


 , Georgios Tzanis 3,†, Εleftherios Karatzanos 3, Michael Koutsilieris 2, Serafim Nanas 3, Anastassios Philippou 2,*
, Georgios Tzanis 3,†, Εleftherios Karatzanos 3, Michael Koutsilieris 2, Serafim Nanas 3, Anastassios Philippou 2,*
1 Department of Life Science, European University Cyprus, 2404 Nicosia, Cyprus
2 Department of Physiology, Medical School, National and Kapodistrian University of Athens, 11527 Athens, Greece
3 Clinical Ergospirometry, Exercise & Rehabilitation Laboratory, Evaggelismos Hospital, National and Kapodistrian University of Athens, 11527 Athens, Greece
†These authors contributed equally.
Abstract
Background: Peripheral myopathy consists a hallmark of heart failure
(HF) and has been associated with poor prognosis. Inflammation has been suggested
to dominate this pathology, while exercise training is typically associated with
the induction of anti-inflammatory mechanisms. However, the current knowledge
regarding the involvement of inflammation-related genes in the exercise
training-induced muscle adaptations in HF patients is very limited. Given that
high-intensity interval training (HIIT) alone or combined with strength training
(COM) has gained ground in HF cardiac rehabilitation, this study aimed to
investigate the local muscle expression of inflammatory and tissue remodeling
factors in HF patients, who underwent 3 months of these training schemes. In
addition, we examined whether these exercise training-induced gene expression
responses are associated with changes in exercise capacity in those patients.
Methods: Thirteen male patients with chronic HF (age: 51
Keywords
- heart failure
- cardiac rehabilitation
- inflammation
- skeletal muscle remodelling
Whilst heart failure (HF) is predominantly a disorder of central haemodynamics
[1], it has been demonstrated to induce deteriorating effects on multiple
peripheral tissues including skeletal muscle [2]. Indeed, there is growing
evidence suggesting that HF leads to structural and functional alternations
within skeletal muscle resulting in muscle cachexia [2, 3], which has been known
as ‘the muscle hypothesis’ of chronic HF [4, 5]. Indeed, Fülster
et al. [6] reported that one in five HF patients experienced muscle
wasting, including those with reduced and preserved (
Systemic and local inflammatory responses appear to be involved in early but
also advanced stages of this pathology [7]. Specifically, studies have shown an
inverse correlation between the level of inflammatory cytokines, tumor necrosis
factor (TNF)-1
Inflammation has been identified as the mechanism by which exercise training-induced skeletal muscle repair and hypertrophy is initiated [12, 18, 19]. Briefly, following muscle-damaging exercise muscle fibers secrete pro-inflammatory factors that recruit immune cells to scavenge muscular debris, allowing muscle regeneration and tissue remodeling [13, 18, 19]. A crucial balance between pro-inflammatory and anti-inflammatory factors appears to attenuate an excessive inflammatory reaction and interactive cytokine responses promote the progression or resolution of muscle inflammation [14]. In HF patients, although there is wealth of evidence demonstrating a reduction of circulating cytokines following exercise training [20, 21], however only one study has measured the levels of intramuscular pro-inflammatory markers following a 6-month exercise training program [22]. In that study a decrease in pro-inflammatory gene expression in the exercised muscles has been reported post-training, along with the absence of monocytes/macrophages infiltration in them [22], suggesting a possible adaptive downregulation of the local inflammatory program as part of the tissue remodeling process.
Interestingly, exercise characteristics, such as type and intensity, as well as the duration of exercise training, is likely to trigger different inflammatory responses [23]. For instance, strenuous and/or resistance exercise have been associated with greater muscular adaptations predominantly due to a larger extent of exercise-induced muscle damage [23]. Notably, superior muscular and cardiopulmonary adaptations following high intensity interval training (HIIT) and/or strength training compared to traditional aerobic exercise of moderate intensity has also been documented in patients with HF [24, 25, 26, 27]. Thus, according to the most recent guidelines of European Society of Cardiology-ECS (2020) [28] and American Heart Association-AHA (2017) [29], combined strength and aerobic training protocols have now been graded as a Class I recommendation in the treatment of HF patients. Nevertheless, there is lack of information regarding the intramuscular responses of inflammatory and tissue remodeling factors potentially as part of the local adaptive mechanisms induced by such exercise protocols in patients with HF.
