






1 Vanke School of Public Health, Tsinghua University, 10084 Beijing, China
2 School of Medicine, Tsinghua University, 10084 Beijing, China
3 Center for Coronary Artery Disease, Division of Cardiology, Beijing Anzhen Hospital, Capital Medical University, 100029 Beijing, China
4 Department of Epidemiology, College of Preventive Medicine, Army Medical University (Third Military Medical University), 400038 Chongqing, China
†These authors contributed equally.
Academic Editor: Jerome L. Fleg
Abstract
Cardiovascular disease (CVD) is the leading cause of death worldwide. Population aging is becoming the most important driver of the CVD epidemic. With the rapid increase in an aging population, the burden of CVD will continuously increase. Most old people also suffer multimorbidity, which is strongly associated with impaired quality of life, disability, dependence, and mortality. However, few reviews evaluated the CVD burden accompanied by population aging and the challenges of CVD care in elderly individuals with multimorbidity. This review identified and summarized the current status of the CVD epidemic associated with aging and highlighted the challenges and needs of CVD care for the elderly.
Keywords
- aging
- cardiovascular disease
- epidemiology
- multimorbidity
- deprescribing
With the significant improvements in public health, sanitation, vaccination, socioeconomic development, public education, and health care, the epidemiological transition in the 20th century was accompanied by decreasing deaths and disability from communicable diseases but a continuous increase in noncommunicable diseases (NCDs) [1]. Of the types of NCDs, cardiovascular disease (CVD) is the leading cause of mortality and morbidity worldwide and