



 , Nihal Callioglu 2
, Nihal Callioglu 21 Department of Obstetrics and Gynecology, Medipol University, 34197 Istanbul, Turkey
2 Department of Perinatology, Health Sciences University, Basaksehir Cam and Sakura Training and Research Hospital, 34197 Istanbul, Turkey
Abstract
Background: Pregnant women with late-onset fetal growth restriction
(LFGR) are at high risk of perinatal morbidity and mortality. However, it is
difficult to identify patients with a higher risk of adverse perinatal outcomes
at the time of diagnosing FGR. The aim of this study is whether
amniotic-umbilical-to-cerebral ratio (AUCR) is a better predictor than
cerebroplacental ratio (CPR) and umblicocerebral ratio (UCR) in detecting short
and long-term adverse perinatal outcomes (APO) in late-onset fetal growth
restriction. Methods: Retrospective cohort study, Doppler examinations
were performed between 35–37 weeks on pregnant women who were followed up in the
obstetrics and gynecology outpatient clinic of Nisa Hospital between April 1st,
2012, and April 1st, 2022, and were considered to have delayed growth according
to the Delphi consensus criteria. Sensitivity and specificity of measurements of
UCR, CPR, and AUCR for predicting a negative intrapartum or postpartum outcome
(fetal distress, Apgar score
Keywords
- umblicocerebral ratio (UCR)
- cerebroplacental ratio (CPR)
- amniotic-umbilical-to-cerebral ratio (AUCR)
Fetal growth restriction (FGR) is defined as the failure of the fetus to reach its growth potential. FGR is one of the leading causes of fetal morbidity and mortality [1]. FGR identified before 32 weeks is defined as early-onset, and FGR starting after 32 weeks is defined as late-onset fetal growth restriction (LFGR) [2]. Early-onset FGR (EFGR) is due to the reduced area of placental villous structures and is rarer than LFGR [3]. LFGR is due to impaired maturation of the villi rather than a reduction in placental surface area [3]. LFGR is associated with an increased risk of adverse perinatal outcomes (APO) such as hypoxemic events and mild neurodevelopmental delay in the short and long term compared with normally grown fetuses. Early recognition of LFGR in the second half of pregnancy is very important for predicting and preventing complications.
In the face of hypoxia and increased placental resistance, fetal cerebrovascular vasodilation occurs and this mechanism is called the brain-protective effect. Studies show that this physiologic regulation, which is intended to protect the baby at the time of birth, may unintentionally harm the fetus [4, 5, 6].
Studies in the literature have reported that the evaluation of Doppler parameters to evaluate uteroplacental adequacy and fetal vascular adaptation to hypoxia plays an important role in the surveillance of the fetus [4, 5]. It is argued that umbilical artery (UA) and middle cerebral artery (MCA) Doppler measurements, the cerebroplacental ratio (CPR), which is defined as the ratio between MCA and UA pulsatility index (PI), and the umblicocerebral ratio (UCR), which is known as the inverse ratio, are more effective predictors is detecting fetal hypoxia and APO [6, 7].
Although both have been described at the same time, CPR has been extensively studied and is used more in clinical practice, and UCR has been studied less in FGR. However, a recent secondary analysis of the trial of umbilical and fetal flow in Europe (TRUFFLE) study [8, 9] found that in EFGR, UCR was a better predictor of neurodevelopment-free survival at 2 years than CPR [9]. In addition, in recent studies, it was reported that the amniotic-umbilical-to-cerebral ratio (AUCR), a new ratio obtained by dividing the single deepest vertical pocket (SDVP) by the UCR, was also effective in predicting perinatal adverse events [10].
Therefore, there is no consensus on which ratio should be preferred in the evaluation of fetal risk in [11, 12]. The aim of this study is whether AUCR is a better predictor than CPR and UCR in detecting short and long-term adverse perinatal outcomes (APO) in Late-onset Fetal Growth Restriction.
This retrospective cohort study was conducted by scanning the data obtained from
the file registration system of patients who were admitted to the obstetrics and
gynecology outpatient clinic of Nisa Hospital for pregnancy follow-up between
April 1st, 2012, and April 1st, 2022. The study was designed according to the
Declaration of Helsinki and was approved by our Institutional Review Board.