Our group has previously found an overall increase in exercise capacity, muscle hypertrophy and capillarization in patients with HF that followed 3 months of either a HIIT or a combined HIIT with strength training program [24, 30]. Based on that evidence, the present study investigated further whether intramuscular inflammation and tissue remodeling factors contribute to those adaptations, advancing our understanding on the molecular pathways that mediate beneficial effects of exercise training on skeletal myopathy in HF patients. Specifically, we investigated and compared the effects of the same HIIT versus combined HIIT with strength training (COM) programs [24, 30] on the transcriptional changes in inflammation- and tissue remodeling-associated factors in skeletal muscle of stable HF patients. In addition, this study examined the potential associations between those gene expression responses and changes in exercise capacity in these patients.
Thirteen male patients with stable HF [age 51
Specific components of the present study have been previously published regarding the effects of exercise training on muscle hypertrophy [24] and angiogenesis [30] in the HF patients. The current work aimed to examine the gene expression of inflammation- and tissue remodeling-related factors in skeletal muscle of these patients in response to exercise training, in order to further characterize the molecular effects of exercise-based cardiac rehabilitation on HF-induced skeletal myopathy. The baseline characteristics of the patients aa well as their medications are shown in Table 1 (Ref. [24, 30]).
| HIIT (N = 6) | COM (N = 7) | ||
|---|---|---|---|
| Age (years) | 47 |
53 | |
| BMI (kg/m |
27 |
27 | |
| HF etiology (ICM/non-ICM) | 2/4 | 3/5 | |
| NYHA (I/II/III) | 2/3/1 | 1/5/1 | |
| Weber class (A/B) | 3/3 | 3/4 | |
| VO |
21.1 |
20.0 | |
| LVESD (mm) | 43 |
47 | |
| LVEDD (mm) | 59 |
62 | |
| LVEF (%) | 37 |
38 | |
| PCWP (mmHg) | 9 |
11 | |
| mPAP (mmHg) | 19 |
21 | |
| RAP (mmHg) | 2 |
4 | |
| Hemoglobin (g/dL) | 14.5 |
13.9 | |
| CI (L/min/m |
2.2 |
2.3 | |
| Medications (%) | |||
| Amiodarone | 50 | 29 | |
| 100 | 100 | ||
| Diuretics | 67 | 71 | |
| ACE inhibitors/ARB | 100 | 100 | |
| MRAs | 100 | 100 | |
Values are given as mean
Detailed description of the design and methods of this study as well as of the exercise training protocols used are given elsewhere [24]. All participants underwent either the HIIT (N = 6) or the combined HIIT with strength (COM, N = 7) exercise training for 3 months, 3 sessions per week. Any missed sessions were compensated at the end of the 12-week scheduled program, so that each patient completed 36 exercise sessions. Both training protocols were of the same total duration (31 minutes). Muscle tissue biopsies were collected from the patients before and after the 3-month training program and transcriptional changes in inflammation- and tissue remodeling-related genes were examined.
Subjects performed an 8–12 min ramp-incremental exercise test, using a gas
exchange analyser (Quark PFT, Cosmed, Rome, Italy) as previously descripted [24].
Briefly, patients requested to perform incremental leg exercise, while oxygen
uptake (VO
At the beginning and 48–72 h after the last exercise training session of the program, percutaneous needle biopsies of the vastus lateralis muscle were obtained using the Bergstrom technique [31], snap frozen and stored, as previously described [24].
