
 , Alfredo Ercoli 3
, Alfredo Ercoli 31 Department of Biomedical, Dental, Morphological and Functional Imaging Science, University of Messina, 98122 Messina, Italy
2 Department of Maternal and Child Health, Obstetrics and Gynecology Clinic, University Hospital of Udine, 33100 Udine, Italy
3 Department of Human Pathology of Adult and Childhood “G. Barresi”, Unit of Gynecology and Obstetrics, University of Messina, 98122 Messina, Italy
4 Department of Medicine, Obstetrics and Gynecology Clinic, University of Udine, 33100 Udine, Italy
5 Department of Obstetrics and Gynaecology, Institute for Maternal and Child Health-IRCCS “Burlo Garofolo”, 34137 Trieste, Italy
Abstract
Background: Recently, new surgical systems less invasive than standard laparoscopy have been developed. Among these, robotic single site surgery is playing a pivotal role. In this field, the da Vinci SP (Single-Port) Surgical System (SP1098) is one of the newest surgical technology that presents innovative characteristics that may lead to better surgical outcomes. Few groups have already published their experience and results with this system in gynecology. Methods: The aim of the present systematic review was to provide a comprehensive overview of the status and applications of da Vinci SP1098 in gynecologic surgery. A systematic review of the literature was performed. Studies were identified until September 2022. Results: Six studies were included, reporting a total of 211 patients. The indication for surgery was both benign and malignant disorders. In terms of operative outcomes, the mean/median docking time varied from 2.1 to 5 min while mean/median operating time from 86.5 to 245 min. There was no conversion to multi-port laparoscopy or laparotomy and no major complications related to SP surgery. Conclusions: In conclusion, the preliminary and limited data available regarding the da Vinci SP1098 Surgical System suggest the technical feasibility and safety for its use in gynecologic surgery, with minimal alteration of the surgical technique.
Keywords
- minimally invasive surgery
- single-port surgery
- robotic surgery
In the last years, minimally invasive surgery has gained more and more ground in
surgery. It has helped in reducing patients’ scarring, morbidity, post-operative
pain and hospitalization time [1, 2]. It has been demonstrated by different
studies that gynecologic procedures performed by endoscopic approaches have
similar or improved outcomes when compared to laparotomic approaches [3, 4].
Moreover, in the last decade, there has been an urge to develop new surgical
systems with the aim to be less invasive than with standard laparoscopy. In this
field, new techniques that employ laparoendoscopic single-port surgery (LESS)
instruments were born [5]. LESS can be considered as a less invasive alternative
to multiport laparoscopy. It comprehends a variety of surgical procedures that
can be performed with one single surgical incision into which all instruments are
inserted through one port. Single-port surgery provides better cosmetic outcomes
and improved patient satisfaction. Moreover, even if LESS approach requires a
revision of the surgical technique and may be challenging to adopt, its efficacy
and safety in gynecologic surgery seems to be comparable to traditional
laparoscopy [6], even if the surgical time seems to be prolonged. LESS presents
some technical difficulties, such as limited movement of instruments, internal
and external clashing between instruments, reduced ability to triangulate,
ergonomic discomfort and poor visualization [7, 8]. Robot surgical systems with
optimized ergonomics can compensate for these limitations by improving
visualization. Since 2009, robotic single site surgery using the da
Vinci
We conducted a systematic search following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, and this study protocol was previously registered with PROSPERO (CRD42023422995) [16]. This systematic review includes patients’ information achieved from previously published studies. A comprehensive literature research was conducted in electronic database (MEDLINE, PubMed and Cochrane Library), from inception through September of 2022. The articles were identified with the use of a combination of the relevant heading term, key words, and word variants for: “Da Vinci Single Port”, “SP1098”, “gynecology”, “gynecologic surgery”. The electronic search and the eligibility of the studies were independently assessed by two of the authors (MA, PR). After the first selection, the authors evaluated the full-text copies of selected papers and separately extracted relevant data regarding study characteristics and outcomes. In addition, references in included articles were reviewed to identify additional eligible articles. Differences were discussed with a third author (SC).
We included all studies reporting surgical data about the use of da Vinci SP1098 platform in gynecological surgery. Studies evaluating other da Vinci robots or the use of da Vinci SP1098 in non gynecologic surgeries were excluded. Only full text papers were considered eligible for the inclusion. Non-English language articles were excluded.
