


 , Ali Can Gunes 3,†, Cemal Tamer Erel 2,4
, Ali Can Gunes 3,†, Cemal Tamer Erel 2,41 Women’s Health Center, American Hospital, 34365 Istanbul, Turkey
2 Turkish Menopause and Osteoporosis Society, 34098 Istanbul, Turkey
3 Department of Obstetrics and Gynecology, Mamak State Hospital, 06270 Ankara, Turkey
4 Department of Obstetrics and Gynecology, Istanbul University Cerrahpasa School of Medicine, 34098 Istanbul, Turkey
†These authors contributed equally.
Abstract
Objective: The objective of this review is to examine the current state of evidence on postmenopausal testosterone use in women and explore its potential benefits and risks using the SWOT analysis method which is an evaluation system that allows reviewing any issue under the headings of strengths, weaknesses, opportunities and threats. Mechanism: Testosterone plays a role in female sexual physiology through its effects on the brain and peripheral tissues. At the central level, it stimulates regions of sexual function and interacts with specific receptors in the brain to regulate sexual desire, arousal, and satisfaction. At the peripheral level, testosterone affects various tissues and organs that are involved in sexual function, including the vagina, clitoris, and labia. Testosterone interacts with the androgen receptor in cells and triggers various physiological responses depending on the tissue. It stimulates sperm production in the testes, promotes bone growth and maintenance, and increases muscle mass and strength through protein synthesis. Testosterone also has a beneficial effect on bone density and the cardiovascular system, reducing the risk of heart disease and stroke. It influences cognitive functions such as memory, processing speed, and executive function through androgen receptor-regulated regions of the brain. Findings in Brief: Postmenopausal testosterone therapy may improve sexual function, muscle mass, and reduce the risk of osteoporosis. However, its long-term safety and effectiveness are still under debate. Testosterone therapy can be effective in treating certain symptoms in postmenopausal women, but it may also increase the risk of cardiovascular events and endometrial cancer, and can lead to adverse symptoms such as acne and hirsutism. Careful monitoring and regular hormone level checks are necessary to ensure safe and effective use. It’s important to consider the potential risks and benefits when deciding whether testosterone therapy is appropriate for a postmenopausal woman. Conclusions: Testosterone therapy in postmenopausal women may be a valuable treatment option for selected women. However, more research is needed to better understand the long-term effects of its use. Further research may also help to determine optimal dosing and route of administration, as well as specific testosterone preparations for women.
Keywords
- postmenopausal women
- testosterone therapy
- SWOT analysis
Testosterone is a steroid hormone that belongs to the androgen group and is produced in the testicles in men and the ovaries in women, as well as by the adrenal glands in both sexes. Testosterone is primarily responsible for the development of male secondary sexual characteristics, such as increased muscle mass and bone density, and for the regulation of spermatogenesis. Although estrogen is the main area of interest when it comes to women’s health, testosterone has also an important role in female physiology. Testosterone, which is used as a precursor in estrogen production, is also very similar in structure to estrogen. While this similarity creates a perfect harmony in the balance of the body, it poses a challenge for researchers to understand the isolated effect of testosterone.
The menopausal period is a crucial cornerstone to understand the female endocrinology. Since life expectancy is prolonged, women spend almost half of their lives in the menopausal period [1]. Although it affects almost all women, the perspectives on menopause vary in different populations. For example, women in the conservative societies cannot express their sexual problems due to the fear of being stigmatized. As a result, sexual dysfunction is normalized by these women [2]. This situation causes the sexual problems in the postmenopausal period to be underestimated and undervalued. In addition, due to the decline in testosterone levels, a variety of symptoms including fatigue and decreased muscle mass can be seen in women.
The decline in testosterone levels in postmenopausal women has prompted interest in testosterone therapy as a potential treatment for these symptoms. The physiological and therapeutic role of testosterone in menopausal women has been examined in many studies. Although there is still a lack of data in the literature, there is also important evidence-based findings on the role of testosterone in the postmenopausal period. However, the safety and efficacy of testosterone therapy in women remains controversial, and more research is needed to fully understand the effects of testosterone therapy in this population. In this study, we aimed to review these studies in the literature by SWOT analysis method which is an evaluation system that allows reviewing any issue under the headings of strengths, weaknesses, opportunities and threats.