RNA extraction from muscle tissue samples and semiquantitative real-time
polymerase chain reaction (RT-PCR) were performed to identify differences between
mRNA expression before and after the 3-month training program. These procedures
and the real-time PCR parameters used are described in detail elsewhere [24]. The
primer set sequences used for the specific detection of each gene are given in
Table 2. Specifically, primers were designed against IL-6, IL-8,
TNF-1
| Target gene | PCR primer sequence | Product size (bp) |
|---|---|---|
| IL-6 | F: 5′-CCTGACCCAACCACAAATGC-3′ | 157 |
| R: 5′-ATCTGAGGTGCCCATGCTAC-3′ | ||
| IL-8 | F: 5′-CCACCGGAAGGAACCATCTC-3′ | 279 |
| R: 5′-TTCCTTGGGGTCCAGACAGA-3′ | ||
| TNF-1 |
F: 5′-AAGAGTTCCCCAGGGACCTCT-3′ | 229 |
| R: 5′-ACATGGAGTAGATGAGGGT-3′ | ||
| TGF- |
F: 5′-CTACTACGCCAAGGAGGTCAC-3′ | 236 |
| R: 5′-ATGGAGTCGTTGGCCACGA-3′ | ||
| uPA | F: 5′-GTCTACCTGGGTCGCTCAAG-3′ | 374 |
| R: 5′-CAGTGGTGGTTTTACGACAC-3′ | ||
| uPAR | F: 5′-CATGCAGTGTAAGACCAACGGGGA-3′ | 253 |
| R: 5′-TGAGACCGGCCCGACAGTGGTAT-3′ | ||
| GAPDH | F: 5′-CATCACTGCCACCCAGAAGA-3′ | 438 |
| R: 5′-TCCACCACCCTGTTGCTGTA-3′ |
F, Forward primer; R, Reverse primer.
Changes in the mRNA expression were assessed using two-way repeated-measures
ANOVA. Where significant F ratios were found for main effects or interaction
(p
Compared with the pre-exercise training values, the expression of IL-8
was significantly increased (p = 0.019), while these increases were not
different between the training groups (p = 0.167). In addition, after
