


 , Maria Sara Mauro 1, Davide Capodanno 1, Dominick J. Angiolillo 2,*
, Maria Sara Mauro 1, Davide Capodanno 1, Dominick J. Angiolillo 2,*
1 Division of Cardiology, Azienda Ospedaliero-Universitaria Policlinico “G. Rodolico – San Marco”, 95125 Catania, Italy
2 Division of Cardiology, University of Florida College of Medicine, Jacksonville, FL 32209, USA
Academic Editor: Boyoung Joung
Abstract
Following percutaneous coronary intervention (PCI), an initial course of dual
antiplatelet therapy (DAPT) with aspirin and a P2Y
Keywords
- acute coronary syndrome
- antiplatelet therapy
- antithrombotic therapy
- chronic coronary syndrome
- percutaneous coronary intervention
- P2Y12 receptor
- pharmacotherapy
- secondary prevention
Initial observations of platelets in the human blood date back to the 19th
century, when Max Schultze and Giulio Bizzozero [1, 2] afterward identified and
described the role of what appeared as unknown blood spherules, both in
vitro and in vivo. Platelets were then found to play a central role in
thrombosis and hemostasis, adhering to one another and to some threads later
recognized as strands of fibrin [3]. Platelets became a therapeutical target in
the 1960s, when the effects of aspirin on bleeding time were correlated to
impairment in platelet response [4]. Approximately 30 years later it became clear
that platelets can be also activated by different stimuli, including the
P2Y
P2Y
Following PCI, irrespective of whether in the context of a patients presenting
with a chronic coronary syndrome (CCS) or acute coronary syndrome (ACS), an
initial course of dual antiplatelet therapy (DAPT) with aspirin and a
P2Y
This article reviews the current evidence on P2Y
Aspirin and P2Y
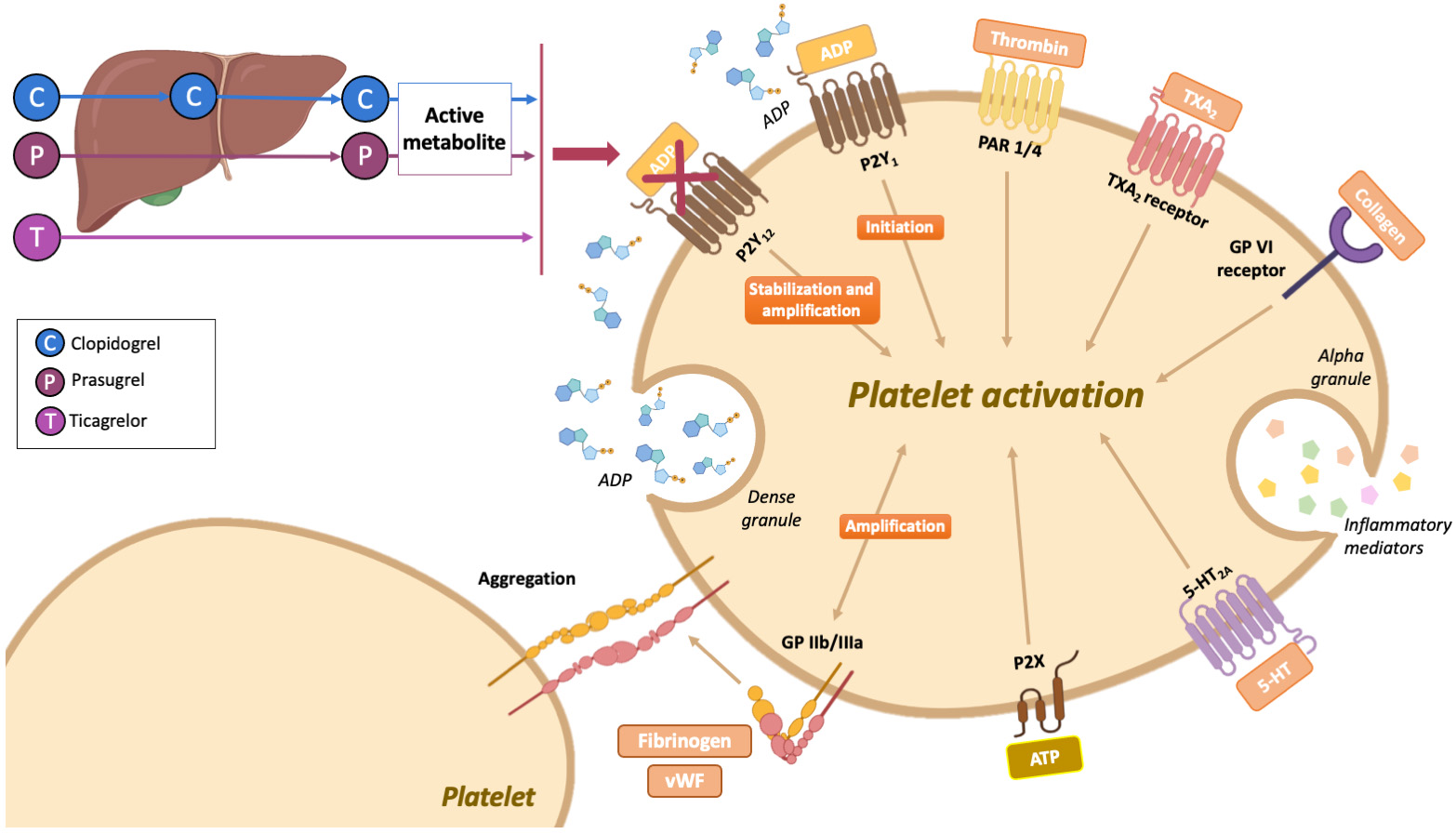 Fig. 1.
