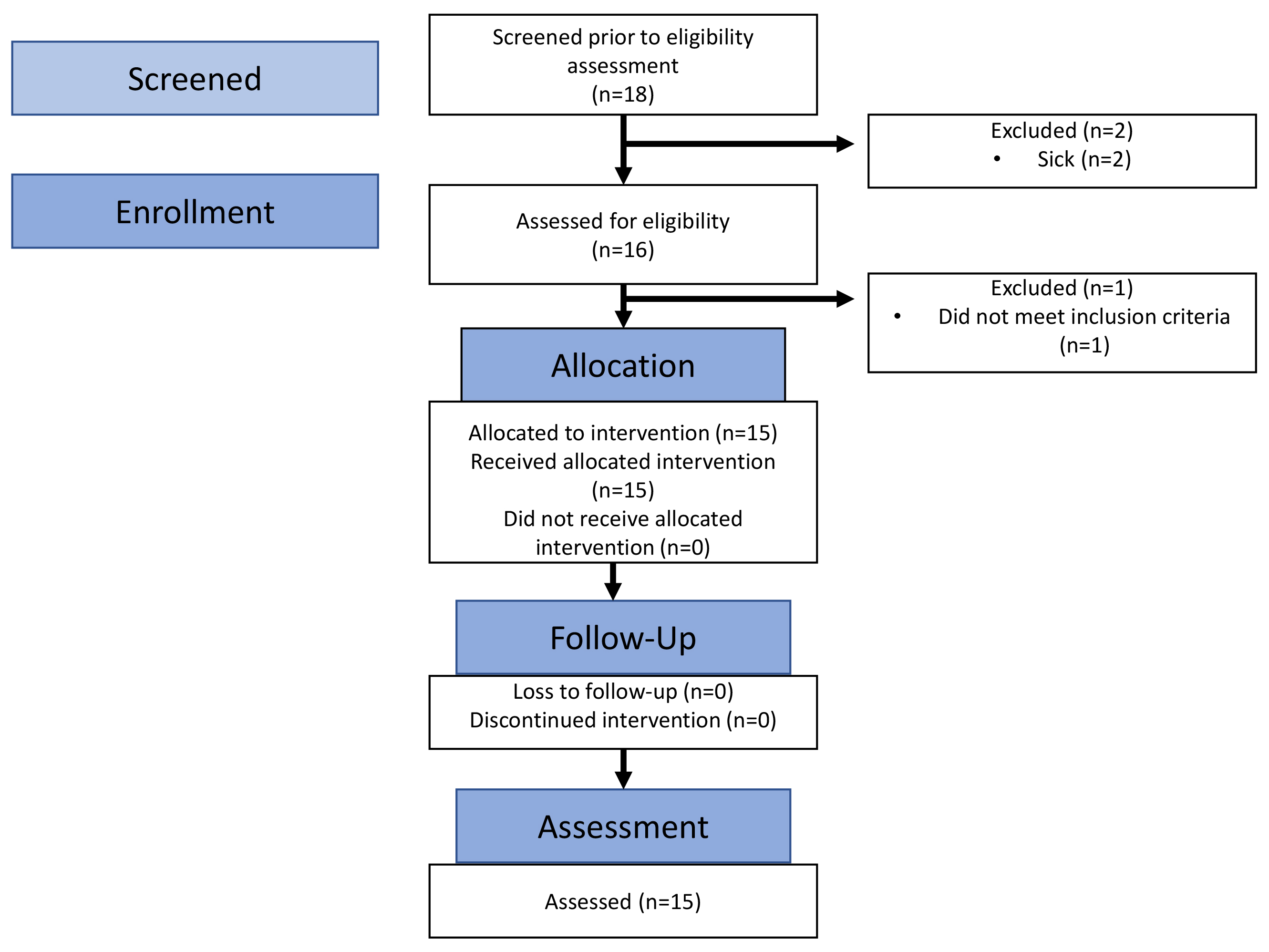 Fig. 2.
Fig. 2.Consort flow diagram of recruitment and retention.
The process for each participant progressed as planned and there were no adverse events. Fidelity to process was 96%. All participants expressed satisfaction with the study and seven participants (47%) requested their laboratory and fitness results. Participant feedback was positive, and no recommendations were made for improving the process.