Ethics committee approval and hospital institution approval were obtained before
the study and written informed consent was obtained from the patients (Date: 18
April 2022, ethic approval number: E-10840098-772.02-2915). One hundred
eighty-five pregnant women who met the inclusion and exclusion criteria were
evaluated in the study. First, second, and third trimester Doppler ultrasound
information in the pregnancy follow-up files of all pregnant women was examined.
In our clinic, fetal follow-up is performed once in the first trimester, once in
the second trimester, once in the early third trimester, and once between 35–37
weeks of gestation, a total of 4 times with Doppler ultrasound. Fetal follow-up
is performed with weekly non-stress-test (NST) after 37 weeks in pregnant women
with no risk. Fetal follow-up was performed with weekly NST and number of fetal
movements (
The inclusion criteria for the study were women aged 18–40 years who underwent Doppler examinations for LFGR at between 35 and 37 gestational weeks.
Fetuses were considered to have late growth restriction according to only the Delphi consensus criteria [13]:
- Gestational age
- Abdominal circumference (AC)/estimated fetal weight (EFW) ratio
Or at least two out of three of the following:
- UA-PI
- AC/EFW
- AC/EFW crossing centiles
The exclusion criteria were maternal drug intake, preeclampsia, multiple
pregnancies, pregnancies with early-onset FGR, i.e.,
Pregnant women whose gestational age was determined according to the crown-rump
length (CRL) obtained in the first trimester were included in the study. All
Doppler measurements were made using Voluson devices (GE Medical Systems, Zipf,
Austria). Doppler parameters were set automatically. As our hospital routine,
measurement was evaluated from three or more similar and sequential waveforms, in
the absence of fetal tachycardia and with an insonation angle as close to
0
All socio-demographic data such as maternal age, body mass index (BMI), smoking, alcohol, socioeconomic status, parity and maternal diseases, and previous and current pregnancy data were evaluated.
Deliveries were managed according to the institution’s routine protocol, and
vaginal delivery was decided after 38 weeks in the absence of other
contraindications. Labor was induced in cases of an unfavorable cervix, by
administration of a slow-release vaginal prostaglandin E2 (10 mg). If the onset
of labor did not occur within 12 h, oxytocin induction was initiated. In cases of
a favorable cervix, artificial rupture of the membranes and oxytocin infusion
were used. Epidural anesthesia was not used in any patients during normal
deliveries. All patients received the same dose of oxytocin induction. There were
no pathologic findings in intrapartum fetal cardiotocography before oxytocin
induction in any patients. Indication for cesarean primary delivery for
non-reassuring fetal status was based on abnormal fetal heart-rate monitoring
with the presence of more than one non-reassuring criterion or any abnormal
feature, including a baseline of
The primary outcome of the study was to calculate the sensitivity and
specificity of UCR, CPR, and AUCR measurements in LFGR to predict negative
intrapartum outcomes (fetal distress, defined as the occurrence of emergency
