


 , Silvia Romiti 1,†, Sara Saltarocchi 1, Wael Saade 1, Flaminia Spunticchia 1, Noemi Bruno 1, Mariangela Peruzzi 1,2, Fabio Miraldi 1, Giacomo Frati 3,4, Ernesto Greco 1, Francesco Macrina 1, Paolo De Orchi 1, Antonino G. M. Marullo 3
, Silvia Romiti 1,†, Sara Saltarocchi 1, Wael Saade 1, Flaminia Spunticchia 1, Noemi Bruno 1, Mariangela Peruzzi 1,2, Fabio Miraldi 1, Giacomo Frati 3,4, Ernesto Greco 1, Francesco Macrina 1, Paolo De Orchi 1, Antonino G. M. Marullo 31 Department of Clinical, Internal Anesthesiological and Cardiovascular Sciences, Sapienza University of Rome, 00161 Rome, Italy
2 Department of Cardiology, Mediterranea Cardiocentro, 80122 Naples, Italy
3 Department of Medico-Surgical Sciences and Biotechnologies, Sapienza University of Rome, 04100 Latina, Italy
4 Department of Angiocardioneurology, IRCCS NeuroMed, 86077 Pozzilli (IS), Italy
†These authors contributed equally.
Abstract
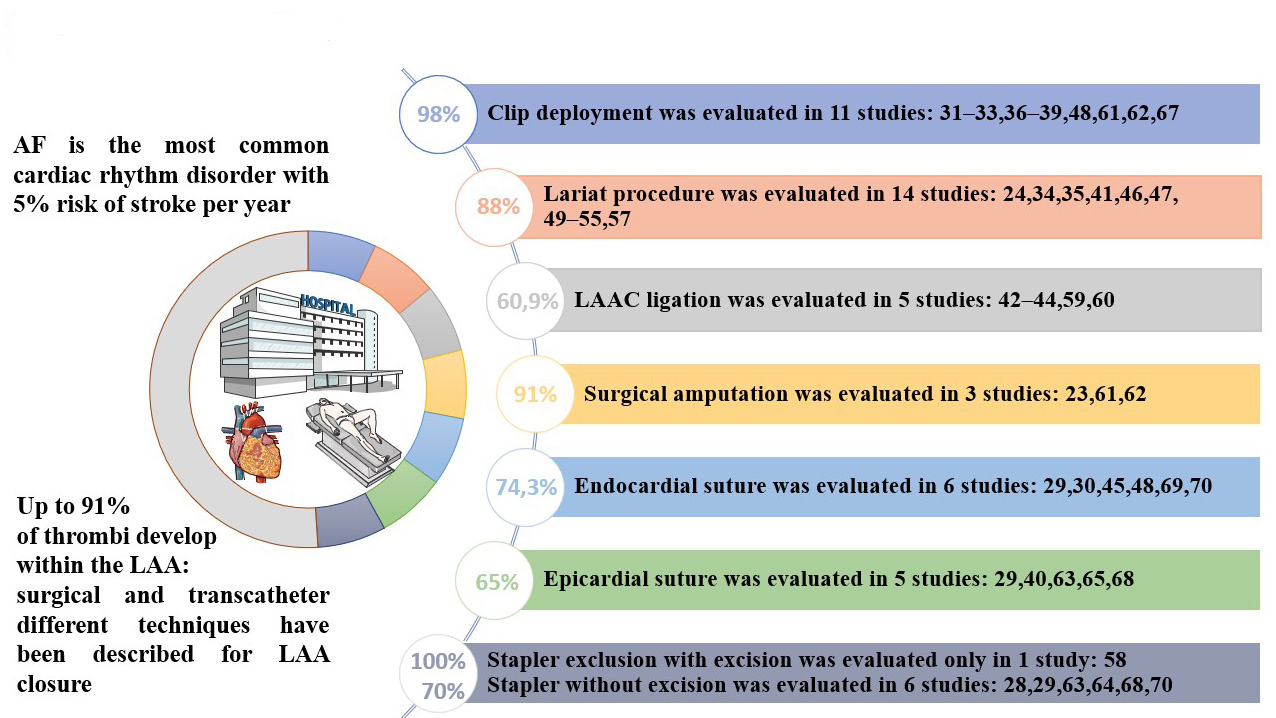
Background: Atrial fibrillation has been identified as an independent risk factor for thromboembolic events. Since 1948 different surgical techniques have described the feasibility and the rationale of left atrial surgical appendage closure. The aim of this systematic review is to evaluate the reported patency rates of different surgical techniques. Methods: This systematic review was conducted according to preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines. Two independent investigators searched the PubMed, Scopus, Web of Science, Cochrane Central Register of Controlled Trials, and OVID® (Wolters Kluwer, Alphen aan den Rijn, Netherlands) to identify relevant studies. Consecutively, a PICO (Population, Intervention, Comparison and Outcomes) strategy assessment of literature was performed to search eventual other relevant studies that may have been ignored. Results: A total of 42 studies were included in our analysis. The total number of patients who underwent surgical left atrial appendage closure was 5671, and in 61.2% an imaging follow up was performed, mostly with transesophageal echocardiographic evaluation. Success rate for the different techniques was: Clip deployment 98%; Lariat procedure 88%; Surgical amputation 91%; Endocardial suture 74.3%, Epicardial suture 65%; Left atrial appendage closure (LAAC) ligation 60.9%; Stapler technique with excision of left atrial appendage (LAA) 100%; Stapler without excision 70%. Conclusions: To date, data on surgical left atrial appendage closure are poor and not standardized, even if reported rates are acceptable and comparable to transcatheter procedures. If validated on large-scale non-retrospective and multicentric studies, these promising developments may offer a valuable alternative for patients with atrial fibrillation (AF) and ineligible for oral anticoagulation therapy.