will become more serious in the foreseeable future because population aging is progressing more quickly compared to the past [2]. With the aging population, the number of elderly individuals who are predisposed to developing incident CVD will continuously increase. With the improvements in health care, the number of survivors with CVD will also significantly increase. Therefore, the CVD epidemic due to rapid aging will become an urgent public health issue and bring new challenges to global health.
However, few reviews evaluated the CVD burden accompanied by aging and the challenges of CVD care in the elderly. Therefore, this review identified and summarized the current status of the CVD epidemic associated with aging and highlighted the challenges and needs of CVD care for the elderly to provide information for future research needs, policy formulation, and resource allocation.
Life expectancy has significantly increased in the past several decades worldwide. Data from the Global Burden of Disease showed that life expectancy at birth increased 8.1 years (12.4%) from 1990 to 2019 (65.4 years in 1990 to 73.5 years in 2019) [3]. Approximately 80% of countries or territories had life expectancies at birth longer than 65 years in 2019 [3]. With improvements in life expectancy at birth, the life expectancy of the elderly is improving more rapidly [4]. The global estimate is that a person 65 years old should have expected to live an additional 17 years in 2015–2020, and this number may rise to 19 years in 2045–2050 [4].
World Population Prospects estimated greater than 700 million elderly people
(age
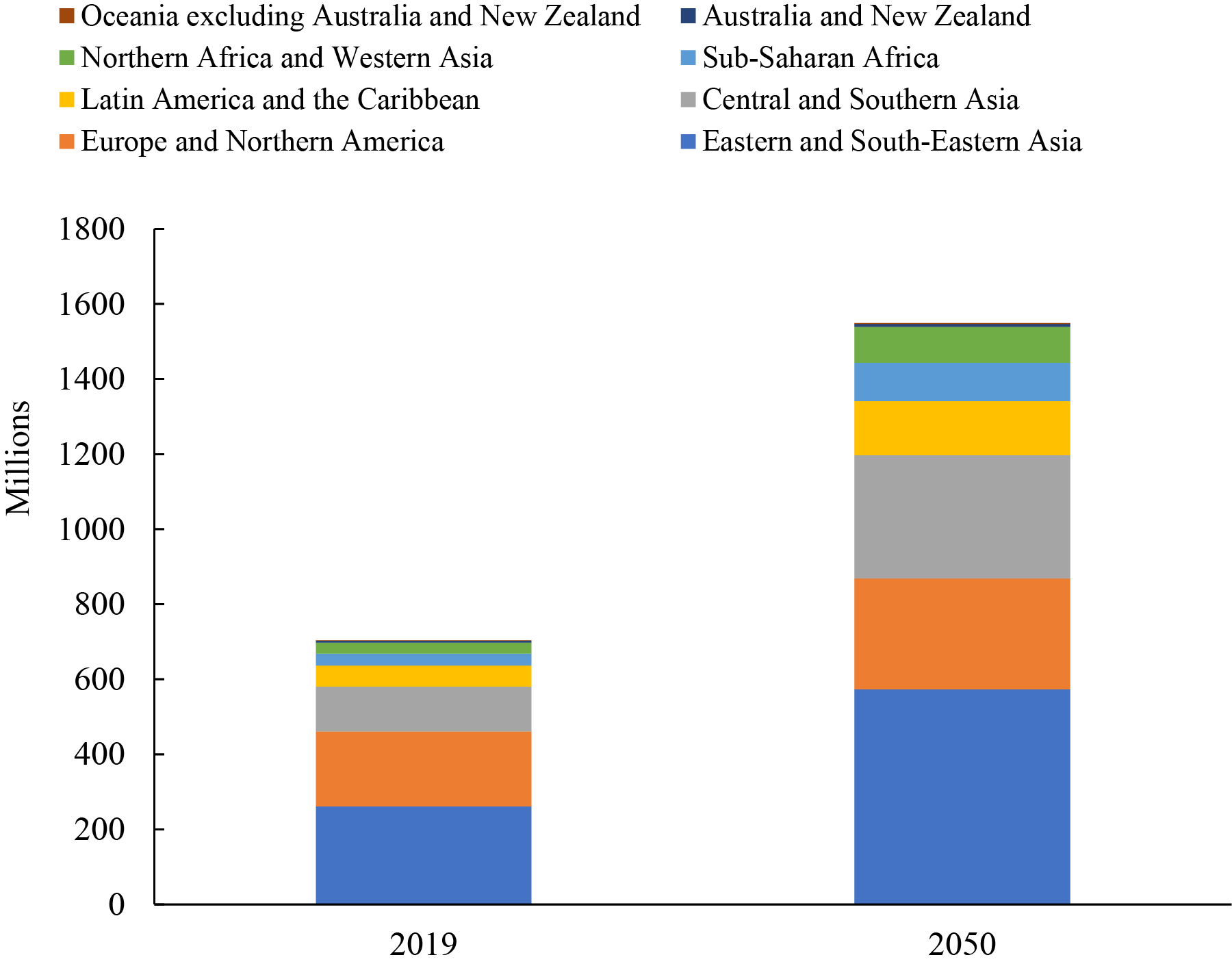 Fig. 1.
