

 , Akash Patel 1
, Akash Patel 11 Department of Cardiology, St Mary Medical Center, Langhorne, PA 19047, USA
Abstract
Background: Epidemiological evidence suggests a J-shaped association between alcohol consumption and cardiovascular mortality, with higher cardiovascular event rates occurring among abstainers and heavy drinkers compared to moderate consumers. However, this hypothesis has been challenged by more recent studies. Furthermore, ethnicity, gender, type of alcoholic beverage, and pattern of alcohol intake, influence the relationship between alcohol and heart health. Methods: We undertook a review of the relavent literature utilizing PubMed. Results: Heavy alcohol consumption causes resistant hypertension, cardiomyopathy, arrhythmias, hemorrhagic strokes, as well as hepatic cirrhosis and pancreatitis. Excessive drinking is the third most preventable cause of death worldwide behind hypertension and smoking. Conclusions: In this review, we discuss the effects of alcohol abuse on hypertension (a major cause of myocardial infarction and stroke) and alcoholic cardiomyopathy. Another article in this Special Issue “Alcohol and Heart Health” discusses the problem with alcohol and arrhythmias sudden cardiac death.
Keywords
- alcoholic
- alcohol abuse
- cardiomyopathy
- hypertension
- heart failure
Alcohol, a psychoactive substance, has been a significant part of human culture for millennia. Throughout history it has been recognized for its harmful potential to individuals, as well as to society, due to its dependence-producing properties. Harmful alcohol consumption contributes to health, social, and economic burdens globally.
Significant alcohol consumption remains highly prevalent globally. In 2018, alcohol consumption averaged 6.4 liters of pure alcohol per person worldwide [1]. In the United States, 85% of individuals 18 years-old or older have consumed alcohol in their lifetime [2]. Furthermore, binge drinking, a major reason for alcohol related problems, is widespread. According to a United States governmental survey in 2019, 26% of individuals aged 18 and older reported binge drinking habits within the last month [3].
The abusive use of alcohol costs billions of dollars globally. In 2010, excessive alcohol consumption cost the healthcare sector approximately 28 billion dollars [4]. If damages related to workplace productivity, crime, and accidents were included, the costs is more than 250 billion dollars a year [4]. The World Health Organization (WHO) reported that excessive alcohol use is a risk factor for more than 200 diseases, accounting for more than 5% of the global burden of diseases and injuries [1]. Furthermore, it acts as a common risk factor for mental disorders and abnormal behavioral conditions [1]. The Organization for Economic Cooperation and Development Strategic Public Health Planning for Non-Communicable Diseases (OECD SPHeP-NCDs) model predicts that consuming more than 1 drink per day for women and 1.5 drinks per day for men will cause 24 million new cases of cardiovascular diseases, 10 million cancer cases,12 million new diabetes cases, and 37 million injury cases between 2020–2050 in 52 countries [5]. Consistent excessive drinking can lead to alcohol use disorder (AUD). Individuals with this condition consume too much alcohol despite the mental and physical harms. In USA, approximately 15 million individuals had been diagnosed with AUD [6].
Excessive alcohol consumption causes 3 million deaths yearly, and it accounts for 5% of all deaths worldwide. It was the 7th leading cause of early death globally in 2016 [7]. In addition, 14% of all deaths of individuals between age 20 and 39 in 2016 were alcohol consumption related [1]. Most alcohol attributable deaths (28.7%) in 2016 were due to injuries. Other complications were cardiovascular diseases (19%), liver cirrhosis and pancreatitis (21.3%), and cancer (12.6%) [1]. Due to increased alcohol consumption seen in adults worldwide, an increased focus needs to be placed on the cardiovascular harms of heavy drinking.
