

 , Hailong Lin 4,*
, Hailong Lin 4,*1 Postgraduate College, China Medical University, 110122 Shenyang, Liaoning, China
2 Department of Cardiology, Dalian Municiple Central Hospital, 116000 Dalian, Liaoning, China
3 Department of Cadre Ward, 79th Group Army Hospital of PLA Army, 111000 Liaoyang, Liaoning, China
4 Geriatrics Center, Dalian Municiple Friendship Hospital, 116000 Dalian, Liaoning, China
†These authors contributed equally.
Academic Editor: Rubattu Speranza
Abstract
Background: The white coat effect is observed in many patients with
hypertension, but its mechanism is still unclear and anxiety is often thought to
be a key point. Methods: A total of 544 patients who met the inclusion
criteria were recruited through outpatient clinics. Three months after systematic
treatment, the office blood pressure and ambulatory blood pressure monitoring
(ABPM) were examined. Patients who reached the ABPM standard were divided into
white coat effect (n = 112) and control (n = 432) groups according to the results
of the office blood pressure. The degree of anxiety in the two groups was
evaluated using the Self-rating Anxiety Scale (SAS) and the Beck Anxiety Scale
(BAI). Differences in anxiety, gender, age, number of antihypertensive drugs,
cost per tablet and marital status were analyzed.
Results: There was no significant difference in the degree of anxiety
between the white coat and control groups, with mean SAS standard scores of 32.8
Keywords
- hypertension
- white coat effect
- Self-Rating Anxiety Scale
- Beck Anxiety Inventory
- blood pressure
The clinical diagnosis of hypertension is usually based on office blood pressure
(OBP). However, it is well-known that blood pressure (BP) in the clinic is
related not only to the basic BP of the individual, but that it may also be
influenced by neuropsychological changes during the patient’s treatment process
[1]. The condition whereby the BP measured at home or the ambulatory BP is lower
than the OBP is referred to as white coat hypertension. The difference between
OBP and out-of-office BP in white-coat hypertension is referred to as the white
coat effect. It is considered clinically significant when the OBP is
Approval for this study was obtained from the Ethics Committee of the Dalian
Municipal Central Hospital (YN2017-042-01). All patients with essential
hypertension from September 2017 to September 2020 were enrolled in the
Cardiology Outpatient department, Dalian Central Hospital, affiliated to Dalian
Medical University. Inclusion criteria were: (1) Age range from 18 to 80 years;
(2) Newly diagnosed with essential hypertension. The diagnostic criteria for
essential hypertension were in accordance with 2010 Chinese guidelines for the
management of hypertension [8]. The office BP before treatment was
All patients were given regular and systematic drug therapy for 3 months in
accordance with the requirements of the 2010 Chinese guidelines [8] the 2013
European Society of Hypertension (ESH)/European Society of Cardiology (ESC)
guidelines [10] and 2018 ESC/ESH guidelines [11] for the management of arterial
hypertension. The addition or subtraction of medications had been stopped for at
least a month. Follow-up visits were made in the outpatient department every two
weeks. The increase or decrease in drug treatment was based on the OBP, HBPM and
patient symptoms. The increase or adjustment of drugs was stopped whenever BP in
the clinic was
The method recommended by the 2010 Chinese guidelines for the management of hypertension [8] was used to measure the sitting BP of subjects in the morning. This was performed with a standard desktop mercury sphygmomanometer (30704005, Yuwell Group, Jiangsu, China) regularly calibrated by a professional doctor in a consulting room.
A Spacelabs Healthcare Automatic 24 h Ambulatory Blood Pressure Monitor (90217, Spacelabs Healthcare Ltd. Seattle, Washington, USA) was used, with standardized measurement performed according to the 2010 Chinese guidelines for the management of hypertension [8, 12]. If the invalid pseudo-error and blank data were found to exceed 30% of the total number, the data was considered invalid and measurements were made again the next day. The patient’s daily life and treatment process remained unchanged during monitoring, with the left upper limb remaining relatively stationary during each measurement.