Steroid hormones are close relatives with each other in terms of their molecular structures. They are conventionally classified as glucocorticoids, mineralocorticoids, progestogens with 21 carbons, androgens with 19 carbons, and estrogens with 18-carbon structures. Testosterone is a steroid hormone with pleiotropic effects. Basically, it functions in three distinct ways: directly, by converting to dihydrotestosterone (DHT) or by converting to estradiol (E2). In circulation, approximately 1% of testosterone is in the free form, while 66% of it is bound to sex-hormone binding globulin (SHBG) and 33% to albumin. Although it was thought that free testosterone is the active form, this is a matter of debate today. Because free testosterone is the most easily degradable form of testosterone, its effect on the body to occurs in a limited time [3]. Therefore, free testosterone seems to be relatively “unstable”. These complex mechanisms make it difficult to understand the isolated changes that testosterone produces in the body.
In the context of postmenopausal testosterone use, it is important to consider the conversion of testosterone into other hormones, such as DHT and estrogen, as this can impact the potential biological activity and therapeutic effects of testosterone therapy. The evidence suggests that DHT levels are initially low in women, at about 0.34 nmol/L. However, after the administration of testosterone, DHT levels increase dramatically to roughly 4–6 nM. This suggests that there is a higher conversion rate of testosterone to DHT compared to estradiol in women [4]. In females, only 0.15% of testosterone is converted into estrogen (E2), and studies have shown that treating women with testosterone does not significantly increase estrogen levels [5, 6].
Testosterone acts on cells through its interaction with the androgen receptor. When testosterone binds to the androgen receptor, it triggers a variety of cellular and physiological responses, depending on the tissue in question [7]. For example, in the bone, testosterone promotes bone growth and maintenance, while in muscle tissue, testosterone promotes protein synthesis, which leads to increased muscle mass and strength. Testosterone also has a beneficial effect on bone density, as it increases bone formation and reduces bone resorption [8]. In postmenopausal women, testosterone has been shown to have a beneficial effect on the cardiovascular system, as it probably reduces the risk of heart disease and stroke [9, 10]. Testosterone influences not only the managing sexual behavioral center in the brain, but also cognitive functions such as episodic memory, working memory, processing speed, visual spatial processing, and executive function, which are regulated by the androgen receptor-regulated regions of the brain in both males and females [11]. In addition, the impact of testosterone on a particular tissue is influenced by the tissue-specific nature of various pioneer factors. These factors are regulatory elements of genes that function as binding platforms for lineage-specific transcription factors and sequence-specific effectors of signaling pathways, and they integrate information related to the cellular environment and intracellular conditions to produce a combined response that affects gene expression patterns [12]. Meanwhile, the occupation of androgen receptors changes quickly in response to fluctuations in circulating testosterone levels, and this process suggests their participation in the negative feedback effects of this steroid on the secretion of gonadotropins [13]. Moreover, estradiol increases the duration of nuclear androgen receptor occupation by the testosterone [14]. Therefore, each different specific tissue shows different response to certain levels of testosterone in its milieu. However, testosterone can also have negative effects especially at high levels. Excessive testosterone can lead to a number of health problems, including acne, hirsutism, irregular cycles, infertility and endometrial cancer [15].
SWOT analysis is a powerful tool for evaluating the internal and external factors that can impact the success of an organization, product, or project. The acronym SWOT stands for strengths, weaknesses, opportunities and threats, and the analysis involves examining each of these four elements in detail to gain a comprehensive understanding of the situation at hand.
Strengths refer to the positive attributes and advantages of a project, such as skilled medical staff, state-of-the-art technology, efficient healthcare delivery processes, and a good reputation for quality care. Weaknesses are the internal factors that hinder the success of the healthcare organization or project, such as a shortage of staff or resources, outdated equipment or technology, communication issues, or inefficient management practices. Opportunities in healthcare might include new medical treatments or procedures, changes in patient demographics or behavior, partnerships with other healthcare organizations, or emerging technologies. Threats are external factors that pose a risk to the success of the healthcare organization or project, such as increased competition, changing government regulations or policies, economic instability, or shifts in patient preferences or expectations.