Participants (n = 15) were 25.9 (
| Characteristics | Frequency (%) or Mean | |
|---|---|---|
| Age | 25.9 | |
| Ethnicity | ||
| African American or black | 0% (0) | |
| Hispanic, Latino/a, or Spanish | 13.3% (2) | |
| White | 80% (12) | |
| Mix of two | 6.7% (1) | |
| Educational attainment | ||
| High school or GED | 13.3% (2) | |
| Some college | 26.7% (4) | |
| Bachelors | 33.3% (5) | |
| Masters | 26.7% (4) | |
| Employment status | ||
| Not working | 13.3% (2) | |
| Part time | 20% (3) | |
| Full time | 66.7% (10) | |
| Medical insurance | ||
| Yes | 100% (15) | |
| Marital status | ||
| Single | 60% (9) | |
| Married or partnership | 40% (6) | |
GED, general educational development; SD, standard deviation.
| Variable | Reference values | Mean |
Descriptor | Sample # at risk |
|---|---|---|---|---|
| Body mass index (BMI) | 32.2 |
obese | 12 (80%) | |
| 18.5–24.9 (normal) | ||||
| 25–29.9 (overweight) | ||||
| Waist-to-hip ratio (WtH) | 0.81 |
moderate risk | 7 (47%) | |
| 0.81–0.84 (moderate risk) | ||||
| Percent bodyfat | 21–32% | 41.1 |
obese | 14 (93%) |
| Lean muscle mass | 98.07 |
low | 7 (47%) | |
| Free testosterone | 0.7–3.6 pg/mL | 7.6 |
high | 11 (73%) |
| Sex hormone binding globulin (SHBG) | 18–144 nmol/L | 23.0 |
normal | 6 (40%) |
| High density lipoprotein (HDL) | 40–59 mg/dL | 63.2 |
high | 3 (20%) |
| Low density lipoprotein (LDL) | 91.0 |
normal | 5 (33%) | |
| Triglycerides (TGs) | 93.0 |
normal | 1 (7%) | |
| VO |
Based on age | 36.8 |
fair | 5 (33%) |
| Upper body muscular endurance | Based on age | 15.4 |
Below average | 7 (47%) |
| Abdominal muscular endurance | Based on age | 21.3 |
Below average | 12 (80%) |
| Flexibility (inches) | Based on age | 18.8 |
average | 6 (40%) |
| Variable | Mean |
|---|---|
| HRQoL total | 3.3 |
| Psychosocial/emotional | 3.2 |
| Fertility | 3.9 |
| Sexual function | 3.3 |
| Obesity/menstrual | 3.1 |
| Hirsutism | 3.1 |
| Coping | 3.4 |
| Depressive symptoms total | 7.3 |
HRQoL, health-related quality-of-life; SD, standard deviation.
| Variable | VO |
Strength 1 | Strength 2 | Flexibility | RAPA 1 | RAPA 2 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (upper) | (abdominal) | (PA level) | (RT) | |||||||||
| R | p | R | p | R | p | R | p | R | p | R | p | |
| BMI | –0.49 | 0.07 | –0.29 | 0.29 | –0.66 | 0.01 | 0.40 | 0.14 | –0.63 | 0.12 | –0.06 | 0.82 |
| % Bodyfat | –0.59 | 0.02 | –0.44 | 0.10 | –0.61 | 0.12 | 0.22 | 0.43 | –0.72 | 0.00 | –0.09 | 0.74 |
| LMM | 0.09 | 0.01 | 0.20 | 0.01 | 0.69 | 0.01 | –0.91 | 0.01 | 1.21 | 0.01 | 0.51 | 0.01 |
| WtH | –0.06 | 0.83 | –0.05 | 0.86 | –0.28 | 0.32 | 0.15 | 0.60 | –0.47 | 0.08 | 0.25 | 0.36 |
| Test |
0.39 | 0.16 | 0.04 | 0.89 | –0.23 | 0.39 | 0.07 | 0.82 | 0.02 | 0.95 | –0.17 | 0.54 |
| SHBG | 0.73 | 0.00 | 0.26 | 0.34 | 0.33 | 0.23 | –0.00 | 0.99 | 0.20 | 0.47 | 0.10 | 0.74 |
| HDL | 0.16 | 0.57 | 0.14 | 0.63 | 0.59 | 0.02 | –0.48 | 0.07 | –0.02 | 0.95 | –0.46 | 0.08 |
| LDL | –0.03 | 0.91 | 0.12 | 0.67 | –0.20 | 0.49 | 0.08 | 0.77 | 0.33 | 0.23 | –0.52 | 0.05 |
| TGs | –0.43 | 0.11 | –0.11 | 0.69 | –0.14 | 0.62 | 0.09 | 0.75 | –0.47 | 0.08 | –0.17 | 0.54 |
| HRQoL | 0.72 | 0.00 | 0.36 | 0.19 | 0.36 | 0.62 | –0.42 | 0.12 | 0.28 | 0.32 | 0.13 | 0.66 |
| DepSx | –0.67 | 0.00 | –0.31 | 0.25 | –0.20 | 0.48 | –0.06 | 0.84 | –0.39 | 0.15 | –0.49 | 0.06 |
BMI, body mass index; LMM, lean muscle mass; SHBG, sex hormone binding globulin;
R, Pearson correlation; DepSx, depressive symptoms; HDL, high density
lipoprotein; PCOS, polycystic ovary syndrome; HRQoL, health-related quality of
life; LDL, low density protein; PA, physical activity; RT, resistance training;
Test
According to a review of funded and published randomized controlled trials,
successful recruitment is
VO
Consistent with studies in other populations, VO
VO
VO
VO
VO
Study participants had “below average” muscular fitness for age, a risk factor for musculoskeletal injuries and osteoarthritis due to poor posture and instability [32]. Evidence suggests that obese individuals have reduced maximum muscle strength relative to body mass compared to non-obese persons [33]. In this study, the three participants with a “normal” BMI scored average to above average on both muscular fitness tests. The two participants with the highest BMIs and percent bodyfat levels were unable to perform the curl-up test and scored poorly on the push-up test. More research is necessary to determine if bodyfat percentage is related to muscle activation and/or muscle morphology, such as muscle volume and architecture [34].
