


 , Christoforos K. Travlos 1,†, Virginia Anagnostopoulou 1, Panagiotis Patrinos 1, Angeliki Papageorgiou 1, Angelos Perperis 1, Chris P. Gale 2,3,4, Konstantinos Α. Gatzoulis 5, Periklis Davlouros 1
, Christoforos K. Travlos 1,†, Virginia Anagnostopoulou 1, Panagiotis Patrinos 1, Angeliki Papageorgiou 1, Angelos Perperis 1, Chris P. Gale 2,3,4, Konstantinos Α. Gatzoulis 5, Periklis Davlouros 11 Department of Cardiology, General University Hospital of Patras, 26504 Patras, Greece
2 Leeds Institute of Cardiovascular and Metabolic Medicine, University of Leeds, LS2 9JT Leeds, UK
3 Leeds Institute for Data Analytics, University of Leeds, LS2 9JT Leeds, UK
4 Department of Cardiology, Leeds Teaching Hospitals NHS Trust, LS1 3EX Leeds, UK
5 First Cardiology Department, National and Kapodistrian University of Athens, Hippokration General Hospital, 11527 Athens, Greece
†These authors contributed equally.
Abstract
Background: Biventricular pacing (BVP) is recommended for patients with
heart failure (HF) who require cardiac resynchronization therapy (CRT). Left
bundle branch area pacing (LBBAP) is a novel pacing strategy that appears to
ensure better electrical and mechanical synchrony in these patients. Our aim was
to systematically review and meta-analyze the existing evidence regarding the
clinical outcomes of LBBAP-CRT compared with BVP-CRT. Methods: Medline,
Embase, Cochrane Central Register of Controlled Trials and Web of Science
databases were searched for studies comparing LBBAP-CRT with BVP-CRT. Outcomes
were all-cause mortality, heart failure hospitalizations (HFH) and New York Heart
Association (NYHA) class improvement. We included randomized controlled trials
(RCTs) and observational studies with participants that had left ventricular ejection fraction (LVEF)
Keywords
- left bundle branch area pacing
- meta-analysis
- resynchronization
Biventricular pacing (BVP) is recommended from the most recent European guidelines as the first-line pacing strategy in patients with heart failure (HF) that require cardiac resynchronization therapy (CRT) [1]. Many studies have shown its beneficial effects on morbidity and mortality in this population [2, 3]. However, 10% of patients cannot be treated by BVP due to having an unsuitable coronary sinus vein, while 30-40% are non-responders to BVP and experience no benefit from this treatment [4]. Conduction system pacing (CSP) has emerged as a solution to CRT downsides and is represented by His Bundle Pacing (HBP) and Left Bundle Branch Area Pacing (LBBAP). Current data demonstrates that HBP offers preservation or even restoration in intra or interventricular synchrony. Thus, it can be applied in HF patients, but it is technically challenging and related to high pacing thresholds [5].
LBBAP is a new pacing modality that can achieve narrow QRS and improve left ventricular function in patients with HF, by engaging the intrinsic conduction pathway of the heart [6]. According to existing evidence, LBBAP results in similar or even better improvement in the electromechanical synchrony compared with BVP [7] and is currently the globally prevailing method of CSP. Nevertheless, a study that systematically synthesizes and exclusively analyzes the effect of LBBAP compared with BVP in hard clinical outcomes is still lacking.
We conducted a systematic review and meta-analysis of observational and randomized controlled trials comparing the two pacing modalities to examine the effectiveness of LBBAP-CRT on all-cause mortality, heart failure hospitalizations (HFH) and New York Heart Association (NYHA) class improvement in HF patients who require CRT.
This systematic review and meta-analysis were performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The protocol of the present study was not registered. All data used and analyses performed in this systematic review and meta-analysis were based on previously published studies.