the completion of the exercise training program there was an overall increase of
the TNF-1
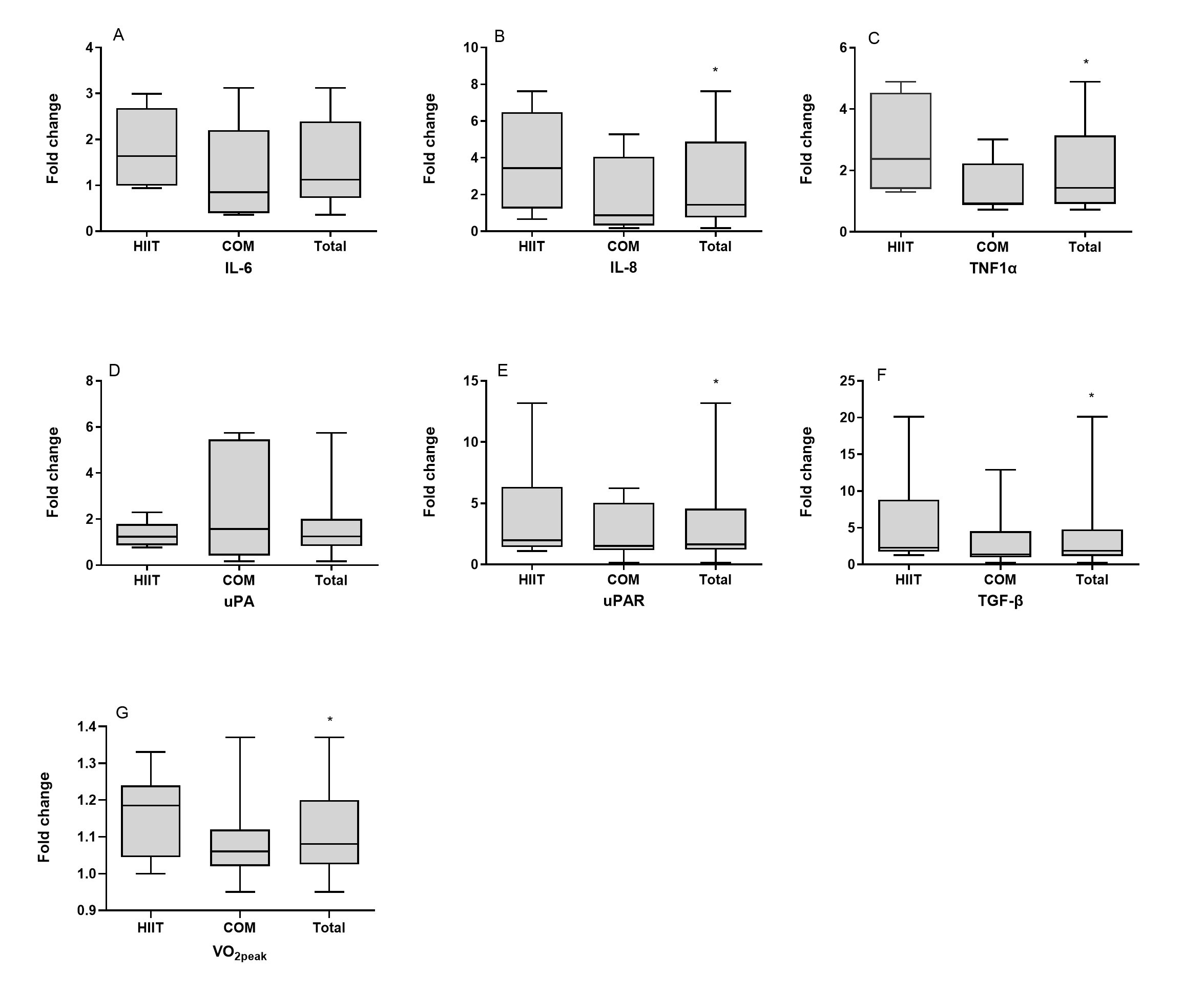 Fig. 1.
Fig. 1.Expression of inflammation- and tissue remodeling-related
factors after exercise training. The box-plot diagrams represent the fold changes
in the mRNA expression of (A) interleukin 6 (IL-6), (B) interleukin 8 (IL-8),
(C) tumor necrosis factor-1 alpha (TNF-1
Given that exercise capacity may possess a prognostic value for HF, we examined
the potential associations between the exercise training-induced fold changes in
the expression of the genes examined and the fold changes in exercise capacity
[VO
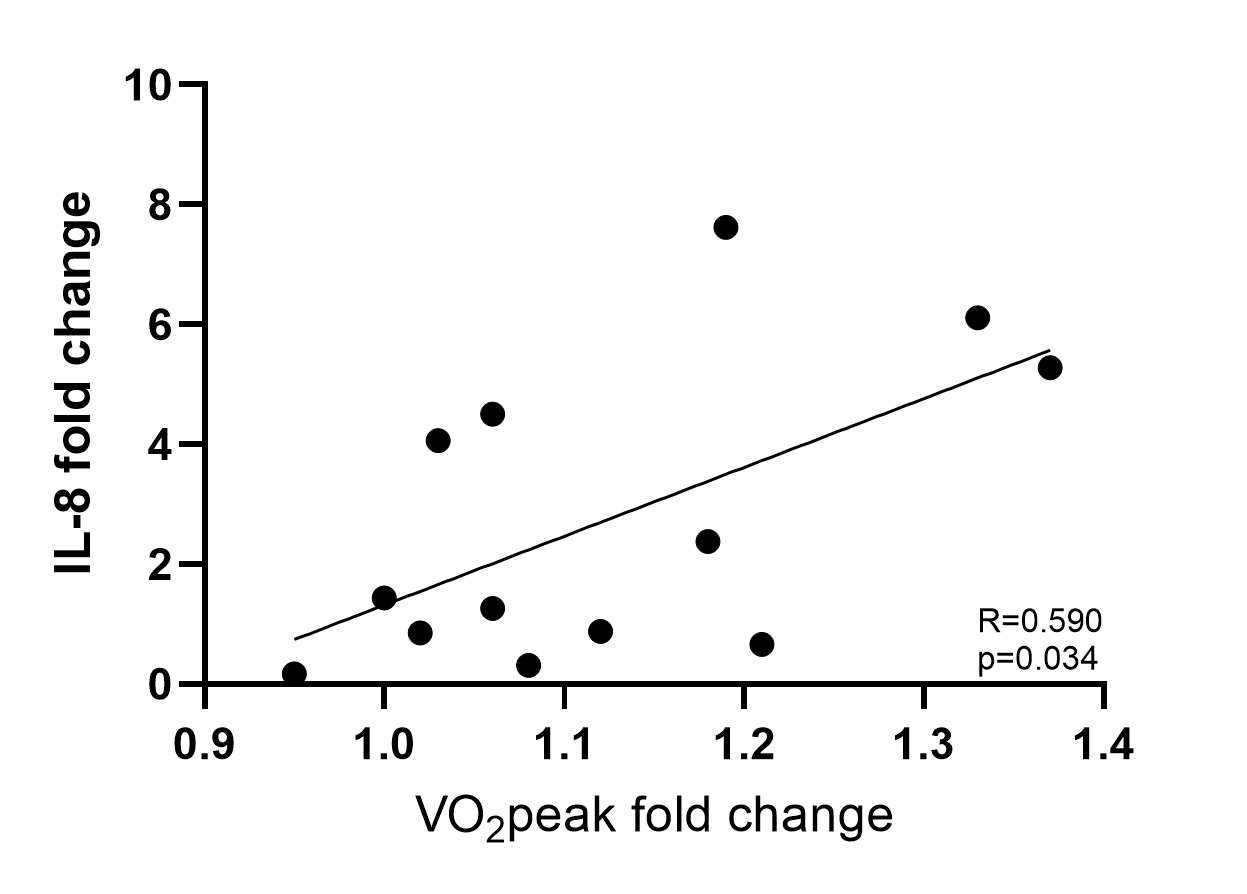 Fig. 2.
Fig. 2.
Association between the fold changes of interleukin 8
(IL-8) in the trained skeletal muscle and the changes in exercise
capacity expressed as fold change of peak oxygen consumption (VO
Skeletal myopathy occurred in HF patients is strongly associated with poor prognosis [6]. Inflammation has been suggested to dominate this pathology [7], while exercise training is typically proposed to counteract muscle cachexia modulating muscle inflammatory status [32, 33]. Nevertheless, there is a growing body of evidence documenting a beneficial role of exercise-induced intramuscular inflammation, which may be functionally related to muscle repair and growth adaptations [12, 13]. With regard to HF patients, however, most of the existing data have associated exercise training with systemic inflammatory profile [32, 33, 34] and only one study has directly measured local, intramuscular inflammation status following exercise training, in which patients requested to perform a traditional aerobic exercise on a daily basis [22]. Given the wealth of studies demonstrating the superior effects of HIIT or combined HIIT with strength training compared to traditional aerobic protocols in HF patients [24, 27, 35, 36, 37], the presented study was the first that investigated and compared the intramuscular expression of inflammatory and tissue remodeling factors following these specific exercise training schemes.
The main findings of our study were that 3 months of either HIIT or combined HIIT with strength training program resulted in similar increases in the expression of pro-inflammatory and tissue remodeling genes in skeletal muscles of HF patients. In addition, fold changes in the intramuscular IL-8 expression were positively correlated with the improvement of exercise capacity in these patients, potentially implying a beneficial role of exercise training-induced local inflammation, as part of an on-going remodeling process in the exercising muscles. Combining these observations with the induction of skeletal muscle hypertrophy [24] and angiogenesis [30] that we have previously reported in these particular groups of HF patients following the same exercise training protocols, we might assume that an intramuscular inflammation program may be associated with muscle remodeling and adaptations to exercise training.