The upper arm electronic sphygmomanometer (HEM7136, OMRON Corporation, Kyoto, Japan) was used in accordance with the 2010 Chinese guidelines for the management of hypertension [8]. Patients were asked to measure BP every morning and evening, after sitting for 5 to 10 minutes before measurement. BP was measured in the sitting position in order to keep the sphygmomanometer and heart at the same level during measurement. The measurement was performed 2 or 3 times repeatedly and the average value was taken. The BP from each measurement was recorded in detail.
Subjects were divided into two groups according to the OBP after 3 months of treatment: (1) The essential hypertension group with the white coat effect (white coat effect group). In these subjects, the difference between the systolic blood pressure (SBP) in the office and the 24 h mean SBP was 20 mmHg or more, and the difference between the diastolic blood pressure (DBP) in the office and the 24 h mean DBP was 10 mmHg or more. (2) The essential hypertension group without the white coat effect (control group). In these subjects, the difference between the SBP in the office and the 24 h mean SBP was less than 20 mmHg, and the difference between the DBP in the office and the 24 h mean DBP was less than 10 mmHg.
The data including gender, age, ethnicity, marital status, number of antihypertensive drugs used, and average daily cost of antihypertensive drugs was collected by uniformly trained professionals in accordance with uniform collection procedures through the uniform epidemiological questionnaires.
The Self-rating Anxiety Scale (SAS) and Beck Anxiety Inventory (BAI) were used to determine the level of anxiety. The survey was conducted in the form of a questionnaire by the same trained medical staff and was given in a quiet special room. The purely academic purpose of the survey was fully explained to the patients before the survey, so as to eliminate the patients’ defensive psychology. After seeking the consent of patients, the two scales were filled in by the patients themselves, and a few patients with a low educational level and/or poor vision were assessed independently according to their own and assisted answers. Before taking the questionnaire, how to fill in the scale correctly and the meaning of each item were explained to each patient, and then they were asked to fill in the questionnaire by making an independent self-assessment of their actual feelings of the last week. Furthermore, all patients had been informed of their OBP and ambulatory BP results before the investigation.
The SAS [13, 14] contains 20 items that measure the frequency of anxiety
symptoms. The score was divided into four levels: 1 (no or little time), 2 (a
small part of the time), 3 (a considerable amount of time), and 4 (most or all of
time), and corresponding to 1, 2, 3, or 4 points, respectively. The score of
items 5, 9, 13, 17, and 19 were in reverse, and the other items were scored in
sequence, as shown in Appendix Table 5. The accumulated score of each item was
the raw score. After the following formula conversion, Y = int (1.25x), in which
the raw score was multiplied by 1.25 and the integral part was taken, the
standard score was calculated. The anxiety severity was defined as follows: a
score of 25–49 represented no anxiety; a score of 50–59 represented mild
anxiety; a score of 60–69 represented moderate anxiety; and a score of 70–100
represented severe anxiety. The national normal mean of raw scores was 29.78
The BAI [14] includes 21 different anxiety symptoms and mainly evaluates the extent to which subjects are bothered by different anxiety symptoms. The subject filling in the questionnaire was required to select the extent to which each symptom bothered them, which was divided into 1 point, representing no influence, 2 points, representing mild influence, 3 points, representing moderate influence, and 4 points, representing serious influence (Appendix Table 6). The scores of all items were accumulated to obtain raw scores, which were then converted into standard scores using the formula: Y = int (1.19x) and taking the integral part. The standard score of 45 was the threshold of judgment, and the higher the score, the more anxious the individual.
Both scales were used, and anxiety was confirmed when the scores were higher than their standard scores.
SPSS Statistics (version 24.0, SPSS Statistics, International Business Machines
Corporation, Armonk, NY, USA) was used for statistical analysis. The measurement
data were presented as the mean
As shown in Fig. 1, 432 patients (79.4%) in the control group and 112 patients (20.6%) in the white coat effect group were enrolled. All of them completed the questionnaire survey, with the recovery rate of 100%.