Fig. 1.Mechanism of action of oral P2Y
Three nucleotide receptors (jointly known as P2 receptors), namely P2X
| Ticlopidine | Clopidogrel | Prasugrel | Ticagrelor | Cangrelor | Vicagrel | Selatogrel | |
| Class | Thienopyridine | Thienopyridine | Thienopyridine | Cyclopentyltriazolopyrimidine | Adenosine triphosphate analogue | Thienopyridine | 2-phenyl-pyrimidine-4-carboxamide analogue |
| Binding | Irreversible | Irreversible | Irreversible | Reversible | Reversible | Irreversible | Reversible |
| Type of binding | Noncompetitive | Competitive | Competitive | Noncompetitive | Competitive | Competitive | Competitive |
| Metabolic conversion | Yes | Yes | Yes | No | No | Yes | No |
| Route of administration | Oral | Oral | Oral | Oral | Intravenous | Oral | Subcutaneous |
| Dose | 250 mg twice daily MD | 600 mg LD, 75 mg daily MD | 60 mg LD, 10 mg daily MD | 180 mg LD, 90 mg twice daily MD | 30 µg/kg bolus, 4 µg/kg/min infusion (two to four hours) | 20 mg LD, 5 mg daily MD | 16 mg |
| Onset of action | Two hours | Two to six hours | 0.5 to four hours | 0.5 to two hours | Two minutes | Four hours | 15 to 30 minutes |
| Offset of action | Seven to 10 days | Seven to 10 days | Seven to 10 days | Three to five days | One to 1.5 hours | Five to 10 days | Eight hours |
| Half-life | Eight to 13 hours depending on age | AM 30 minutes | AM seven hours | AM nine to 12 hours | Three to five minutes | AM 45 minutes | Four to 7 hours |
| Approved for clinical use | Yes | Yes | Yes | Yes | Yes | No | No |
| Abbreviations: AM, active metabolite; LD, loading dose; MD, maintenance dose. | |||||||
Conversely, the fundamental mechanism responsible for the antithrombotic effects
of aspirin is the irreversible inhibition of cyclooxygenase-1 (COX-1), which
suppresses the platelet production of TXA
Pharmacodynamic studies have suggested that aspirin discontinuation is followed
by increased platelet reactivity by the COX-1 pathway, while pathways depending
on other agonists (e.g., ADP, TXA
The TEMPLATE trial used a panel of platelet function tests after randomly
allocating 110 ACS patients undergoing PCI to receive either ticagrelor
monotherapy or DAPT with aspirin and ticagrelor for four weeks, with both
strategies followed by aspirin monotherapy for additional four weeks [28].
Platelet aggregation in response to TRAP-6 (primary outcome), TXA
In the TWILIGHT platelet sub-study (n = 51), ticagrelor monotherapy and DAPT were compared in terms of thrombus size (primary endpoint) and platelet reactivity following different stimuli. Blood thrombogenicity (i.e., thrombus size in the ex-vivo Badimon perfusion chamber) was similar between the two groups as well as platelet reactivity in response to ADP and thrombin. By contrast, platelet reactivity after arachidonic acid or collagen was higher among patients receiving ticagrelor monotherapy, highlighting the unequivocal role of aspirin in the inhibition of the COX-1 pathway [29].
The GLOBAL LEADERS platelet sub-study, excluding patients on DAPT with aspirin and clopidogrel, explored the restoration of platelet reactivity after withdrawal of aspirin at one month or ticagrelor at 12 months [30]. Cessation of either component of DAPT led to a substantial increase in platelet reactivity, with differential effects depending on the specific investigated activation pathway. After aspirin withdrawal, there was a marked recovery of platelet aggregation induced by arachidonic acid or collagen; by contrast, cessation of ticagrelor was followed by a prompt recovery of platelet aggregation in response to ADP or collagen [30].
