
 , Lin Min 1,3, Lin Li 1,3,*
, Lin Min 1,3, Lin Li 1,3,*
1 Key Laboratory of Birth Defects and Related Diseases of Women and Children, Sichuan University, Ministry of Education, 610041 Chengdu, Sichuan, China
2 Department of Gynecology Vip Nursing, West China Second University Hospital, West China School of Nursing, Sichuan University, 610041 Chengdu, Sichuan, China
3 Department of Gynecology and Obstetrics, West China Second University Hospital, Sichuan University, 610041 Chengdu, Sichuan, China
Abstract
Background: Cervical stump cancer is a rare disease, which is
subsequent to a previous subtotal hysterectomy. Among patients who underwent a
subtotal hysterectomy, approximately 1%–3% develop cervical stump cancer which
represents 3%–9% of all the cervical cancers. Methods: After
acquiring consent from our ethics committee, we recruited the subjects and
reviewed the patients’ data of those who were admitted to our hospital from
January 2010 to December 2022. Written informed consent from all the study
participants was acquired, and all materials complied with the Declaration of
Helsinki and ethical standards. The patients’ data records, including clinical
characteristics, treatment methods, human
papillomavirus (HPV) infection conditions before the operation, complications of
the treatment and follow-up status were analyzed. The HPV infection status was
detected by Tellgen systems (Tellgen Corporation, Shanghai, China). SPSS software (Version 22.0, IBM
Company, Armonk, NY, USA) was used for data analysis. Data is shown as mean
Keywords
- cervical stump cancer
- subtotal hysterectomy
- retrospective analysis
Subtotal hysterectomy is a cervix-sparing hysterectomy, which was first performed by Manchester School of Medicine in 1843 [1]. Advocates hypothesized that the remaining cervix may help pelvic support, sexual response and urinary function as well as being associated with shorter operative time, decreased blood loss and less operative complications [2]. Thus, subtotal hysterectomy was routinely undertaken in China for benign gynecologic conditions in the past decades. Although total hysterectomy has taken the place of subtotal hysterectomy, there still remains a large number of women experienced a subtotal hysterectomy with retained cervical stump.
The first cervical stump cancer was reported in 1895 [3]. Among the patients receiving a subtotal hysterectomy, approximately 1%–3% will develop cervical stump cancer resulting in 3%–9% of all cervical cancers [4]. The mean age for the stump cancer patient was older when compared to those with cervical cancer, which may add to a poorer prognosis [5]. There was no difference in the long term prognosis for radiotherapy treated squamous cell carcinoma cervical stump cancer and other cervical carcinomas, however the prognosis for adenocarcinoma stump cancers was worse than those with an intact uterus [4, 6].
Although the incidence trend of cervical stump carcinoma has risen in recent years, clinical research is still insufficient. Thus, we present this retrospective analysis and review of the related literatures.
The study was reviewed and approved by the ethics committee of West China Second University Hospital, Sichuan University, China. All the patients were recruited following the receipt of written consent between January 2010 to December 2022; all procedures performed in the study were in accordance with the ethical standards of the institutional research committee and with the declaration of Helsinki. Inclusion criteria for patients included: (1) cervical biopsies diagnosed with cervical stump cancer by two pathologists; (2) benign gynecological diseases for previous subtotal hysterectomy. The stage of the tumor was classified by utilizing the International Federation of Gynecology and Obstetrics (FIGO) criteria (2018) for cervical cancer. The patients’ data records, including clinical characteristics, treatment methods, complications of the treatment and follow-up status were analyzed. The human papillomavirus (HPV) infection status was detected by Tellgen systems (Tellgen Corporation, Shanghai, China).
Written informed consent from all the study participants were acquired, and all subjects complied with the Declaration of Helsinki and ethical standards.
SPSS software (Version 22.0, IBM Company, Armonk, NY, USA) was used for data
analysis. Data is shown as mean
There were 127 cervical stump cancer patients received treatment in our hospital. The mean age of patients was 48.41 years, ranging from 33–63 years. There was a mean time of 10.89 years between subtotal hysterectomy and diagnosis of stump cancer (ranging from 0.8 to 27 years) (Table 1).
| Varies | Cervical stump cancer | |
| Age (years) | 48.41 | |
| Body mass index (BMI) (kg/m |
24.48 | |
| Age at sex debut (years) | 20.06 | |
| Sex partners | 2.43 | |
| Interval time between subtotal hysterectomy and diagnosis of stump cancer (years) | 10.89 | |
| Family history of cancer | ||
| Yes | 39 | |
| No | 88 | |
| HR-HPV |
||
| Positive | 115* | |
| Negative | 12 | |
Notice: Data is shown as mean
*Some cases infected with more than one subtype simultaneously.