Fig. 1.Number of persons aged 65 years or over by region, 2019 and 2050 [4]. The number of people aged 65 years or over would double from 700 million in 2019 to more than 1.5 billion in 2050 worldwide, and the largest number of older people were in Eastern and Southeastern Asia, with 261 million old people in 2019 and 573 million in 2050. By 2050, there will be more elderly people in Central and Southern Asia than in Europe and Northern America. Therefore, most developing countries will face a serious problem of rapid aging in the next 30 years.
However, a healthy, disease-free lifespan, i.e., healthspan, did not increase with lifespan [5]. An average of 16–20% of life is now spent in late-life chronic diseases, which are dominated by CVD, cancer, and neurodegenerative diseases [5]. Early estimates from the United States Vital Statistics demonstrated that eliminating CVD deaths would add 5.5 years to life expectancy [6]. Therefore, reducing CVD is very important to improve the quality of life of the elderly.
The total number of CVDs nearly doubled from 271 million in 1990 to 523 million in 2019, and the number of CVD deaths steadily increased from 12.1 million in 1990 to 18.6 million in 2019, which accounted for one-third of total deaths [3, 7]. Over 80% of all CVD deaths are attributable to two conditions, ischemic heart disease (IHD) and stroke, which are very typical age-related diseases [3].
With increasing age, the proportion of CVD deaths to total deaths increased
(Fig. 2, Ref. [3]). Among people
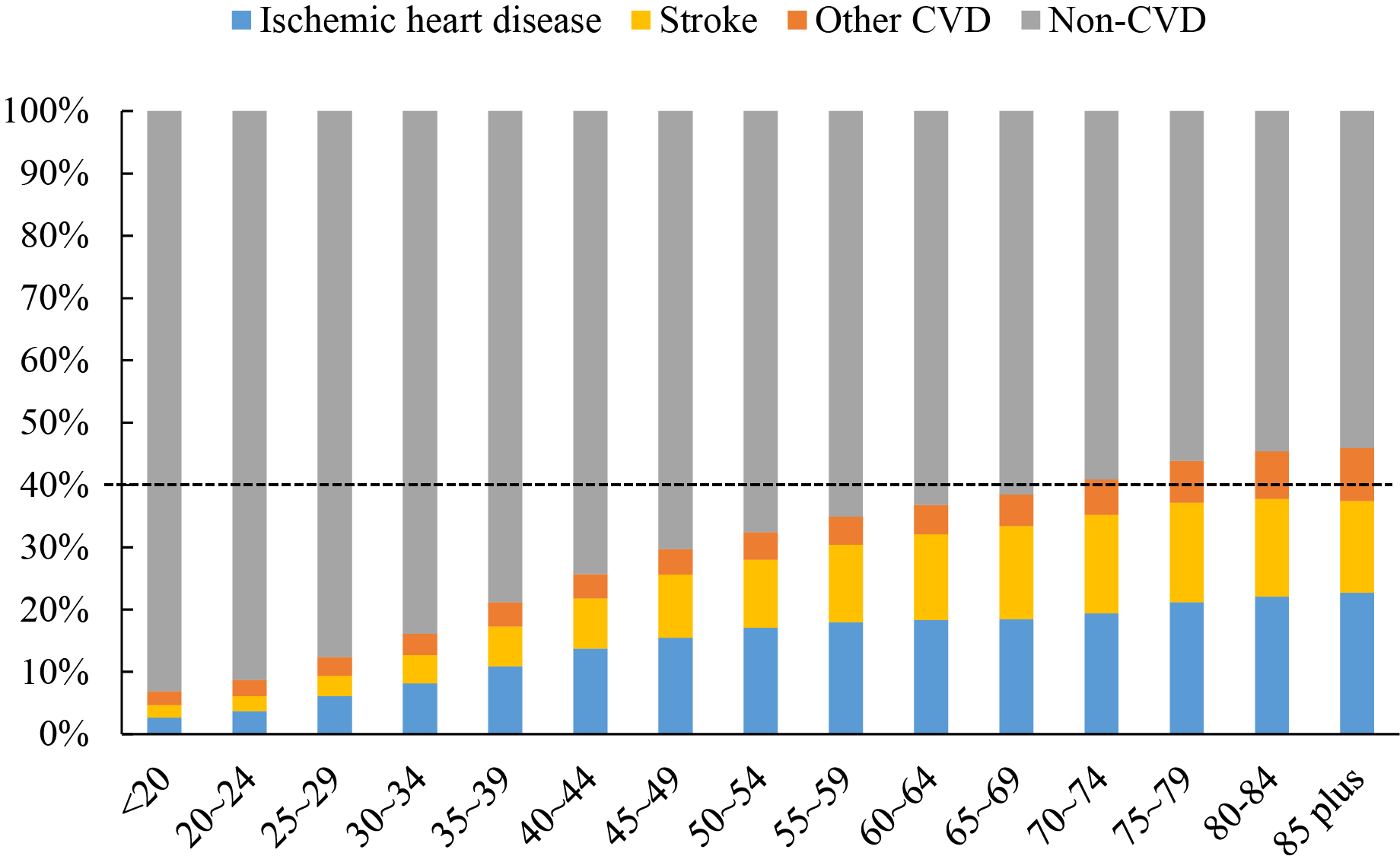 Fig. 2.
Fig. 2.Proportions of CVD in total deaths by age group [3]. With increasing age, the proportion of CVD deaths, dominated by ischemic heart disease and stroke, to total deaths increased. Among people
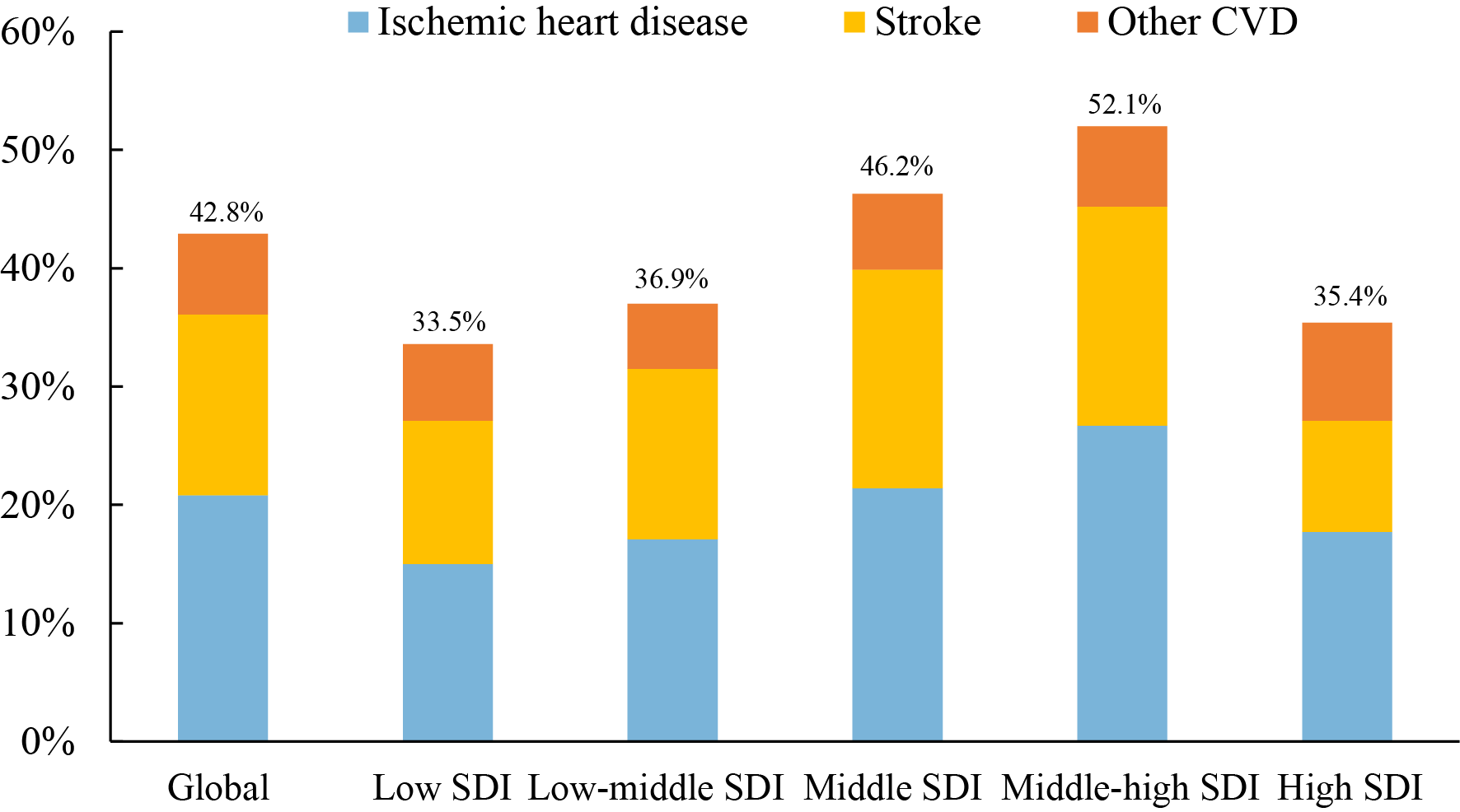 Fig. 3.
