
 , Alessandro Bulfoni 2, Stefano Salvatore 1, Massimo Candiani 1
, Alessandro Bulfoni 2, Stefano Salvatore 1, Massimo Candiani 11 Obstetrics and Gynaecology Department, IRCCS San Raffaele Scientific Institute, 20132 Milan, Italy
2 Department of Gynaecology, Division of Obstetrics and Gynaecology, IRCCS Humanitas Clinical and Research Center, San Pio X, 20089 Milan, Italy
Abstract
Background: The Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome is the most common cause of uterine aplasia, with a worldwide frequency of 1 in 4500 females. Although abundant literature is present regarding the different available methods for creating a neovagina in MRKH syndrome, the attention dedicated to these women’s reproductive potential remains insufficient. Methods: Online searches were carried out in PubMed database during November and December 2020. The search included a combination of the various terms (e.g., MRKH, vaginoplasty, uterus transplantation, infertility treatment, gestational surrogacy, etc.). The following inclusion criteria were used: (1) The articles should be written in English or French language. (2) The article should have been published by an official scientific organization. Results: Until few years ago, the only option for women with MRKH syndrome was legal adoption, now gestational surrogacy (GS) and uterine transplantation (UTx) have become new fertility options available to these patients. Discussion: GS is officially recognized in several countries and widely practiced. On the other hand, UTx, although the great recent technical improvements, is far from being an option for all women with MRKH syndrome secondary to its complexity and the necessary immunologic therapies.
Keywords
- Mayer-Rokitansky-Küster-Hauser syndrome
- Assisted reproductive technology
- Gestational surrogacy
- Uterus transplantation
Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome is a congenital disorder characterized by agenesis of the Müllerian ducts (uterus and upper two-thirds of the vagina) in karyotypic normal females (46, XX), with normal external genitalia, and secondary sex characteristics [1]. MRKH syndrome occurs in approximately 1 in 4500 female live births. Despite being a rare disorder, it has been reported as the second most common cause of primary amenorrhea (after gonadal dysgenesis) and affects about 10% of women with primary amenorrhea [2]. MRKH syndrome is classified into two groups: typical/type I (isolated uterovaginal agenesis) and atypical/type II (additional abnormalities of the kidneys, skeleton, heart and auditory system). Type I MRKH represents 56–72% of the affected patients while the frequency of type II MRKH syndrome is 28–44% [3]. Some atypical MRKH syndrome cases also fulfill the criteria of Müllerian duct aplasia, renal aplasia, and cervicothoracic somite dysplasia (MURCS) [4]. The etiology of MRKH syndrome has not yet been clarified. As some evidence demonstrates a familial occurrence prompting researchers to investigate possible genetic causes [5].
Online searches were carried out in PubMed database during November and December 2020. The search included a combination of the various terms (e.g., MRKH, vaginoplasty, uterus transplantation, infertility treatment, gestational surrogacy, etc.).
The criteria for an article to be included for the review of the literature are:
• The research should be written in English or French or translated into this language from their original version.
• The article should have been published by an official scientific organization.