The reasons for previous subtotal hysterectomy were fibromyoma (82 cases, 64.6%), placental implantation or intrapartum hemorrhage (20 cases, 15.7%), adenomyosis (15 cases, 11.8%), atypical hyperplasia of endometrium (9 cases, 7.1%), and uterus rupture due to traffic accident (1 case, 0.8%).
Vaginal bleeding and postcoital bleeding (93 cases, 73.2%), pelvic pain (17 cases, 13.4%), and abnormal cytology (17 cases, 13.4%) were the most common clinical symptoms. The median interval between the onset of symptoms and a diagnosis was 7.42 months. Twenty-two cases were diagnosed within 2 years of the subtotal hysterectomy.
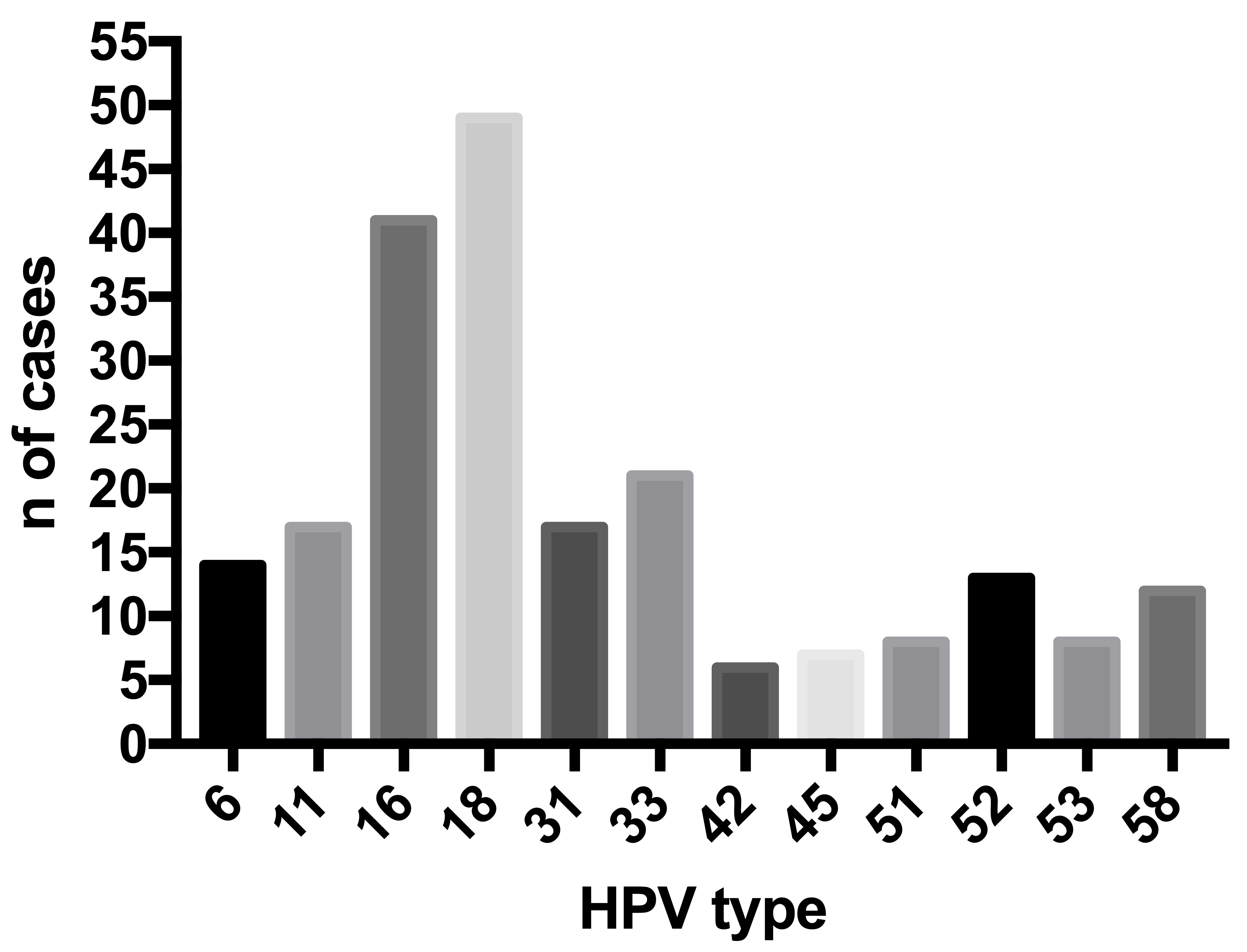
After diagnosed with cervical stump cancer, all the patients received cervical human papillomavirus screening, the distributions with HPV types were in Fig. 1.