Graphical Abstract
Keywords
- left atrial appendage closure
- LAAC
- surgical closure
- left atrial appendage
- atrial fibrillation
Atrial fibrillation (AF) is the most common cardiac rhythm disorder, with an estimated worldwide prevalence of around 46.3 million of people in 2016 with higher incidence according to age and ethnicity [1]. AF has been identified as an independent risk factor for thromboembolic events and is associated with higher incidence of morbidity and mortality due to ischemic stroke and, accordingly, should not be considered a benign disease [1]. The actual risk of stroke in patients with AF is estimated 5% per year, and this percentage may further increase when other risk factors, such as age, hypertension and left ventricular dysfunction, are associated [1]. The left atrial appendage (LAA) has been suspected and therefore studied as a possible source of thromboembolism as early as 1925 [2]. Originally the LAA has been described as a non-functioning anatomical structure, an embryological remnant and subsequently as the “most lethal human attachment” [3]. Nowadays its physiological activity is well established. Function of the LAA includes modulation of the sympathetic and parasympathetic tone, production of the natriuretic peptide balance, left atrium (LA) pressure and volume overload, and contribution to the diastolic filling of the left ventricle [4, 5]. The latter, however, is severely impaired during AF, especially when the LAA presents all the criteria of the Virchow’s triad (stasis; vascular endothelial injury, due to the overstretching of the atrial muscle fibers with fibroblastic infiltration and subsequent inflammation; blood alteration, related to platelet activation and inflammation) [6, 7]. Therefore, in patients with nonvalvular AF, up to 91% of thrombi develop within the LAA compared with patients with valvular AF, in whom LAA localization is ~57%.
LAA can be considered a finger-like extension of the left atrium muscular wall,
an embryonic remnant that develops during the fourth week of gestation after the
development of the LA that occurs during the third week [8]. On average the LAA
has a length of 46 mm and a volume of 9 mL. The LAA lies within the pericardium,
anteriorly to the left pulmonary veins and inferiorly to the pulmonary artery,
adjacent to the free wall of the left ventricle. Importantly, it’s close to the
left phrenic nerve and the left circumflex artery. The LAA can be structurally
divided into two parts: the ostium and the body. The ostium represents the point
of convergence between the antero-lateral walls of the LA and the LAA pectinate
muscles. Several three-dimensional morphologies of left appendage junctions with
the LA have been identified on computed tomography: oval-shaped, teardrop-shaped,
foot-shaped, triangular, and round-shaped, among which the oval configuration,
observed in 68.9% of cases, represents the most common anatomical outline [9].
Moreover, the LAA main body conformation can range from single-lobed, bilobed
and, most commonly, trilobed. In a recent classification, based on computed
tomography and magnetic resonance imaging, four different LAA shapes were
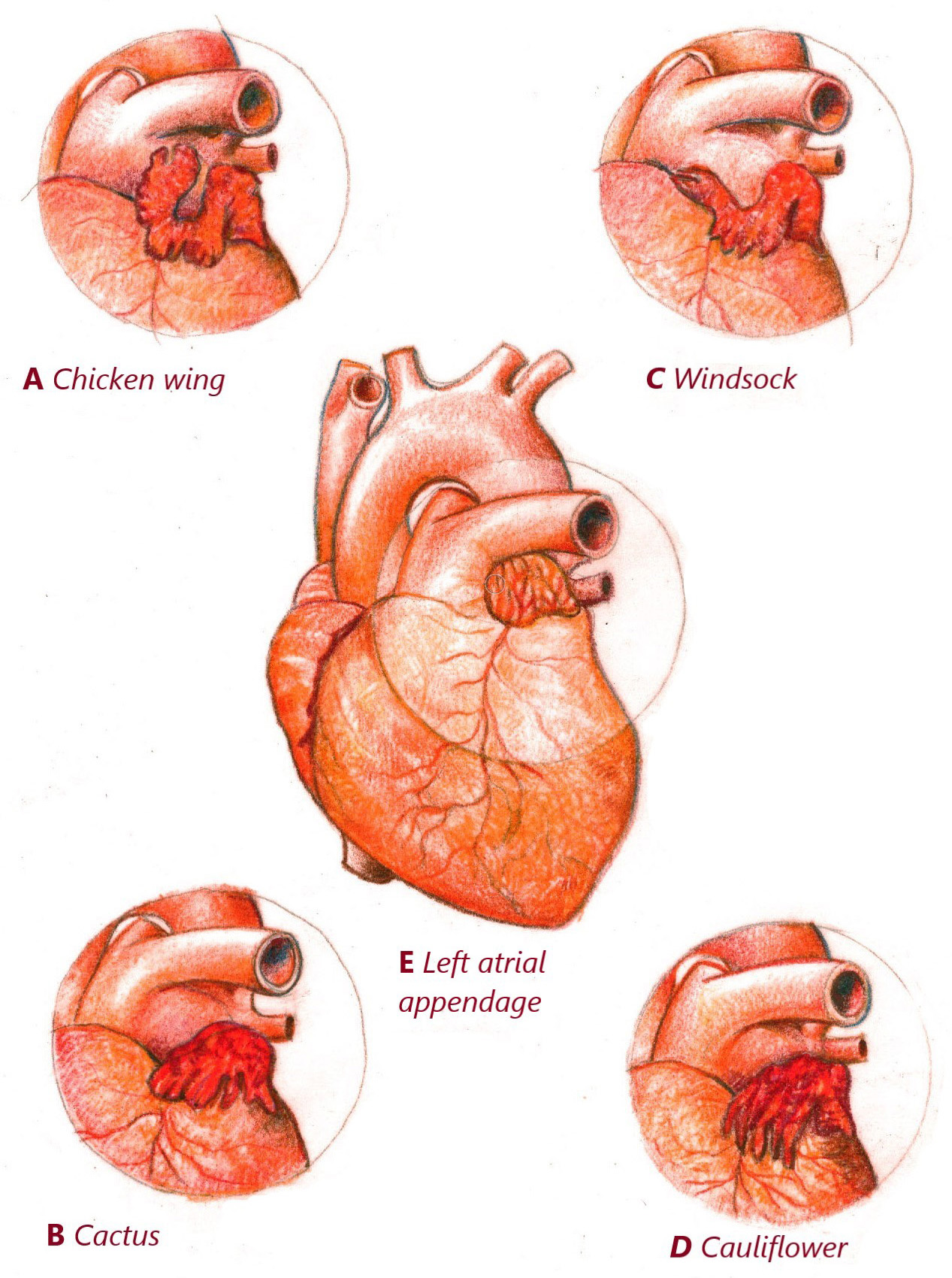
classified: chicken wing (48%), cactus (30%), windsock (19%) and cauliflower
(3%) [10] (Fig. 1). According to this classification, chicken-wing morphology is
a protective factor in terms of thromboembolic events and is associated with
lower thromboembolic risk even in accordance with comorbidities and
CHA
 Fig. 1.
Fig. 1.Left atrial appendage classification according to morphologies. (A) LAA Chicken wing shaped. (B) LAA Cactus shaped. (C) LAA Windsock shaped. (D) LAA Cauliflower shaped. (E) Left atrial appendage. LAA, left atrial appendage.
