



 , Esther Pueyo 4,5,†, Thijs M.H. Eijsvogels 6
, Esther Pueyo 4,5,†, Thijs M.H. Eijsvogels 61 Growth, Exercise, NUtrition and Development (GENUD) Research Group, University of Zaragoza, 50009 Zaragoza, Spain
2 Department of Physiatry and Nursing, Faculty of Health and Sport Science (FCSD), University of Zaragoza, 22002 Huesca, Spain
3 Instituto Agroalimentario de Aragón (IA2), Centro de Investigación y Tecnología Agroalimentaria de Aragón (CITA), Universidad de Zaragoza, 50013 Zaragoza, Spain
4 Biomedical Signal Interpretation and Computational Simulation (BSICoS), Aragón Institute for Engineering Research (I3A), IIS Aragón, University of Zaragoza, 50018 Zaragoza, Spain
5 CIBER de Bioingeniería, Biomateriales y Nanomedicina, CIBER-BBN, 28029 Madrid, Spain
6 Radboud Institute for Health Sciences, Department of Physiology, Radboud University Medical Center, 6500 HB Nijmegen, The Netherlands
†These authors contributed equally.
Academic Editor: Alessandro Zorzi
Abstract
Background: The health benefits of sports and exercise training are well known. However, an acute bout of exercise transiently increases the risk of sudden cardiac death (SCD). To minimize the cardiovascular risks of exercise, more insight into the prevention and causes of SCD is needed. Methods: The observatory for the prevention of sudden death in sports, PREMUBID, was created with the aim of fostering research to assess the benefits and risks of exercise at different volumes and intensities and to get insight into the underlying mechanisms of potentially cardiac (mal) adaptations. Results: The observatory gathers researchers from a wide range of disciplines working at institutions in Europe and North America. The guiding principles of PREMUBID are to broaden the understanding of SCD in sports, strengthening collaborative research across the globe, and to develop, implement and evaluate robust pre-participation screening and emergency care strategies to further reduce the number of fatal cardiac events in sport events. During the inaugural meeting of the observatory, members and affiliated researchers discussed possibilities to initiate collaborative research projects and to exchange staff and students to share information and practices to prevent SCD. The final goal is to translate the obtained knowledge to understandable messages for the general population and healthcare workers to ensure that the population at large benefits from it. Conclusions: The PREMUBID consortium aims to produce novel knowledge and insights in SCD prevention, in order to maximize the health benefits associated with acute and long-term exercise training.
Keywords
- sudden cardiac death
- sport
- research
- network
The health benefits of sports and exercise training are widely acknowledged.
Compelling evidence supports a strong and curvilinear association between regular
physical exercise and a risk reduction for all-cause mortality, cardiovascular
mortality and sudden cardiac death (SCD) [1, 2, 3]. Nevertheless, sports
participation is known to transiently increase the risk for sudden cardiac arrest
and SCD, which has an extensive social impact due to its apparent preventable
nature [4]. SCD incidence varies widely across studies, with an event rate
ranging from 0.31 to 2.1 per 100,000 person-years [5, 6, 7, 8] depending on age, sex [9]
and sport level participation [5] of the population. The majority of
exercise-related SCDs occur during recreational sports rather than in organized
competitive sports and most of these SCDs occur in adults above 35 years of age
[10]. The relative risk of SCD during and up to one hour after vigorous exertion
is higher when compared with rest or more moderate activities. For example, a
3-fold increase in risk was reported in a retrospective case-crossover study
involving both men and women (n = 206) [11], whereas a 17-fold increased risk was
found in another cohort including only men (n = 21,481) [12]. Individuals with
the lowest levels of regular physical activity (i.e.,
Atherosclerotic coronary artery disease is the most common cause of SCD in
middle aged and older athletes [5, 11, 14], whereas hereditary or congenital
heart diseases have most commonly been associated with exercise-related SCD in
young athletes (
Based on the importance of research to understand the benefits and risks of exercise at different volumes and intensities and to get insight into the underlying mechanisms, a group of sport researchers developed a roadmap for the creation of a research network under a call from the Spanish High Council for Sport. Their goal was to build an international framework able to harness the strong desire for collaboration within the sports cardiology community and to identify barriers that impede multicenter partnerships. In 2021, the observatory ‘Prevention of sudden death in sports: a global and multidisciplinary observatory for scientific research and knowledge transfer’ (PREMUBID, a Spanish acronym for Observatorio Científico en Red para el Estudio y la PREvención de la MUerte SúBIta en el Deporte) was founded (PREMUBID, Fig. 1). PREMUBID aims to serve as a model organization to link geographically distant research groups to foster research on exercise-related SCD.