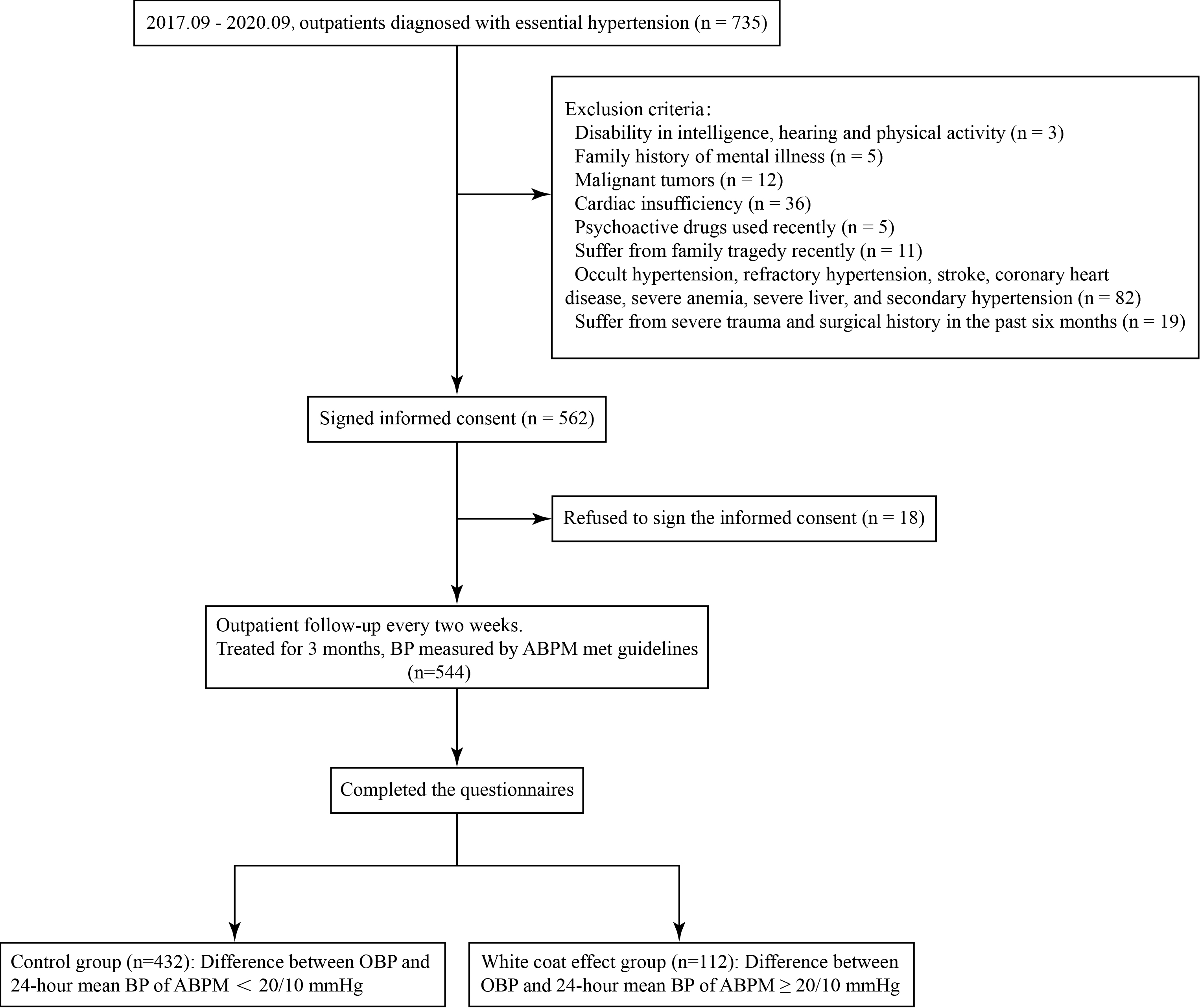 Fig. 1.
Fig. 1.Flowchart of the study. BP, blood pressure; ABPM, ambulatory blood pressure monitoring; OBP, office blood pressure.