cesarean section (CS) for fetal distress or non-reassuring fetal status, defined
as the presence of a pathologic cardiotocography tracings interpreted by
physicians according to the International Federation of Gynecology and Obstetrics
(FIGO) consensus guidelines on cardiotocography) or postpartum outcomes (Apgar
score at 5 minutes
In the analysis of the data, number (n), percentage (%), mean, standard
deviation, and minimum and maximum values were used. The normality of the data
was evaluated according to the skewness and kurtosis coefficient. Students’
t-test was used to compare the mean of two independent groups. Pearson
Chi-square test and Fisher’s exact test were used to compare the ratios in two or
more groups. Multivariate logistic regression analysis was performed for UCR,
CPR, and AUCR values. In the model using the Enter method, UCR, CPR, and AUCR
values explained 20.2% of APO according to Nagelkerke R Square (Nagelkerke
R
Table 1 presents the distribution of the descriptive characteristics of the
participants. The mean maternal age of the participants was 27.11
| Variables | All pregnancies (n = 184) | ||
| Demographic characteristics | |||
| Maternal age (Mean |
27.11 |
Range: 17–43 | |
| Gravidity (Mean |
1.97 |
Range: 1–10 | |
| Parity (Mean |
0.73 |
Range: 0–3 | |
| BMI (Mean |
28.56 |
Range: 19.53–44.15 | |
| Smoking (%) | |||
| No | 168 | 91.3 | |
| Yes | 16 | 8.7 | |
| Disease (%) | |||
| No | 159 | 86.4 | |
| Yes | 25 | 13.6 | |
| Systemic disease (%) | |||
| No | 159 | 86.4 | |
| Hypertension (HT) | 4 | 2.2 | |
| Hypothyroidism | 11 | 6.0 | |
| Epilepsy | 2 | 1.1 | |
| Gestational HT | 2 | 1.1 | |
| Asthma | 1 | 0.5 | |
| Anemia | 1 | 0.5 | |
| Gestational diabetes | 1 | 0.5 | |
| Rheumatic disease | 3 | 1.6 | |
| Fetal movement | |||
| Good ( |
174 | 94.6 | |
| Poor ( |
10 | 5.4 | |
| Prenatal Ultrasound and Doppler variables | |||
| MCAPI (Mean |
1.52 |
Range: 0.50–2.90 | |
| lUAPI (Mean |
0.93 |
Range: 0.54–1.55 | |
| Oligohydramnios (Single deepest pocket |
|||
| No | 155 | 84.2 | |
| Yes | 29 | 15.8 | |
| Uterine Artery Notch (%) | |||
| No | 170 | 92.4 | |
| Unilateral or bilateral | 14 | 7.6 | |
| Outcome parameters | |||
| Mean gestational age at birth in weeks (Mean |
37.19 |
Range: 35.6–38.0 | |
| Type of delivery (%) | |||
| Spontaneous vaginal delivery | 64 | 34.8 | |
| Cesarean section (CS) | 120 | 65.2 | |
| CS primary | 58 | ||
| CS secondary | 62 | ||
| 5th min Apgar (Mean |
8.54 |
Range: 6–10 | |
| Fetal distress | |||
| No | 150 | 81.5 | |
| Yes | 34 | 18.5 | |
| pH (Mean |
7.29 |
Range: 7.04–7.41 | |
| APO | |||
| No | 128 | 69.6 | |
| Yes | 56 | 30.4 | |
| Intensive care requirement (%) | |||
| No | 152 | 82.6 | |
| Yes | 32 | 17.4 | |
| Gender (%) | |||
| Female | 94 | 51.1 | |
| Male | 90 | 48.9 | |
| Mean birth weight in grams (Mean |
2388.18 |
Range: 1840–2800 | |
| UCR (Mean |
0.70 |
Range: 0.34–1.80 | |
| CPR (Mean |
1.61 |
Range: 0.56–2.98 | |
| AUCR (Mean |
67.90 |
Range: 7.50–176.59 | |
UCR, umbilicocerebral ratio; CPR, cerebroplacental ratio; AUCR, amnioumblicocerebral ratio; BMI, body mass index; MCAPI, middle cerebral artery pulsatility index; UAPI, umbilical artery pulsatility index; APO, adverse perinatal outcomes; SD, standard deviation.