Given that most pharmacodynamic studies conducted thus far have used assays that
are specific to appraise the effects of pathways inhibited by a given
antiplatelet agent, more studies evaluating the diverse effects of the different
antiplatelet regimens (e.g., aspirin monotherapy, P2Y
Several randomized clinical trials (RCTs) have investigated the role of
P2Y
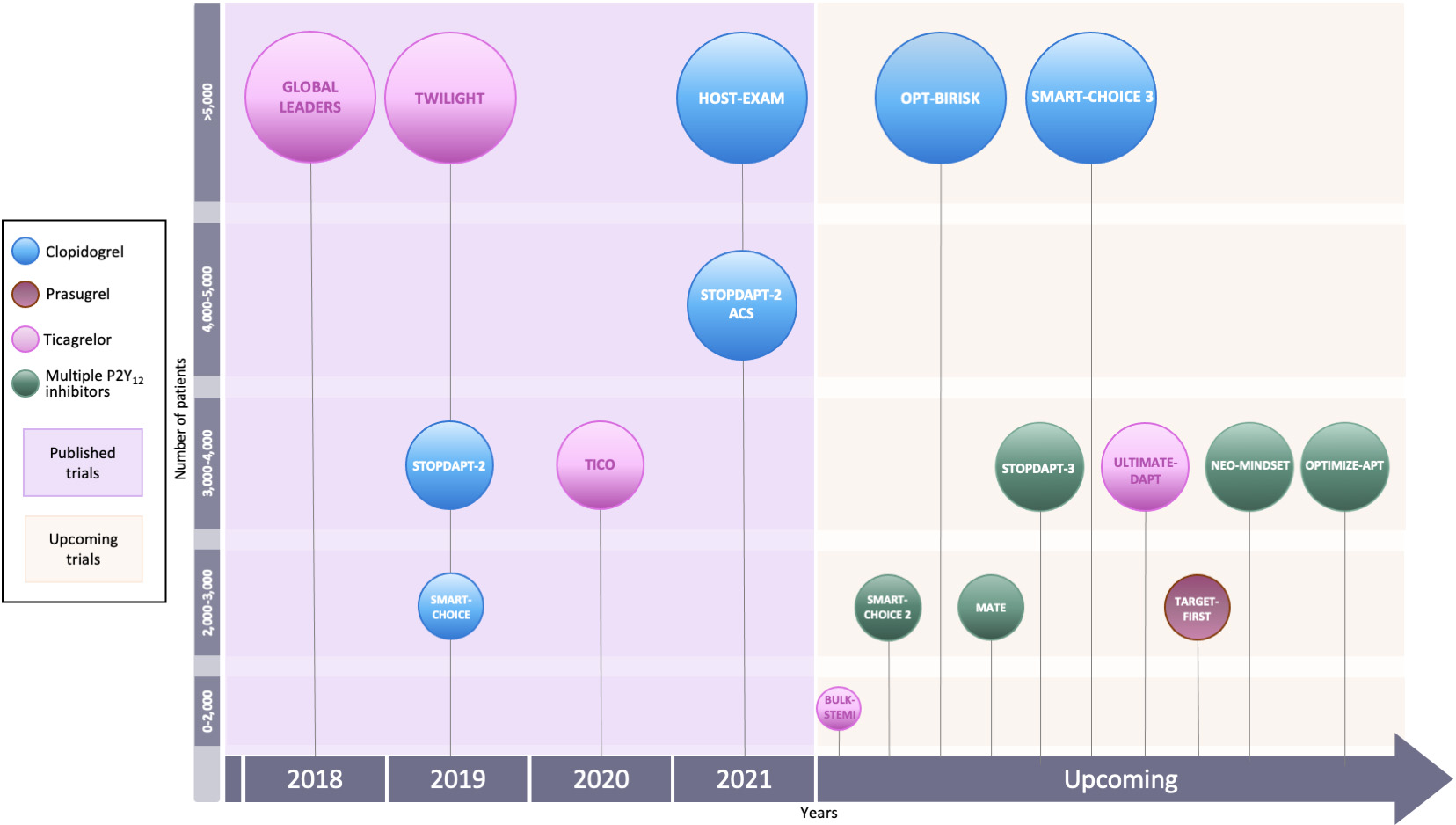 Fig. 2.
Fig. 2.Randomized clinical trials of P2Y
RCTs on early P2Y
RCTs investigating short DAPT followed by aspirin monotherapy showed consistent
benefits in terms of bleeding mitigation as compared to standard DAPT (i.e., six
to 12 months depending on the clinical setting). Although conclusive findings
about ischemic protection cannot be drawn mostly due to the enrolment of low-risk
patients and some lack of statistical power, meta-analyses have warned about the
potential increase in the risks of myocardial infarction (MI) or stent thrombosis
following early DAPT discontinuation [31, 32]. Evidence of bleeding reduction with
clopidogrel monotherapy compared with DAPT in the setting of cerebrovascular
disease prompted the initiation of RCTs in PCI patients to investigate DAPT
shortened to three months followed by P2Y
| SMART-CHOICE | TWILIGHT | TICO | |
| Population | East-Asian patients undergoing PCI (n = 2993) | Patients at high risk of bleeding or ischemic events undergoing PCI (n = 7119) | East-Asian patients with ACS undergoing PCI (n = 3056) |
| ACS | 58% | 65% | 100% |
| P2Y |
Clopidogrel | Ticagrelor | Ticagrelor |
| Randomization timing | At the time of PCI | Three months after PCI | At the time of PCI |
| Investigational strategy | DAPT for three months, followed by P2Y |
P2Y |
DAPT for three months, followed by P2Y |
| Control strategy | DAPT for 12 months | DAPT for 12 months | DAPT for 12 months |
| Follow-up | Twelve months from randomization | Twelve months from randomization (i.e., 15 months from PCI) | Twelve months from randomization |
| Primary outcome(s) | Death, MI or stroke (difference 0.4%; one-sided 95% CI -∞ to 1.3%; p = 0.007 for noninferiority) | BARC type 2, 3 or 5 bleeding (HR 0.56; 95% CI 0.45 to 0.68; p |
Death, MI, stent thrombosis, stroke, target-vessel revascularization or TIMI major bleeding (difference –1.98%; 95% CI –3.50% to –0.45%; HR 0.66; 95% CI 0.48 to 0.92; p = 0.01) |
| Death, MI or stroke (difference –0.06%; 95% CI –0.97 to 0.84; HR 0.99; 95% CI 0.78 to 1.25; p | |||
| Bleeding outcome | BARC type 2-5 bleeding (HR, 0.58; 95% CI, 0.36 to 0.92; p = 0.02) | BARC type 2, 3 or 5 bleeding (HR 0.56; 95% CI 0.45 to 0.68; p |
TIMI major bleeding (HR 0.56; 95% CI 0.34 to 0.9; p = 0.02) |
| Results are presented by reporting the effect of interventional strategy versus
reference treatment. Abbreviations: ACS, acute coronary syndrome; BARC, bleeding academic research consortium; CI, confidence interval; DAPT, dual antiplatelet therapy; HR, hazard ratio; MI, myocardial infarction; PCI, percutaneous coronary intervention; P2Y | |||
The SMART-CHOICE open-label noninferiority trial randomized 2993 East Asian
patients undergoing PCI to three-month DAPT followed by clopidogrel monotherapy
or 12-month DAPT [35]. P2Y
TWILIGHT was a randomized double-blind RCT exploring the effect of aspirin
discontinuation after three months of DAPT in patients at high risk of bleeding
or ischemic events undergoing PCI [39]. After three months, 7119 patients who had
not adverse events while on DAPT were randomized to receive ticagrelor plus
placebo or ticagrelor plus aspirin for additional one year. The primary endpoint
was BARC bleeding type 2, 3 or 5, while ticagrelor monotherapy was also tested
for noninferiority to DAPT with respect to major adverse cardiovascular events
(MACEs). At 12 months after randomization, ticagrelor monotherapy significantly
reduced the incidence of bleeding (4.0% vs. 7.1%; HR 0.56; 95% CI 0.45 to
0.68; p