 Fig. 1.
Fig. 1.PREMUBID logo.
At the inauguration, PREMUBID convened a 42-member multidisciplinary consortium consisting of sport scientists, cardiologists, sport medicine specialists, exercise physiologists, sport coaches, managers and bioengineers, with members from Spain, the Netherlands, Italy, Great Britain and the United States of America (Fig. 2). Researchers, clinicians and representatives of sport- and health-related organizations are welcome to join the consortium and can contact the authors to apply for membership through the PREMUBID website (https://www.premubid.info).
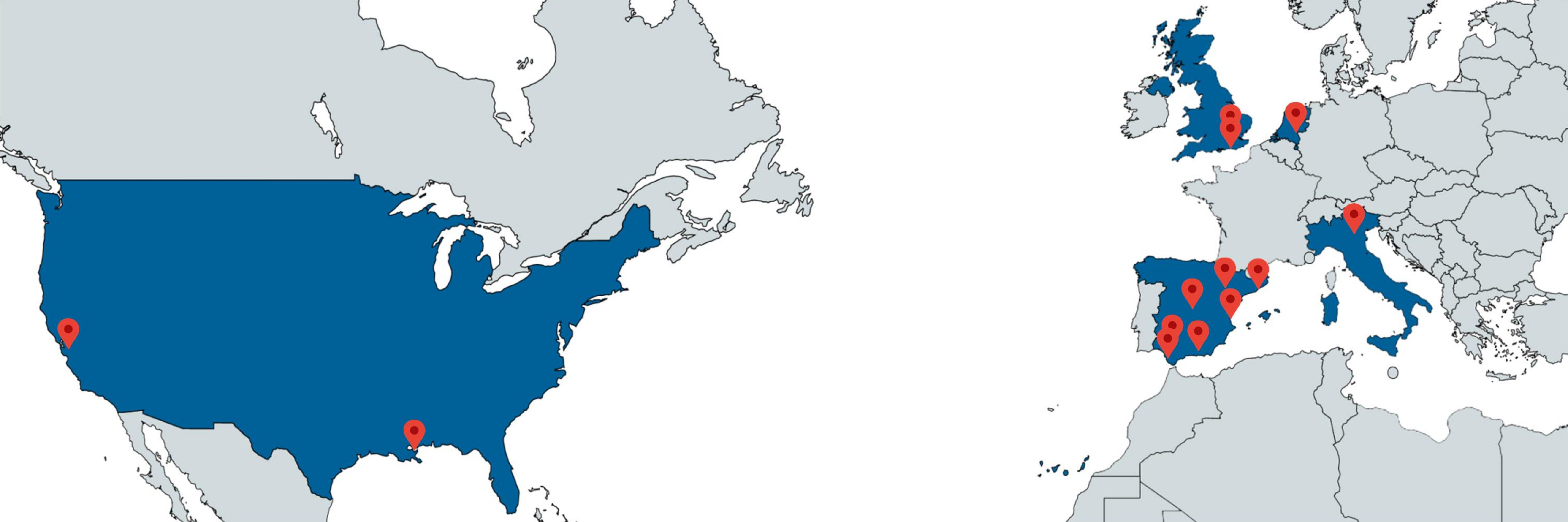 Fig. 2.
Fig. 2.PREMUBID member sites.