The relationship between abdominal fitness and obesity indices among women in general is not well studied. A cross-sectional study of healthy men and women aged 18–30 found that women had lower abdominal strength due to anatomical differences and higher bodyfat mass [35]. Findings from another cross-sectional study indicated that obesity had a significant negative impact on core muscular endurance among young adult men, regardless of which obesity measure was assessed [36]; however, a prospective study comparing normal-weight women with PCOS (phenotype D) to women without PCOS, using obesity indices, revealed that women with PCOS had lower muscle endurance than the control group of normal-weight women [30]. The researchers hypothesized that factors such as insulin resistance and visceral adiposity may damage muscle function in women with PCOS by slowing protein synthesis [26].
Women with PCOS and increased levels of lean muscle mass demonstrated strong and significant performance with abdominal strength. However, less than half of the women had normal to elevated lean muscle mass. This finding indicates that increased lean muscle mass can yield greater core strength, thus providing evidence for resistance training as a component of physical fitness. Resistance training studies for women with PCOS have resulted in improved strength measures, although core strength was not directly measured [37, 38].
Contrary to other research [39], the women in this study had high HDL, a
protective factor for cardiovascular disease. The finding of high HDL was
counter-intuitive, given the fair VO
Physical activity level had strong negative associations with percent bodyfat among the women with PCOS in this pilot study. Physical activity is defined as any bodily movement produced by skeletal muscles that requires energy expenditure [40], and thus includes all types of exercise.
The strong negative association between physical activity level and percent bodyfat is consistent with the literature. Many studies have revealed that performing regular aerobic exercise, especially of vigorous intensity, decreases bodyfat percentage over time [41]. This was true among women with and without PCOS [42]. Performing other modalities of physical activity, such as resistance training, also reduces percent bodyfat over time, especially at higher intensities and in presence of greater lean mass [43].
The performance of resistance training, as determined by RAPA, had a strong negative relationship with low density lipoprotein (LDL).
The negative association between resistance training and LDL is supported by the scientific literature. Research findings of a systematic review revealed that LDL decreased with resistance training, especially when the resistance training involved either an increased volume of movement (i.e., an increased numbers of sets and/or repetitions) or a larger load (i.e., weight lifted X repetitions X number of sets). All studies examining the differential effects of exercise types showed that resistance training had a greater impact on LDL (decrease) than either fewer sets or the isolated use of aerobic activity [44]. Other researchers reported that as little as one hour per week of high-volume resistance training, independent of aerobic activity, conferred a 40–70% lower risk for cardiovascular disease [45].
While increased lean muscle mass was inversely related to flexibility, we argue that those with lean muscle mass would also benefit from flexibility training, of which less than half participated. Fitness for anyone involves a holistic approach of cardiovascular, strength, and flexibility traing [46]. Despite debate [47], these authors hypothesize that full range of motion, provided by flexibility training, enables strength gains from resistane exercise.