There was no significant difference in office SBP (169.1
The highest raw score of SAS in the control group was 58, and the lowest score
was 20, with an average of 25.7
| Groups | SAS Score | BAI Score | ||||||
| Raw | p | Standard | p | Raw | p | Standard | p | |
| Control group (n = 432) | 25.7 |
0.137 | 31.8 |
0.170 | 26.7 |
0.126 | 31.2 |
0.119 |
| White coat effect group (n = 112) | 26.2 |
32.8 |
26.9 |
31.4 | ||||
| SAS, Self-Rating Anxiety Scale; BAI, Beck Anxiety Inventory. | ||||||||
The highest raw score of BAI in the control group was 58, and the lowest score
was 21, with an average of 26.7
The respondents were all Han Chinese, and the medication use was summarized in
the Appendix Table 8. The proportion of females, age, daily cost of
antihypertensive drugs, and number of antihypertensive drugs in the white coat
effect group were significantly higher than those in the control group (p
| Items | Control group | White coat effect group | p | |
| (n = 432) | (n = 112) | |||
| Gender | ||||
| Male (n, %) | 243 (56.3) | 24 (21.4) | ||
| Female (n, %) | 189 (43.7) | 88 (78.6) | ||
| Age (years) | 56.6 |
67.4 |
||
| Number of antihypertensive drugs (n, %) | ||||
| 1 | 21 (4.9) | 0 | ||
| 2 | 104 (24.1) | 0 | ||
| 3 | 214 (49.5) | 42 (37.5) | ||
| 4 | 93 (21.5) | 70 (62.5) | ||
| Daily cost of antihypertensive drug (yuan) | 4.6 |
7.7 |
||
| Cost per tablet (yuan) | 1.6 |
2.2 |
||
| Marital status (n, %) | ||||
| Unmarried | 0 | 1 (0.9) | 0.058 | |
| Married | 417 (96.5) | 104 (92.8) | ||
| Widowed | 15 (3.5) | 7 (6.3) | ||
With the white coat effect as the dependent variable, and anxiety, gender, age, daily cost of antihypertensive drugs, number of antihypertensive drugs, and marital status as independent variables, logistic regression analysis was performed (Table 3). The results showed that gender, age, number of antihypertensive drugs and cost per tablet were factors related to the white coat effect (Table 4).
| Risk Factors | Variables | Assignment |
| Anxiety | X |
“0” for non-anxiety, “1” for anxiety |
| Gender | X |
“0” for female, “1” for male |
| Age | X |
Specific values |
| Number of antihypertensive drugs | X |
Specific values |
| Cost per tablet | X |
Specific values |
| Marital status | X |
“0” for unmarried, “1” for married, “2” for widowed |
| White coat effect | Y | “0” for non-white coat effect, “1” for white coat effect |
| Risk Factors | B | SE | Wald | p | OR | 95% CI |
| Anxiety | 0.313 | 0.554 | 0.318 | 0.573 | 1.367 | 0.461–4.049 |
| Gender | –1.230 | 0.347 | 12.579 | 0.292 | 0.148–0.577 | |
| Age | 0.216 | 0.027 | 66.136 | 1.241 | 1.178–1.307 | |
| Number of antihypertensive drugs | 1.957 | 0.282 | 47.974 | 7.075 | 4.067–12.307 | |
| Cost per tablet | 1.340 | 0.228 | 34.601 | 3.820 | 2.444–5.971 | |
| Marital status | –1.139 | 0.656 | 3.015 | 0.082 | 0.320 | 0.089–1.158 |
| B, regression coefficient; SE, standard error; OR, odds ratio; CI, confidence interval. | ||||||
In the present study, we found that there was no significant difference in anxiety status between the white coat effect group and the control group. However, gender, age, number of antihypertensive drugs used and coat per tablet were the influence factors of white coat effect in hypertensive patients during treatment.
The concept of the white coat effect was described precisely by Mancia et al. in 1983 [15]. When a patient was undergoing traumatic intra-arterial ambulatory BP monitoring in the consulting room, a doctor in a white coat entered the room, then the patient’s BP suddenly rose rapidly and was at its highest point within 4 minutes, with an average increase of 27/14 mmHg. The BP gradually dropped within 10 minutes. The term white coat hypertension was originally limited to untreated individuals but has been extended to patients under antihypertensive treatment in whom only OBP has not been treated to target, with the term white coat uncontrolled hypertension (WUCH), compared with sustained uncontrolled hypertension (SUCH) [11]. The white coat effect is used to describe the difference between an elevated OBP and a lower home or ambulatory BP in both untreated and treated patients.