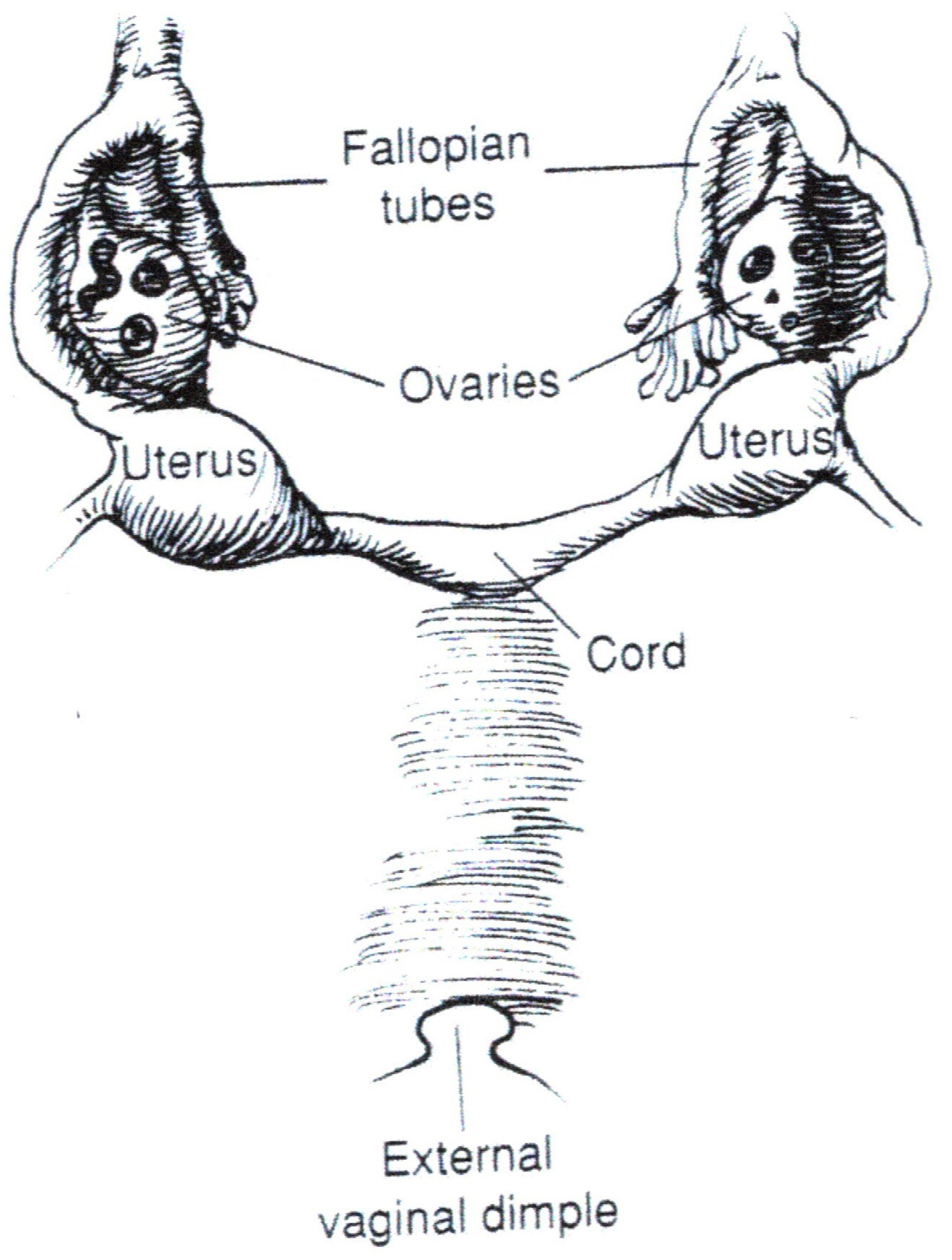
In patients with MRKH syndrome, the uterus is represented by bilateral rudimentary bulbs that vary in size, not usually palpable, connected to fallopian tubes, and are located on the lateral pelvic sidewall adjacent to the normal ovaries. Depending on their size, these rudimentary uterine bulbs may or may not contain a cavity lined by endometrial tissue (Fig. 1).