Exercise-induced unaccustomed mechanical loading of skeletal muscle can
stimulate the activation of aseptic inflammation, the local production of
cytokines and the extracellular matrix (ECM) remodeling program [13], which
include pro- and anti-inflammatory factors, and factors of the TGF-
The present study showed a similar increase in pro-inflammatory cytokines
(IL-8, TNF-1
The findings of the present study further support a potential functional role of local inflammation in the exercise-induced muscle adaptations and clinical benefits, revealing that intramuscular increase of IL-8 following the 3-month cardiac rehabilitation was positively associated with the improvements in exercise capacity of these HF patients. Specifically, IL-8 has been found to act as a local messenger to promote angiogenesis via its receptor [47] and given our recent findings documenting elevated capillary density and increased angiogenetic activity in these patients [30], we might speculate that exercise training-induced IL-8 increase may be involved in the angiogenic/remodeling program of the exercised muscles, supporting the improvement of functional capacity of these patients. Indeed, increased muscular capillarization facilitates oxygen transport [48], which in return contributes to the improvement exercise tolerance. Although there are, yet, no studies showing a causative association of local IL-8 expression to exercise capacity, a recent study observed a positive relation between circulating IL-8 levels and improved performance in marathon runners [49]. Further studies are required to corroborate the potential beneficial role of intramuscular IL-8 expression in exercise training-induced adaptations particularly in patients with CHF.
Local muscle inflammation can activate tissue remodeling pathways and a
continuous coordination between inflammatory and remodeling factors is required
for an efficient structural remodeling and adaptation of skeletal muscle [50].
Specifically, components of the uPA/uPAR/TGF-
Overall, to the authors’ knowledge this is the first study that examined and compared the expression changes of key inflammatory and tissue remodeling factors in skeletal muscle after a HIIT or combined HIIT with resistance training program in patients with CHF, revealing a gene expression profile compatible with exercise-induced cellular and functional adaptations of the trained muscles that we previously had characterized in the same CHF patients [24, 30].
The potential of this study to detect significant differences between groups regarding the expression of the factors explored may be limited by its small sample size. Moreover, the ability to confirm the functional significance of the expression changes in the inflammation- and tissue remodeling-related factors at the protein level is limited by the transcriptional nature of the study and, thus, future studies are needed to evaluate this question. Overall, further studies are required to reach definite conclusions regarding the impact of the type of exercise-training, HIIT or HIIT in combination with strength training, on the induction of inflammatory and tissue remodeling factors in skeletal muscle, not only after the completion but also at various time points during the training programs in patients with CHF. It’s worth mentioning that an age-matched group (N = 13), which did not participate in any training program nor undergo muscle biopsies, had been also included in this study as a control group in comparison with the effects of both exercise training programs (HIIT and combined HIIT) as a whole on aerobic capacity [24]. Retrospectively, we think that this control group would have been utilized to compare the inflammatory/remodeling responses of skeletal muscle in those patients with the responses observed in the training groups of the study. Thus, further studies that will include a control group not participating in an exercise-based rehabilitation program are encouraged, to examine whether CHF patients exhibit an exaggerated inflammatory response to exercise, given their skeletal myopathy. Finally, our observations on exercise-induced inflammation have been limited to skeletal muscle and we did not collect information regarding systemic inflammation status. As such, further studies should also include parallel measurements of inflammatory factors in the circulation to characterize the overall inflammatory response to exercise training programs in CHF patients.
This study provided insights regarding the intramuscular molecular responses of key inflammatory and tissue remodeling factors to different exercise training programs, within the context of characterizing a potential network of biological processes that regulate the exercise-induced adaptive alterations of skeletal muscle in patients with CHF. These processes might ultimately counteract skeletal myopathy and improve exercise capacity of those patients. We found an overall upregulation of pro-inflammatory and tissue remodeling factors following both HIIT and combined HIIT with strength training program, which may suggest that inflammatory responses are part of an ongoing remodeling process in the exercising muscle. Given that these types of exercise training have gained significant ground in cardiac rehabilitation of patients with CHF, more studies are required to further describe the molecular signature of skeletal muscle adaptive remodeling during and after different exercise training programs in these patients typically characterized by muscle wasting.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Conceptualization—AT, GT, EK, SN, MK and AP; methodology—AT, GT, EK and AP; data curation and formal analysis—AT, GT and AP; writing—original draft preparation—AT; writing—review and editing—GT, EK, SN, MK and AP. All authors have read and agreed to the published version of the manuscript.
The study was approved by the Human Study Committee of our institution (No. 4522/20.11.07) and informed consent was obtained from all participants.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.