The primary outcome was the feasibility of da Vinci SP1098 in gynecologic surgery, evaluating the rate of conversion to multi-port laparoscopy or laparotomy and complications related to single port surgery. The second outcome was the post-operative data. We have also analyzed the total number of cases and the characteristics of the patients. These were expressed as mean or median. We reported patients’ characteristics including age, body mass index, previous history of abdominal surgery, and diagnosed disease. Data collection also included indication for surgery, kind of surgery, estimated blood loss, conversion to multiport robotic surgery or laparotomy and length of hospital stay. The docking time was defined as the time from driving the robot patient cart to the placement of robotic instruments through the port; whereas the operation time was the time from the skin incision to its closure. Clavien-Dindo classification system was used in grading intraoperative and postoperative complications [17].
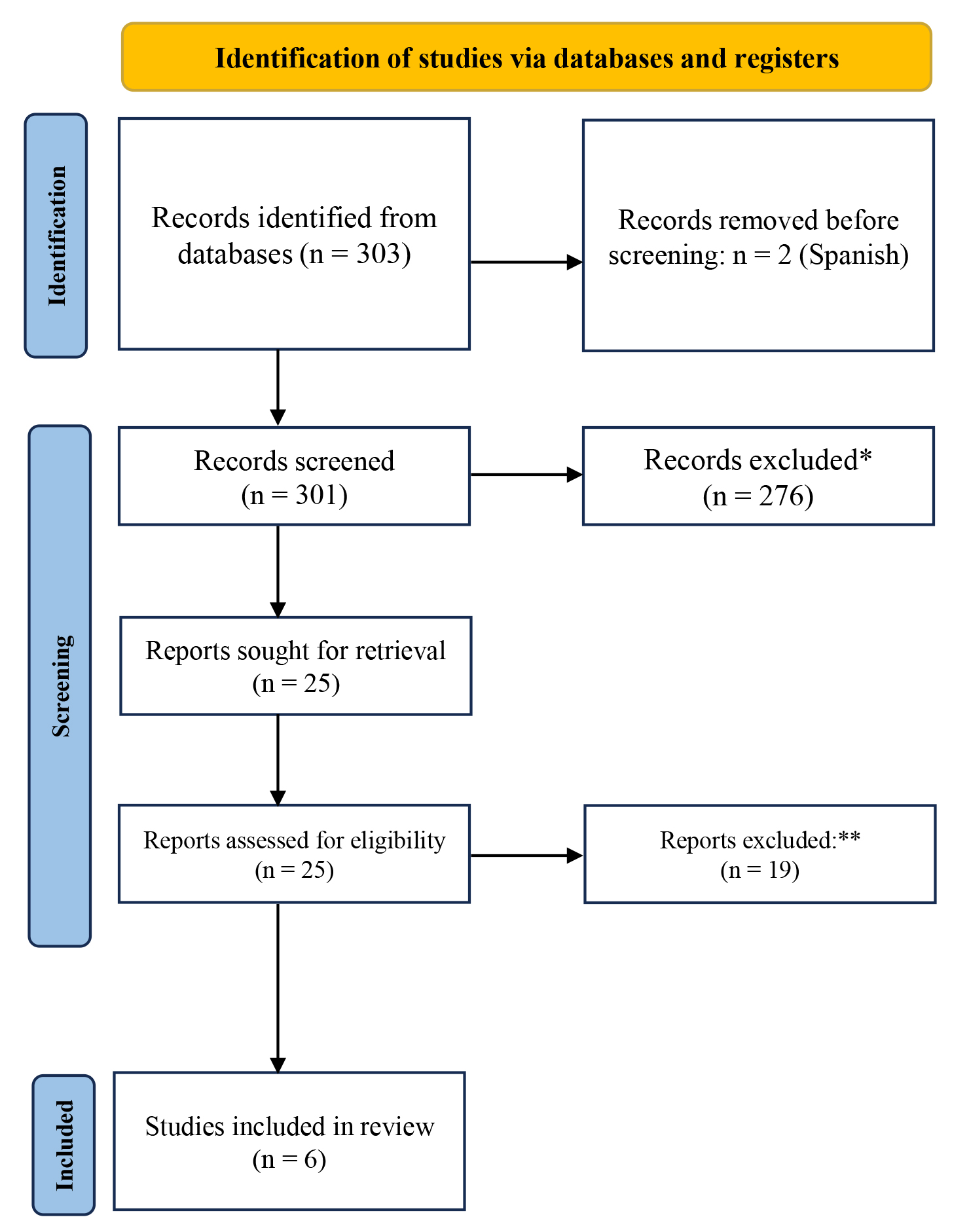
The first search, retrieved a total of 303 studies. 2/303 studies were excluded because of non-English language; 276/303 studies were excluded because they were about non-gynecologic surgeries; 19/303 studies were instead excluded because they were not specifically about da Vinci SP108. This selection, retrieved a final number of six studies (Prisma Flow Diagram, Fig. 1). Of the six identified studies, five were retrospective while one was a prospective observational study [18].
 Fig. 1.