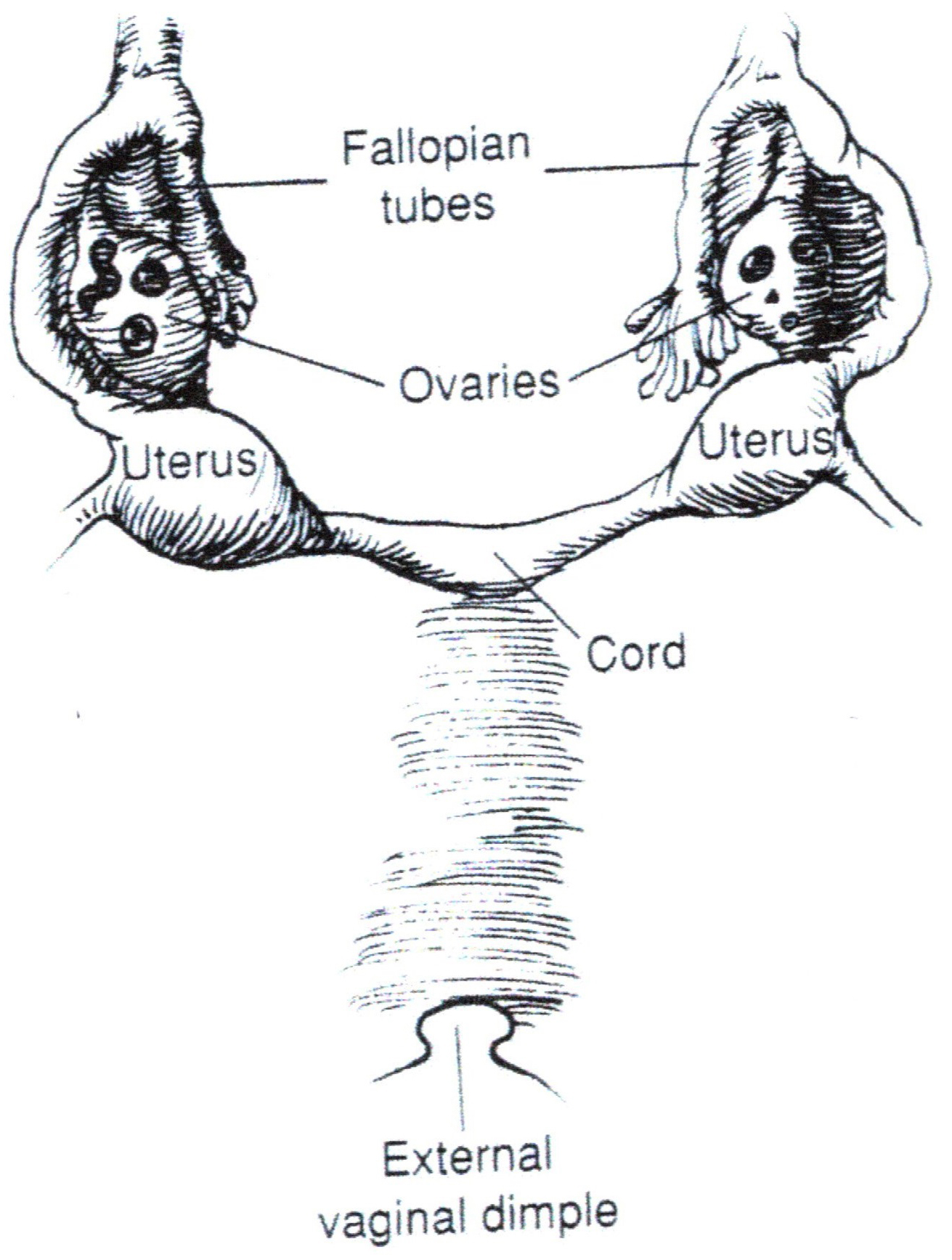
If present, the endometrial tissue can appear immature or, rarely, can demonstrate cyclic response to ovarian hormones [6]. In rare occurences, active endometrium can exist within the uterine anlagen and endometrial cavity. These patients can develop a large hematometra due to the accumulation of trapped blood. Cyclic abdominal pain is relieved by the excision of the active uterine anlagen [7]. Several malformations have been reported in association with MRKH syndrome (Table 1, Ref. [4, 8]). These associations are related to the Wolffian and Müllerian ducts interaction, between the eighth and ninth week of gestation. The area most involved is the urogenital tract: resulting in unilateral renal aplasia, pelvic kidney, horseshoe kidney, and double ureter [9, 10, 11]. Skeletal alterations that have been described include spina bifida, sacralization of L5, lumbarization S1, and anomalies of the cervical vertebrae.