The specific mechanism of the white coat effect is not clear, and it is speculated to be related to a stress response. According to Kai et al. [16] and Pioli et al. [17], when patients received pressure measurements by medical staff in the consulting room, the scenario was likely to cause a stress and alert response in patients, resulting in excessive tension and activation of the sympathetic catecholamine system, leading to an increase in BP in the clinic. Perhaps the words of the medical staff might also affect the measured BP [18]. Smith et al. [19] and Caini et al. [20] did find that activity of the sympathetic nervous system and renin-angiotensin system were increased in patients with the white coat effect. There are obvious individual differences in stress responses, which are related to individual neurologic characteristics. Anxiety is a common neurological personality trait. Previous studies [21, 22, 23] have shown that anxiety patients are prone to hypertension.
Peiliang et al. [24] and Cobos et al. [25] have found that anxiety might be related to the white coat effect, but this study did not support this possibility. This study did not find that hypertensive patients with the white coat effect were more anxious than hypertensive patients without the white coat effect. Moreover, it was also found that the anxiety score of all hypertensive patients included in the study was not higher than the constant index of the normal population, which was different from previous studies [26, 27]. First, in previous studies, anxiety assessment was mostly carried out before treatment, while the anxiety assessment in this study was conducted after 3 months of antihypertensive treatment. In addition to specialized drug treatments for hypertensive patients, non-drug treatment including general psychological counseling was emphasized in the study. Although the psychological counseling was not professional, it was speculated that it might play a role. Second, the authoritative personnel in the hypertension outpatient clinic might provide a strong psychological comfort to patients. The professional capacities of medical staff provided patients confidence in the diagnosis and treatment of hypertension during the follow-up visit. This study showed that anxiety was not necessary for the white coat effect. Hypertensive patients without anxiety could also have a transient, hidden mood fluctuation after entering the clinic, which triggers a neuroendocrine reaction and temporarily increases BP, which is the white coat effect.
Furthermore, this study also analyzed the relationship between gender, age, number of antihypertensive drugs, cost per tablet, and marital status, and the white coat effect of treated hypertensive patients. This study found that BP before treatment and marital status had nothing to do with the white coat effect, but females and elderly patients were more likely to have the white coat effect, which was consistent with other research reports [28, 29]. Moreover, this study also found that both the number of antihypertensive drugs and the cost per tablet were related to the white coat effect, namely, the more antihypertensive drugs used, the higher cost per tablet spent, the greater the possibility that the white coat effect occurred. The mechanism of the white coat effect in women is not clear; it may be related to female hormones. Oyola et al. [30] found that women were more prone to exaggerated response to stress, due to the enhanced activity of hypothalamo-pituitary-adrenal (HPA) axis resulting from the increased level of estradiol under stress. However, this proposition has been disputable, and needs to be further studied [31]. It has long been reported [32, 33] that untreated elderly patients were prone to the white coat effect, and this study showed that the white coat effect in hypertensive patients with effective antihypertensive treatment was also related to age. The reasons why the white coat effect was likely to occur in the elderly might be as follows. On the one hand, the mental sensitivity of elderly patients to diseases was generally enhanced [34], which easily triggers neuroendocrine reactions. On the other hand, the elasticity of the aorta in elderly patients is decreased, which reduced the buffering ability to the increasing pressure because of the change in cardiac stroke volume. When psychological stress led to an increase in cardiac stroke volume, the increase in SBP was more pronounced. The relationship between the number of antihypertensive drugs and the cost per tablet and the white coat effect might be related to the following aspects: First, the increase or decrease of drugs based on OBP might lead to overuse of antihypertensive drugs in hypertensive patients with the white coat effect. The home BP was referred to when adding or reducing drugs, and the 24 h ambulatory BP level of the white coat effect group was not lower than that of the control group, but this possibility cannot be completely ruled out. Second, it meant that BP was difficult to control, and the condition was serious when the number of antihypertensive drugs used was large and the cost per tablet was high, which could cause greater psychological impact on the pressure measurement of patients in the office. Third, patients who used multiple antihypertensive drugs with a high cost and with difficulty in controlling BP might have a stronger rapid pressor reflex mechanism, so that the white coat effect was more obvious.