Similarly, the TICO trial investigated ticagrelor monotherapy after three-month DAPT in East Asian ACS patients [50]. Differently from the TWILIGHT trial, patients (n = 3056) were randomized at the time of PCI to receive either three-month DAPT followed by ticagrelor monotherapy or 12-month ticagrelor-based DAPT. Ticagrelor monotherapy was significantly associated with lower rates of the primary endpoint of net adverse cardiovascular events (NACEs) as compared to DAPT (3.9% vs. 5.9%; difference –1.98%; 95% CI –3.50% to –0.45%; HR 0.66; 95% CI 0.48 to 0.92; p = 0.01), driven by a reduction in major bleeding (1.7% vs. 3.0%; HR 0.56; 95% CI 0.34 to 0.91; p = 0.02), without a significant difference in the risk of MACCE (2.3% vs. 3.4%; HR 0.69; 95% CI 0.45 to 1.06; p = 0.09) or stent thrombosis (0.4% vs. 0.3%; HR 1.51; 95% CI 0.43 to 5.33; p = 0.53). Results were similar in multiple subgroup analyses and in a landmark analysis between three and 12 months [50].
Despite limitations and heterogeneity in the design and conduction of these RCTs, in aggregate they showed that shortening DAPT to three months by withdrawing aspirin is associated with a reduction in bleeding as compared to standard DAPT, with no overt signals of harm with respect to ischemic or thrombotic protection, both in CCS and ACS patients.
DAPT can be also shortened by withdrawing aspirin after only one month as investigated by three RCTs (Table 3).
| GLOBAL LEADERS | STOPDAPT-2 | STOPDAPT-2 ACS | |
| Population | Patients undergoing PCI (n = 15,968) | East-Asian patients undergoing PCI (n = 3045) | East-Asian patients with ACS undergoing PCI (n = 4169) |
| ACS | 47% | 38% | 100% |
| P2Y |
Ticagrelor | Clopidogrel | Clopidogrel |
| Randomization timing | At the time of PCI | At the time of PCI | At the time of PCI |
| Investigational strategy | DAPT for one month, followed by P2Y |
DAPT for one month, followed by P2Y |
DAPT for one-to-two months, followed by P2Y |
| Control strategy | DAPT for 12 months, followed by aspirin monotherapy for 12 months | DAPT for 12 months | DAPT for 12 months |
| Follow-up | Twenty-four months from randomization | Twelve months from randomization | Twelve months from randomization |
| Primary outcome(s) | Death or Q-wave MI (rate ratio 0.87; 95% CI 0.75 to 1.01; p = 0.073) | Cardiovascular death, MI, stroke, stent thrombosis, or TIMI major or minor bleeding (difference –1.34%; 95% CI –2.57 to –0.11; HR 0.64; 95% CI 0.42 to 0.98; p |
Cardiovascular death, MI, stroke, stent thrombosis, or TIMI major or minor bleeding (HR 1.14; 95% CI 0.80 to 1.62; p = 0.06 for noninferiority) |
| Bleeding outcome | BARC type 3-5 bleeding (rate ratio 0.97; 95% CI 0.78 to 1.20; p = 0.77) | Major bleeding (absolute difference –1.13%; 95% CI –1.84% to –0.42%; HR 0.26; 95% CI 0.11 to 0.64; p = 0.004 for superiority) | TIMI major or minor bleeding (absolute difference –0.63%; 95% CI –1.20% to –0.06%; HR 0.46; 95% CI 0.23 to 0.94) |
| Results are presented by reporting the effect of interventional strategy versus
reference treatment. Abbreviations: ACS, acute coronary syndrome; BARC, Bleeding Academic Research Consortium; CI, confidence interval; DAPT, dual antiplatelet therapy; HR, hazard ratio; MI, myocardial infarction; PCI, percutaneous coronary intervention; P2Y | |||
The GLOBAL LEADERS multicenter open-label superiority RCT randomized 15,968
all-comer PCI patients to either one-month DAPT with aspirin and ticagrelor
followed by ticagrelor monotherapy for 23 months or standard 12-month DAPT with
aspirin and a P2Y
The STOPDAPT-2 noninferiority RCT investigated a one-month DAPT with aspirin and
clopidogrel or prasugrel followed by clopidogrel monotherapy as compared to
standard DAPT with aspirin and clopidogrel for 12 months in 3045 East Asian
patients undergoing PCI [64]. One-month DAPT was noninferior and also superior to
standard DAPT in terms of NACE at 12 months (2.36% vs. 3.0%; absolute
difference –1.34; 95% CI –2.57% to –0.11%; HR 0.64; 95% CI 0.42 to 0.98;
p
Similarly, the STOPDAPT-2 ACS trial enrolled 4136 Japanese patients undergoing PCI due to an ACS (partially from the STOPDAPT-2 cohort) translating the same design of the STOPDAPT-2 trial to a different population. One-month DAPT failed to prove noninferior to 12-month DAPT for NACE (3.2% vs. 2.8%; absolute difference 0.37%; 95% CI –0.68% to 1.42%; p = 0.06 for noninferiority), with a numerical increase in MACE (2.8% vs. 1.9%; absolute difference 0.90%; 95% CI –0.02% to 1.82%; HR 1.50; 95% CI 0.99 to 2.26), particularly MI (HR 1.91; 95% CI 1.06 to 3.44), and a reduction in bleeding (0.5% vs. 1.2%; absolute difference –0.63%; 95% CI –1.20% to –0.06%; HR 0.46; 95% CI 0.23 to 0.94); there was no difference in stent thrombosis between the two groups (0.5% vs. 0.2%; HR 2.29; 95% CI 0.70 to 7.42) [69].