We systematically searched Medline, Embase, Cochrane Central Register of
Controlled Trials (via Ovid framework) and Web of Science databases from
inception to February 8, 2023, for studies comparing LBBAP with BVP for CRT in
patients with HF. Search terms were “left bundle branch pacing” AND
“biventricular pacing”. Clinical studies were included if they met the
following criteria: (1) randomized controlled trials (RCTs) or observational
trials that compared a LBBAP group (LBBAP-CRT) with a BVP group (BVP-CRT) for CRT
in patients with HF; (2) studies comparing all-cause mortality and/or HFH rates
and/or NYHA class improvement between the two
groups; (3) the participants of the studies should have (i) symptomatic HF with
left ventricular ejection fraction (LVEF)
We excluded: case reports, editorials, letters, review articles, congress
abstracts, animal studies, studies in individuals aged
Studies in which the study arm was referred as CSP and included both patients that received HBP and LBBAP were excluded as data exclusively for LBBAP could not be extracted and our aim was a pure comparison of LBBAP-CRT vs BVP-CRT.
The primary outcome was all-cause mortality from baseline to longest follow-up as defined in each study. Secondary outcomes were HFH and NYHA class improvement.
Articles were screened for inclusion by two independent investigators (CT and GL) who also extracted data on all-cause mortality, HFH rates and NYHA class improvement, using the same Excel spreadsheet. Data regarding study characteristics, number of participants, patient baseline characteristics, duration of follow-up, inclusion criteria and procedural success rate were also collected. For each continuous data type, the sample mean and standard deviation were extracted. If the results were reported as median and interquartile range, we converted them using the Wan’s et al. [8] method, into sample mean and standard deviation. Data for all outcomes of interest were extracted at the longest follow-up time point.
The quality of included studies was assessed by using the Newcastle–Ottawa
scale (NOS) for observational studies and the Cochrane Risk of Bias 2 assessment
tool (ROB 2.0) for RCTs. Data were pooled for each outcome of interest (mean