Some 15.8% of the participants had oligohydramnios, 7.6% had unilateral or
bilateral notches, and 5.4% had poor fetal movement. Of the participants whose
mean gestational week of delivery was 37.19
In Table 2, a comparison of the descriptive characteristics of the participants
according to the presence of APO is given. The MCAPI value was statistically
significantly lower in the group with APO (p = 0.001), and the UAPI
value was significantly higher (p = 0.001). The UCR value was
statistically significantly higher in the group with APO (p
| Normal (n = 128) | APO (n = 56) | p value | ||
| Maternal age | 27.27 |
26.77 |
0.560 | |
| Gravidity | 2.05 |
1.79 |
0.204 | |
| Parity | 0.80 |
0.57 |
0.118 | |
| BMI | 28.52 |
28.66 |
0.850 | |
| Disease | ||||
| No | 110 (85.9%) | 49 (87.5%) | 0.776 | |
| Yes | 18 (14.1%) | 7 (12.5%) | ||
| Smoking | ||||
| No | 118 (92.2%) | 50 (89.3%) | 0.573* | |
| Yes | 10 (7.8%) | 6 (10.7%) | ||
| Fetal movement | ||||
| Good ( |
121 (94.5%) | 53 (94.6%) | 0.999* | |
| Poor ( |
7 (5.5%) | 3 (5.4%) | ||
| MCAPI | 1.51 |
1.34 |
0.001 | |
| UAPI | 0.91 |
1.07 |
0.001 | |
| Oligohydramnios (Single deepest pocket |
||||
| No | 107 (83.6%) | 48 (85.7%) | 0.716 | |
| Yes | 21 (16.4%) | 8 (14.3%) | ||
| Uterine Artery Notch | ||||
| No | 115 (89.8%) | 55 (98.2%) | 0.067* | |
| Unilateral | 13 (10.2%) | 1 (1.8%) | ||
| Gestational Age at delivery (weeks) median | 37.20 |
37.17 |
0.702 | |
| Interval scan to delivery: days, median (range) | 1 (0–2) | 1 (0–1) | 0.762 | |
| Type of delivery | ||||
| Spontane vaginal delivery | 52 (40.6%) | 12 (21.4%) | 0.012 | |
| Cesarean section | 76 (59.4%) | 44 (78.6%) | ||
| Emergency Cesarean section | 0 | 34 (60.27%) | ||
| 5th min apgar | 8.88 |
7.77 |
||
| Fetal distress | ||||
| No | 128 (100.0%) | 22 (39.3%) | NA | |
| Yes | 0 (0.0%) | 34 (60.7%) | ||
| pH | 7.31 |
7.24 |
||
| Intensive care requirement | ||||
| No | 127 (99.2%) | 25 (44.6%) | ||
| Yes | 1 (0.8%) | 31 (55.4%) | ||
| Sex | ||||
| Female | 70 (54.7%) | 24 (42.9%) | 0.140 | |
| Male | 58 (45.3%) | 32 (57.1%) | ||
| Mean birth weight in grams | 2387.03 |
2390.80 |
0.892 | |
| UCR | 0.63 |
0.86 |
0 | |
| CPR | 1.74 |
1.34 |
0 | |
| AUCR | 73.24 |
55.70 |
0.001 | |
Independent Samples t-test. Pearson’s Chi-square, *Fisher’s Exact Test, NA, Not available; UCR, umbilicocerebral ratio; CPR, cerebroplacental ratio; AUCR, amnioumblicocerebral ratio; BMI, body mass index; MCAPI, middle cerebral artery pulsatility index; UAPI, umbilical artery pulsatility index.
The AUCs for CPR, UCR, and AUCR were 0.70 (95% CI: 0.62–0.79), 0.70 (95% CI: 0.62–0.79), and 0.66 (95% CI: 0.58–0.75), respectively (Figs. 1,2,3) (Table 3).