Heavy alcohol use is defined as greater than 4 drink per day or 14 drinks per week for men and greater than 3 drinks per day or 7 drinks per week for women [8]. While numerous studies suggest a cardioprotective effect of light to moderate alcohol consumption, especially on coronary artery disease, heavy alcohol consumption, abuse and binging, can negatively affect the cardiovascular system. Potential cardiovascular detrimental effects include congestive heart failure, dilated cardiomyopathy, sudden cardiac death and hemorrhagic stroke. Some of these cardiovascular complications are the result of alcohol-induced hypertension. In this review, we discuss the effects of alcohol abuse on hypertension (a major cause of myocardial infarction and stroke) and alcoholic cardiomyopathy. Another article in this Special Issue “Alcohol and Heart Health” discusses the problem with alcohol and arrhythmias and sudden cardiac death.
Hypertension is the most common medical condition in the world, with 1.28 billion cases in 2021 [9]. Hypertension is a major cause of premature death worldwide [10]. Moreover, many individuals with hypertension are unaware that they have it (~46%) [9]. It is a risk factor for stroke, cardiovascular and kidney diseases [9, 10]. According to WHO, increased alcohol consumption is a major risk factor for developing hypertension [9]. The correlation between alcohol consumption and hypertension had been investigated in cross sectional, cohort and epidemiological studies across various populations. Meta-analyses of these studies have also been performed and published in the last decade which provide the strongest evidence for an association between alcohol and hypertension.
Roerecke et al. [11] conducted a meta-analysis investigating the incidence of hypertension in moderate drinking individuals. Their analysis included 361,254 participants from 20 original cohort studies. They found the relationship between alcohol and hypertension is dependent on gender and dose. Any amount of drinking was shown to be associated with more hypertension in men. In women, no risk was found at 1 to 2 drinks per day, but greater risk was found at higher levels of consumption [11]. Similar results were observed by Aladin and colleagues [12]. They found that moderate drinkers (7–13 drinks/week) were at increased risk for stage 1 and stage 2 hypertension, when compared to never drinkers, in 17,059 subjects from NHANES III (Third National Health and Nutrition Examination Survey) [12].
Another meta-analysis by Roerecke et al. [13], investigating whether
reducing the intake of alcohol had any effect on blood pressure, studied data
from 36 trials. They demonstrated that individuals who had
McFadden and colleagues [14], studying the effects of daily alcohol consumption on blood pressure, found that there is a statistically significant increase in blood pressure immediately after alcohol intake.
Chen et al. [15] applied a Mendelian randomization approach to study the effects of alcohol on blood pressure in subjects with the alcohol dehydrogenase 2 (ALDH2) genotype (aldehyde dehydrogenase 2 is a major enzyme in alcohol metabolism). They concluded that alcohol intake had a significant immediate effect on blood pressure, as well as it increasing the risk for hypertension [15].
Jung et al. [16] recently conducted a regional analysis of the relationship between alcohol and hypertension. They found that the risk of hypertension is dose dependent in both Asian and western populations [16]. Further, hypertension risk is evident even at lower levels of consumption compared to recommended guidelines. Asian populations showed a higher risk of hypertension at low doses of alcohol compared to a western population [16]. Another meta-analysis showed that even at low to moderate doses of alcohol, men had an increased trend towards development of hypertension, when compared to women [17]. Table 1 (Ref. [18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29]) shows study characteristics for studies included in the above reviews and meta-analyses examining alcohol use and hypertension.