value, standard deviation and sample size for continuous variables and number of
events and sample size for dichotomous variables), to compare the outcomes
between LBBAP-CRT and BVP-CRT groups. Weighed mean difference (WMD) was the
effect measure for continuous variables while dichotomous variables were reported
as risk ratio (RR) and 95% confidence intervals (CIs) were used both for
continuous and dichotomous outcomes. A fixed-effects (Mantel–Haenszel)
meta-analysis was conducted if I
Sensitivity analysis was performed for all the outcomes to explore the consistency of the results, by removing one study at one time (“leave-one-out sensitivity analysis”).
In total, 769 studies were retrieved and 11 were included in this systematic review and meta-analysis [7, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18] (Fig. 1). Ten were observational studies [9, 10, 11, 12, 13, 14, 15, 16, 17, 18] and one was RCT [7]; all compared LBBAP-CRT with BVP-CRT providing data for outcomes of interest.
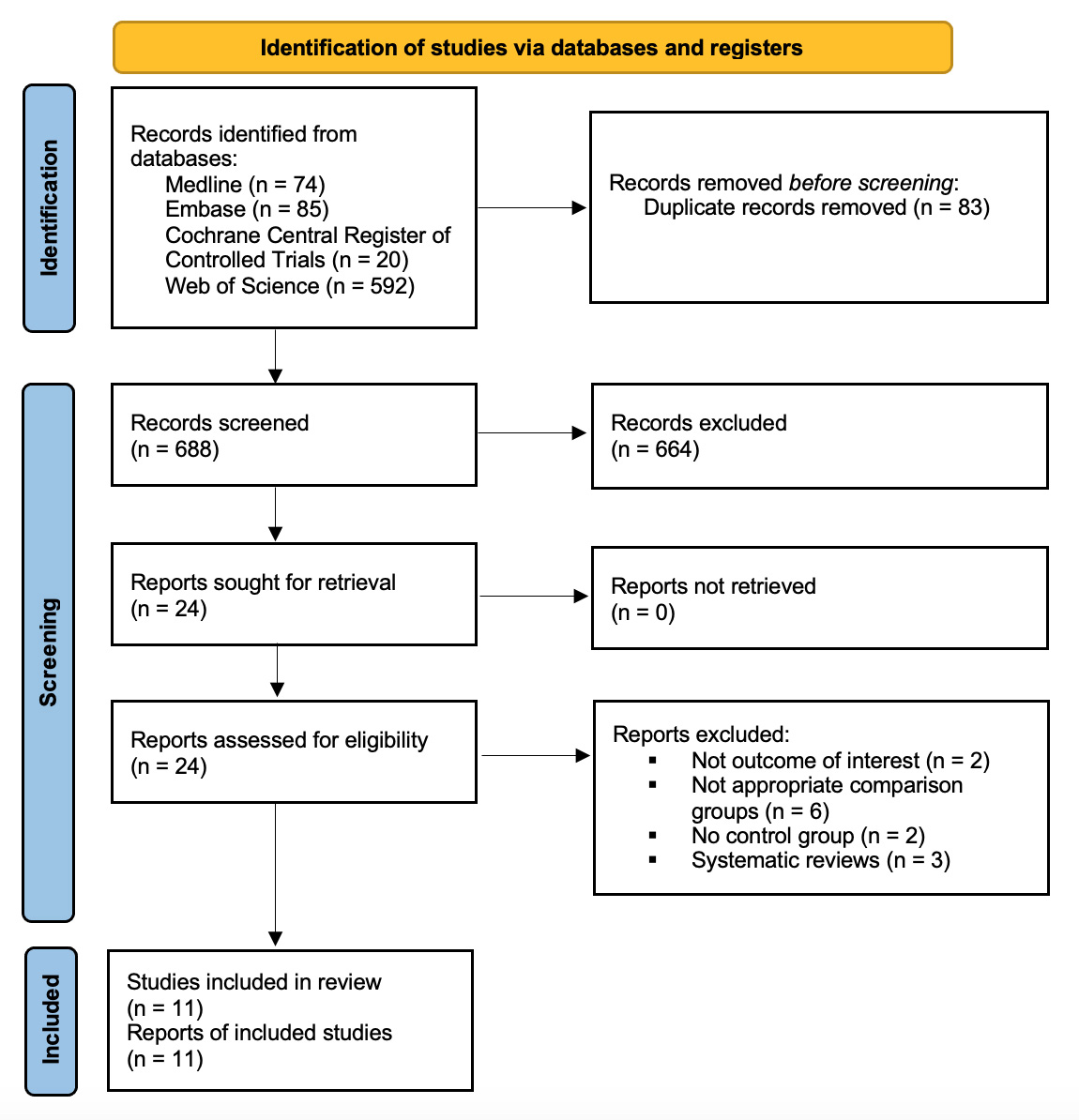 Fig. 1.
Fig. 1.Flow diagram of literature search.
Patient baseline characteristics are presented in Table 1 (Ref. [7, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18]). A
total of 3141 individuals were enrolled in these 11 trials (1290 in the LBBAP-CRT
group and 1851 in the BVP-CRT group). The mean follow-up duration was 14.6
| Study | Centers (n) | Country | Study type | Treatment group | Patients (n) | Follow-up, months | Age, years | Male, % | Baseline LVEF, % | NICM (n) | ICM (n) | AF (n) | Inclusion criteria | Procedural success rate % | NOS scale and ROB 2.0 |
| Chen et al. [9] 2022 | 4 | China | Observational, prospective | LBBAP-CRT | 49 | 12 | 67 |
49 | 29.05 |
36 | 13 | 4 | HF, NYHA II-IV, LVEF |
98 | 9 |
| BVP-CRT | 51 | 64 |
58 | 28.36 |
41 | 10 | 3 | NR | |||||||
| Diaz et al. [18] 2023 | 5 | International | Observational, prospective | LBBAP-CRT | 128 | 11 |
70 |
69 | 25.20 |
82 | 46 | 65 | HF, NYHA II-IV, LVEF |
84.4 | 9 |
| BVP-CRT | 243 | 70 |
71 | 26.70 |
243 | 100 | 122 | NR | |||||||
| Guo et al. [10] 2020 | 1 | China | Observational, prospective | LBBAP-CRT | 21 | 14 |
66 |
43 | 30.00 |
19 | 2 | 3 | HF, NYHA II-IV, LVEF |