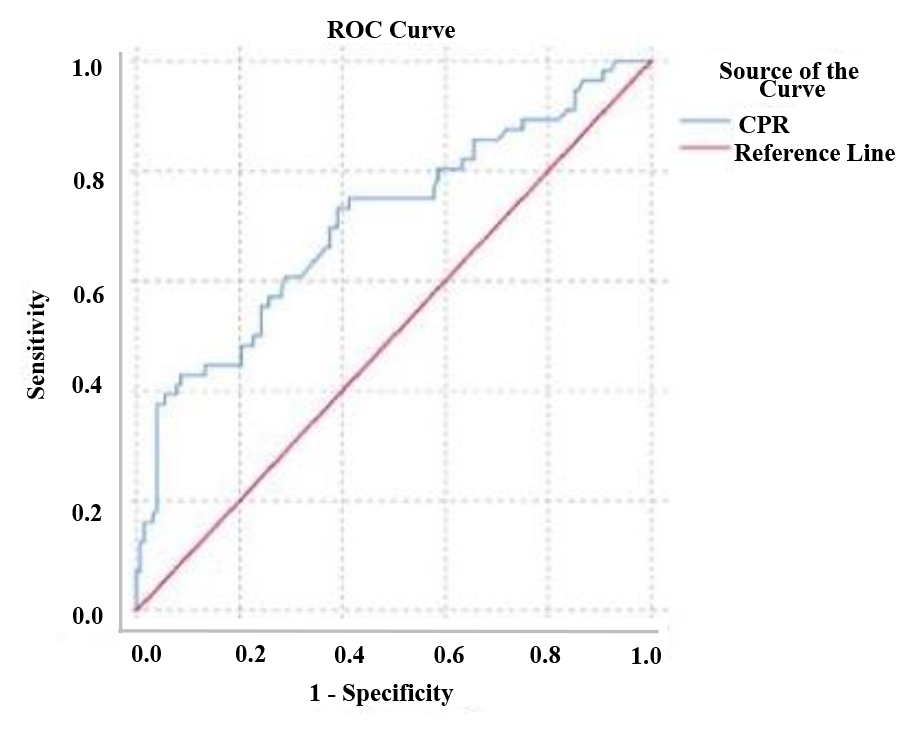 Fig. 1.
Fig. 1.Receiver operating characteristic (ROC) curve for prediction of perinatal outcome based on the cerebroplacental ratio (CPR) values.
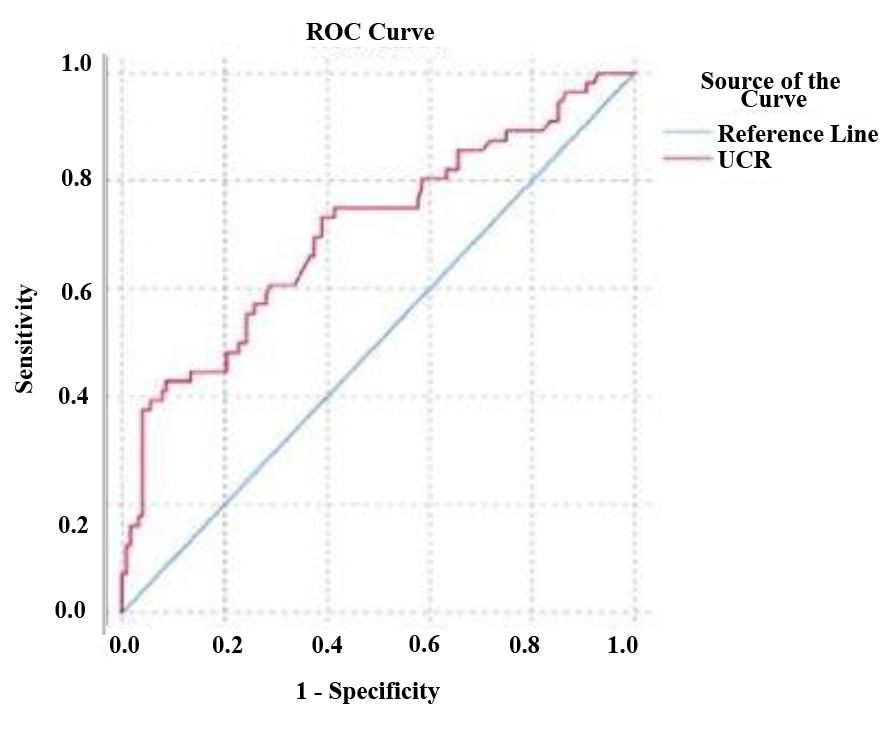 Fig. 2.
Fig. 2.ROC curve for prediction of perinatal outcome based on the umblicocerebral ratio (UCR) values.