| Typical | Tubes, ovaries, and renal system are present and normal |
| Atypical | Malformations in the ovarian or renal system |
| MURCS | Malformations in the skeleton and/or heart, muscular weakness and renal malformations |
| MURCS, Müllerian aplasia, renal aplasia and cervicothoracic somite dysplasia (association). | |
Cardiac malformations and sensory disturbances, such as unilateral hearing problems, appear to be less common. Notably, a screening test can be performed in both cases [12]. Brown [13] and Fraser [14] demonstrated that the ovarian function is intact and demonstrated correctly timed pubarche, thelarche and normal hormonal secretion. Alterations in the ovary and tubes can vary in their severity. Several authors [10, 15] have described a polycystic degeneration of the ovaries. Rokitansky [16], Bompiani and Rigat [17] described hypoplastic ovaries. In a 53-patient series published in 2005, two patients showed bilateral gonadal streaks and one had unilateral ovarian aplasia [18]. As a result of the ovarian function’s failure, estrogen levels can be reduced, resulting in subsequent effects on the secondary sexual characteristics and bone metabolism. The first line examination panel should include hormones measurements.
The treatment of vaginal agenesis is the creation of a neovagina, which can be done both by surgical or non-surgical approach [19]. The aim of the vaginoplasty is the creation of a neovagina which resembles as much as possible the normal one. It should be satisfying in appearance, function, and feeling without excessive morbidity. According to the American College of Obstetricians and Gynaecologists, primary vaginal elongation by dilation is the appropriate first-line approach in most patients because it is safer, patient-controlled and more cost effective than surgery [20]. Particularly in many European countries, surgical vaginoplasty such as laparoscopic Vecchietti [21] or Davydov [22] procedure is often chosen by women as first line treatment and vaginal dilation is only used as post-operative maintenance support. Behind this preference, there is a strong desire to obtain an immediate satisfying result, which is not possible with the slowly-progressing dilation techniques that require months of constant perseverance. Surgical vaginoplasty techniques can be categorized as follows:
1. Creation of a perineal pouch (Williams vaginoplasty [23] and subsequent modifications [24]).
2. Lining of a neovaginal space. This includes procedures based on the McIndoe technique [25] (neovaginal space dissected between the bladder and rectum and then lined with different types of tissue).
3. Intestinal vaginoplasty [26].
4. Laparoscopic procedures including the Vecchietti procedure [21] and Davydov procedure [22].
The MRKH syndrome has been extensively investigated. The available evidence has been summarized in well conducted reviews regarding the etiological hypothesis, surgical and non-surgical treatment options and the effects of therapies on sexual and psychological functioning. Currently research efforts have begun to focus on another issue of great importance for the well-being of affected patients being their reproductive prognosis. In fact, the compromised fertility of this disease causes important psychological distress and fertility counselling should be a cornerstone of MRKH patients’ care. In the present narrative review, we desire to present the varied options proposed in order to solve the infertility of affected women.
Once the diagnosis is made, several medical sessions should be scheduled. The first session should focus on a detailed explanation of Müllerian agenesis along with constant psychological support. Once the patient reaches initial acceptance of the diagnosis, specific and detailed counselling should be dedicated to fertility options. It is important to emphasize that although women will never conceive naturally, they can still become mothers if this is their desire [27]. Until recently, the only option for women with MRKH syndrome was legal adoption. With the improvements in assisted reproduction technology (ART), gestational surrogacy (GS), and uterine transplantation (UTx) have become new fertility options available to these patients. The discussion of the reproductive potential of patients with MRKH syndrome should address all of these issues.
Following the recent progress of in vitro fertilization (IVF), GS has become an option for the patient to become a mother. The first step is the oocyte retrieval from the MRKH patient and obtaining sperm sample from her partner. Following fertilization, the resulting embryo is transferred to the womb of another woman known as the gestational surrogate carrier. Following a successful delivery, the commissioning couple will then become parents [28].