87.5 | 9 |
| BVP-CRT | 21 | 65 |
43 | 29.80 |
19 | 2 | 1 | NR | |||||||
| Hua et al. [11] 2022 | 1 | China | Observational, prospective | LBBAP-CRT | 21 | 24 |
66 |
71 | 30.05 |
NR | NR | 5 | HF, NYHA II-IV, LBBB | NR | 8 |
| BVP-CRT | 20 | 68 |
75 | 31.40 |
NR | NR | 4 | NR | |||||||
| Li et al. [12] 2020 | 3 | China | Observational, prospective | LBBAP-CRT | 27 | 6 | 58 |
60 | 28.80 |
23 | 4 | 5 | HF, NYHA II-IV, LVEF |
81.1 | 8 |
| BVP-CRT | 54 | 59 |
60 | 27.20 |
46 | 8 | 11 | NR | |||||||
| Liang et al. [13] 2022 | 2 | China | Observational, retrospective | LBBAP-CRT | 154 | 31 | 67 |
61 | 32.30 |
126 | 28 | 46 | HF, NYHA II-IV, LVEF |
94 | 9 |
| BVP-CRT | 337 | 62 |
70 | 30.30 |
304 | 33 | 70 | NR | |||||||
| Rademakers et al. [14] 2023 | 1 | Netherlands | Observational, prospective | LBBAP-CRT | 31 | 6 | 68 |
48 | 28.00 |
20 | 11 | 9 | HF, NYHA II-IV, LVEF |
78 | 8 |
| BVP-CRT | 40 | 71 |
68 | 31.00 |
26 | 14 | 13 | NR | |||||||
| Vijayaraman et al. [17] 2023 | 15 | International | Observational, retrospective | LBBAP-CRT | 797 | 33 |
69 |
64 | 27.00 |
479 | 263 | 286 | HF, NYHA II-IV LVEF |
NR | 9 |
| BVP-CRT | 981 | 68 |
70 | 26.00 |
550 | 386 | 364 | NR | |||||||
| Wang et al. [15] 2020 | 1 | China | Observational | LBBAP-CRT | 10 | 6 | 65 |
90 | 26.80 |
9 | 1 | NR | HF, NYHA II-IV, LVEF |
100 | 7 |
| BVP-CRT | 30 | 63 |
77 | 26.38 |
27 | 3 | NR | NR | |||||||
| Wang et al. [7] 2022 | 2 | China | RCT | LBBAP-CRT | 20 | 6 | 62 |
35 | 28.30 |
20 | 0 | 0 | HF, NYHA II-IV, LVEF |
90 | Low |
| BVP-CRT | 20 | 65 |
65 | 31.10 |
20 | 0 | 0 | NR | |||||||
| Wu et al. [16] 2021 | 1 | China | Observational, prospective | LBBAP-CRT | 32 | 12 | 67 |
44 | 30.90 |
31 | 1 | 7 | HF, NYHA II-IV, LVEF |
NR | 9 |
| BVP-CRT | 54 | 68 |
54 | 30.00 |
47 | 7 | 11 | NR |
LVEF, left ventricular ejection fraction; AF, atrial fibrillation; HF, heart failure; CRT, cardiac resynchronization therapy; NYHA, New York Heart Association; BVP, biventricular pacing; LBBAP, left bundle branch area pacing; ICM, ischemic cardiomyopathy; NICM, non ischemic cardiomyopathy; NOS, Newcastle-Ottawa scale; ROB 2.0, Cochrane Risk of Bias 2 assessment tool; LBBB, left bundle branch block; NR, not referred; VP, ventricular pacing.