| Study | Study design | Country | Number of participants | % Men and women | Average age (years) | Alcohol consumption | HR/OR/RR (95% Confidence Interval) |
| Bae et al., 2002 [18] | Nested Case Control | South Korea | 988 | 100% Men | 40–59 | 71–280 g/week | OR: |
| 1.84 (1.31–2.56) | |||||||
| Sesso et al., 2008 [19] | Prospective Cohort | United States of America | 42,303 | 32% Men | Men: 52 | 5–6 drinks/week | RR: |
| 68% Women | Women: 53.8 | Men: 1.15 (1.04–1.27) | |||||
| Women: 0.90 (0.80–1.00) | |||||||
| Forman et al., 2009 [20] | Prospective Cohort | United States of America | 83,882 | 100% Women | 27–44 | 5.1–10.0 g/day | HR: |
| 10.1–15.0 g/day | 0.84 (0.78–0.90) | ||||||
| 15.1–29.9 g/day | 0.98 (0.91–1.07) | ||||||
| 1.11 (1.01–1.23) | |||||||
| 1.61 (1.42–1.82) | |||||||
| Ascherio et al., 1996 [21] | Prospective Cohort | United States of America | 41,541 | 100% Women | 38–63 | 20–29.9 g/day | RR: |
| 1.46 (1.21–1.76) | |||||||
| 1.32 (1.11–1.57) | |||||||
| Halanych et al., 2010 [22] | Prospective Cohort | United States of America | 659 | 56.6% Men | 18–30 | 7–14+ drinks/week | HR: |
| 43.4% Women | 1.33 (0.76–2.32) African-American Men | ||||||
| 1.47 (0.44–4.96) European-American Men | |||||||
| Peng et al., 2013 [23] | Prospective Cohort | China | 32,389 | 74.2% Men | 49.9 | 50–99 g/day | RR: |
| 25.8% Women | 100–149 g/day | 1.80 (1.63–2.00) | |||||
| 2.06 (1.83–2.31) | |||||||
| 2.28 (1.99–2.61) | |||||||
| Okubo et al., 2014 [24] | Prospective Cohort | Japan | 45,428 | 35.6% Men | 40–79 | 20–39.9 g/day | HR: |
| 64.4% Women | 20–59.9 g/day | Men: | |||||
| 1.29 (1.24–1.35) | |||||||
| 1.45 (1.39–1.52) | |||||||
| 1.57 (1.46–1.70) | |||||||
| Women: | |||||||
| 1.10 (1.03–1.17) | |||||||
| 1.14 (0.93–1.40) | |||||||
| 1.29 (0.89–1.87) | |||||||
| Diederichs et al., 2017 [25] | Prospective Cohort | Germany | 2231 | 47.5% Men | 18–79 | OR: | |
| 52.5% Women | Men: 2.88, p-value 0.014 | ||||||
| Women: 2.13, p-value 0.092 | |||||||
| Saremi et al., 2004 [26] | Prospective Cross Sectional | United States of America | 3789 | 34.2% Men | 36.3 | 1–2 drinks/day | HR: |
| 65.8% Women | Men: 1.20 (0.95–1.53) | ||||||
| Women: 1.48 (1.24–1.78) | |||||||
| Yoo et al., 2019 [27] | Prospective Cohort | South Korea | 6259 | 34.5% Men | 40–69 | HR: | |
| 65.5% Women | Men: 1.292 (1.033–1.617) | ||||||
| Women: 1.128 (0.652–1.952) | |||||||
| Fuchs et al., 2001 [28] | Prospective Cohort | United States of America | 8334 | 33.2% White Men | 45–64 years | 1 to 209 g/week | OR: |
| 40% White Women | White men: 0.88 (0.71–1.08) | ||||||
| 10.0% Black Men | White women: 0.89 (0.73–1.09) | ||||||
| 16.8% Black Women | Black men: 1.71 (1.11–2.64) | ||||||
| Black women: 0.88 (0.59–1.33) | |||||||
| Ohmori et al., 2002 [29] | Prospective Cohort | Japan | 267 | 39% Men | 40+ | 23–45 g/week | RR: |
| 61% Women | Men: 2.60 (1.50–4.49) |
Table notes: OR, odds ratio; HR, hazard ratio; RR, relative risk.
Thus, the risk of hypertension is dose dependent with higher use of alcohol contributing to higher hypertension risk. Other factors which contribute include gender, timing of alcohol consumption (e.g., binging), and genetics.
Alcoholic cardiomyopathy is a type of dilated cardiomyopathy (DCM) demonstrating increased left ventricular (LV) mass and decreased ventricular function. Alcoholic cardiomyopathy is similar to other dilated non-ischemic cardiomyopathies. The majority of alcohol abusers are asymptomatic for years. Most never develop clinical manifestations of congestive heart failure. However, most alcoholics do demonstrate preclinical heart muscle disease. Autopsies reveal dilated cardiomyopathic in alcoholics not experiencing symptomatic heart failure [30]. It has been estimated that 2% of heavy alcohol users ultimately develop symptomatic alcoholic cardiomyopathy. And because there are so many alcoholics, approximately 35% of all non-ischemic cardiomyopathies are caused by excessive alcohol use [31, 32, 33].