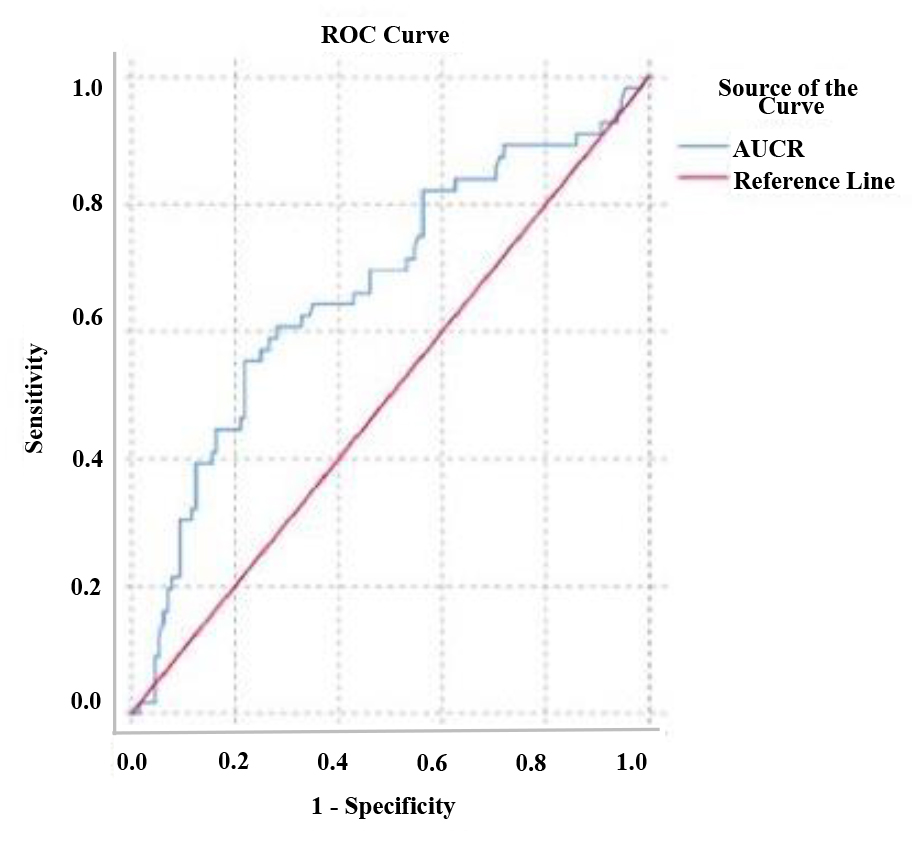 Fig. 3.
Fig. 3.ROC curve for prediction of perinatal outcome based on the amniotic-umbilical-to-cerebral ratio (AUCR) values.
| AUC (95% CI) | Cut off | Sensitivity (%) | Specificity (%) | p value | |
| UCR | 0.707 (0.621–0.792) | 0.6562 | 69.6 | 62.5 | 0.000 |
| CPR | 0.707 (0.621–0.792) | 1.5239 | 69.6 | 62.5 | 0.000 |
| AUCR | 0.668 (0.58–0.756) | 61.2500 | 64.3 | 64.8 | 0.000 |
CI, confidence interval; AUC, area under the curve; UCR, umbilicocerebral ratio; CPR, cerebroplacental ratio; AUCR, amnioumblicocerebral ratio.
Table 4 Multivariate logistic regression analysis of UCR, CPR, and AUCR in the
group with APO. There was no statistically significant correlation between CPR,
UCR, and AUCR Doppler parameters in fetuses with LFGR in terms of detecting APO
(p
| OR | 95% CI | p value | ||
| UCR | 1.640 | 0.473 | 3.510 | 0.630 |
| CPR | 1.557 | 0.235 | 3.301 | 0.646 |
| AUCR | 0.999 | 0.984 | 1.014 | 0.907 |
UCR, umbilicocerebral ratio; CPR, cerebroplacental ratio; AUCR, amnioumblicocerebral ratio; OR, odds ratio; CI, confidence interval.
Doppler ultrasound measurements play an important role in the early detection of APO in FGR. Increased placental insufficiency in FGR leads to a pathophysiologic distribution of blood flow, such as loss of fetal cerebral blood flow advantage and decreased renal perfusion [16]. The relationship with placental insufficiency in fetuses with LFGR is weaker than in fetuses with EFGR [16]. For this reason, umbilical artery Doppler findings are insufficient in detecting APO in LFGR [17]. In the study of Lees et al. [6], it was found that 20% of fetuses with LFGR with normal UAPI values had a decrease in MCAPI due to the brain-protective effect. It has also been reported that LFGRs with low MCAPI values are associated with fetal distress, stillbirth, and long-term negative neurologic development [18].