The outcome of all-cause mortality was studied in ten trials including 3045
patients. In the LBBAP-CRT group, 114 events were reported (9%) vs 214 in the
BVP-CRT group (11.9%). There was a statistically significant difference between
the two groups (RR: 0.71, 95% CI: 0.57 to 0.87; I
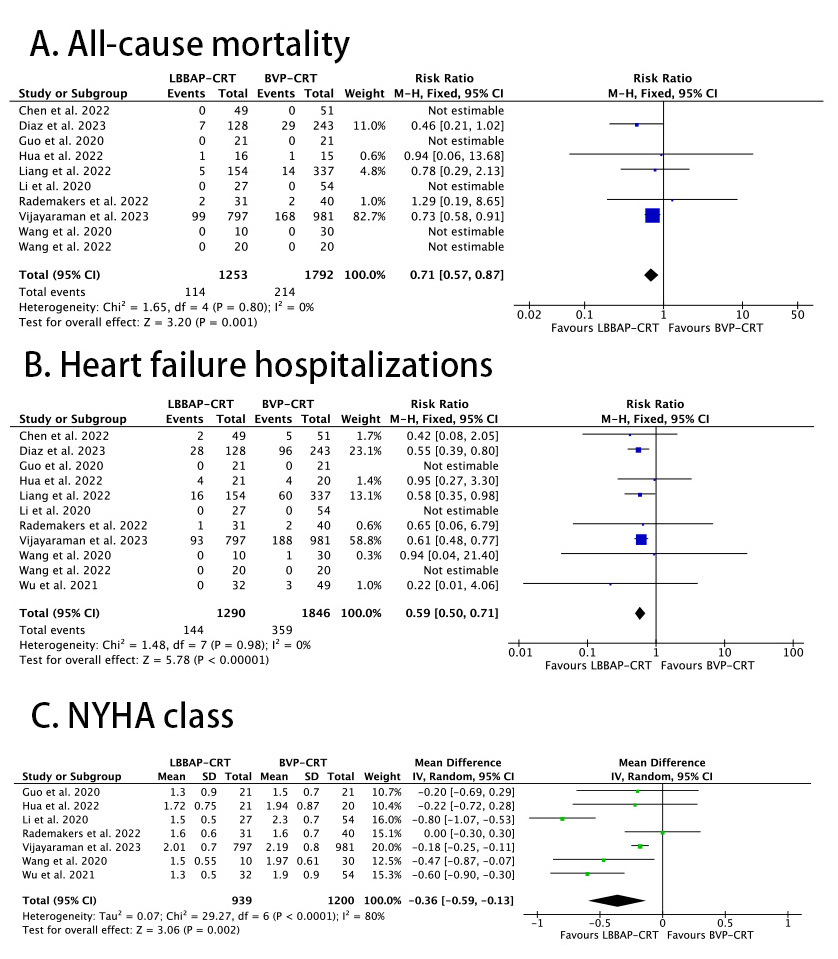 Fig. 2.
Fig. 2.Forest plots of LBBAP-CRT vs BVP-CRT for: (A) all-cause mortality; (B) heart failure hospitalizations; (C) NYHA class at longest follow-up. CRT, cardiac resynchronization therapy; NYHA, New York Heart Association; BVP, biventricular pacing; LBBAP, left bundle branch area pacing.
Sensitivity analysis was performed to explore the consistency of the results, by
removing one study at a time (“leave-one-out sensitivity analysis”). For the
outcomes of HFH and NYHA class improvement the results remained robust. For the
outcome of all-cause mortality, the result was found to be driven by Vijayaraman
et al., 2023 [17]. Excluding this study from the analysis, there was no
statistically significant difference between the two groups (RR: 0.61, 95% CI:
0.34 to 1.08; I
Reducing HFH symptoms and mortality is central to the management of patients
with HF. Evidence from RCTs demonstrated that receipt of BVP-CRT for HF is
effective in reducing mortality and HFH but does not allow the physiological
activation of ventricles that LBBAP-CRT does. Also, the significant rate of
non-responders to BVP remains an important drawback. A systematic review and
meta-analysis has demonstrated the superiority of conduction system
pacing—incorporating both HBP and LBBAP—compared to CRT in terms of
electrical resynchronization, left ventricular ejection fraction, NYHA class
improvement and rate of heart failure hospitalizations. All-cause death did not
show any statistically significant difference between the two groups and the mean
time of observation for this parameter was 11
A more updated systematic review and meta-analysis by Kim et al. [20] compared again CSP vs CRT in heart failure patients and the striking finding was a significant difference in all-cause mortality (odds ratio [OR] 0.68, 95% confidence interval [CI]: 0.56–0.83) with a median follow up time of 10.1 months. This discrepancy can be explained by the fact that more and larger observational studies were incorporated [17, 18].
Of note, both Vijayaraman et al. [17] (in multivariate analysis) and Diaz et al. [18] failed to demonstrate a clear benefit when analyzed separately on all-cause mortality.
