Background: The ratio of fibrinogen to -glutamine transferase
(FGR) was used to predict long-term prognosis in patients with coronary heart
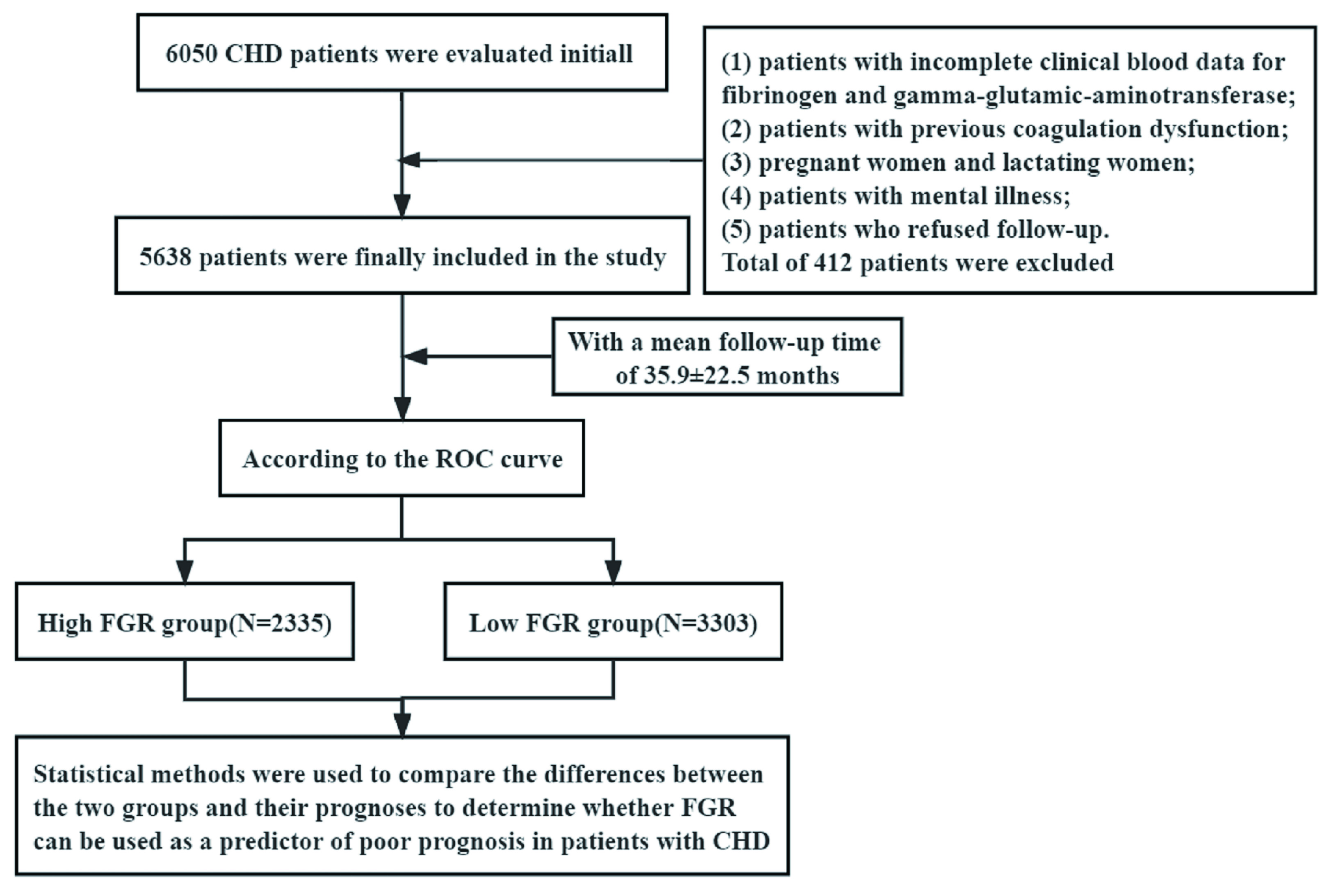
disease (CHD). Methods: A total of 5638 patients with CHD who were
hospitalized from January 2008 to December 2016 were retrospectively enrolled in
the study. The mean follow-up time was 35.9 22.5 months. The follow-up
endpoints were major cardiac and cerebrovascular adverse events (MACCE). The
optimal FGR cut-off value was determined and divided into high- and low-FGR
groups according to the receiver operating characteristic (ROC) curve.
Statistical methods were used to compare the differences between the two groups
and their prognoses to determine whether FGR can predict prognosis in patients
with CHD. The traditional predictors were incorporated into the logistic
regression model to observe the correlation between these indicators and
all-cause mortality (ACM) events. We compared the prediction performance of FGR
and traditional predictors on the occurrence of ACM events by ROC curves.
Results: The optimal cut-off value was determined via a ROC analysis
(FGR = 1.22, p = 0.002), and subjects were classified into high and low
FGR groups. The follow-up found that the incidence of MACCE in the high FGR group
was higher than that in the low FGR group. The COX multivariate regression model
showed that high FGR was independently correlated with the occurrence of MACCE.
In addition, the Kaplan–Meier survival curve showed that the risk of events was
significantly increased in the group with high FGR. With increases in the FGR
ratio, the risk of MACCE was increased. The ROC curve revealed that the risk of
ACM was statistically different between the FGR and the traditional risk factor
model (p = 0.002), (Fibrinogen (p = 0.008),
-glutamine transferase (GGT) (p = 0.004), and N-terminal pro
brain natriuretic peptide (NT-ProBNP) (p = 0.024)). The comparison
between other different models were not statistically significant (p
0.05). The area under the FGR model curve was larger than that of the traditional
risk factors, fibrinogen, GGT and NT-ProBNP models. Conclusions: High
FGR can increase the risk of MACCE in patients with CHD; additionally, it can be
used as a new biomarker for long-term prognosis in CHD patients. Clinical
Trial Registration: All details of this study are registered on the website
(http://www.chictr.org.cn), registration number: ChiCTR-ORC-16010153.