The GS arrangement may be commercial or altruistic. In the latter case, the carrier is typically a close relative [29]. GS is not allowed in most parts of the world, secondary to cultural, religious or legal reasons [30]. In fact, GS is tolerated in several European countries, such as Portugal, Cyprus, Belarus, Romania and The Netherlands when performed on an altruistic basis. It is completely legal in the UK and Greece, but no compensation is allowed. In Finland since 2007, even altruistic GS is illegal. In the US every state has its own legal position. In Canada, only altruistic GS is allowed. California, Russia and Ukraine allow commercial GS, with an average procedure cost of about 50,000 euro, less than the 100,000 euro cost reported in California [31]. International scientific societies of Obstetrics and Gynaecology like FIGO published recommendations in 2007 [32]. FIGO suggests that surrogate arrangements should not be commercial and are best arranged by non-profit agencies. GS is a practice performed by many MRKH patients living where GS in not available, raising concerns regarding the reproductive tourism. However, this controversial practice is not always a viable solution since not all home countries recognize children born abroad through surrogacy. For example, the children of single women who travelled abroad for GS are not recognized by Israel [33].
There are numerous the clinical risks associated with GS practice. Multiple-gestation pregnancy rates are higher with the associated pathologies of hyperemesis, gestational hypertension, gestational diabetes, anemia, preterm labor, haemorrhage and caesarean delivery. For this reason, a single embryo transfer is commonly suggested. Lastly, we should highlight the high level of emotional and psychological distress suffered by all parties involved. In fact the mental involvement stressors, especially during the last month of gestation, are often quite strong. Although it seems that patients with MRKH syndrome have a fair chance of achieving live birth through IVF and GS, more data is needed to draw firm conclusions [28].
A new era for MRKH patients who desire motherhood started in 2014 in Sweden, with the first baby born after UTx [34]. Currently, more than 70 UTx procedures have been performed in MRKH patients. Following these events, approximately 20 babies have been born worldwide in Sweden, USA, Serbia, India, France, Germany, Lebanon, Czech Republic, China and Brazil (Table 2, Ref. [35, 36, 37]). There are reports of MRKH women having delivered twice [3].
| Year | Country | Number of patients | Recipient’s pathology | Donor’s status | Pregnancy outcome |
| 2000 | Saudi Arabia | 1 | Postpartum hysterectomy | Alive | None |
| 2011 | Turkey | 1 | MRKH | Dead | Miscarriage |
| 2012–2013 | Sweden | 9 | MRKH (8) Hysterectomy (Cervical cancer) (1) | Alive | 8 LB |
| 2015 | China | 1 | MRKH | Alive | NR |
| 2015 | Texas, USA | 5 | MRKH | Alive | 4 LB |
| 2016–2019 | Ohio, USA | 2 | MRKH | Dead | 2 LB |
| 2016–2018 | Czech Republic | 9 | MRKH | Alive (5) Dead (4) | 1 LB |
| 2016 | Brazil | 1 | MRKH | Dead | 1 LB |
| 2017 | Texas, USA | 11 | MRKH (9) Hysterectomy (Myomas) (2) | Alive (9) Dead (2) | 6 LB |
| 2017 | Germany | 3 | MRKH | Alive | 2 LB |
| 2017 | Serbia | 1 | NR | Alive | NR |
| 2017 | India | 4 | MRKH (3) Asherman (1) | Alive | 3 LB |
| 2017 | Sweden | 2 | NR | NR | NR |
| 2019 | France | 1 | NR | NR | NR |
| 2020 | Lebanon | 1 | MRKH | Alive | 1 LB |
| LB, Live Births; NR, Not reported. | |||||
The volume of UTx procedures performed is increasing rapidly. The need for a precise database collecting all the cases and outcomes calls for the creation of an international registry of uterus transplantation cases with follow-up of patients, children and donors. This registry has now been announced, but it is still to be developed [35].