The LAA architecture is complex with non-uniform wall thickness consisting of endocardial and epicardial fibers arranged in different orientations [9]. Alterations in LAA flow velocity and structural remodeling of the endothelium are involved in the increased thromboembolic risk in AF patients. In fact, LAA has been shown to possess mechanical and homeostatic properties and a pivotal role in the development of the major AF complications. The LAA flow velocity depends on its morphology, gender, cardiac rhythm, aging, left ventricular function and heart valve disease such as mitral stenosis. Interestingly, chicken wing shaped LAA has been correlated with a higher flow velocity compared with cactus and cauliflower morphologies probably justifying its minor risk of thromboembolic events. In patients with atrial fibrillation LAA flow velocity has been reported to be lower than the one measured in normal sinus rhythm, with an inverse relationship with ventricular rate, age, and female sex [11]. Additionally, the LAA plays a key role in volume homeostasis by producing atrial and brain natriuretic peptides which act increasing renal sodium excretion and, consequently, reducing extracellular volume and blood pressure. Moreover, new evidence suggests an involvement in the regulation of the adrenergic system and renin-aldosterone system (RAA) [12].
Considering the pivotal role of LAA in thrombi formation and migration in AF patients, surgical and/or transcatheter LAA exclusion techniques are emerging as safe, feasible and increasingly adopted treatment for mechanical thromboprophylaxis, even in elderly patients [13]. Since 1948, when Madden et al. [14] evidenced the feasibility and the rationale of this procedure during mitral valve surgery [15, 16], concomitant surgical closure of the left atrium appendage (sLAAC) in cardiac surgery, even using minimally invasive and video assisted approach [17, 18, 19, 20, 21], was associated with lower risk of cerebrovascular events in patients with AF. Ando et al. [22] reported in a systematic review and meta-analysis that sLAAC significantly decreased the risk of mortality and prevented cerebrovascular complication at 30-day follow-up, especially in patients with pre-operative AF.
Different techniques have been described and adopted for the sLAAC such as
epicardial exclusion (oversew, purse string, with or without
polytetrafluoroethylene (PTFE) reinforcement), epicardial excision (with stapler,
with stapler and excision of the left appendage, with or without reinforcement,
with epicardial clips or through snares/suture loops), or endocardial suture
ligation, with or without amputation [23] (Figs. 2,3). Another described
technique, generally adopted in patients with a large base appendage, is the
closure through autologous or bovine pericardial patches. The continuously rising
interest in this procedure also led to the introduction of newer techniques, such
as the invagination of the appendage in the left atrium, and hybrid techniques
that combine a surgical and/or percutaneous approach to an endovascular one, such
as the Lariat Device technique [24] (Fig. 2). Results of sLAAC are often
confounding due to lack of standardized criteria for definition of Left Atrial
Appendage Closure (LAAC) success. Different studies (see Table 1), in fact, tend to arbitrarily
assess patency of the LAA with different criteria, that may be either more
stringent (as in case of complete absence of flow and stump) or more permissive
(Stump or Flow
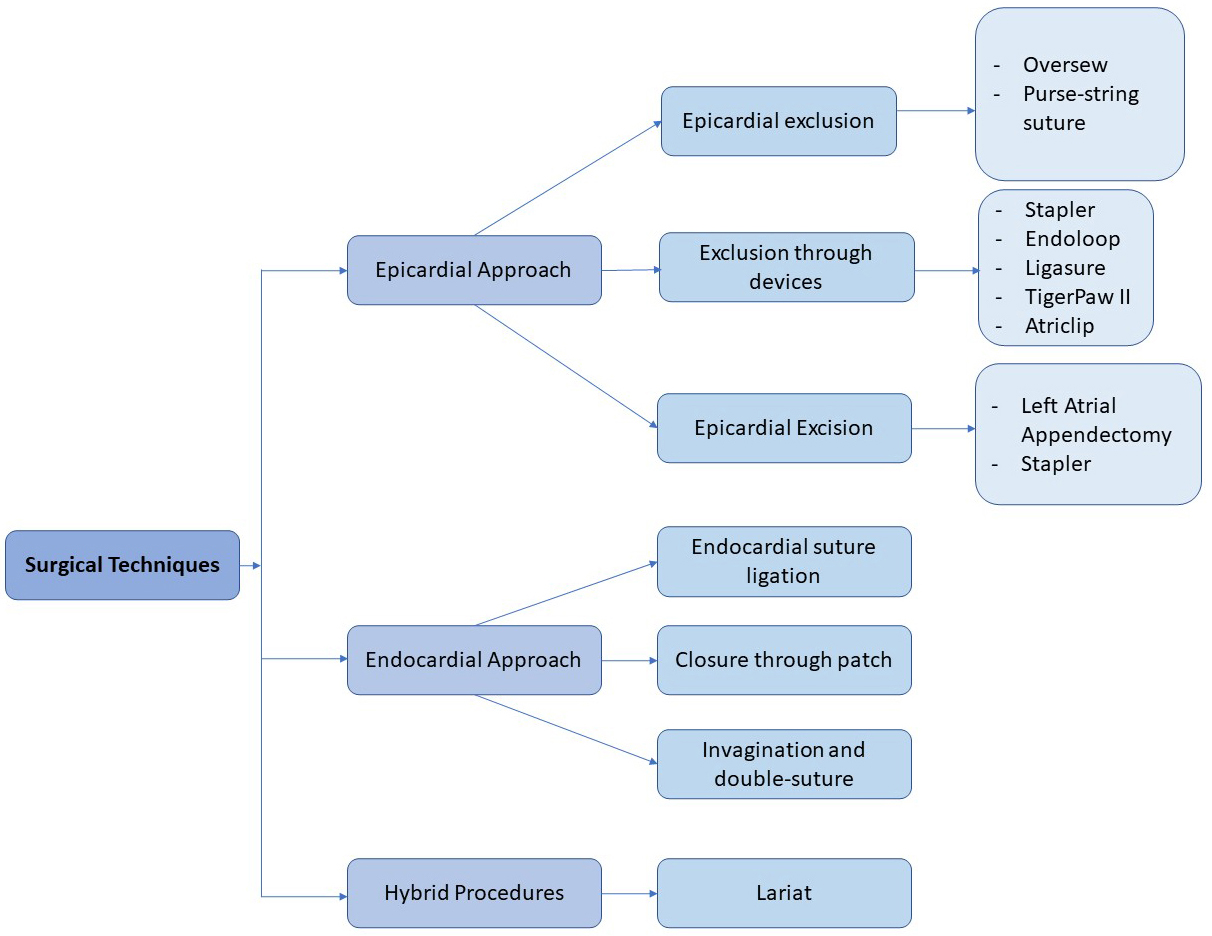
 Fig. 2.