Each PREMUBID member is expected to attend the biannual scientific meeting and communicate about new study proposals to gauge interest and extend the possibility to other members to participate in new initiatives. PREMUBID Executive Committee includes four members: chair, vice-chair, secretary and treasurer. A research coordinator from each geographical site is appointed, and serves as the primary contact for the Executive Committee. The Executive Committee (Fig. 3) is responsible for planning and setting the agenda for the PREMUBID scientific meeting, communicating regularly with all members about new studies, funding opportunities, conducting reviews, monitoring ongoing studies and developing and disseminating guidelines for preventing SCD in sports. A core principle of PREMUBID is its open membership without restrictions by discipline, specialty or research training. All members can put forth new ideas to develop full proposals for funding or share databases. The following network goals are established as guiding principles: (1) Identify shared international research interests in SCD in sport. (2) Establish and test efficient and flexible ways of developing and implementing multicenter research projects. (3) Pool the expertise of researchers and develop cohesiveness between centers involved in PREMUBID. (4) Generate knowledge through clinical and epidemiological studies in sport-related SCD. (5) Develop and disseminate guidelines and best practices for preventing SCD in sports.
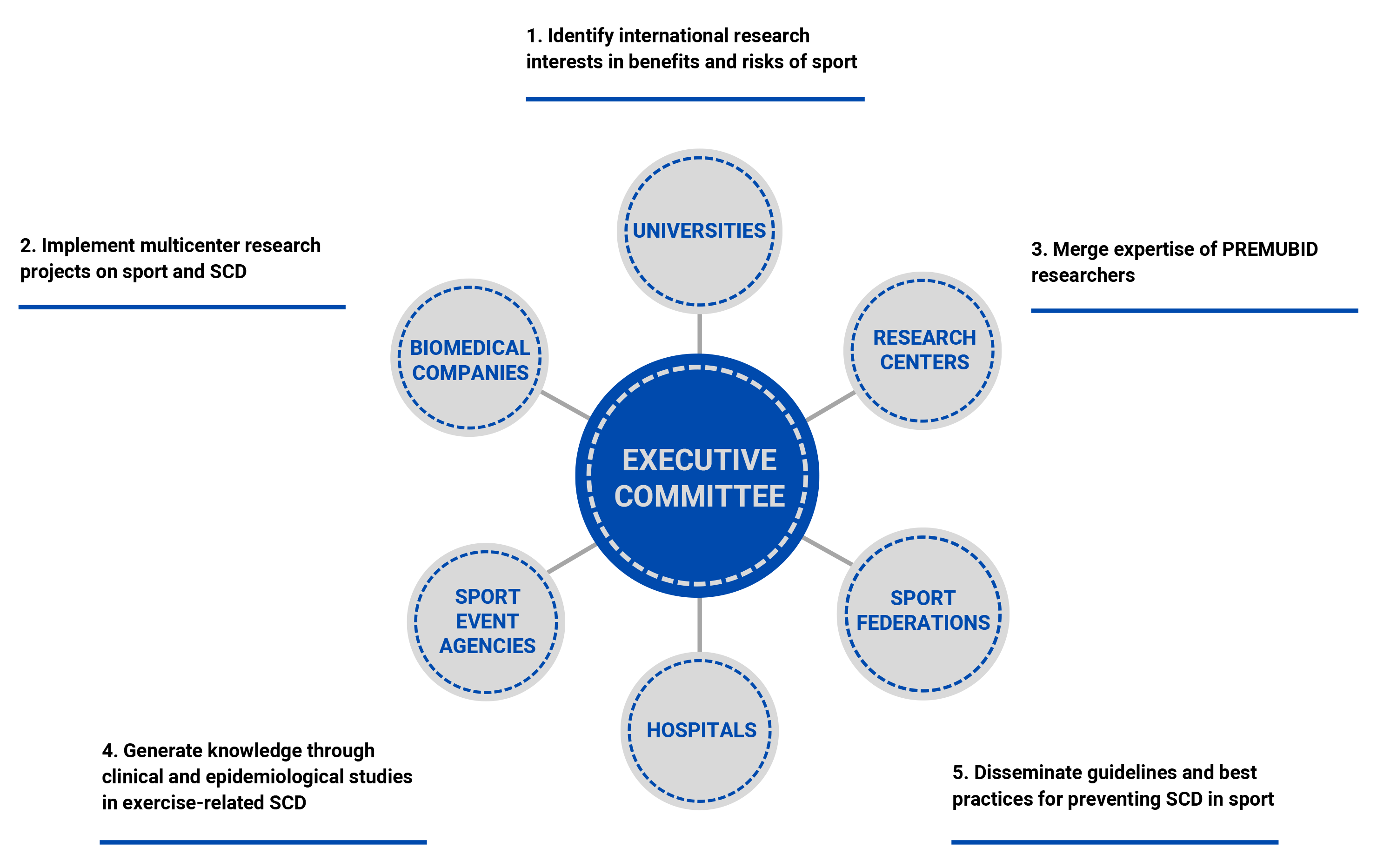 Fig. 3.