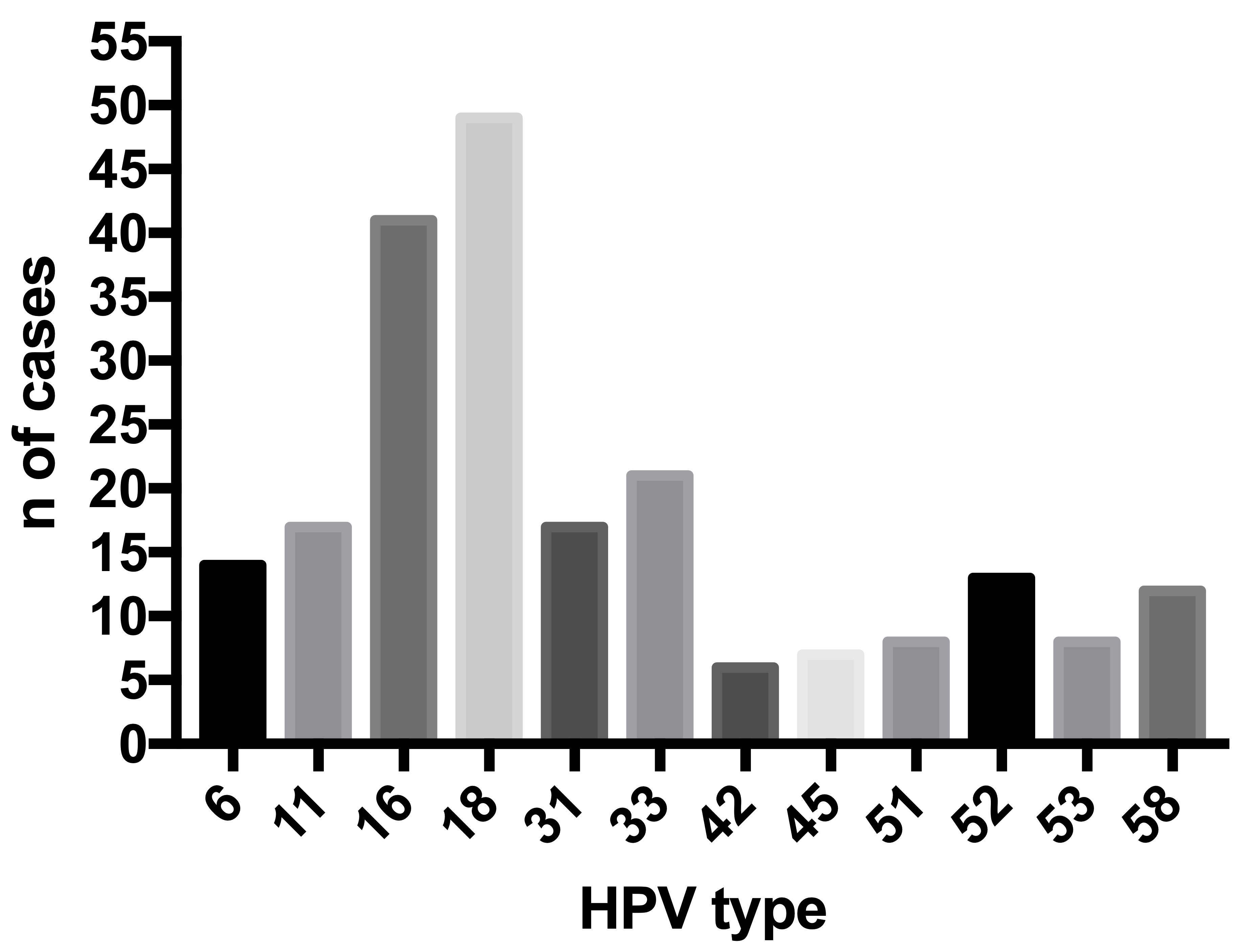 Fig. 1.
Fig. 1.The distributions with HPV types. Notice: Some cases infected with more than one subtype sponteneaous. HPV, human papillomavirus.
Among the 127 stump cancer cases, 72 (57.5%) cases were squamous carcinoma (SCC), adenocarcinoma (AC) in 39 (30.7%) cases, adenosquamous carcinoma (ASC) in 11 (8.7%) cases, neuroendocrine (NE) in 3 (2.4%) cases and undefined type in 2 (1.6%) patient.