Our aim was to focus strictly on LBBAP because it has now been adopted as the
first-choice method in CSP by the majority of the operators and seems that this
is the technique that will prevail over HBP in the future. In this systematic
review and meta-analysis of 11 studies, we found that LBBAP-CRT is associated
with lower mortality, lower risk of HFH than BVP-CRT and a greater improvement in
NYHA class than BVP-CRT. However, it has to be highlighted, as stated above in
the sensitivity analysis, that the outcome of all-cause mortality was mainly
driven by Vijayaraman’s study [17]. Another older retrospective study by
Vijayaraman including fewer centers, and as a result fewer patients, was
conducted showing a smaller benefit of CSP over CRT in HFH and no difference on
all-cause mortality. Moreover, the first chronological study had a follow-up of
27
Vijayaraman et al. [17] in his more recent study reports a lower death
rate (12% in CSP group vs 17% in BVP) compared to our meta-analysis (9% in
LBBAP vs 11.9 in BVP) The most reasonable explanation for this difference is the
longer follow-up period of Vijayaraman et al. [17] (33
All-cause mortality benefit is the quintessence of a therapeutic intervention in medicine. This meta-analysis cannot provide robust data that could affect our daily clinical practice in terms of resynchronization in HF patients. It does though generate a strongly based hypothesis that should be further validated in a large, randomized study designed and powered to demonstrate all-cause mortality benefit, if this finally exists. Until then, the data presented above about all-cause mortality benefit should be interpreted with caution.
A number of observational studies [9, 10, 12] and one RCT [7] have found that
LBBAP-CRT achieves better electromechanical synchrony in terms of QRS duration
reduction and improvement of echocardiographic parameters compared with BVP-CRT,
in the short-term follow-up. In BVP-CRT patients, electrical remodeling (native
QRS shortening
This short-term predominance of LBBAP-CRT in the limited existing evidence seems to be translated into better clinical outcomes in terms of HFH rate and improvement in NYHA class. In the largest so far, a study comparing LBBAP-CRT to BVP-CRT in HF patients, Vijayaraman et al. [17], reports a HFH rate of 12% in LBBAP-CRT vs 19% in BVP-CRT [17]. These results are similar to our meta-analysis (11.1% in LBBAP-CRT vs 19.4% in BVP-CRT). Moreover, Vijayaraman et al. [17] proceeded to complete a sub-analysis in patients that had a left bundle branch block (LBBB) on their baseline electrocardiogram (ECG), whilst only 61% of the patients in his cohort had LBBB preimplant. The benefit of LBBAP is numerically larger if LBBB preexists. These better results of LBBAP-CRT in NYHA class and HFH in LBBB patients may be due to the fact that LBBAP can completely correct LBBB by placing the lead beyond the block site while BVP-CRT reduces the QRS without correcting the LBBB. This advantage may be the reason for the better electromechanical parameters of LBBAP-CRT that can lead to better clinical symptoms improvement. As in all-cause mortality, large multicenter, randomized controlled trials in different subgroups of patients (ICM – non-ICM) are needed to shed adequate light regarding benefit in HFH rate and NYHA class improvement.
Our study has certain limitations. First, ten out of 11 included studies were observational studies (with biases of confounding by indication and confounding), and the one RCT included was not sufficiently powered for the outcomes of interest. Thus, data from the RCT were pooled with that from observational studies which can lead to some uncontrolled bias. Second, the majority of the studies had a small sample size which can lead to inaccuracy of the effects. Third, most of the studies had a short follow-up period which is in contrast with the outcomes of interest that are considered as long-term. Fourth, some studies that explored patients with conduction system pacing including both LBBAP and HBP were excluded as data strictly about LBBAP could not be extracted. Fifth, patients that received both an LBBP lead and an LV lead as an optimized resynchronization strategy (left bundle branch optimised cardiac resynchonization treatment-LOT CRT) were excluded from our meta-analysis. Sixth, the protocol of this systematic review was not registered, and this fact may be considered as a limitation.
In our study, we showed that LBBAP-CRT has better results in all-cause mortality, HFH, and NYHA class improvement compared with BVP-CRT. However, larger, multicenter, randomized controlled trials are needed to verify our results concerning the clinical outcomes of this novel pacing method in patients with HF requiring CRT.
Data are available upon reasonable request from the corresponding author at levent2669@hotmail.com.
GL, CT, CG, KG and PD had substantial contribution on the conception and design of the review and meta-analysis; CT, VA, PP, APa, APe contributed to the data acquisition and data analysis; GL CT contributed to the data interpretation; GL, CT, APa, APe contributed to the writing of the meta-analysis; CG, KG, PD reviewed critically the meta-analysis; All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
Not applicable.
This research received funding by RAYCAP S.A.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.