Fig. 3.Organizational chart of PREMUBID including its 5 key goals.
The single-day inaugural meeting was held at the University of Zaragoza (Huesca, Spain). The onsite and online program [24] offered sessions for researchers, clinicians, students and non-governmental organizations about vigorous exercise and SCD. In the inaugural conference, Dr. Eijsvogels [25, 26, 27] reviewed recent studies covering the acute and long-term cardiovascular consequences of extreme exercise on heart health. Next, Dr. Bailón and Dr. Pueyo [28, 29, 30, 31, 32, 33] described biomedical engineering methods for the analysis of ECG recordings from athletes and the characterization of risk markers of SCD. The conference closing was presented by Dr. Sanchis-Gomar [34, 35, 36, 37, 38], who discussed how exercise contributes to cardiovascular health, including novel findings on the impact of exercise intensity and duration on cardiac function.
During the meeting, PREMUBIBD members and other researchers shared information and exchanged knowledge about best practices to prevent and manage SCD. Attendees showed common interests in high-quality research and dissemination to achieve safe sport participation in varied environments and during competitive events throughout the world. They discussed possibilities to initiate a research project with ambitious objectives while achievable on a low-budget, voluntary basis and to exchange staff and students to stimulate learning, exchange skills and knowledge and undertake joint studies.
Strong working relationships are beginning to emerge among PREMUBID members. These relationships are expected to provide opportunities to answer relevant questions on SCD in sports through large collaborative research studies that can only be conducted in an international context involving large numbers of individuals, both male and female, young and old and amateur and elite athletes. Translating the obtained knowledge into sports practice is deemed fundamental to ensure that the whole population benefits from the high-quality research conducted by PREMUBID scientific observatory.
A core element for PREMUBID success, and a constant challenge in research, is funding. Large grants are required to conduct multicenter studies. Although the observatory has no annual funding budget yet, it is committed to promote the submission of high-quality studies to research calls. Also, PREMUBID aims to work with all involved investigators to broaden the understanding of vigorous exercise’s acute and chronic cardiovascular complications, which can lead to novel research and opportunities for funding.
Currently, PREMUBID comprises representatives from Europe and North America. PREMUBID is committed to encourage and support involvement from other geographical regions. Such global collaboration is expected to result in more large-scale and generalizable knowledge of SCD in sports.
The observatory will work closely with healthcare professionals and knowledge mobilization groups to encourage dissemination and transfer of knowledge to achieve the ultimate aim of improving the care of athletes. Updates in PREMUBID research priorities will be defined after consultation with a broad range of stakeholders, including researchers, public health practitioners and sport event managers. The distinct roles of the involved members will be clearly identified to integrate research into a translational pathway.
Our understanding of the risks of (vigorous) exercise on SCD is advancing, but further research is required to improve the knowledge of the causes underlying exercise-related SCD. Such insight is expected to serve as a basis for the development of methods to prevent the occurrence of SCD in sport. The recently founded PREMUBID observatory has 5 key priorities with the aim to broaden the understanding of SCD in sports, strengthening a more collaborative research across the globe and propose more robust pre-participation screening and emergency care strategies to reduce the number of fatal cardiac events in sport activities.
All authors were involved in the design the paper. NG and EP wrote the manuscript and TE provided help and advice on drafting, editing, supervision and reviewing. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript.
Not applicable.
Not applicable.
This research was funded by Consejo Superior de Deportes (grant number 13/UPB/21) and Ministerio de Ciencia e Innovación (research project PID2019-105674RB-I00).
The authors declare no conflict of interest.