Data suggest that most alcoholics develop significant changes in cardiac function and myocyte structure after consuming on average greater than 90 grams of alcohol daily for at greater than 5 years [34, 35, 36, 37]. Cardiac damage due to longstanding heavy alcohol consumption is not beverage or quantity specific and varies depending on the population studied. Genetic and environmental factors play a role, as well as the specific beverage type used by a culture or individual.
Studies have examined the association between alcohol abuse and cardiomyopathy
[31, 32, 33]. In one case control study researchers found that 40% of DCM cases
were attributable to excessive alcohol use history [38]. In another case control
study by Komajda et al. [39], abnormal use of alcohol was found to be
strong predictor for cardiomyopathy cases irrespective of the type of beverage
used. Gillet et al. [40] found that the higher use of alcohol (
| Study | Study design | Country | Number of participants | % Men and women | Average age (years) | Alcohol consumption | HR/OR/RR (95% Confidence Interval) |
| Klatsky et al., 2005 [42] | Prospective Cohort | United States of America | 1035 | 44.4% Men | 74 | 1–2 drinks/day | RR: |
| 55.6% Women | 3–5 drinks/day | 1.0 (0.8–1.3) | |||||
| 1.2 (0.9–1.6) | |||||||
| 1.7 (1.1–2.6) | |||||||
| Park et al., 2018 [43] | Prospective Cohort | South Korea | 49,714 | 72.2% Men | 49.1 | 15–30 g/day | OR: |
| 27.8% Women | 30–60 g/day | 1.25 (1.08–1.44) | |||||
| 1.33 (1.15–1.54) | |||||||
| 1.32 (1.11–1.57) | |||||||
| Larsson et al., 2015 [44] | Meta analysis | United States of America Canada Sweden Finland | 6211 | Variable among studies | 21–85 | 14 drinks/week | RR: |
| 1.07 (0.77–1.48) | |||||||
| Whitman et al., 2017 [41] | Prospective Cohort | United States (California) | 268,084 | 68.6% Men | 48.8 | 7–14+ drinks/week | HR: |
| 31.4% Women | 2.34 (2.29–2.39) | ||||||
| Sidorenkov et al., 2011 [45] | Cohort Autopsy Study | Russia (Arkhangelsk) | 318 | 46.9% Male | 30–70 years | 7–14+ drinks/week | OR: |
| 53.1% Female | 1.36 (0.74–2.48) | ||||||
| Aguilar et al., 2004 [46] | Prospective Cohort | Canada United States of America | 2228 | 82.5% Men | 58 | 1–10 drinks/week | HR: |
| 17.5% Women | 0.93 (0.75–1.17) | ||||||
| 1.25 (0.91–1.72) | |||||||
| Li et al., 2016 [47] | Prospective Cohort | China | 10,824 | 46.1% Men | 54 | 1–2 drinks/day | OR: |
| 53.9% Women | 3+ drinks/day | 1.183 (0.774–1.808) | |||||
| 1.482 (1.117–1.965) | |||||||
| Yousaf et al., 2014 [48] | Prospective Cohort | United States (Minnesota) | 2042 | 52.3% Men | 63.1 | OR: | |
| 47.7% Women | 1–2 drinks/day | 0.14 (0.04–0.43) | |||||
| 1.56 (0.39–5.20) | |||||||
| 4.75 (1.18–15.98) |
Table notes: OR, odds ratio; HR, hazard ratio; RR, relative risk.
The toxic effects on alcohol on muscle cells are well recognized [49, 50]. In 1989, researchers demonstrated that long term alcohol use produces toxic effects on striated muscles, including heart and skeletal muscles [51]. Investigators also found that acetaldehyde, a metabolite of alcohol metabolism, negatively affected cardiac and skeletal muscle [52]. In vitro studies conducted on cardiomyocytes found that ethanol interferes with a number of muscle cell functions. For example, Guarnieri and Lakatta [53] demonstrated that ethanol inhibits the calcium-myofilament interaction, interfering with electromechanical coupling of muscle cell contractile filaments. Das and Harris [54] found that mitochondrial adenosine triphosphate (ATP) synthase becomes defective in the presence of alcohol leading to further loss of function in rat cardiomyocytes. Other studies found that ethanol has apoptotic effects on cardiac myocytes damaging overall function of heart [55, 56].