The strongest clinical indication is represented by women with a strong desire for fertility who suffer from MRKH syndrome and live in countries where GS is banned. According to current data, UTx is an effective method to achieve fertility in a selected group of patients. The chance to obtain a live birth is higher than 80% in patients when the transplanted uterus remain in situ for more than six months [36].
Initially, UTx was considered inappropriate as it was expensive and a hazardous elective procedure in order to experience pregnancy and delivery when less cumbersome and less invasive options were available [38]. Patients should receive extensive counselling about all of the potential risks including the IVF procedure, a minimum of 3 major surgeries (UTx, caesarean section, and hysterectomy), exposure to immunosuppressive drugs, graft failure risk and all the complications related to pregnancy [36]. Ultimately the will of the patient will guide the final treatment decision. A Czech survey published in 2018 showed that two thirds of the MRKH patients with a surgically created neovagina were interested in receiving a UTx [38]. Moreover, most women surveyed in the UK, a country where GS is permitted, prefer UTx over gestational surrogacy and adoption. In Sweden, randomly selected women preferred UTx over GS [39, 40, 41]. A recent study including more than 3000 Japanese women showed that UTx has a 2-fold higher acceptance rate when compared to GS. Behind these opinions, there might be moral concerns about using a paid surrogate, the desire to bear the child in her own body and the psychological and social complications of entrusting her embryo and future child to another woman. UTx can be of great help, especially for Muslims patients who seek fertility. The Muslim faith under sharia law does not allow GS [42]. UTx transplantation is peculiar in several features: it is not a life-saving organ, but is a life-enhancing as well as a life-giving organ. What is unique to UTx, compared to other kinds of transplant, is its fleeting and momentary profile. It is the first ephemeral transplantation since immunosuppression is maintained for a short time before removing the graft [43]. This usually happens within 5 years, after the woman has realized their reproductive desires. In fact, UTx is the only organ transplant where success is defined both by its function and the delivery of a healthy offspring. At least 18 months are needed to determine the final success of UTx, as pregnancy attempts should be delayed for 12 months [44]. Regarding the donor, they should be aware they will be unable to bear any future pregnancies. In case of a close familiar relationship with the recipient, they may suffer excessive psychological pressure while postponing their personal interests. On the contrary, when the donor is unrelated to the recipient, doubts are commonly raised about the freedom of this action. In the UK, the HTA [Human Tissue Authority] performs a more thorough assessment when a person is offering to donate an organ to a stranger, rather than to a relative or friend. Donors are allowed to recover expenses, but without making any profit. A further concern with the rewarded donation is the fact that the wealthy could exploit the poor, essentially buying their fertility.
In general, the UTx surgery of the MRKH women starts with a longitudinal midline incision. A dissection is performed between the neovagina, the bladder and the rectum followed by an external iliac arteries and veins dissection. At this point, the uterus is placed into the pelvis. Internal iliac segments on the graft’s uterine vessels are connected to the external iliac vessels. Following reperfusion, end-to-end vaginal anastomosis is performed, with the fixation of the uterus to the ligaments. The immunosuppression regimen used for the UTx is a standard induction therapy, based on calcineurin inhibitors like tacrolimus, similarly to what is used in kidney transplantation [45]. Such immunosuppression protocol can be potentially dangerous in the MRKH patient who undergoes intestinal vaginoplasty. For this reason, this group of patients is not suited for UTx. These drugs are nephrotoxic and their use should be limited. This is of particular interest in MRKH syndrome, where a single kidney is present in several patients. A 2019 study [36] found a 75% risk of pre-eclampsia in women with single kidneys following UTx. This risk is higher than the 35% risk reported in previous studies [46]. Most of the babies born after UTx were healthy children, who were delivered prematurely by Cesarean section for different causes. Currently, no evidence exists about an increased risk for intrauterine growth restriction. Nonetheless, several potential risks to the fetus require prompt attention: the effect of immunosuppressive drugs, a lack of appropriate blood flow to the uterus during gestation, and the increased risk of preeclampsia [47, 48, 49].