Fig. 1.Study selection flow diagram (in accordance with PRISMA 2020 flow diagram). *276 studies were excluded because, even if they regarded da Vinci Single Port, they were not about gynecologic field. **19 studies were excluded because they were not about da Vinci Single Port (they regarded other da Vinci robots instead).
One study was a comparative report: Lee et al. [19] compared two types of single-incision robotic sacrocolpopexy, single-site robotic sacrocolpopexy, using da Vinci Xi or Si system and single-port robotic sacrocolpopexy, using da Vinci SP. In our review, we have considered only the 9 cases of robotic sacrocolpopexy with da Vinci SP. All the studies were published between 2020 and 2022.
Six articles have been published about the use of da Vinci SP1098 robot in
gynecologic surgery, yielding a total of 211 patients. Detailed patient
demographics and operative results are presented in Table 1,2 (Ref. [8, 18, 19, 20, 21, 22]). In all studies, except one [8], the data were reported as mean.
The mean/median age of patients ranged from 37 to 67.6 years while the
mean/median body mass index ranged from 21.5 to 27.85 kg/m
| Study | Institution | Study design | N | Age (years) mean | BMI mean (kg/m |
Prior surgery | Indications | Procedures (number) |
| Shin HJ, et al. (2020) [22] | Ewha Womans University Seoul Hospital | Retrospective | 31 | 47.7 | 22.7 | 15: TH, myomectomy, ovarian cys- tectomy for endometriosis, salpingectomy, C-section, and appendectomy | Uterine fibroid (18), Adenomyosis (1), Benign ovarian cyst (6), POP (6) | TH + AS (7), Hysteroscopy + AS, SCP (6), Hysteroscopy + AS, SCP, TOT 1), Myomectomy 6), Myomectomy + AS (5), Myomectomy + hysteroscopy (1), AS (3), AS + hysteroscopy (2) |
| Misal M, et al. (2020) [21] | Mayo Clinic, Arizona | Retrospective | 8 | 46.3 | 27.8 | 5: C-section, ablation of endometriosis, salpingectomy and uterine artery embolization for fibroids | AUB (5), post-menopausal bleeding (2), risk reduction surgery (1) | TH + BS (3), MRH + BS + E (1), TH + BS + E (2), TH + BSO (1), TH + BSO + E (1) |
| Ganesan V, et al. (2020) [20] | University of Texas Southwestern | Retrospective | 3 | 67.6 | 26.7 | TH (3/3) Colporrhaphy (2/3) | POP | SCP |
| Lee SR, et al. (2021) [19] | University of Ulsan College of Medicine, Seoul Asan Medical Center | Retrospective | 8 | 66.1 | 23.9 | NR | POP | SCP |
| Lee JH, et al. (2022) [18] | Ewha Womans University Seoul Hospital | Prospective | 61 | 38.5 | 22.7 | 10 | Uterine fibroid | Miomectomy |
| Kwak YH, et al. (2022) [8] | Women’s Cancer Center, Yonsei Can- cer Center in Seoul, Korea | Retrospective | 100 | 37 (median) | 21.5 (median) | 14 | Uterine fibroid (76), Adenomyosis (1), Benign ovarian cyst (2), Endometrial cancer (14), Cervical cancer (7) | Myomectomy (76), TH (2), Endometrial cancer surgical staging (14), RH (3), Radical trachelectomy (3), ovarian cystectomy (2) |
SP, Single-Port; AS, adnexal sugery; AUB, abnormal uterine bleeding; BMI, body mass index; BS, bilateral salpingectomy; BSO, bilateral salpingo-oophorectomy; C-section, cesarean section; E, resection of endometriosis; MRH, modified radical hysterectomy; NR, not recorded; POP, pelvic organs prolapse; RH, radical hysterectomy; SCP, sacrocolpopexy; TH, total hysterectomy; TOT, Transobturator midurethral tension free vaginal tape insertion.
| Study | Operative time mean (min) | Docking time mean (min) | Hospital stay mean (day) | Estimated blood loss mean (mL) | Need for conversion to LPT or MP | Post-operative complications | Follow-up (months) |
| Shin HJ, et al. (2020) [22] | 126.3 | 2.2 | 4.6 | 93.9 | None | 1 (3.2%) | NR |
| Misal M, et al. (2020) [21] | 86.5 | NR | same-day discharge | 37.5 | None | 2 (25%) | 1.5 |
| Ganesan V, et al. (2020) [20] | 225.7 | NR | 1 | 23.3 | None | None | 1 |
| Lee SR, et al. (2021) [19] | 141.8 | 2.31 | NR | 71.25 | None | 2 (25%) | 12 |
| Lee JH, et al. (2022) [18] | 149.9 | 2.1 | 4.5 | NR | None | 15 (24.6%) | NR |
| Kwak YH, et al. (2022) [8] | 245 (median) | 5 (median) | 2.8 | 50 (median) | None | 1 (1%) | NR |
LPT, Laparotomy; MP, Multi-port laparoscopy; NR, not recorded.