The CPR and UCR, the ratios between MCAPI and UAPI, were first described in
1987. It has been reported that these two ratios are more valuable than UAPI and
MCAPI alone in predicting high perinatal morbidity and mortality [19, 20]. CPR has
been used more often than UCR because it is more easily interpreted in clinical
practice [6, 19]. In fetuses with growth restriction, CPR was described as being
moderately to highly significant in the determination of perinatal morbidity and
mortality, and the strength of this relationship was found to be even higher in
the case of EFGR [7]. In this study, CPR was found to be statistically
lower in the group with APO compared with the other group. Intrauterine Growth Restriction, PORTO study, it
was found that the APO risk was 11 times higher in FGR with CPR
In the literature, there are few studies evaluating UCR in the early detection of APO. Whereas, in cases of placental insufficiency, because there is lower cerebral and higher umbilical artery impedance, the UCR tends to asymptote towards infinity, emphasizing the differences between abnormal values. CPR shows an asymptote tendency towards zero. Therefore, it can be hypothesized that the UCR is a more valuable ratio. In the secondary analysis of the TRUFFLE study, the relationship between MCA, CPR, and UCR in FGR was investigated, and it was found that UCR was a more valuable ratio than other Doppler parameters in determining the probability of being healthy without neurodevelopmental disorders (odds ratio (OR) = 0.88, 95% CI: 0.78–0.99) [8]. However, when the literature is examined, different results have been reported for both ratios. Some authors emphasize that the use of Doppler for APO in FGR is limited and there is no difference between CPR and UCR rates [7, 18, 24].
AUCR may be considered to have a positive effect on the prediction of APO because reduced renal blood flow in FGR leads to impaired fetal urine production and decreased AFV. Stumpfe et al. [10] found that the addition of SDVP to the UCR improved the predictive accuracy of negative outcomes in fetuses and that the estimation made using UCR was superior to CPR in their study with 165 term pregnant women with Small for Gestational Age (SGA). Although a statistically significant relationship was found between CPR, UCR, and AUCR and negative perinatal outcomes in fetuses with LFGR in this study, there was no statistically significant correlation between CPR, UCR, and AUCR in Doppler parameters in terms of detecting APO.
This study had some limitations. These included being a retrospective study, having a relatively small number of patients with APO, having Doppler findings measured by different physicians, obstetricians not being blinded to prenatal examination results, the cross-sectional single measure design that could not account for serial changes in Doppler indices, the evaluation of adverse intrapartum outcomes, and the use of cardiotocography alone to perform instrumental deliveries, which might overestimate the number of fetuses with actual fetal distress.
The use of close ultrasound modalities in the definition and follow-up of FGR, and being one of the few studies evaluating cases by combining Doppler parameters and amniotic fluid volume were among the strengths of the present study.
A low AUCR and CPR, a high UCR were significantly associated with APO in fetuses with late-onset fetal growth restriction in this study. There was no difference in the diagnostic performance between AUCR, CPR, and UCR in predicting adverse outcomes. Further large prospective studies are needed to confirm these findings and ascertain whether combining different obstetric and fetal characteristics might improve the diagnostic APO in singleton pregnancies with LFGR.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
DKG and NC designed the research study. DKG and NC performed the research. DKG analyzed the data. Both authors contributed to editorial changes in the manuscript. Both authors read and approved the final manuscript. Both authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was designed according to the Declaration of Helsinki and was approved by Medipol University Review Board. Ethics committee approval and hospital institution approval were obtained before the study and written informed consent was obtained from the patients (Date: 18 April 2022, ethic approval number: E-10840098-772.02-2915).
We would like to express our gratitude to all those who helped us during the writing of this manuscript. Thanks to all the peer reviewers for their opinions and suggestions.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.