In the pooled STOPDAPT-2 total cohort, clopidogrel monotherapy was noninferior (and not superior) to standard DAPT in terms of net benefit (2.84% vs. 3.04%; HR 0.94; 95% CI 0.70 to 1.27; p = 0.001 for noninferiority; p = 0.68 for superiority), with a reduction in bleeding (0.50% vs. 1.31%; HR 0.38; 95% CI 0.21 to 0.70; p = 0.002), without a significant increase in the risk of MACE (2.40% vs. 1.97%; HR 1.24; 95% CI 0.88 to 1.75; p = 0.14 for noninferiority; p = 0.23 for superiority) [70].
Results from these trials showed that shortening DAPT to one month could be a viable option in selected patients (e.g., high bleeding risk, particularly among CCS patients), with a note of caution and more data warranted in patients with ACS.
There is also preliminary evidence about very early (i.e., immediately after the
procedure) aspirin withdrawal in patients undergoing PCI. The only experience in
this setting is represented by the ASET pilot study, which is also the only
investigation of prasugrel monotherapy so far [71]. This multicenter open-label
single-arm study enrolled 201 CCS patients with low anatomical complexity (i.e.,
SYNTAX score
Meta-analyses of the GLOBAL LEADERS, SMART-CHOICE, STOPDAPT-2, TWILIGHT and TICO
trials confirmed that shortening DAPT to one or three months by discontinuing
aspirin reduced the incidence of bleeding as compared with standard DAPT, without
any increase in MACE, both in CCS and ACS patients [72, 73]. In addition, an
individual patient-level meta-analysis of six RCTs (also including the small
DACAB trial on ticagrelor monotherapy after coronary artery bypass grafting
[CABG]) confirmed that P2Y
Collectively, the results of these RCTs and meta-analyses suggest that
shortening DAPT to three or one month and continuing with P2Y
P2Y
The first randomized comparison between aspirin and a P2Y
In patients with coronary artery disease, clopidogrel monotherapy was tested over aspirin in patients with stabilized MI or with CCS, with overall neutral results [80, 81]. Similar findings were obtained with ticagrelor monotherapy compared to aspirin in patients undergoing CABG [82, 83]. However, all these trials were small, conducted in heterogeneous patient cohorts and did not avail from the use of current therapeutical standards of care.
A meta-analysis of 42,108 patients with established atherosclerosis from nine
randomized trials showed that, compared to aspirin, P2Y
Some modern day evidence on the use of P2Y
| GLOBAL LEADERS landmark analysis | HOST EXAM | |
| Population | All-comer PCI patients who did not experience any adverse event during the first year and who adhered to the assigned treatment (n = 11,121) | East-Asian patients undergoing PCI (n = 5530) |
| ACS | 46% | 70% |
| P2Y |
Ticagrelor | Clopidogrel |
| Randomization timing | At the time of PCI (main trial) | Six-to-18 months after PCI |
| Investigational strategy | P2Y |
P2Y |
| Control strategy | Aspirin monotherapy for 12 months | Aspirin monotherapy for 24 months |
| Follow-up | Between 12 and 24 months from randomization | 24 months from randomization (30–42 months from PCI) |
| Primary outcome(s) | Death, or Q-wave MI (adjusted HR 0.74; 95% CI 0.58 to 0.96; p = 0.022) | Death, non-fatal MI, stroke, readmission due to ACS or major bleeding (HR 0.73; 95% CI 0.59 to 0.90; p = 0.0035) |
| Bleeding outcome | BARC type 3–5 bleeding (adjusted HR 1.89; 95% CI 1.03 to 3.45; p = 0.005) | BARC 2–5 bleeding (HR 0.70; 95% CI 0.51 to 0.98; p = 0.036) |
| Results are presented by reporting the effect of interventional strategy versus
reference treatment. Abbreviations: ACS, acute coronary syndrome; BARC, Bleeding Academic Research Consortium; CI, confidence interval; HR, hazard ratio; MI, myocardial infarction; PCI, percutaneous coronary intervention; P2Y | ||
This analysis included more than 11,000 patients who did not experience any adverse event during the first year and who adhered to the assigned treatment. Ticagrelor monotherapy significantly reduced the incidence of MACE with respect to aspirin monotherapy (1.90% vs. 2.60%; adjusted HR 0.74; 95% CI 0.58 to 0.96; p = 0.022), but this came at the price of a significant increase in BARC bleeding type 3-5 (0.5% vs. 0.3%; adjusted HR 1.89; 95% CI 1.03 to 3.45; p = 0.005) [19].