Research has shown alcohol consumption affects all areas of cell protein metabolism, from its synthesis to degradation. Human and mouse tissue studies demonstrated alcohol is a myocardial toxin and causes ultrastructural damage. Alcohol damage can include sarcoplasmic reticulum edema, contractile element fragmentation, intercalated disc expansion, and fatty deposition [57]. Alcohol produces dose dependent depression of contractile function in rat cardiomyocytes due sarcoplasmic calcium depletion [58] and decreased myofilament calcium sensitivity [59]. Studies have found an inverse relationship between use of alcohol and protein synthesis [60, 61]. Vary and colleagues [62] showed that chronic alcohol feeding in rats produced lower heart weights due to a 25% loss of cardiac proteins and a 30% reduction in the rate of protein synthesis. Potential mechanisms of alcoholic cardiomyopathy are shown in Fig. 1. Of note, Steiner and colleagues [60] reported that only chronic heavy consumption interferes with protein synthesis while moderate use has little to no effect.
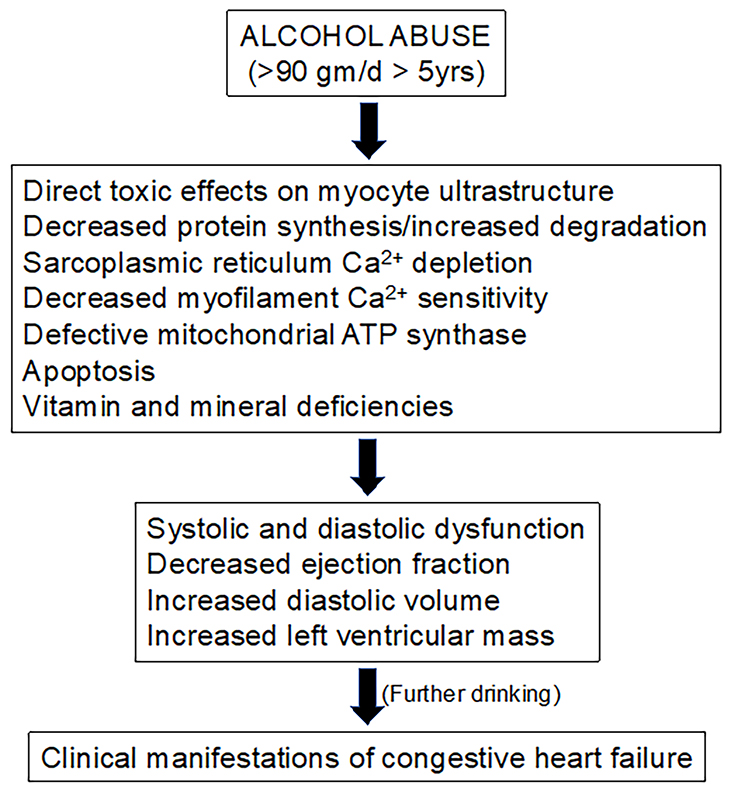 Fig. 1.
Fig. 1.Potential mechanisms of alcoholic cardiomyopathy. ATP, adenosine triphosphate.
Asymptomatic impairment of echocardiographic systolic and diastolic function parameters is found in most alcoholics [51]. Alcoholics have lower left ventricular ejection fraction, increased end diastolic volume, decreased mean fractional shortening and a larger mean left ventricular mass in a dose-dependent fashion [51]. Only a small percentage go on to develop overt manifestations of heart failure.
Symptomatic alcoholic cardiomyopathy is similar to other dilated cardiomyopathies. Diagnosis can be complicated by the presence of other risk factors. Taking a good history is important to rule out other risk factors, including prescribed and non-prescribed drugs (e.g., doxorubicin and cocaine), diabetes and coronary artery disease. Alcoholic cardiomyopathy is a diagnosis of exclusion.