Fig. 2.Surgical left atrial appendage closure classification.
 Fig. 3.
Fig. 3.Surgical techniques of left atrial appendage closure. (A) Endoloop Snaring. (B) Surgical stapler. (C) Epicardial excision. (D) Purse string exclusion.
| Author | Year | N. patients | N. patients at FU | Definition of complete closure | Time to mean echocardiographic FU | Intraoperative echocardiographic assessment | Intraoperative success rate | Follow-up assessment | Type of LAAC | Success rate |
|---|---|---|---|---|---|---|---|---|---|---|
| Kiankhooy MD et al [68] | 2022 | 100 | 97 | 3 | 685 | TEE | 100% | TEE | Clip | 96% |
| Shirasaka T et al [47] | 2021 | 8 | 8 | 0 | 7 | TEE | 100% | TEE | Endocardial | 100% |
| 6 | 6 | Clip | 100% | |||||||
| Fleerakkers J et al [39] | 2020 | 13 | 13 | 0 | - | TEE | 100% | CT Scan | Clip | 100% |
| Suematsu Y et al [33] | 2020 | 43 | 43 | 0 | 90 | TEE | 100% | CT Scan | Clip | 100% |
| Kats ES et al [61] | 2000 | 50 | 20 | 3 | 1900 | TEE | 67% | TEE | Ligation | 60% |
| Hirnle G et al [44] | 2020 | 50 | 19 | 0 | 180 | TEE | 100% | TEE + CT Scan | Endocardial | 95% |
| Tilz RR et al [57] | 2020 | 138 | 103 | 2 | 181 | TEE | 94.2% | TEE | Lariat | 97.10% |
| Lin B et al [40] | 2020 | 74 | 74 | 0 | 200 | - | - | TEE | Epicardial | 72% |
| Güner A et al [67] | 2020 | 101 | 101 | 3 | 90 | - | - | TEE | Epicardial | 65.3% |
| Ellis CR et al [46] | 2020 | 33 | 33 | 0 | 30 | TEE + Angiography | 100% | TEE or CT Scan | Lariat | 82% |
| Parikh V et al [35] | 2019 | 108 | 80 | 0 | 365 | TEE | 93% | TEE | Lariat | 96.3% |
| Mohanty S et al [45] | 2019 | 306 | 306 | 0 | 30 | - | - | TEE | Lariat | 73.50% |
| Fu M et al [66] | 2019 | 257 | 257 | 3 | 365 | - | - | TEE | Stapler | 76.70% |
| Caliskan E et al [64] | 2018 | 291 | 23 | 3 | 1080 | TEE | 100% | CT Scan | Clip | 100% |
| Van Laar C et al [31] | 2018 | 222 | 222 | 0 | 180 | TEE | - | TEE or CT Scan | Clip | 95% |
| Park-Hansen J et al [30] | 2018 | 101 | 10 | 0 | 524 | - | - | TEE | Endocardial | 100% |
| Fink T et al [59] | 2018 | 44 | 35 | 3 | 183 | TEE + Angiography | 100% | TEE | Lariat | 66% |
| Ohtsuka T et al [28] | 2018 | 201 | 194 | 0 | 30 | TEE | 100% | CT Scan | Stapler | 97.50% |
| Ellis CR et al [38] | 2017 | 65 | 65 | 0 | 90 | TEE | 100% | CT Scan | Clip | 93.90% |
| Kurfist V et al [63] | 2017 | 101 | Unknown | 3 | 90 | TEE | 98% | TEE | Clip | 100% |
| Cullen MW et al [29] | 2016 | 93 | 93 | 0 | 30 | TEE | - | TEE | Amputation | 100% |
| Epicardial | 41% | |||||||||
| Endocardial | 71% | |||||||||
| Stapler | 71% | |||||||||
| Lee R et al [60] | 2016 | 28 | 21 | 3 | 140 | TEE | 87.5%–100% | TEE | Endocardial | 57% |
| Stapled Excision | 100% | |||||||||
| Amputation | 100% | |||||||||
| Bartus K et al [53] | 2016 | 58 | 48 | 1 | 90 | TEE + Angiography | 100% | TEE | Lariat | 92.30% |
| Lakkireddy D et al [49] | 2016 | 682 | 480 | 0 | 90 | TEE | 98% | TEE | Lariat | 93.3% |
| Pillarisetti J et al [56] | 2015 | 259 | 259 | 2 | 365 | TEE | 98% | TEE | Lariat | 87% |
| Sievert H et al [34] | 2015 | 139 | 127 | 0 | 45 | TEE + Angiography | 99% | TEE | Lariat | 90% |
| Stone D et al [55] | 2015 | 25 | 22 | 2 | 45 | TEE + Angiography | 100% | TEE | Lariat | 100% |
| Aryana A et al [41] | 2015 | 72 | 72 | 0 | 90 | - | - | CT Scan | Ligation | 64% |
| Emmert MY et al [37] | 2014 | 40 | 32 | 0 | 1080 | TEE | 100% | CT Scan | Clip | 100% |
| Miller MA et al [52] | 2014 | 41 | 41 | 1 | 100 | TEE + Angiography | 93% | TEE or CT Scan | Lariat | 76% |
| Price MJ et al [54] | 2014 | 145 | 63 | 2 | 112 | TEE | 94% | TEE | Lariat | 93% |
| Zapolanski A et al [62] | 2013 | 808 | 56 | 3 | - | TEE | 100% | TEE | Ligation | 94.70% |
| Bartus K et al [51] | 2013 | 89 | 65 | 1 | 365 | TEE | 96% | TEE | Lariat | 98% |
| Massumi A et al [50] | 2013 | 20 | 17 | 1 | 96 | TEE + Angiography | 100% | TEE | Lariat | 100% |
| Adams C et al [42] | 2012 | 12 | 12 | 0 | 90 | TEE | 100% | CT Scan | Ligation | 25% |
| Ailawadi G et al [36] | 2011 | 70 | 61 | 0 | 90 | TEE | 95.7% | TEE or CT Scan | Clip | 98.3% |
| Slater AD et al [58] | 2011 | 60 | 54 | 3 | 90 | TEE | 93.3% | TEE | Tigerpaw II | 100% |
| Salzberg SP et al [32] | 2010 | 34 | Unknown | 0 | 90 | TEE | 100% | CT Scan | Clip | 100% |
| Kanderian AS et al [69] | 2008 | 137 | 137 | 3 | 243 | - | - | TEE | Amputation | 73% |
| Endocardial | 23% | |||||||||
| Stapler | 0% | |||||||||
| Healey JS et al [65] | 2005 | 52 | 44 | 3 | 60 | - | - | TEE | Stapler | 72% |
| Epicardial | 45% | |||||||||
| García-Fernández MA et al [43] | 2003 | 58 | 58 | 0 | 2082 | - | - | TEE | Ligation | 89.70% |
| Johnson WD et al [3] | 2000 | 437 | Unknown | TEE | Stapler | 100% | ||||
| Epicardial | 100% |
Definition of Complete Suture: (0) absence of leaks and of flow between LAA and
left atrium; (1) residual flow
LAA, left atrial appendage; FU, follow-up; TEE, transesophageal echocardiography; CT Scan, computed tomography scan; LAAC, left atrial appendage closure.