The only randomized head-to-head comparison between clopidogrel and aspirin in patients undergoing contemporary PCI is represented by the multicenter open-label HOST-EXAM trial, which enrolled 5530 East Asian patients who maintained DAPT without adverse events for six-to-18 months after PCI (Table 4). Patients were randomly allocated to either aspirin monotherapy or clopidogrel monotherapy [20]. At two years, clopidogrel monotherapy was associated with a significantly lower incidence of NACE (5.70% vs. 7.70%; HR 0.73; 95% CI 0.59 to 0.90; p = 0.0035), reflecting reductions in both MACE (3.70% vs. 5.50%; HR 0.68; 95% CI 0.52 to 0.87; p = 0.003) and BARC bleeding type 2–5 (2.30% vs. 3.30%; HR 0.70; 95% CI 0.51 to 0.98; p = 0.036). However, there was no difference between the two strategies in terms of all-cause death; from a numerical standpoint, clopidogrel monotherapy was associated with numerically increased rates of all-cause death (1.90% vs. 1.30%; HR 1.43; 95% CI 0.93 to 2.19; p = 0.101), driven by noncardiac death (1.20% vs. 0.80%; HR 1.47; 95% CI 0.85 to 2.52; p = 0.167), mainly cancer-related [20]. This finding should be interpreted with caution due to statistical limitations, in the wait for the HOST-EXAM Extended study that will follow-up patients for a median of 10 years.
Recently, a network meta-analysis of 73,126 patients from 19 studies using DAPT
as common comparator showed a potential net clinical benefit of P2Y
Collectively, the evidence from these trials and meta-analyses supports
P2Y
Antiplatelet therapy is also recommended for patients undergoing PCI requiring
long-term OAC, with a brief period of triple therapy (i.e., aspirin, P2Y
In the early phase after PCI, both DAPT and OAC are required. Two RCTs in the
era of vitamin K antagonists (VKAs) paved the way to the concept of transitioning
from an initial triple antithrombotic therapy to a subsequent DAT [89, 90]. WOEST,
a pioneer RCT of aspirin-free strategies, demonstrated that dual therapy with
clopidogrel and VKA from the time of PCI was superior to long triple therapy with
DAPT plus VKA (for at least one month and up to one year) in reducing bleeding
without increasing MACE [89]. The ISAR-TRIPLE trial explored the reduction of
triple therapy duration from six months to six weeks and, differently from the
WOEST trial, stopped the P2Y
Four RCTs investigated DAT with clopidogrel and a direct oral anticoagulant
(DOAC; i.e., rivaroxaban, dabigatran, apixaban, edoxaban) following a short
course of triple therapy (randomization time from PCI from zero to 14 days across
trials) [91]. The PIONEER AF-PCI showed a reduction in one-year clinically
relevant bleeding with DAT (rivaroxaban 15 mg once daily plus a
P2Y
Two RCTs questioned the role of antiplatelet therapy in patients requiring OAC beyond one year after PCI [97, 98].
In the OAC-ALONE noninferiority trial, prematurely terminated due to slow enrolment, OAC alone failed in proving noninferior to DAT in terms of one-year MACE [97].
The AFIRE trial, comparing rivaroxaban monotherapy to DAT with rivaroxaban and an antiplatelet agent, was stopped early because of increased mortality in the DAT group: at a median follow-up of 24 months, rivaroxaban monotherapy was noninferior to DAT for ischemic events and superior for bleeding [98].
The external validity of these RCTs is limited due to the enrolment of East-Asian patients, the high prevalence of VKA adoption in the OAC-ALONE, and the use of rivaroxaban doses not approved for stroke prevention in the AFIRE trial.
Based on the evidence stemming from RCTs and meta-analyses, both European and American guidelines yielded recommendations on antithrombotic therapy for the early and long-term secondary prevention after PCI [8, 9, 75, 99, 100].
The 2019 guidelines on CCS by the European Society of Cardiology (ESC)
recommended aspirin and clopidogrel for six months after PCI (class of
recommendation [COR] I, level of evidence [LOE] A). Due to the lack of solid
evidence at the time, there were no recommendations about P2Y
Similarly to European guidelines, the 2021 guidelines on coronary artery
revascularization by the American College of Cardiology (ACC), the American Heart
Association (AHA) and the Society for Cardiovascular Angiography & Interventions
(SCAI) introduced a recommendation for short DAPT (one to three months) with
subsequent transition to P2Y
Regarding long-term secondary prevention, ESC guidelines on CCS recommended lifelong aspirin for patients with a previous MI or revascularization (COR I, LOE A). However, clopidogrel was recommended as an alternative in patients with aspirin allergy or intolerance (COR I, LOE B) or in preference to aspirin in patients with either peripheral artery disease or a history of ischemic stroke or transient ischemic attack (COR IIb, LOE B) [75].