By conducting a SWOT analysis, the information gathered can then be used to develop strategies and tactics that capitalize on strengths, address weaknesses, take advantage of opportunities, and mitigate threats. Herein, we reviewed and summarized the literature on postmenopausal testosterone therapy using a SWOT analysis (Fig. 1).
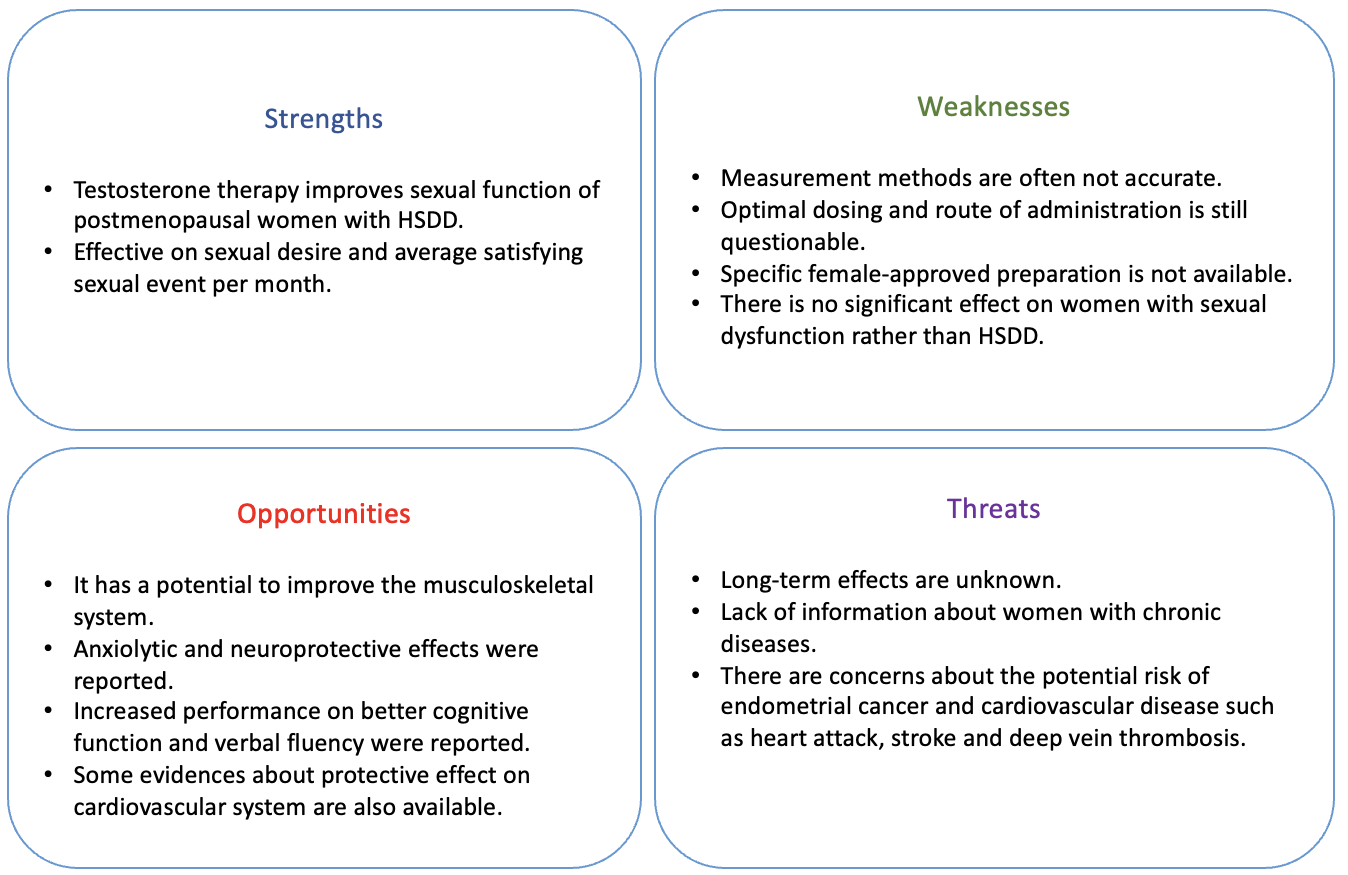 Fig. 1.