Following the birth of the first child from a deceased donor (DD) uterus, which occurred in Brazil in 2018 [50], the fertility goal of MRKH has been achieved with both living donors (LD) and DD. Since there is a mismatch between the uterine organ demand and the LD availability, the success after uterine transplantation from a DD paved the way to a potential larger donor group [51]. Both altruistic and non-altruistic LDs of the uterus will not provide a sufficient organ source for the potential recipients allowing DDs to become a potential resource. Therefore, it might be possible to use both of the two options synergistically in the future [52, 37]. The main benefit to utilize LDs is pragmatic. It allows appropriate elective planning of a complex operation with a multidisciplinary team. Since the uterus is not a vital organ, the use of LD poses a less ethical dilemma than donation of other organs [53]. On the other hand, the main advantage of the use of uterine DD is the avoidance of harm related to the recovery surgery in the LD [54]. Donor hysterectomy is a complex surgery with a high morbidity being similar to radical hysterectomy. In particular, it is challenging to perform the dissection of the uterine vessels. It has been proposed as an alternative the use of ovarian veins for blood drainage. The mean surgical time has been reported to be 11.5 hours in the Swedish trial. The mean intraoperative blood loss was 920 mL in the donor surgery. Major complications included urinary tract injuries, thrombosis, infection and haematoma. Grade IIIb Clavien-Dindo complications such as ureteric injuries, ureterovaginal fistula and vaginal cuff dehiscence have been described in different studies [55, 56, 57]. Moreover, procurement surgery in DD is less demanding with wider vessels patches being retrieved and used for anastomosis. Anonymity of the donation is another advantage of DD. This DD anonymity has a positive impact on the recipient’s psychology avoiding the feeling of a debt to the LD.
One of the most common doubts raised by MRKH patients is whether their daughter will share the same phenotype. “Will my child have a uterus?” is a frequent question posed during the fertility counselling [58]. Although there have been some reports of familial aggregates of Müllerian agenesis, the vast majority of the daughters of MRKH women who gained motherhood through IVF have normal reproductive anatomy [58]. No specific cause has been identified at this time since organogenesis is a complex process, involving an interplay of different factors. A monogenic genetic etiology is supported by the reported association between MRKH syndrome and renal malformations in familial pedigrees [5, 59, 60]. In contrast, the polygenic or non-genetic etiological hypothesis is based on the cases that occur sporadically, the lack of recurrence in surrogate pregnancies’ outcomes and the reports of discordant twin pairs [61, 61, 62, 63, 64]. When we discuss the possible ways MRKH syndrome can be inherited, one has always to keep in mind that the nature of this syndrome itself hinders its transmission. In fact, infertility can obscure, at least partially, the vertical transmission of the trait and thus lead to an underestimation of the genetic heritability. Currently, there is no chance to perform preimplantation screening for this pathology. However, it is likely that the daughters of MRKH women will have a normal reproductive system. Women with associated anomalies, other than genital tract ones, have a higher chance of transmitting their disorders to their children [65, 66]. Following UTx and GS progress as fertility treatments, more MRKH patients will gain biological motherhood in the future. We can foresee an increase regarding the demand for prenatal diagnosis but recommend that antenatal diagnosis only be performed in women with a solid genetic diagnosis following extensive genetic counselling.