In patients with a concomitant indication for OAC, ESC guidelines on NSTE-ACS
and atrial fibrillation recommended a very short triple therapy (i.e., one week)
followed by DAT (clopidogrel plus a DOAC) up to six months and then OAC alone
(COR I, LOE B) [88, 99]. Similarly, a focused update of the AHA/ACC/Heart Rhythm
Society guidelines for the management of atrial fibrillation and an updated North
American expert consensus document recommended a periprocedural triple therapy
followed by DAT with a P2Y
A number of RCTs on P2Y
| Trial | Population | Trial Design | Investigational strategy | Control strategy | Primary outcome |
| BULK-STEMI NCT04570345 | Patients with ACS undergoing PCI (n = 1002) |  |
Ticagrelor | DAPT (aspirin plus ticagrelor) | NACE, MACCE and BARC 3 or 5 bleeding at 12 months from randomization |
| TARGET-FIRST NCT04753749 | Patients with ACS undergoing PCI (n = 2246) |  |
Clopidogrel, prasugrel or ticagrelor | DAPT (aspirin plus any P2Y |
NACCE and BARC 2, 3 or 5 bleeding at 11 months (between one and 12 months from PCI) |
| ULTIMATE-DAPT NCT03971500 | Patients with ACS undergoing PCI (n = 3486) | 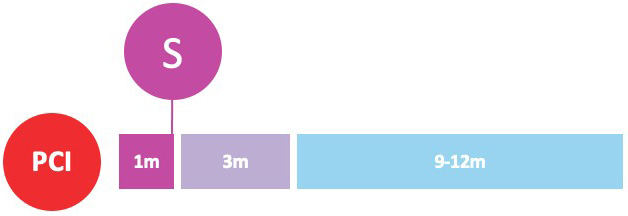 |
Ticagrelor plus matching placebo | DAPT (aspirin plus ticagrelor) | MACCE and BARC 2, 3 or 5 bleeding at 11 months (between one and 12 months from PCI) |
| MATE NCT04937699 | Patients with ACS undergoing PCI (n = 2856) | 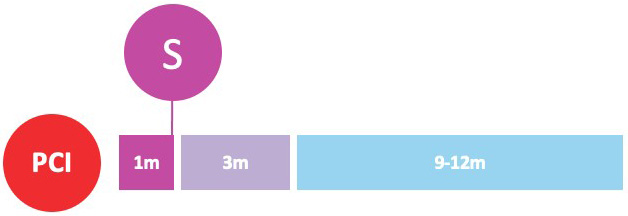 |
Low-dose ticagrelor followed by clopidogrel | DAPT (aspirin plus ticagrelor) | NACCE at 11 months (between one and 12 months from PCI) |
| OPTIMIZE-APT NCT05418556 | Patients with CCS or ACS undergoing intracoronary imaging-guided PCI (n = 3944) | 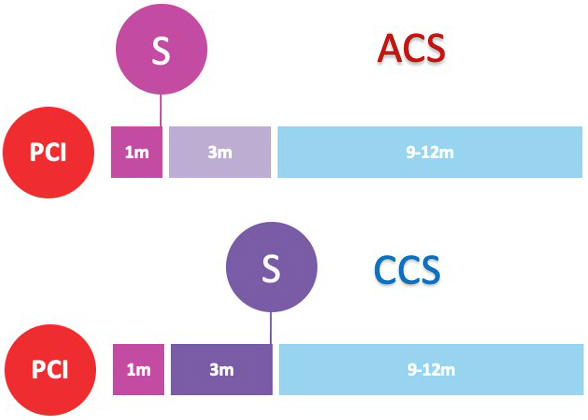 |
One-month DAPT (aspirin plus clopidogrel) followed by 11-month clopidogrel in CCS; three-month DAPT (aspirin and ticagrelor or prasugrel) followed by nine-month ticagrelor or prasugrel in ACS | One-year DAPT (aspirin plus clopidogrel, prasugrel or ticagrelor, according to clinical setting) | One-year BARC type 2, 3 or 5; one-year NACE; one-year MACE |
| NEO-MINDSET NCT04360720 | Patients with ACS undergoing PCI (n = 3400) | 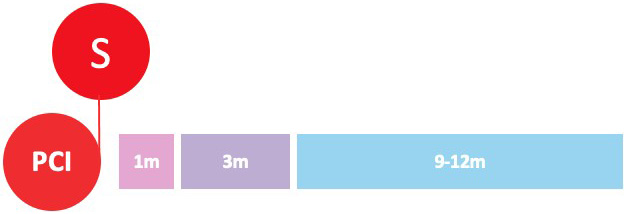 |
Prasugrel or ticagrelor | DAPT (aspirin plus prasugrel or ticagrelor) | MACCE and BARC type 2, 3 or 5 bleeding at 12 months |
| STOPDAPT-3 NCT04609111 | Patients undergoing PCI with ACS or at high risk of bleeding (n = 3110) | 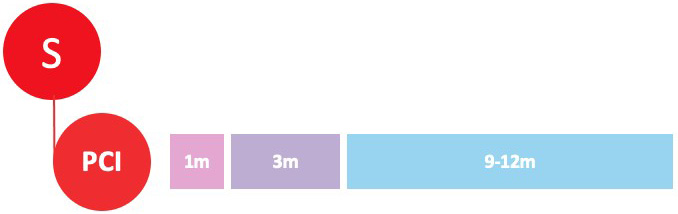 |
Prasugrel before PCI, followed by clopidogrel one month after PCI | DAPT with aspirin and prasugrel, followed by aspirin monotherapy at one month | MACCE and BARC 3 or 5 bleeding at one month |
| OPT-BIRISK NCT03431142 | Patients with ACS undergoing PCI at high risk of both bleeding and thrombosis (n = 7700) |  |
Clopidogrel | DAPT (aspirin plus clopidogrel) | BARC 2, 3 or 5 bleeding at nine months from randomization |
| SMART-CHOICE3 NCT04418479 | Patients undergoing PCI at high risk of thrombosis (n = 5000) | 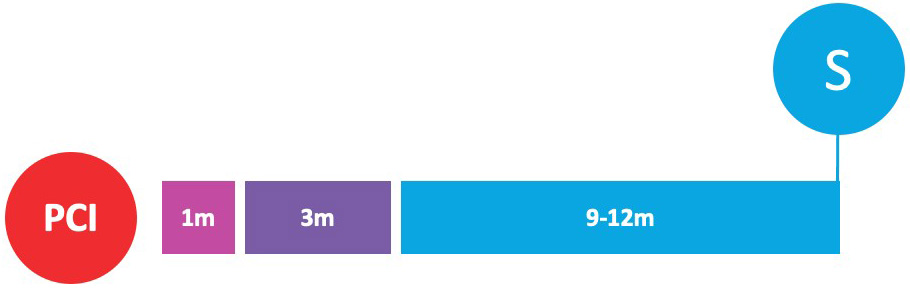 |
Clopidogrel | Aspirin | MACCE at one year after last patient enrolment |
| SMART-CHOICE 2 NCT03119012 | Patients undergoing PCI with bioresorbable scaffold implantation (n = 1520) | 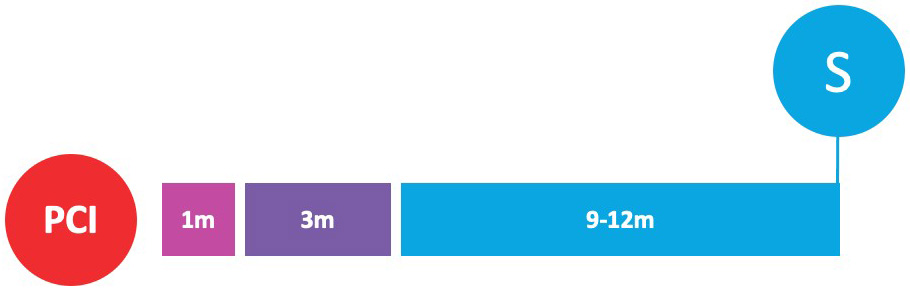 |