The present review provides a summary of the available studies on single-port
robotic surgery using da Vinci SP1098 system in gynecologic field. Robotic single
site surgery was introduced in order to combine the advantages of LESS and
robotic surgery. However, instruments clashing, and the unfavorable ergonomics of
robotic single site surgery can be an issue for the surgeon [23]. Robotic single
site surgery is characterized by several advantages compared to conventional
LESS: better triangulation at the surgical site and improved ergonomics during
surgery. In addition, the robotic platform provides three-dimensional
visualization, a stable camera platform, fine movement, and tremor control
[20, 21, 22]. Reducing number of ancillary trocars should decrease port site
complications, such as herniation of the small bowel and obstruction through the
8 mm robotic port sites. However, robotic single site surgery still presents some
drawbacks, that are mainly the collision and clashing of instruments [24]. The da
Vinci SP1098 platform is the last technologic development in single port surgery,
and it presents innovative characteristics that overcome the limitations
above-mentioned and expand the range of surgical applications. Indeed, this
platform offers to the surgeon similar functionality as the da Vinci multiport
platform, with the exception that 3 multiarticular wrist instruments and a hree
dimensional high resolution (3D-HD) articulated scope are introduced through a
single port. This technology permits distal triangulation of the instrument,
excellent internal and external range of movement and 360
In our review, we analyzed five retrospective studies and only one prospective report. Lee et al. [18] conducted a prospective observational pilot study to evaluate the robotic-single port myomectomy using da Vinci SP platform. In our systematic review, the surgeries incorporated were heterogeneous with mean/median operating time from 86.5 to 245 min, so it was difficult to directly compare them with surgeries performed with different approaches. According to our review, the most commonly perfomed surgery with da Vinci SP1098 was myomectomy. Only in a few cases da Vinci SP1098 was used to treat oncological cases.
The only study that compares da Vinci SP1098 to other robotic platforms is the
manuscript of Lee et al. [19]. They compared 40 cases of single site
robotic sacrocolpopexy, using the da Vinci Xi or Si system, with 8 cases of
sacrocolpopexy, using da Vinci SP. There were no differences in the mean
operative time and in the console time between the two groups (135.3
Concerning the limitations of the SP1098 platform compared to the multiport robotic platform, as highlighted by Ganesan et al. [20], they are the limited surgical field (about 10–25 cm from the port), and restriction of possible movements when all the instruments are deployed. Other drawbacks are that the right angle produced by the elbow joint requires more workspace than the straight instruments, and this could be an obstacle when operating on large-sized uteri. Moreover, although an ancillary trocar can be used for procedures such as suctioning and irrigation, there is still difficulty with the movements of the assistant [22]. Most recently, a new single-port entry system, designed only for da Vinci SP1098, was introduced: the Uni-Port. It has four entry ports of different sizes that can accommodate one da Vinci SP cannula, one 10–15 mm-sized laparoscopic instrument, and two 5 mm-sized laparoscopic instruments at the same time [8].
The main limit of our review is that the data available in the literature are limited and they consist mainly of pilot studies, case series and case reports with a small number of cases and with a short follow-up. Moreover, only one comparative study has been conducted in gynecological surgery and no randomized control studies are present in the literature. Although a small number of cases were included in this review, the heterogenous patients’ characteristics and miscellaneous surgeries performed are reflective of high-volume gynecology practices. Randomized prospective studies that compare da Vinci SP1098 system with conventional LESS or robotic multi-port surgeries are needed to evaluate the possible benefits of this innovative platform. Additional studies examining postoperative outcomes, surgical costs and prospective studies comparing this modality to traditional robotic surgery are needed.
The preliminary and limited data available in the literature on the use of da Vinci SP Surgical System (SP1098) seem to suggest its technical feasibility and safety for gynecologic surgery, with minimal alteration in surgical techniques.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Conceptualization, MA and SC; methodology, GV; validation, AE, RG and LD; formal analysis, MA and SR; investigation, PR and GS; writing—original draft preparation, PR; writing—review and editing, SR and MA; supervision, GV. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work to take public responsibility for appropriate portions of the content and agreed to be accountable for all aspects of the work in ensuring that questions related to its accuracy or integrity.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest. Stefano Cianci is serving as one of the Editorial Board members and Guest editors of this journal. Roberta Granese are serving as one of the Editorial Board members of this journal. We declare that Stefano Cianci and Roberta Granese had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Christos Iavazzo.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.