Fig. 3.Proportions of CVD in total deaths among people over 70 years by
SDI group [3]. Among people
| Stage | Characteristics of the CVD epidemic in different countries | Typical Asian countries | |||
| CVD mortality | Spectrum of diseases (Proportion in total deaths) | Proportion of premature CVD death in all CVD death | Life expectancy | ||
| Stage 1: Early stage of CVD epidemic | Low | CVD: approximately 20–30% | High, approximately 50% | Relatively short, approximately 65–70 years | India, Nepal, and Pakistan |
| CMNND: close to or greater than CVD | |||||
| Cancer: much lower than CVD, approximately 10% | |||||
| Dementia: very few | |||||
| Stage 2: Stage of rapidly increasing CVD | High; rapidly increasing | CVD: quite high, even higher than 40% | Lower, 20–50% | Long, approximately 70–75 years | Georgia, Armenica, Azerbaijan, Uzbekistan, Turkmenista,Kazakhstan, China, Lebanon, Mongolia |
| CMNND: fewer than 10% | |||||
| Cancer: lower than CVD, but higher than stage 1 | |||||
| Dementia: low | |||||
| Stage 3: Stage of decreasing CVD | Decreasing | CVD: high, but lower than stage 2, approximately 20–30% | Lowest, less than 20% | Longer, above 80 years | Japan, South Korea, Israel |
| CMNND: fewer than 10% | |||||
| Cancer: more dominant, more than 30% | |||||
| Dementia: markedly increasing | |||||
| Abbreviations: CVD, cardiovascular disease; CMNND, communicable, maternal, neonatal, and nutritional diseases. | |||||
Although CVD is the main cause of death, case fatality decreased with
improvements in medical treatment [9]. Therefore, the number of people who
survive CVD is increasing [3]. The Global Burden of Disease estimated that
there
were 200 million people
Multimorbidity is the coexistence of two or more chronic conditions, and it has
become prevalent with an aging population and the decline in mortality [10]. The
prevalence of multimorbidity is over 50% in the elderly and significantly
increases with age [11]. Among people
Due to the high prevalence of CVD, CVD combined with other conditions has become the most common type of multimorbidity for the elderly. However, the combined conditions with CVD are complex, and the complexity increases with age. For example, the management of hypertension and IHD, two concordant conditions, is relatively easy in middle-aged and young-old populations. However, the management strategy becomes more complicated and controversial in the elderly. Different guidelines proposed different blood pressure targets due to different perspectives [16, 17, 18, 19, 20, 21, 22, 23, 24] (Table 2). The discordant conditions, which are less directly related to pathogenesis or treatment strategies [15], such as IHD and cancer, are often difficult or hopeless for specialists because current clinical guidelines and research primarily target single disease-specific care, and the evidence for co-treatment of discordant conditions is insufficient, especially for elderly individuals, who are often excluded or less represented in large-scale trials [10]. This situation should be urgently and extensively corrected because CVD rarely presents as an isolated disease in the elderly, and the number of elderly people with these comorbidities will explode.