Clopidogrel, prasugrel or low-dose ticagrelor | DAPT (aspirin plus clopidogrel or low-dose ticagrelor) | MACCE at 36 months from randomization |
| Abbreviations: ACS, acute coronary syndrome; BARC, bleeding academic research consortium; CCS, chronic coronary syndrome; DAPT, dual antiplatelet therapy; m, months; MACCE, major adverse cardiac and cerebrovascular event; MACE, major adverse cardiovascular event; NACCE, net adverse cardiac and cerebrovascular event; NACE, net adverse cardiovascular event; NCT, clinicaltrials.gov number; PCI, percutaneous coronary intervention; S, DAPT shortening timing. | |||||
In the setting of ACS, three RCTs are investigating DAPT shortening to one
month, followed by a transition to a P2Y
Transitioning a similar concept to a higher risk setting, the BULK-STEMI (NCT04570345) will randomize patients who completed three months of DAPT after PCI for STEMI to receive either ticagrelor monotherapy or DAPT for additional nine months; the primary endpoints will be NACE, MACCE and major bleeding at one year.
Interestingly, two RCTs are exploring an even more precocious “aspirin-free”
approach, consisting of an immediate P2Y
Several trials are also assessing the role of long-term P2Y
In patients undergoing PCI, DAPT with aspirin and a P2Y
Such data has now been integrated into practice guidelines which now reinforce
the evidence on P2Y
ACC, American college of cardiology; ACS, acute coronary syndrome; ADP, adenosine 5’ diphosphate; AHA, American heart association; BARC, Bleeding
Academic Research Consortium; CABG, coronary artery bypass grafting; CCS, chronic
coronary syndrome; CI, confidence interval; COR, class of recommendation; COX-1,
cyclooxygenase-1; DAPT, dual antiplatelet therapy; DAT, dual antithrombotic
therapy; DOAC, direct oral anticoagulant; ESC, European society of cardiology;
HR, hazard ratio; LOE, level of evidence; MACCE, major adverse cardiac and
cerebrovascular event; MACE, major adverse cardiovascular event; MI, myocardial
infarction; NACE, net adverse cardiovascular event; NNT, number needed to treat;
NSTE-ACS, non-ST-segment elevation acute coronary syndrome; OAC, oral
anticoagulation; OR, odds ratio; PCI, percutaneous coronary intervention;
P2Y
AG and MSM drafted the manuscript. DC and DJA revised the manuscript for important intellectual content.
Not applicable.
Not applicable.
This research received no external funding.
AG and MSM declare no conflict of interest. DC declares that he has received consulting fees or honoraria from Sanofi, Daiichi Sankyo and Terumo. DJA declares that he has received consulting fees or honoraria from Abbott, Amgen, AstraZeneca, Bayer, Biosensors, Boehringer Ingelheim, Bristol-Myers Squibb, Chiesi, Daiichi-Sankyo, Eli Lilly, Haemonetics, Janssen, Merck, PhaseBio, PLx Pharma, Pfizer, and Sanofi. D.J.A. also declares that his institution has received research grants from Amgen, AstraZeneca, Bayer, Biosensors, CeloNova, CSL Behring, Daiichi-Sankyo, Eisai, Eli Lilly, Gilead, Janssen, Matsutani Chemical Industry Co., Merck, Novartis, Osprey Medical, Renal Guard Solutions and Scott R. MacKenzie Foundation.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.