Among the 127 cases, 73 cases (57.5%) were in stage I, 45 (35.4%) were in stage II, 8 (6.3%) cases were in stage III, and 1 (0.8%) patient was in stage IV. The distribution of stage associated with pathology is presented in Table 2.
| Variate | SCC | AC | ASC | NE | Others | Total | ||||||
| Stage | No. | % | No. | % | No. | % | No. | % | No. | % | No. | % |
| I | 38 | 29.9 | 22 | 17.3 | 8 | 6.3 | 3 | 2.4 | 2 | 1.6 | 73 | 57.5 |
| II | 28 | 22.0 | 14 | 11.0 | 3 | 2.4 | 0 | 0 | 0 | 0 | 45 | 35.4 |
| III | 5 | 3.9 | 3 | 2.4 | 0 | 0 | 0 | 0 | 0 | 0 | 8 | 6.3 |
| IV | 1 | 0.8 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0.8 |
| Total | 72 | 56.6 | 39 | 30.7 | 11 | 8.7 | 3 | 2.4 | 2 | 1.6 | 127 | 100 |
SCC, squamous carcinoma; AC, adenocarcinoma; ASC, adenosquamous carcinoma; NE, neuroendocrine carcinoma.
To our patients, the treatment methods for cervical stump cancer are the same as for cancer of cervix. Ninety-five cases in early stages received transvaginal trachelectomy or a radical trachelectomy and pelvic lymphadenectomy (either laparoscopic or laparotomic abdominal). The rest 32 cases in late stages received concurrent chemoradiotherapy. The details of the stump patients are in Table 3.
| Variate | Transvaginal trachelectomy (10 cases) | Laparoscopic surgery (54 cases) | Laparotomic abdominal surgery (33 cases) | p | |
| Age (years) | 47.88 |
48.32 |
49.01 |
0.572 | |
| Interval time between subtotal hysterectomy and diagnosis of stump cancer (years) | 11.23 |
10.01 |
10.76 |
0.464 | |
| Blood loss (mL) | 202 |
267 |
525 |
0.015 | |
| Surgery time (min) | 128 |
212 |
279 |
0.047 | |
| Stage | |||||
| I | 5 | 45 | 25 | 0.067 | |
| II | 5 | 9 | 8 | ||
| Lymph node metastasis | |||||
| Yes | 2 | 18 | 12 | 0.617 | |
| No | 8 | 34 | 21 | ||
| Lymph vascular space invasion | |||||
| Yes | 3 | 22 | 14 | 0.776 | |
| No | 7 | 32 | 19 | ||
| Resection margin of the vaginal involvement | |||||
| Yes | 1 | 5 | 3 | 0.996 | |
| No | 9 | 49 | 30 | ||
| Hospital stay (d) | 5.77 |
7.31 |
8.59 |
0.031 | |
| Urinary catheter removement (d) | 14.66 |
21.54 |
21.98 |
0.32 | |
| Residual urine volumes (mL) | 66.76 |
80.32 |
73.87 |
0.18 | |
Seventeen cases (stage I-9 cases, II-6 cases, III-2 cases, IV-0 cases) lost follow-up after discharging from our hospital and the rest 110 cases were included in the follow-up. The median observation time was 65 months (range 4–129 months). The 5-year disease-free rate for all patients was 51.8% (57 cases, stage I-35 cases, II-21 cases, III-1 case, IV-0) and the 5-year overall survival for all patients was 77.3% (85 cases, stage I-50 cases, II-32 cases, III-3 cases, IV-0), respectively. Poor histologic differentiation correlated with a decreased long-term progression-free survival. Cigarette addiction patients, and those receiving prolonged courses of external beam irradiation, had a trend toward a worse prognosis. Vaginal bleeding (31 cases), gastrointestinal symptoms (25 cases) and vaginal contracture (17 cases) were the most common complications.