| Committee | Publication year | Population | Threshold to start therapy (mmHg) | Blood pressure target (mmHg) |
| International Society of Hypertension [16] | 2020 | SBP |
SBP | |
| SBP | ||||
| Hypertension Canada [17] | 2020 | Low risk (no target organ damage or cardiovascular risk factors | SBP |
SBP |
| High risk of cardiovascular disease | SBP |
SBP | ||
| Diabetes mellitus | SBP |
SBP | ||
| All others | SBP |
SBP | ||
| Hypertension Branch of Chinese Geriatrics Society [18] | 2019 | SBP |
SBP | |
| SBP |
SBP | |||
| SBP |
130 | |||
| The Japanese Society of Hypertension [19] | 2019 | Adults |
Lifestyle modifications should be attempted in all individuals with blood pressure |
Office blood pressure |
| SBP | ||||
| Home blood pressure | ||||
| SBP | ||||
| Adults |
Office blood pressure | |||
| SBP | ||||
| Home blood pressure | ||||
| SBP | ||||
| NICE [20] | 2019 | OBPM |
OBPM | |
| ABPM/HBPM | ||||
| ABPM/HBPM mean |
OBPM | |||
| ABPM/HBPM | ||||
| European Society of Cardiology [21] | 2018 | OBPM |
SBP 120–129 for most and DBP | |
| ABPM | ||||
| HPBM | ||||
| 65–79 years | SBP |
SBP 130–139 and DBP | ||
| SBP |
SBP 130–139 and DBP | |||
| American College of Cardiology [22] | 2017 | Adults with no history of CVD and with an estimated 10-year ASCVD risk |
SBP |
SBP |
| Patients with clinical CVD or adults with an estimated 10-year ASCVD risk of 10% or higher | SBP |
SBP | ||
| SBP |
Ambulatory: Goal SBP | |||
| high burden of comorbidity, limited life expectancy, clinical judgment, patient preference: assess risk/benefit | ||||
| European Society of Hypertension [23] | 2016 | 60 |
SBP |
SBP |
| SBP |
SBP 140–150 | |||
| Joint National Committee 8 [24] | 2014 | All ages with DM and/or CKD | SBP |
SBP |
| SBP |
SBP | |||
| SBP |
SBP | |||
| ABPM, ambulatory blood pressure monitoring; DBP, diastolic blood pressure; HBPM, home blood pressure monitoring; OBPM, Office blood pressure monitoring; SBP, systolic blood pressure. | ||||
Hypertension, diabetes, and dyslipidemia are well-known risk factors and highly prevalent comorbid conditions of CVD [25, 26, 27], especially atherosclerotic cardiovascular disease (ASCVD), which is a combination of IHD and ischemic stroke.
Among all of the risk factors for death in the elderly, high
blood pressure ranks first regardless of region [3] (Fig. 4,
Ref. [3]). Greater than two-thirds of elderly individuals with CVD likely have
hypertension [28, 29]. However, a study in China found that only 13.0% of
patients with hypertension and CVD had controlled hypertension [30]. Uncontrolled
hypertension was associated with significantly increased risks for CVD mortality
in 60- to 69-year-olds (risk ratio [RR], 2.6; 95% confidence interval [CI],
2.4–2.9) and 70- to 79-year-olds (RR, 1.9; 95% CI, 1.8–2.0) [30]. The
Hypertension in the Very Elderly Trial (HYVET) of antihypertensive therapy for
people aged
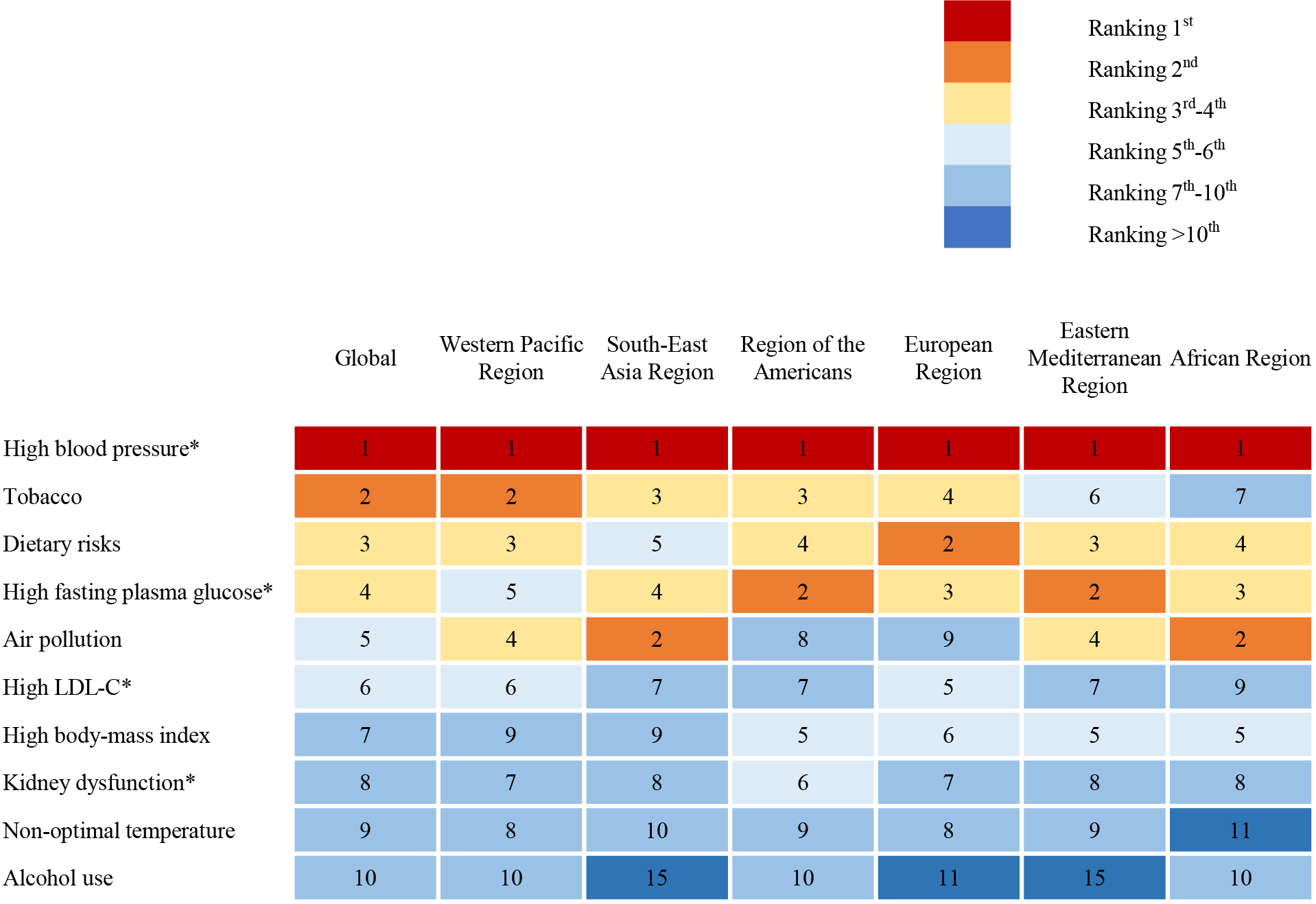 Fig. 4.