This study was a single-center study, which has its inherent limitations. The small sample size may have led to sampling deviations. Because of geographical limitations, the patients in this study were Han Chinese, and the white coat effect of other ethnicities was not analyzed. The white coat effect of patients before antihypertensive treatment was not analyzed, which may cause aberrations in the analysis of the results after treatment. In short, more comprehensive research is needed in the future.
Anxiety may not be the cause of the white coat effect in patients with hypertension during treatment. Female, old age, number of antihypertensive drugs used, and cost per tablet were related to the white coat effect in hypertension patients during treatment. Clinically, attention should be paid to the identification of the white coat effect in the diagnosis and treatment of hypertension, and the treatment plan should be adjusted according to the situation.
HL and YG designed the research study and checked the manuscript. DX, HQ and ZL performed the research and analyzed the data. PY and HX interpreted data and revised the manuscript. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript.
The study protocol was approved by the ethics committee of Danlian Municiple Central Hospital (Approval Number: YN2017-042-01).
Not applicable.
This work was supported by grants from the National Natural Science Foundation of China (81970310, 82070239, 82170328), Natural Science Foundation of Liaoning Province (2020-MS-036), and Young Talent Fund of Military Science and Technology Project (18-JCJQ-QT-018).
The authors declare no conflict of interest.
| Items | No or very little time | A small part of time | A considerable amount of time | Most or all of the time |
| 1. I feel more nervous or anxious than usual. | 1 | 2 | 3 | 4 |
| 2. I’m afraid for no reason. | 1 | 2 | 3 | 4 |
| 3. I easily get upset or frightened. | 1 | 2 | 3 | 4 |
| 4. I think I might go crazy. | 1 | 2 | 3 | 4 |
| *5. I think everything is fine. | 4 | 3 | 2 | 1 |
| 6. My hands and feet trembled. | 1 | 2 | 3 | 4 |
| 7. I suffer from headaches, neck pains and backaches. | 1 | 2 | 3 | 4 |
| 8. I feel weak and tired easily. | 1 | 2 | 3 | 4 |
| *9. I feel calm and I tend to sit still. | 4 | 3 | 2 | 1 |
| 10. I feel my heart beating fast. | 1 | 2 | 3 | 4 |
| 11. I am troubled by bouts of dizziness. | 1 | 2 | 3 | 4 |
| 12. I have seizures or feelings of fainting. | 1 | 2 | 3 | 4 |
| *13. I breathe in and out easily. | 4 | 3 | 2 | 1 |
| 14. I have numbness and tingling in my hands and feet. | 1 | 2 | 3 | 4 |
| 15. I am troubled with stomachache and indigestion. | 1 | 2 | 3 | 4 |
| 16. I often have to urinate. | 1 | 2 | 3 | 4 |
| *17. My hands and feet are often dry and warm. | 4 | 3 | 2 | 1 |
| 18. I’m flushed and hot. | 1 | 2 | 3 | 4 |
| *19. I fall asleep easily and get a good night’s sleep. | 4 | 3 | 2 | 1 |
| 20. I have nightmares. | 1 | 2 | 3 | 4 |
| *The score of items 5, 9, 13, 17 and 19 are in reverse. | ||||
| Items | None | Mild | Moderate | Severe |