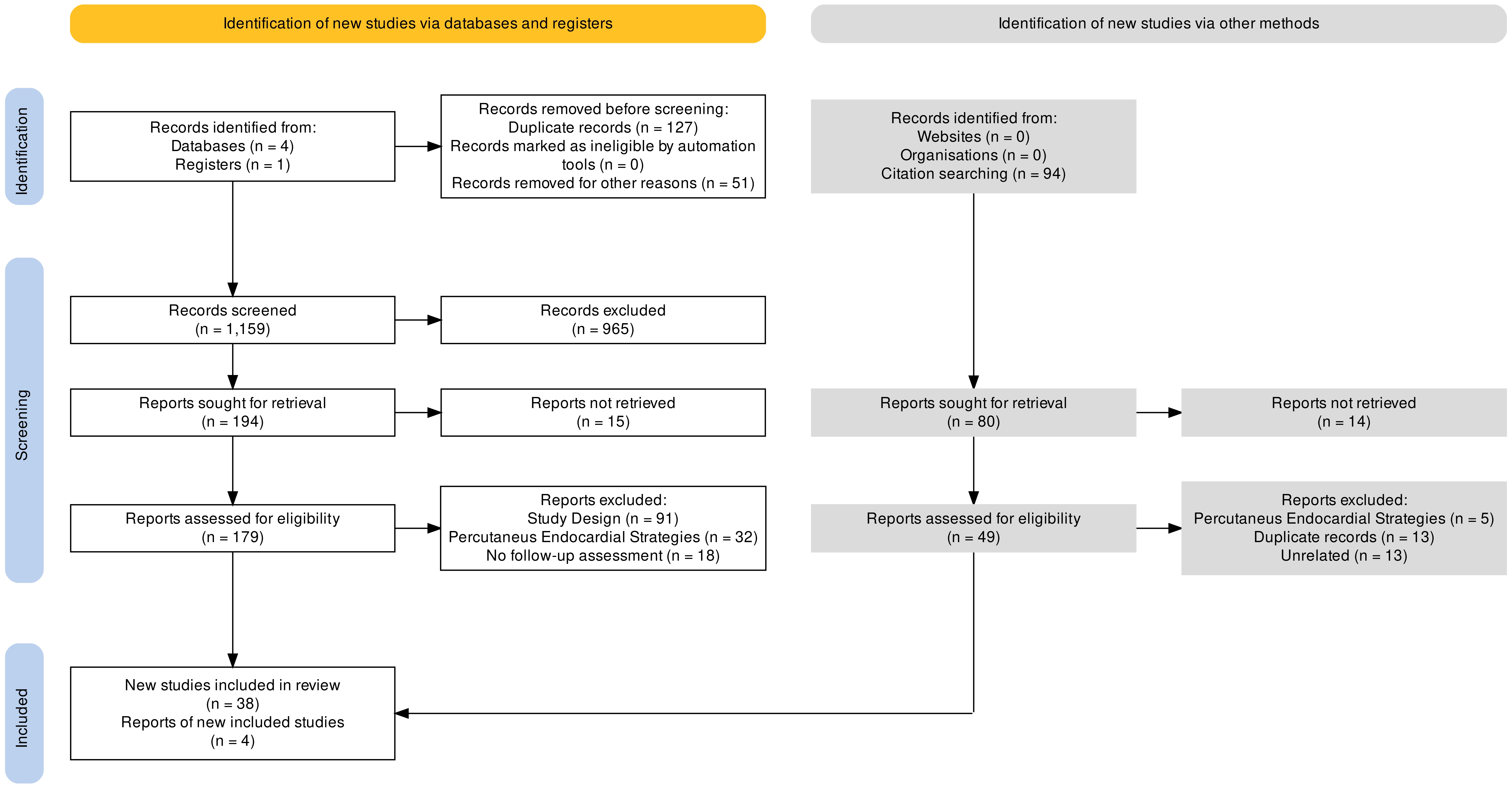
This review adhered to preferred reporting items for systematic reviews and meta-analyses guidelines (PRISMA) [25] and was performed in line with a prespecified protocol. Two independent investigators (MDA and SR) searched the PubMed, Scopus, Web of Science, Cochrane Central Register of Controlled Trials (CENTRAL), and OVID to identify relevant studies. The following key medical subject headings (MeSH) terms and Emtree terms were used: left atrial appendage, LAAC, surgical closure or surgical occlusion. The search was extended from inception up to December 31, 2022. Case reports, editorials, expert opinions, review articles, guidelines, animal studies and non-English studies were arbitrarily excluded (Fig. 4). Two investigators independently screened all titles and abstracts to identify studies that met the inclusion criteria and extracted relevant data. After this primary evaluation, two authors personally screened the reference list of previous reviews and metanalysis to identify possible eligible trials. Consecutively, a PICO (Population, Intervention, Comparison and Outcomes) strategy assessment of literature [26] was performed to search eventual other relevant studies that may have been ignored. The following terms were used for analysis: P (atrial fibrillation); I (surgical left atrium appendage closure); C (left atrium appendage closure); O (complete closure) (Fig. 4). Once individual studies were identified, efficacy and safety data were represented in the form of a simple pooled analysis. The lack of control groups in individual studies limited our ability to perform a meta-analysis of the presented data. Therefore, statistical significance for each measured variable could not be generated. Microsoft Excel (Microsoft 365 MSO, version 2305 Build 16.0.16501.20074, Microsoft Corporation, Redmond, WA, USA) was used for all data analysis, with categorical data expressed as frequencies and percentages (%) and continuous data expressed as mean. The risk of bias of this analysis was assessed by using the ROBVIS (Risk-of-bias VISualization) [27].