Fig. 4.Top-ranked risk factors contributing to death in people over 70 years by WHO region [3]. The chart shows the top 10 ranked risk factors for death in people over 70 years of age. The number in the chart represents the ranking of risk factors and high blood pressure ranks first regardless of region. * Highly prevalent combined conditions of cardiovascular disease. WHO, World Health Organization; LDL-C, low-density lipoprotein cholesterol.
Clinical guidelines classified patients with CVD and diabetes into extreme-risk groups [39]. At least one-third of patients with CVD have diabetes [40, 41]. With the rapid increase in the prevalence of diabetes in the general population, the proportion of diabetes in patients with CVD will likely continue to increase. A meta-analysis reported that diabetes was associated with a 1.7-fold higher risk of early mortality in patients with myocardial infarction/acute coronary syndrome (ACS), and the relative risk of early death associated with diabetes did not change over time based on the 86 studies published from 1970 to 2011 [42]. Zhou et al. [41] also found that diabetes was associated with a two-fold higher risk of in-hospital all-cause death and a 1.5-fold higher risk of major adverse cardiovascular events (odds ratio [OR], 1.54; 95% CI, 1.39–1.72) and a 2-fold risk of all-cause death (OR, 2.04; 95% CI, 1.78–2.33) in 2018. These findings suggest that advancements in the management of CVD patients during the last decades did not lead to a reduction in diabetes-induced risk. The use of SGLT-2 inhibitors or GLP-1 receptor agonists in patients with CVD and diabetes in clinical practice [43, 44, 45] are expected to reduce diabetes-induced risk.
Patients with a history of ASCVD are defined as a very-high-risk population
[46], and an LDL-C goal of
Although multiple guidelines were issued and updated for the management of hypertension, diabetes, and dyslipidemia in adults and emphasize that the treatment goals of the elderly should not be too strict [21, 22, 47, 50, 51, 52, 53, 54], treatment strategies for elderly patients with CVD are far more complicated. Clinicians should provide personalized guidance based on the elderly’s overall health status and weigh the expected timing of benefits against life expectancy [47, 55, 56] based on the currently limited research evidence and clinical experience.
The glomerular filtration rate (GFR) steadily declines with normal aging, but
this process may be influenced by superimposed diseases, such as hypertension,
diabetes and CVD [57]. A recent study reported that 57% of patients with ACS
aged
With improvements in longevity, geriatric syndromes, generally including frailty, sarcopenia, cognitive impairments, depression, urinary incontinence, vertigo, and falls, have attracted increased attention in recent years [15].
Frailty is a biological syndrome that is characterized by hypofunction of multiple physiological systems and vulnerability to stressors [64]. Five to 17% of older adults are affected by frailty [65]. Frailty and CVD are closely related [66, 67]. Frailty leads to an increased incidence of CVD, and CVD accelerates frailty [67, 68]. Because the tools and cutoff values to define frailty vary between different studies, the prevalence of frailty ranges from 10% to 60% [68]. Many studies consistently demonstrated that frailty significantly increased the risk of CVD and mortality [67, 69]. The Outcomes of Sleep Disorders in Older Men (MrOS Sleep) study estimated that frailty was associated with 84% increased CVD mortality (hazard ratio [HR], 1.84; 95% CI, 1.35–2.51), when ignoring the competing risk [70].
With increasing lifespan, the population of elderly with cognitive impairment is
also increasing. According to a meta-analysis, the median prevalence of cognitive
impairment is as high as 20% in people
Urinary incontinence is also common in the elderly [78], and it is often exacerbated by heart failure and risk factors for CVD, such as obesity, hypertension, and diabetes [79, 80, 81]. Some commonly used cardiovascular drugs also increase the risk of urinary incontinence, such as loop diuretics, angiotensin-converting enzyme inhibitors (ACEIs), and alpha-blockers [81, 82, 83, 84]. Urinary incontinence seriously affects the quality of life and increases the risk of sleep disturbance, depression, and social isolation [81, 85].