When considering IVF, the hormonal background of affected patients should be carefully investigated. Cases of aberrant gonadotrophin levels, hyperprolactinemia, high anti-Müllerian hormone and hyperandrogenism have been reported [67, 68]. In a group of 69 women with MRKH syndrome, more than half had biochemical hyperandrogenemia with only a few demonstrating clinical signs of androgen excess [69]. Some authors [70] have suggested that the FSH, LH, and inhibin B irregularities seen in some MRKH patients, may be due to the absence of normal ovarian-uterine communication in affected women. There is concern about which optimal ovarian stimulation protocol should be utilized in these patients. MRKH patients showed hormonal responses similar to those of women with normal pelvic anatomy and ovulation induction is generally easy to obtain [71, 72]. It is necessary to assess the menstrual phase in these patients to decide when to initiate ovarian stimulation and synchronization with the GS carrier. Since there is no outflow tract of menstrual blood, some authors have suggested different determination methods which include oral contraceptives [73], measurement of serum progesterone levels to diagnose the luteal phase and start of pituitary downregulation using GnRH agonist, followed by ovarian stimulation with gonadotropins utilizing long GnRHa protocol [72]. Women with type I and II MRKH have shown similar rates of clinical pregnancies, ranging from 17 to 37%. The first group needed less gonadotropins for stimulation and obtained more follicles, oocytes and cleaving embryos [74]. A further concern is the technical feasibility of the oocyte retrieval. Oocyte retrieval in patients with MRKH poses several challenges and an experienced IVF physician is needed [71]. Some of the neovaginas, especially those obtained with surgical methods, may lack tissue elasticity, making transvaginal oocyte recovery demanding [75]. Moreover, in MRKH patients the ovaries are often located in a more cranial and lateral position along the pelvic sidewalls, thus representing an additional problem for the retrieval [27]. In selected cases, laparoscopic or transabdominal recovery may be necessary. Finally, it should be remembered that, since both the Müllerian structures and gonads arise from the genital ridge, in rare instances an ovary may be congenitally absent [76]. As ovarian tissue may be found in the upper abdomen, at the pelvic brim level, or within the inguinal canal, imaging modalities such as magnetic resonance may help locate gonads before ovulation induction. Another issue is the condition of the pelvis at the time of oocyte retrieval. In fact, the pelvic cavity of the patients who received invasive surgeries for the creation of the neovagina, such as intestinal vaginoplasty, commonly show surgical adhesions [77]. Better intraabdominal results are reported in laparoscopic techinques, such as Vecchietti [22] or Davydov [23]. An interesting proposal is that of Candiani et al.[78] who recently reported the outcome of a new procedure. He proposes the oocyte pickup at the same time of the creation of the neovagina. In this work, he reported an average of 8.8 mature oocytes frozen for each patient. The combination of these two procedures may alleviate the psychological stress of a second operation for oocyte retrieval following the vaginoplasty.
In MRKH syndrome, creating a neovagina represents the first step to developing a fully satisfying life both from the emotional and relational point of view. Currently, the discussion of the potential fertility cannot be left behind. The management of MRKH women should always include some space and time for the fertility options counselling. In the past, adoption was the only viable option. IVF has made GS possible and following the progress of UTx, another way is currently available. In both scenarios, these patients will need a preliminary oocyte retrieval and fertilization in vitro that must necessarily precede the transplantation. UTx after the successful live births of about 20 infants [3], appears to be an exploitable option to gain motherhood for women affected by MRKH syndrome. The number of UTx procedures performed is expected to increase exponentially in the future, as several established teams are present worldwide. It is quite clear that UTx can hardly be considered an option for all women with MRKH syndrome secondary to its complexity and the necessary immunologic therapies. Failure of the procedure is a real possibility, and the deep sense of anguish perceived when UTx turns out unsuccessful can be devastating. Some UTxs will be rejected and removed and in other cases pregnancy will not be achieved or will not come to term [79]. It is currently too soon to consider UTx as a safe mode of management and we are still far from incorporating this method into therapeutic protocols targeted for infertility treatment for women with MRKH syndrome. Prospective trials are warranted to establish if this intervention has all the required features to be applied on a larger scale.
FF developed the concept and wrote the manuscript. AB participated in writing the manuscript. SS participated in writing the manuscript. MC analysed the data and coordinated efforts. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript.
Not applicable.
Thanks to all the peer reviewers for their opinions and suggestions.
This research received no external funding.
The authors declare no conflict of interest.