 Fig. 4.
Fig. 4.PRISMA Chart.
Two independent investigators (MDA and SR) extracted the following data from the included studies: authors, year of publication and baseline features, including type of surgical LAAC, time to follow-up evaluation, type of echocardiographic assessment, whether intraoperative assessment was performed and eventual imaging modality, rate of LAAC success. Since definition of LAAC success was not standardized and the results in terms of outcome differ between authors, the criteria used to determine LAAC success was included in the dataset. Literature search retrieved 1337 + 94 relevant reports, of which 42 included analyses of complete LAAC (cLAAC) at follow-up after surgical closure (Fig. 4).
Forty-two studies (see Table 1) were included in our analysis. The total number of patients underwent sLAAC was 5671, and in 3471 (61.2%) an imaging follow up was performed. Mean imaging follow-up was performed at 299.8 days (7 to 2082 days). Transesophageal echocardiographic (TEE) evaluation was performed in 28 of 42 studies, cardiac computed tomography scan (CT scan) in 10 of 42 studies, while 4 studies combined both imaging strategies according to patient characteristics, namely chronic renal impairment and stumps at TEE assessment (see Table 1).
However, these studies differ in patient selection methods, design, and, most importantly, definition of success rate.
Different definitions of success rate have been adopted by different authors for
evaluation of complete LAAC closure (cLAAC) at follow-up assessment. From 42
studies on this topic, 21 defined complete closure as full absence of leaks and
flow between LAA and left atrium [28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49]; 4 studies suggested a residual
flow
Of all valuated studies, 6 compared results of different techniques, while 36/42 reported success rate of the procedure. Clip deployment was valuated in 11 studies [31, 32, 33, 36, 37, 38, 39, 47, 63, 64, 68], reporting a mean success rate of 98% (range 93.9%–100%). Intraoperative imaging assessment of effectiveness of cLAAC was observed in 100% of patients (range 95.7%–100%), with a total population of 985 patients, of which 562 were also evaluated at follow-up. Fourteen studies [34, 35, 45, 46, 49, 50, 51, 52, 53, 54, 55, 56, 57, 59] investigated Lariat procedure (SentreHEART, Inc., currently Atricure Inc. Redwood City, CA, United States) and reported mean follow up rates of 88% (range 66%–100%), while intraoperative success was obtained in 98% of patients (range 93%–100%). A total of 2087 patients underwent Lariat procedures, and 80% underwent imaging follow-up. Surgical amputation was evaluated in 3 studies [29, 60, 69], with a mean success rate of 91% (range 73%–100%). Complete LAA closure through endocardial suture was obtained in 74.3% of cases (range 23%–100%), analyzed in 6 studies [29, 30, 44, 47, 60, 69], while Epicardial suture [3, 29, 40, 65, 67] obtained a success rate of 65% (range 41%–100%). LAAC ligation, evaluated in 5 studies [41, 42, 43, 61, 62], has proven to be a little more efficient, with a success rate of 60.9% (range 25%–94.7%). Results of the stapler technique were analyzed both with and without excision of the LAA: stapler exclusion with excision of the LAA was evaluated only in 1 study [60] with a success rate of 100%, while stapler without excision, evaluated in 6 studies [3, 28, 29, 65, 66, 69], had a success rate of 70%, although it may be considered less predictable (range 0%–100%).
The techniques of sLAAC can be divided according to the surgical approach into epicardial, endocardial and hybrid procedures (Figs. 2,3).
Within the macro-area of epicardial surgical approach to LAAC, we may identify exclusion techniques, with sutures or devices and excision techniques. Oversew is one of the simplest techniques to perform LAAC: it’s based on the mobilization of the base of the LAA, to increase the distance between the base of the suture and the circumflex artery, followed by the closure of the LAA with a vascular clamp, therefore 2 nonabsorbable, braided, 2-0 ligatures are applied and knotted with a distance of 5 mm from each other [70]. Another possible epicardial suture technique is the Purse-string suture exclusion (Fig. 3D): the base of the LAA is carefully mobilized and a purse string suture (generally nonabsorbable, braided, 2-0 suture), mostly reinforced with PTFE felt pledgets, is placed and then tied at the base of the LAA [71].
Different devices have been used and validated to LAAC. Surgical non-cutting
staplers, with or without pericardial buttressing, require careful positioning at
the neck of the LAA, with the closing mechanism that provides a rapid and precise
closure of the appendage. A bovine pericardial strip can be used to reinforce the
staple line. Endoloop snaring consists in a detachable snare loop (Endoloop)
positioned at the base of LAA and secured [72] (Fig. 3A). LigaSure
vessel-sealing system (epicardial welding) (LigaSure Xtd
Epicardial excision techniques include left atrial appendectomy/surgical cut-and-sew amputation, a strategy based on the amputation of the LAA at the base by excision, and the neck of the LAA is therefore oversewed in multiple fashions, such as running/mattress suture, with single or double layers, with or without pledgets reinforcement (Fig. 3C). Surgical cutting staplers, with or without pericardial buttressing, which is the same procedure described for non-cutting stapler, but in this case the appendage is removed (Fig. 3B).
Different endocavitary techniques have been described to perform LAAC. One of the most used is Endocardial suture ligation, with or without amputation: through a left atriotomy, a single or double-layer suture is placed at the base of the LAA, in a running or mattress-like fashion. Another possibility is an Endocardial Purse-String Suture in which an endocardial suture ligation is generally performed with a monofilament, non-absorbable 3-0 suture, with or without PTFE reinforcement [74]. Other described techniques are Closure through autologous or bovine pericardial patch, performed in cases of a large base of the LAA: a patch exclusion may be performed through a non-treated autologous or bovine pericardium patch using 4-0 polypropylene running suture technique; and Invagination and double-suture technique, performed through invagination of the LAA, generally though suction [48], into the LA, with 2 purse-string sutures positioned at the base to permanently prevent its evagination [75].