Functional decline, sensory loss, frailty, sarcopenia, and falls are also common in elderly individuals and may affect cardiovascular care to varying degrees. Regardless of hospitalization or outpatient follow-up for CVD, it is an important time window to identify geriatric syndromes. Clinicians should provide professional evaluation and prevention advice [15, 66].
In summary, it is very important to identify multimorbidity for older adults with CVD and perform research. First, it is necessary to understand the burden of CVD combined with other diseases in the elderly in different countries and regions and identify the most common disease combinations and current treatment measures. Then, multidisciplinary expert discussions and targeted clinical trials should be initiated for the elderly to provide evidence for clinical practice. Multidimensional health outcomes, such as function, health status, and quality of life, in addition to death and disability, should be considered in these studies.
Because multimorbidity is common in the elderly, the treatment of these diseases
relies heavily on medical therapy. The prevalence of polypharmacy, which is
generally defined as the use of five or more medications [86], is high in the
elderly. The “wave 6” of the Survey of Health, Aging, and Retirement in Europe
(SHARE) database showed that the overall prevalence of polypharmacy was as high
as 32.1% (95% CI, 31.5%–32.7%) in older community-dwelling older adults
across 17 European countries plus Israel [87]. Polypharmacy was more prevalent in
hospitalized patients with CVD. Using the treatment of ACS as an example, at
least 5 core medications should be provided according to guideline
recommendations, including antiplatelet drugs (e.g., aspirin and P2Y
In addition to the DDIs of different drugs, adverse drug reactions (ADRs), which is a more inclusive term, are more common in older patients [95]. ADRs occur in up to one-third of older outpatients and two-fifths of older hospitalized patients and account for one-tenth of all emergency department visits [96]. Patients using five or more drugs have an approximately 88% risk of ADRs, including an increased risk of malnutrition, renal insufficiency, metabolic disorders, bleeding, geriatric syndromes, and further decreased quality of life [97]. Therefore, the relationship between CVD, chronic conditions/diseases and ADRs is complex and interdependent (Fig. 5).
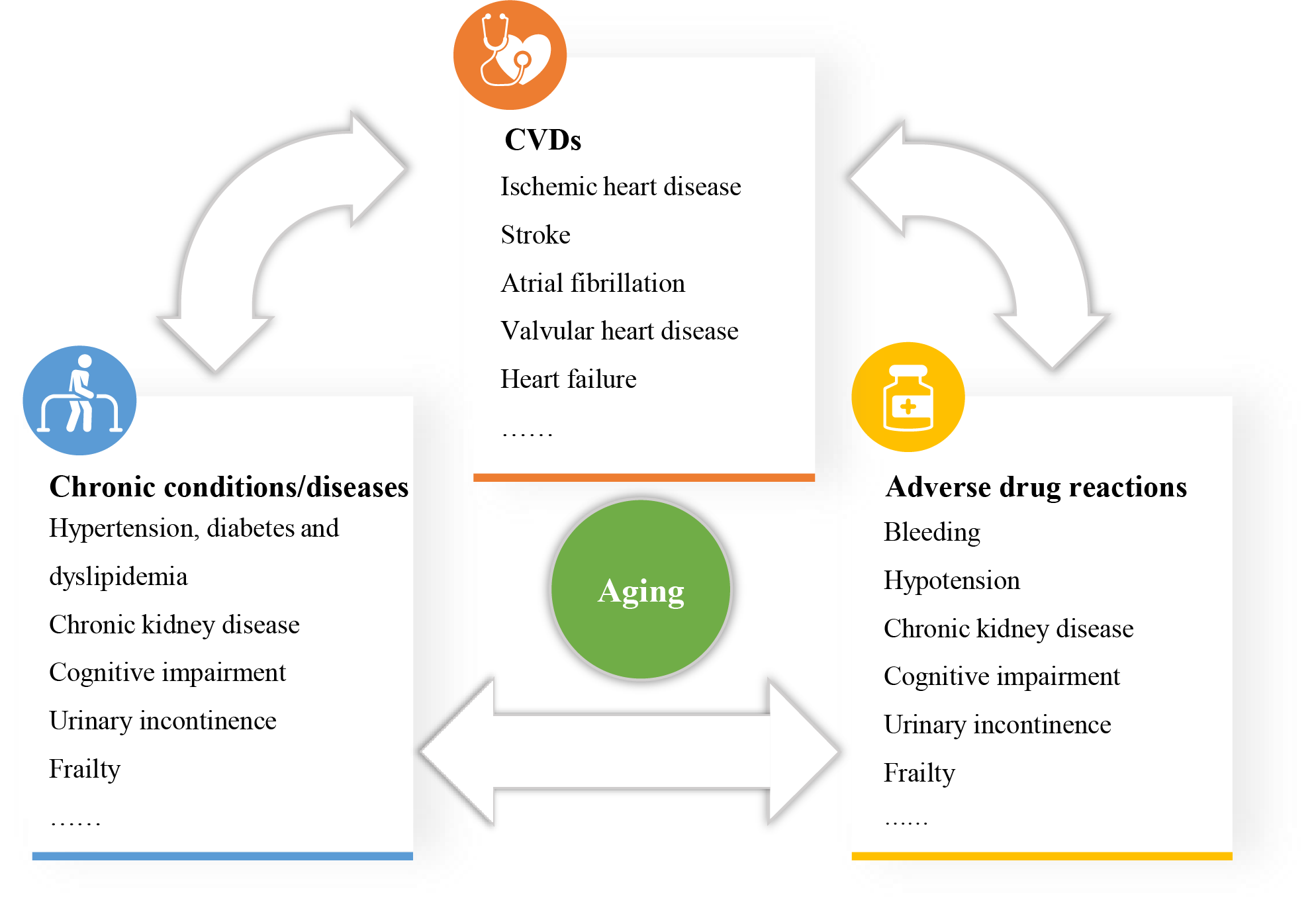 Fig. 5.