This pilot study was conducted to assess the feasibility of conducting health and fitness assessments of women with PCOS. Possible associations between anthropometrics, PCOS biomarkers, HRQoL, and depressive symptoms among women with PCOS with that of fitness and self-reported physical activity levels were also explored. The study involved a convenience sample, thus minimizing external validity. The sample was small; however, there were several strong statistically significant associations between participants’ fitness levels and their biopsychosocial characteristics. A glucose tolerance test was not included in this study due to cost. However, an SHBG level, a marker of insulin resistance, and consequently, a predictor of diabetes was included [3]. Indirect fitness measures may result in less precision; however, indirect measures were chosen as safer alternatives for those women with PCOS who were sedentary or not regularly physically active. Self-report measures of physical activity can lack accuracy. Digital wearable devices will be considered in future studies. Lastly, information about medication-use was not collected and may have confounded results.
This pilot study had several strengths. Recruitment and process procedures flowed such that 15 women with PCOS were recruited within three summer months on a college campus during the Covid-19 pandemic when remote learning was mandated. The participants provided a medically confirmed PCOS diagnosis. Anthropometrics were precisely measured by trained professionals using established protocols and body composition was determined with DEXA, a gold standard for total body composition assessment [12]. The list of PCOS biomarkers was not exhaustive but representative, and it allowed for exploration of associations between fitness and health indicators. Biomarkers measured that specifically reflected the unique physiologic challenges of women with PCOS included free testosterone, SHBG (a marker of insulin resistance), and total lipid panel.
Randomized controlled trials in which health and fitness data are collected from women with PCOS are needed to confirm possible associations between fitness and PCOS clinical features. As such, the authors are currently planning to pilot a two-armed randomized controlled trial of an exercise intervention for women with PCOS to establish proof-of-concept [48]. We will incorporate the processes of health and fitness testing within the future study to compare pre-post results and between- and within-group differences between the intervention and control groups, while also assessing health and fitness as secondary outcomes.
In summary, the research team’s processes for recruitment and collection of health and fitness data from women with PCOS met feasibility parameters. Given the small sample size of this process feasibility study, the authors recognize the opportunities to expand recruitment efforts (e.g., social media and referral networks) and the battery of biomarkers (e.g., fasting serum glucose). Data from fitness assessments may help identify PCOS clinical features, and thus help reveal possible health risks among women with PCOS. Research evidence, although limited at this time, supports associations between fitness and health outcomes in other populations. The scientific literature also includes evidence that most types of physical activity confer hormonal or metabolic benefit when performed regularly and at higher intensities. This study supported current research and added associations between fitness indices and health outcomes not yet explored.
ACSM, American College of Sports Medicine; BMI, body mass index; DepSx,
depressive symptoms; DEXA, dual energy x-ray absorptiometry; HDL, high density
lipoprotein; HRQoL, health-related quality of life; LDL, low density lipoprotein;
PCOS, polycystic ovary syndrome; PA, physical activity; PHQ-8, personal health
questionnaire; RAPA, rapid assessment of physical activity; RT, resistance
training; SHBG, sex hormone binding globulin; Test
The dataset for this process feasibility study can be found via Open Science Framework at https://osf.io/8skdy/?view_only=67bee5c0dc4547df9cdac185fc71c425.
PJW conceived of the study idea. PJW and CFC designed the research study. PJW performed the research. PJW and MDW performed data analysis. PJW, CFC, RMD, MDW, and BMP worked together to interpret data. CFC and BMP provided supervision. PJW drafted the manuscript. CFC, RMD, MDW, and BMP provided revisions to the manuscript. PJW, CFC, RMD, MDW, and BMP gave final approval of the final version to be published. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Research protocols were approved by the University of South Carolina’s (USC) Institutional Review Board (Pro00106153). Written informed consent was obtained from each participant after explaining the study’s purpose, risk, and benefits.
The authors thank the women who participated in the study and appreciate the NIH National Institute of Nursing Research and the Center for Advancing Chronic Care Outcomes through Research and iNnovation (ACORN) in the College of Nursing at the University of South Carolina (USC) for support. The authors also thankful for the staff at the Clinical Exercise Research Center at the USC Arnold School of Public Health and for the laboratory services at Lexington Medical Center.
The study was made possible from the primary’s author receipt of an NIH Ruth L. Kirschstein National Research Service Award (NRSA) Individual Predoctoral Fellowship (1F31 NR019206-01A1).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.