| Not much disturbance | Feel uncomfortable but tolerable | Can barely endure | ||
| 1. Numbness or tingling | 1 | 2 | 3 | 4 |
| 2. Feel hot | 1 | 2 | 3 | 4 |
| 3. The legs tremble | 1 | 2 | 3 | 4 |
| 4. Can’t relax | 1 | 2 | 3 | 4 |
| 5. Fear of something bad happening | 1 | 2 | 3 | 4 |
| 6. Dizziniess | 1 | 2 | 3 | 4 |
| 7. Palpitations or increased heart rate | 1 | 2 | 3 | 4 |
| 8. Distracted | 1 | 2 | 3 | 4 |
| 9. Frightened | 1 | 2 | 3 | 4 |
| 10. Nervous | 1 | 2 | 3 | 4 |
| 11. Choked | 1 | 2 | 3 | 4 |
| 12. The hands tremble | 1 | 2 | 3 | 4 |
| 13. Shake | 1 | 2 | 3 | 4 |
| 14. Afraid of out of control | 1 | 2 | 3 | 4 |
| 15. Dyspnea | 1 | 2 | 3 | 4 |
| 16. Fear of dying | 1 | 2 | 3 | 4 |
| 17. Panic | 1 | 2 | 3 | 4 |
| 18. Indigestion or abdominal discomfort | 1 | 2 | 3 | 4 |
| 19. Fainting | 1 | 2 | 3 | 4 |
| 20. Face redness | 1 | 2 | 3 | 4 |
| 21. Sweating (not due to heat) | 1 | 2 | 3 | 4 |
| BP | Control group | White coat effect group | p | |
| (n = 432) | (n = 112) | |||
| OBP before treatment | ||||
| SBP | 168.6 |
169.1 |
0.433 | |
| DBP | 111.0 |
111.3 |
0.574 | |
| OBP after treatment | ||||
| SBP | 131.2 |
160.9 |
||
| DBP | 81.7 |
96.2 |
||
| 24 h mean BP after treatment | ||||
| SBP | 116.0 |
118.0 |
||
| DBP | 74.5 |
75.1 |
0.231 | |
| Daytime mean BP after treatment | ||||
| SBP | 120.7 |
122.5 |
||
| DBP | 78.1 |
77.2 |
0.031 | |
| The difference between OBP and 24 h mean BP after treatment | ||||
| SBP | 15.2 |
42.9 |
||
| DBP | 7.3 |
21.1 |
||
| The difference between OBP and daytime mean BP after treatment | ||||
| SBP | 10.5 |
38.4 |
||
| DBP | 3.6 |
19.0 |
||
| 24 h mean BP and daytime mean BP after treatment of the white coat effect group,
compared with the office BP after treatment of the same group, | ||||
| Medication | Control group | White coat effect group | p |
| (n = 432) | (n = 112) | ||
| Nifedipine (Bayer, 30 mg) | 30 (6.9%) | 35 (31.3%) | |
| Amlodipine (Pfizer, 5 mg) | 21 (4.9%) | 28 (25.0%) | |
| Amlodipine (Landi, 5 mg) | 177 (41.0%) | 21 (18.8%) | |
| Lacidipine (Sanchine, 4 mg) | 126 (29.2%) | 27 (24.1%) | 0.289 |
| Benazepril (Novartis, 10 mg) | 80 (18.5%) | 13 (11.6%) | 0.083 |
| Perindopril (Acertil, 4 mg) | 45 (10.4%) | 13 (11.6%) | 0.716 |
| Irbesartan (Coaprovel, 150 mg) | 64 (14.8%) | 18 (16.1%) | 0.740 |
| Telmisartan (Boehringer Ingelheim, 80 mg) | 8 (1.9%) | 25 (22.3%) | |
| Telmisartan (CCPC, 80 mg) | 87 (20.1%) | 9 (8.0%) | 0.003 |
| Bisoprolol (Merck, 5 mg) | 71 (16.4%) | 20 (17.9%) | 0.719 |
| Metoprolol (AstraZeneca, 25 mg) | 239 (55.3%) | 66 (58.9%) | 0.493 |
| Hydrochlorothiazide (Yunpeng, 25 mg) | 94 (21.8%) | 64 (57.1%) | |
| Irbesartan Hydrochlorothiazide* (Coaprovel, 150 mg/12.5 mg) | 69 (16.0%) | 15 (13.4%) | 0.501 |
| Telmisartan Hydrochlorothiazide* (CCPC, 40 mg/12.5 mg) | 31 (7.2%) | 19 (17.0%) | 0.001 |
| *When calculating the number of drugs, one compound preparation was counted as two drugs. CCPC, Suzhou Chung-Hwa Chemical & Pharmaceutical industrial CO., LTD. | |||
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.