Clinical findings of heart failure, including a S3 gallop, jugular venous dilation, cardiomegaly, and rales can be present. Co-existing alcoholic cirrhosis can lead to diagnostic confusion. Supraventricular arrhythmias (holiday heart syndrome) and sudden cardiac death are complications of alcohol abuse. Causes of death in alcoholic cardiomyopathy are similar to those with idiopathic cardiomyopathy, progressive chronic heart failure and sudden cardiac death [34]. Coexisting alcoholic cardiomyopathy and cirrhosis carries a worse prognosis [63].
Studies have not found an association between drinking in moderation and the development of cardiomyopathy. In fact, studies have reported a beneficial effect of moderate drinking in reducing mortality for patients with heart failure. For example, the Framingham heart study reported a lower incidence of heart failure with moderate alcohol consumption compared to patients who drank less than 1 drink per week [64, 65]. Another study reported a statistically significant reduction in the incidence of heart failure in individuals consuming moderate alcohol among older adults compared to those abstaining from alcohol [66]. In the Physicians Heart Study I, they observed a 56% decreased risk of heart failure in association with moderate consumption of alcohol [64].
The treatment of alcoholic cardiomyopathy is similar to that of other non-ischemic cardiomyopathies. Complete abstinence from alcohol is the mainstay of treatment, though even moderation may help. Four-year mortality for those who continue to abuse alcohol is near 50%. Treatment centers around heart failure guidelines from the European Society of Cardiology or the American College of Cardiology. Guideline-directed therapy begins with a combination of beta-blockers and an angiotensin-converting enzyme inhibitor, angiotensin receptor blocker, or angiotensin blocker-neprilysin inhibitor, and an aldosterone receptor antagonist [31]. Symptomatic management may require diuretic therapy. Co-existing nutritional deficiencies (vitamins, minerals such as magnesium, selenium, or zinc) should be supplemented. If concurrent atrial fibrillation is present, digitalis and anticoagulants may help.
Abstinence-maintaining medications, such as naltrexone, acamprosate, disulfiram, and nalmefen have shown some success in cardiomyopathy patients [67]. Spironolactone has recently been evaluated as a potential therapy in alcoholic cardiomyopathy patients, demonstrating not only therapeutic effects on treatment of cardiomyopathy, but an effect of reducing alcohol craving [68]. Little data is published for heart transplantation in alcoholic cardiomyopathy patients, and relapse would be a concern. Relapse rates in a study of liver transplants was 5.6 cases per 100 patients per year for any alcohol use and 2.5 cases per 100 patients per year for heavy alcohol use [69]. Likelihood of myocyte and contractile recovery depend first on amount and duration of alcohol consumption. Irreversible changes with cell death and fibrosis prevent recovery. For viable myocytes to recover, abstinence and compliance with guideline-directed medical therapy are necessary, as with any dilated cardiomyopathy.
Current guidelines and most physicians today will recommend to their patients limiting alcohol consumption to one drink per day for women, and two drinks per day for men. While epidemiological data suggests that light to moderate alcohol consumption can have advantageous cardiovascular effects, newer studies have shown that these recommendations should be tailored for each individual patient. In patients with or at higher risk for hypertension, newer studies show that even moderate drinking can lead to the progression of hypertension.
Abusing alcohol can cause a cardiomyopathy similar to other dilated cardiomyopathies. While the majority of alcoholics are clinically asymptomatic (mild systolic and diastolic dysfunction) and may never develop clinical manifestations of heart failure, a small percentage go on to develop symptomatic dilated cardiomyopathy. Because there are so many heavy drinkers, alcoholic cardiomyopathy may be the most common nonischemic dilated cardiomyopathy.
Not applicable.
AP and VF reviewed the literature and prepared the manuscript. AP and VF contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
Not applicable.
This research received no external funding.
The author declares no conflict of interest. Vincent Figueredo is serving as one of the Editorial Board members and Guest editors of this journal. We declare that Vincent Figueredo had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Carl J. Lavie and Guido Grassi.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.