Fig. 1.A SWOT (strengths, weaknesses, opportunities and threats) analysis of testosterone therapy in postmenopausal women.
One of the major strengths of testosterone therapy in postmenopausal women is its potential to improve sexual function. Testosterone plays a role in female sexual physiology through its effects on the brain and peripheral tissues. At the central level, testosterone acts on specific receptors in the brain to regulate sexual desire, arousal, and satisfaction, and it has been shown that its biological function in modulating sexual desire is a specific androgen-receptor-mediated effect that does not require conversion into estradiol [16]. It also influences the hypothalamic-pituitary-gonadal axis, which regulates the production and release of hormones involved in reproduction. At the peripheral level, testosterone affects various tissues and organs that are involved in sexual function, including the vagina, clitoris, and labia. Testosterone increases the expression of androgen receptors, promotes the epithelial cell proliferation in the vagina and stimulates blood flow and oxygenation to these tissues, which can enhance sensitivity and increase the likelihood of orgasm [17, 18]. Testosterone has been shown to have beneficial effects on both the smooth muscle compartment and immune response of the vagina [19]. In addition, testosterone may interact with other hormones, such as estrogen and progesterone, to regulate sexual function. For example, estrogen and testosterone may work together to maintain vaginal health and elasticity, which is important for sexual comfort and satisfaction. Interestingly, a recent study revealed that the human vagina has the ability to produce its own androgen, which includes testosterone and DHT, expressing all the necessary enzymes required for their synthesis [20]. The exact mechanism by which testosterone and other hormones interact to regulate sexual function is not fully understood, and more research is needed to better understand this relationship.
Testosterone, which plays an important role in female sexual function, has the potential to be a treatment option in sexual dysfunctions. Studies in the literature show that exogenous testosterone is quite effective especially on the patients with acquired type hypoactive sexual desire disorder (HSDD) [21]. Testosterone was reported to be effective on sexual desire and average satisfying sexual event per month in postmenopausal women [22, 23, 24, 25]. Also, the application of topical estrogen and testosterone therapy may be an effective treatment for postmenopausal women experiencing vestibulodynia [26].
These potential benefits suggest that testosterone therapy may be a valuable treatment option for selected women.
The determination of serum levels of different forms of testosterone poses some problems, with measurement methods of free testosterone often being inaccurate. Therefore, it is commonly recommended to measure total testosterone and SHBG together. Measuring total testosterone by liquid chromatography–tandem mass spectrometry (LC-MS/MS) has an accurate sensitivity but recent research has revealed that SHBG may also be metabolically active. Its blood level is labile and it has been found that there is a strong correlation with BMI (Body Mass Index), central obesity and insulin levels [27, 28, 29]. Because of the challenges on measurement and complexity of physiological mechanism, the exact impacts of testosterone on women’s health arouses curiosity.
There are currently no products specifically intended for use in women, while there are preparations that are used for women at much lower doses than in men. Unfortunately, the available testosterone preparations also differ from country to country. There are still questions about the optimal dosing and route of administration of testosterone therapy in women. Generally reduced dosing of male-approved preparations are preferred. Although it appears to be a safe treatment, there are possible androgenic side effects like acne, hirsutism, hyperlipidemia and endometrial cancer [30, 31]. However, we also recognize the safety data coming from a recent meta-analysis, which revealed that only oral testosterone increased serum lipids while transdermal administration of testosterone was not associated with any increase in cardiovascular risk factors [32]. Some studies have also suggested that the use of topical testosterone products may be associated with an increased risk of skin irritation and other adverse effects [33].
Although testosterone therapy is beneficial on HSDD, there is no significant effect on women with normal sexual function or sexual dysfunction other than acquired-HSDD [21]. There is still conflicting information on testosterone’s potential impact on cardiovascular tissues and cells. A direct correlation between a higher androgenic profile and cardiovascular events is supported by four cohort studies [34, 35, 36, 37]. There are not enough high-quality clinical studies on the musculoskeletal system and the central nervous system [38]. The relative risk of venous thromboembolism also increase with the testosterone usage [39]. Anxiety, depression and aggression are associated with the supratherapeutic testosterone levels [40].