Hybrid procedures combine a percutaneous, generally subxiphoid, approach to an endocardial one and in this regard Lariat procedure (SentreHEART Inc, Redwood, CA, USA) is the most performed. Access to the pericardium is performed through a subxiphoid approach, with needle directed in anterior-lateral direction. An occlusion balloon, back loaded with a magnet-tipped endocardial guide wire, is positioned in the LAA through transseptal puncture under fluoroscopic guidance. The magnet-tipped epicardial guide wire is inserted into the pericardial space and attached to an endocardial magnet-tipped guide wire. The snare is then advanced over the epicardial wire and positioned over the LAA. Snare positioning at the ostium of the LAA is guided by balloon location at the opening of the LAA and confirmed with TEE assessment. The snare is therefore closed and a left atriogram is performed to assure the absence of a stump. Surgical suture is tightened to ligate and exclude the LAA. The Lariat snare is removed from the pericardial space and cutted [53]. Evidence on the results of sLAAC is mostly derived from non-randomized case series, monocentric observational cohort studies or retrospective registries with limited follow-up. Those results are often marginal and sometimes conflicting, and there is a selection bias due to the limited population of this studies compared to the wide use of LAAC devices. However, current guidelines for the management of AF still recommend surgical occlusion or exclusion of the LAA for stroke prevention in patients with contraindication for long-term anticoagulant treatment (Class IIb, Level B) and in patients undergoing cardiac surgery or thoracoscopic AF surgery (Class IIb, Level C) [76].
To identify eventual biases and highlight possible failures of the described techniques, here we present a discussion of the studies with lower success rates.
Cullen and colleagues [29] retrospectively reviewed patients undergoing TEE within 30 days from cardiac surgery and surgical LAA to guide cardioversion. Their rate of LAA patency was higher after suture closure compared to surgical excision or stapler closure, with an overall incidence of patency of 37%. One of the possible biases in this study is the small number of patients for the different surgical techniques (7 patients underwent Stapler exclusion, 23 LAA amputation), associated with the retrospective nature of this study, and the selection of patients who experienced post-operative AF.
Kanderian and colleagues [69] studied 137 of 2546 patients who underwent LAA closure with TEE follow-up. An exclusion technique was adopted in 52 (38%), while 85 (62%) received an excision procedure, of which 80% had scissor excision and oversew and 20% had cutting stapler excision. Rate of successful closure reached 40%, with 60% of suture exclusions failed due to persistent flow on TEE, and 60% of the stapled exclusion failed for large remnant. This study indeed highlighted the importance of a complete LAA occlusion, since 41% of the patients with unsuccessful closure had LAA thrombus formation compared with 0% of the successful closure group and 0% of the excision group. This well-known study reports the lowest success rate in literature, especially regarding exclusion endocardial suture, that has a success rate of 23%. Possible biases of this studies regard patient selection and the retrospective nature of the study: only patients that underwent TEE for other causes (that include, aortic dissection, transient ischemic attack [TIA], endocarditis, left ventricular thrombus) were included, therefore only 5.4% of patients that underwent surgical LAAC were evaluated. Suboptimal patency rate for internal ligation was evidenced also by Lee and colleagues [60]: even if it was performed on a small number of patients (N = 8), it evidenced a patency rate of 43%. Other techniques valuated in this study designed as a randomized, prospective trial (Amputation and Stampler Excision), revealed good outcomes with a complete closure of 100%.
Katz and colleagues [61] studied 50 patients who underwent LAA ligation and concomitant mitral valve surgery. The technique applied for LAA ligation was the endocardial suture exclusion, and the results evidenced that 36% of LAA ligations were incomplete: 50% of the unsuccessful closures had spontaneous echo contrast or thrombus in the LAA and 22% had thromboembolic events.
García-Fernández and colleagues [43] reviewed 58 patients that underwent mitral valve surgery and concomitant LAA ligation, with a group control of 147 patients who underwent isolate mitral valve surgery. The incompletely occluded LAAs rate was 10.3%, with evidence that no LAA occlusion and incomplete LAA occlusion were major risk factors for the development of thromboembolic sequelae at follow-up.
Among studies valuating Lariat procedure, 2 evidenced significantly worst success rates [52, 59]. Fink and colleagues [59] performed a retrospective study in 44 patients that underwent LAA ligation with Lariat, with 35 patients that underwent TEE follow-up, and a patency rate of 34%. As stated by the authors, the institution had no previous experience with this device, and this may explain the obtained results, since those patients may be part of the learning curve of the center. Miller and colleagues [52] experienced similar patency rates (74%). Their analysis, even if performed on a small population (41 consecutive patients), included 4 centers, therefore few procedures were performed at each center: possible learning curve may be evidenced also by the high rate of complication, in particular perforation of LAA, that occurred in 9% of the patients, with 50% of them requiring open surgical correction.
Two studies reported low success rate for epicardial surgical ligation [41, 42]. Adams and colleagues [42] performed LAA ligation with an Endoloop® suture ligature (Johnson & Johnson, Cincinnati, OH, USA) on 12 patients. Surgery was performed by a single operator, and, at 3-month follow-up, CT scan evidenced a rate of LAA patency of 75%, even if intraoperative TEE was negative. As correctly stated by the authors, possible explanation for these findings may be: edema of the LAA, induced by cardiopulmonary bypass, that reduces over time, possibly leading to a re-establishment of a connection between LA and LAA; suture ligature not placed deep enough on the base of the LAA due to concern to the circumflex coronary artery. One possible bias may be in the choice of CT for follow-up evaluation, that, as stated, maybe too sensitive in detecting a communication, and no TEE evaluation was performed to complete the analysis. Aryana and colleagues [41] valuated, with CT angiography imaging, 72 patients after LAA ligation in conjunction with mitral valve/AF surgery in a single-center, nonrandomized analysis. Surgical ligation was performed by 5 experienced operators with an oversewing technique with a double-layer of running Prolene suture. As stated from the authors, CT angiography has not been validated as the test of choice for LAAC closure assessment; however, it was able to detect incomplete LAAC in 24% of the patients, with a residual stump in 12% of the patients. Oversewing technique evidenced not-so-brilliant results also in the analysis of Lin and colleagues [40] and Güner and colleagues [67]. The former was a retrospective analysis of 193 patients that underwent TEE after surgical LAAC for any reason. The oversewn technique was performed with a double layer of running suture with or without excision of the LAA (and without any reference of relative frequencies). The main bias of this study, as correctly stated from the authors, is that of patient selection, since only patients that required TEE for any reason were included in this study, including possible endocarditis and stroke/TIA (8/74) [40]. Similar results were evidenced also by Güner and colleagues [68], with a procedural success rate of 65.3%. This multicentric, retrospective study, analyzed oversewing technique with a double-layer of running prolene suture. The inability to review TEE of all patients that underwent LAAC limited the population to 101 patients, therefore the percentages might not be representable to all patients undergoing surgical LAAC.