Fig. 5.The complex relationship between CVD, chronic conditions/diseases and adverse drug reactions. Chronic conditions/diseases influence the occurrence and progression of CVDs. Meanwhile, CVDs can affect the management of chronic conditions/diseases. Multimorbidity results in polypharmacy, and polypharmacy is bound to increase adverse drug reactions. Adverse drug reactions will affect the treatment of CVD and other diseases, and finally, affect the prognosis of patients. CVD, cardiovascular disease.
One study found that approximately two-fifths of the patients were taking one or more drugs that were deemed unnecessary [98]. With an evolutionary shift toward a “less-is-more” attitude for medication use, clinicians should comprehensively understand the ADRs and DDIs of polypharmacy, reduce unnecessary medications and develop an individualized medication plan for their elderly patients.
In addition to the compatibility of different types of drugs, the doses of drugs
for the elderly are also worthy of attention [99]. The current guidelines
recommend providing dual loading doses of aspirin and a P2Y
Aging always results in a series of physiological and pathological changes, which narrow the therapeutic ranges of drugs and increase the risk of side effects. Therefore, the dose of different drugs should be separately evaluated and prescribed for the elderly.
One of the most concerning problems of patients with CVD is whether they need
medications for life. Many current clinical medications for CVD do not have a
time limitation and are routinely administered over many years, such as aspirin,
statins, ACEIs/ARBs, and
Deprescribing is the process of medication withdrawal or dose reduction to improve the patient’s outcome/function, lessen the drug burden, and prevent drug-related adverse events [105]. However, barriers exist in deprescribing in the clinical practice of CVD [105]. First, the evidence for deprescribing is insufficient, although several randomized controlled trials found that deprescribing resulted in a potential reduction in mortality, falls, depression, and improvements in cognitive function and psychomotor function [105, 106, 107, 108]. Second, the attitudes of the patient’s families toward deprescribing may be negative because active and aggressive treatment has been deeply rooted in their hearts and they worry that deprescribing may raise patients’ concerns that physicians are “giving up” on them. Third, efficient communication lines between multidisciplinary teams are lacking. Clinicians from one specialty are particularly cautious and reluctant to remove medications prescribed by another specialty, which may have a risk of medical malpractice. Fourth, tools for deprescribing are not universally available for clinicians and patients [105, 109]. Several tools predominantly focused on the care of older adults [109], including the Assess, Review, Minimize, Optimize, Reassess (ARMOR) tool, the Good Palliative-Geriatric Practice (GPGP) algorithm, the American Geriatrics Society (AGS) Beers criteria, and Screening Tool of Older Persons’ Potentially Inappropriate Prescriptions (STOPP) criteria, should be referred for further tool development.
Population aging is becoming the most important driver of the CVD epidemic worldwide. With the rapid aging population, the burden of CVD will continuously increase, especially for middle- and low-SDI regions. Most elderly people also suffer from multimorbidity, which is strongly associated with impaired quality of life, disability, dependence, and mortality. The rigid application of clinical practice guidelines for single disorders may contribute to polypharmacy, adverse drug interactions, and unnecessary cost. Although many challenges in promoting deprescribing remain, we should prepare to better meet the treatment goals of the elderly. Good-quality integrated care and long-term care services for CVD and multimorbidity, should be provided for the elderly. Some countries developed national policies to support comprehensive assessments of the health and social care needs of older people, and we hope that more age-friendly cities, communities, and hospitals will be constructed.
Conceptualization,WNL, MGZ and GQZ; Methodology, MGZ; Software, MGZ and GQZ; Validation, YHZ and JMZ; Formal Analysis, MGZ; Resources, MGZ.; Data Curation, GQZ; Writing –– Original Draft Preparation, MGZ and GQZ; Writing –– Review & Editing, MGZ, GQZ, YHZ, JMZ, FC and WNL; Visualization, MGZ and YHZ; Supervision, WNL, FC and JMZ; Project Administration, WNL and FC; Funding Acquisition, WNL and GQZ.
Not applicable.
Not applicable.
This study is supported by China’s National Key R & D Program (2020YFC2004800) and the National Natural Science Foundation of China (81900454).
The authors declare no conflict of interest.