In addition to sexual life, testosterone therapy has been shown to have a positive impact on other aspects of health. Postmenopausal testosterone therapy has a potential to improve muscle mass and strength. Testosterone has anabolic effects on musculoskeletal system. It was reported that high levels of free testosterone increase the bone mineral density (BMD) and bone fracture risk rises in the low levels of it [41, 42]. In a study including 2166 patients, a strong correlation between free testosterone levels and muscle mass, muscle strength and bone microarchitecture was reported [43].
Testosterone therapy may also have a positive effect on brain function. Anxiolytic and neuroprotective effects of testosterone were reported in the literature [44, 45]. Increased performance on better cognitive function and verbal fluency was also found in observational studies [46, 47]. In a recent study and a review, it was reported that testosterone therapy improves mental state and slow the progression of the Alzheimer’s disease [48, 49].
Recent studies on vascular aging have focused on the function of estradiol in the vascular aging of women, but less is known about the effects of diminishing testosterone levels in both sexes. Traditionally it is thought that higher levels of testosterone increase the cardiovascular disease (CVD) risk. Women’s vascular aging seems to be slower than men’s until menopause and recent studies on testosterone’s impact on cardiomyocytes have found that it prevents apoptosis, reduces oxidative stress, and enhances intracellular calcium ion signaling [10, 50, 51]. Additionally, testosterone enhances vasomotor tone and reduces peripheral vascular resistance [9, 52].
In the light of these benefits, testosterone may be beneficial for general body health and well-being. As a result, it may have a positive effect on obesity, diabetes mellitus or hypertension. Therefore, testosterone therapy may offer opportunities for improving overall postmenopausal health.
The lack of long-term safety data on cardiovascular, cancer, and chronic diseases poses the main threat of testosterone therapy in postmenopausal women, despite short-term studies showing promising results [30]. Furthermore, there is no data available about testosterone therapy in the presence of chronic diseases. Interestingly, a randomized controlled study, whose protocol was published in 2012, investigated the use of testosterone gel in 3656 postmenopausal patients with HSDD who had high cardiovascular risk, was completed prematurely and the results were not reported [53]. This raises doubts about the safety of the use of testosterone, especially in postmenopausal women with high cardiovascular risk.
There are concerns about the potential for testosterone therapy to increase the risk of cancer and CVD [54, 55]. It should be highlighted that testosterone treatment has been shown to not induce or increase the risk of breast cancer [56]. However, the risk of endometrial cancer is found to be higher in women with increased levels of total and free testosterone [31]. Several factors have been identified to increase the risk of CVD in postmenopausal women, such as an earlier age of natural menopause, iatrogenically induced menopause during the premenopausal period, vasomotor symptoms, sleep disturbance, and depression [57]. Also, it is known that menopausal hormone therapy has been suggested to reduce CVD risk, especially when initiated within ten years of menopause or before age 60. However, this clarity is not available for postmenopausal testosterone use because studies in the literature are very limited. Some studies have associated testosterone therapy with an increased risk of CVD, including heart attack, stroke, and deep vein thrombosis [33, 55].
Testosterone therapy has been proposed as a potential treatment option for various symptoms and conditions that may occur in postmenopausal women. This includes improving sexual function, increasing muscle mass and strength, and reducing the risk of osteoporosis.
Based on the available evidence, it seems that testosterone therapy can be effective in treating certain symptoms in postmenopausal women, such as decreased sexual desire and dyspareunia in selected HSDD patients and vulvodynia/vestibulodynia. However, the long-term safety of testosterone therapy remains a concern, with studies suggesting an increased risk of cardiovascular events and breast cancer. In addition, testosterone therapy can also lead to the development of adverse symptoms, such as acne and hirsutism, and may suppress natural testosterone production. It is important to consider these potential risks and benefits when deciding whether testosterone therapy is appropriate for a postmenopausal woman. Careful monitoring and regular monitoring of hormone levels is crucial to ensure the safe and effective use of testosterone therapy. Patients should be counseled regarding the lack of long-term safety data and in order to prevent supraphysiologic dosing (Fig. 1).
In conclusion, testosterone therapy in postmenopausal women remains a controversial topic, and further research is needed to fully understand its potential benefits and risks.
FA, ACG and CTE contributed to the study conception and design. Literature search was performed by FA and ACG. The first draft of the manuscript was written by FA and ACG. The article was edited by CTE. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.