Stapler devices were valuated both in the studies of Fu and colleagues [66] and Healey and colleagues [65].
The study performed by Fu and colleagues [66] is a single-center, prospective
cohort study that assesses the safety and efficacy of thoracoscopic LAA. LAAC was
performed on 257 consecutive patients with a thoracoscopic-assisted bilateral
intercostal approach, without cardiopulmonary bypass. The stapler used (Johnson
& Johnson EZ-45G, New Brunswick, NJ, USA) employs 2 lines of staples to resect
and suture the LAA. At 3- and 12-months TEE assessment, success rate was 76.7%,
considered as eventual residual stump
Overall, surgical rates of complete closure in our analysis were 82%, with variable results depending on the surgical technique used. In addition, most of the studies included in this analysis are retrospective in design and performed mostly in single centers, and tendentially with few patients, therefore wariness must be practiced about sLAAC failure rates.
Some explanations have been proposed for the high rate of incomplete sLAAC, and in particular for endocardial suture: cautious suture bites may be positioned a little higher and more superficial in the atrial wall to avoid the circumflex artery and there may be a technical difficulty to reach the distal edge of the LAA, in particular in patients that present a mitral valve annuloplasty ring or prosthesis [77]. Furthermore, oedema due to the surgical gesture may justify LAA recanalization at follow up, and different LAA morphologies may be responsible for an incomplete closure of the ostium. Internal ligation is mostly associated with gap at follow-up, due to tears through the tissue, especially if the patient is in sinus rhythm, while excision, either surgical or stapled, are mostly associated with stump evident at intraoperative evaluation [60].
Difficulty in evaluating sLAAC may be due also to the different thresholds used
to identify incomplete closure by different authors, and to the absence of a
routinary TEE evaluation at follow-up. The recently published SCAI/HRS Expert
Consensus Statement on Transcatheter LAAC [78] identifies
Evidence of the potential benefits of sLAAC are results of LAAOS III (Left Atrial Appendage Occlusion Study) [80], which is a large prospective, multicenter Randomized Controlled Trial (RCT) evaluating the effect of LAAC on neurological complications. This study evidenced that, in AF patients that underwent cardiac surgery, sLAAC was associated with lower incidence of neurologic complications. This study, however, did not perform an imaging evaluation of LAAC closure at follow-up, therefore it adds little to the evaluation of the different surgical techniques. Furthermore, a magnitude of techniques were accepted, and no evaluation is performed based on the surgical strategy adopted.
The same issue, the absence of LAAC evaluation at follow-up, may be evidenced in another recent, prospective, multicenter RCT, the ATLAS Study (AtriClip® Left Atrial Appendage Exclusion Concomitant to Structural Heart Procedures) [81] that evaluates the impact of post-operative AF in patients that had no surgical LAAC and patients who underwent LAAC with AtriClip. This study recruited patients with no previous history of AF, although this “protective” treatment is not recommended by latest guidelines. ATLAS demonstrated the safety and effectiveness of Atriclip for LAAC and a potential protective effect of LAAC on postoperative AF (POAF): in LAAC group, even if POAF rate was higher, incidence of thromboembolic rate was lower.
Hopefully, a definitive answer on the role of preventive LAAC in patients undergoing cardiac surgery for another indication will be provided by the Left Atrial Appendage Exclusion for Prophylactic Stroke Reduction (LeAAPS) (NCT05478304) [82] that will evaluate thromboembolic events in 6500 patients with increased risk for stroke and AF, randomly assigned to LAAC with AtriClip or not. Evaluation at follow-up of results of surgical closure, however, will not be included in the primary outcomes [83].
Several biases may be evidenced in this review, as summarized in Fig. 5 (Fig. 5A,B). In particular, the studies reported are mostly single center, retrospective case series, where no randomization is performed. Therefore, to estimate the risk of bias of this analysis, we used the ROBVIS (Risk-of-bias VISualization) [27].
 Fig. 5.
Fig. 5.ROBVIS: Risk-of-bias VISualization. (A) Traffic Light Plot for risk of bias domains. (B) Weighted bar plots of the distribution of risk-of-bias for each domain.
As expected, considering the typology of article included in this review, a selection bias is particularly evident: not all patients included in the studies were included in the analysis, contrarily to what is expected from a target randomized trial. Considering the post-intervention domains, the most urgent bias may be a bias due to missing data, since follow-up evaluation is not complete for all individuals initially included and followed, and particularly a bias in measurement of outcomes, since the reported cut-off for LAAC failure differ greatly from different authors, and also the modality of imaging varies in the different studies. In addition, most of the studies reported evaluate LAAC combined with other surgical procedures, and, as stated from the Cochrane Risk of Bias guidance [84], co-interventions are a potentially important source of bias, even if stand-alone LAAC has been validated only in the most recent guidelines [76].
In general, this review highlights the absence of unified criteria for LAAC complete closure, that does not allow a proper comparison of the results described in the scientific literature with different techniques, along with absence of LAAC evaluation as primary endpoint in most of the reported studies: patients frequently underwent imaging follow-up due to clinical reason, and therefore this may alter the reported results of the surgical procedure.
The increasing prevalence of AF and the increased morbidity and mortality related to thromboembolic stroke have resulted in intensive research on stroke prevention and stroke related-risk reduction strategies, with a renewed interest in the possible surgical strategies for LAA occlusion. These techniques, initially performed only as a concomitant procedure during open-heart surgery, are now including some stand-alone surgical procedures in minimally invasive settings to directly address LAA.
However, data on the safety and feasibility of surgical LAA occlusion are poor and with conflicting results.
Evaluation of surgical techniques, their standardization, univocal cut-offs for failure and a definite follow-up assessment are essential to increase the reproducibility and therefore expand the potential of this procedure. If further validated on large-scale non-retrospective and multicentric studies, this promising surgery may offer a valuable alternative for patients with AF and ineligible for oral anticoagulation therapy.
MDA, SR and AGMM designed the research study. MDA and SR performed the research and wrote the manuscript. SS, WS, FS, NB and PDO provided help with tables and content. FM and FrM, MP, EG,GF analyzed the data and revised it critically. FM, FrM and AGMM revised the article critically for important intellectual content. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest. Mariangela Peruzzi is serving as Guest Editor of this journal. We declare that Mariangela Peruzzi had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Buddhadeb Dawn.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.