Although supracervical hysterectomy is being gradually abandoned, it is still performed in some remote areas with poor medical care in China [2]. Most patients in less developed areas lack regular follow-up screening for cervical cancer and seek medical help only after the appearance of clinical symptoms such as abnormal vaginal bleeding and vaginal discharge [2]. Thus, the cervical stump carcinoma was diagnosed late after the sub-total hysterectomy [2]. From current theory, cervical stump cancer can be classified as two types: the one arising after subtotal hysterectomy within 2 years and the one formulating de novo from the stump itself after 2 years of the subtotal hysterectomy [7]. The former one can be a pseudo syndrome, which the cancer may have been already existed without notice and left behind the subtotal hysterectomy. Some researchers suggested a minimum interval time of 2 years between subtotal hysterectomy and diagnosis of stump cancer is necessary to support a true cervical stump cancer [8]. As described, in our study the time elapsed between the subtotal hysterectomy and the diagnosis of cancer of the cervical stump was various from 0.8 to 27 years. Some cases diagnosed within 2 years after subtotal hysterectomy drew our attention because of the fact that patient must already have been presenting the tumor at the time of the surgery. Thus, a 2-year mini-mum interval between subtotal hysterectomy and diagnosis is required to establish a true diagnosis of carcinoma of the cervical stump.
The morbidity of stump cancer is varied from 0.2% to 3.0% [9, 10, 11, 12, 13]. Both of this study and previous literature presented that fibromyoma is the most common reason for the former operation [1]. Based on another research of our team, we found that younger patients preferred to subtotal hysterectomy to cope with benign gynecological diseases and paid lower attention to medical follow-up examines and younger females are usually more active in sex action with higher possibility of HPV infection [14].
Squamous cancer is the most common type in cervical cancer, accounting for about 75% and adenocarcinoma is the second place, accounting for about 20% [6]. HPV-16 is associated with cervical squamous cancer incidence and HPV-18 is associated with adenocarcinoma formulation [15]. In our research, the proportion of adenocarcinoma was 30.7% in cervical stump cancer, and the incidence of HPV-18 infection was higher than HPV-16, which possibly suggested the endocervical lesion maybe missed by the cervical cytology screening after the subtotal hysterectomy. The sensitivity of pap-test is about 40%, in order to elevate this rate, HPV-DNA molecular testing can be added and the combination reached a sensitivity about 90% [16]. By the way, neither HPV-DNA nor Pap-test can predict patients’ risk of progression. We suppose that prior to the subtotal hysterectomy, a cervical cancer and HPV screening may be in arranged.
Patients with stage II carcinoma were found most frequently [17]. Hellström et al. [6] studied 145 cases of cancer of the cervical stump from 1959 to 1987, also found the greatest frequency in that stage. Considering the time that elapses for a tumor to reach stage II is very long, leading to the suspicion that the patients that underwent subtotal hysterectomy were probably inadequately followed up with Pap smears after the surgery.
To those patients within stage I or IIb, surgery is the prior treatment method [17]. Because of the disturbed anatomy, adhesion formations by the former surgery, the stump operation can be more difficult. Comparing with laparotomy, laparoscopy provides more clearly identify the ureter, and fewer injuries occur during the operation, a shorter recovery time and hospital stay, and fewer postoperative complications because it is a minimally invasive surgical operation [18].
To late stages, an individualized and comprehensive concurrent chemoradiotherapy is recommended. Intra-cervical radiotherapy may be hampered by the shorter cervical canal. After radiotherapy, high rate of complications has been reported [10, 19, 20]. Based on our study, the changed anatomy lead to more challenge in choosing the position of radiation target and dose distributions, which may answer to the poorer prognosis and complication. The prognosis of stump cancer in early is similar to cervical cancer; while, it is worse in stage III and IV compared with cervical cancer in the same stages [21].
Higher complication rates have been reported by other authors after radiotherapy [20]. In our cases, the patients treated by radiotherapy suffered no severe complications. Furthermore, in relation to radiotherapy, it seems that the changed anatomy after subtotal hysterectomy causes limitations on the delivery of appropriate radiation doses, which may be responsible for the poorer prognosis [9].
This research analyzed clinical characteristics to arouse attention to the rare disease of cervical stump cancer. However, due to the cases are limited, we did not have a further Hierarchical analysis.
The frequency of cervical stump cancer is low, it should be well considered when deciding between supra-vaginal and total hysterectomy and the patients should be well informed the risk for retaining the cervical stump and further cervical stump cancer screening is mandatory. Cervical cytological screening, biopsy and endocervical curettage should be taken before a subtotal hysterectomy.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
JW: Project development, data collection and management, statistical analysis, manuscript writing; XZ: Data collection and management, statistical analysis, manuscript writing, submitting the manuscript; LM: Design of the work, obtaining funding, critical revision of the manuscript, manuscript writing, supervision; LL: Project development, statistical analysis, critical revision of the manuscript, supervision. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was reviewed and approved by the ethics committee of West China Second University Hospital (No.2020-036), Sichuan University, China. All the patients were recruited following the receipt of written consent.
Not applicable.
This study was funded by the Science and Technology Department of Sichuan Province, China (2022YFS0081).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.