


 , Nevin Hotun Şahin 2
, Nevin Hotun Şahin 21 Nursing Department, Faculty of Health Sciences, Eastern Mediterranean University, 99628 Famagusta, Northern Cyprus, via Mersin 10, Turkey
2 Department of Women Health and Gynecologic Nursing, Florence Nightingale Nursing Faculty at Istanbul University Cerrahpasa, 34381 Şişli/İstanbul, Turkey
Abstract
Background: Sterile water injection is rapidly gaining popularity as a
method of pain relief in labor. The purpose of this single-blinded randomized
controlled study is to investigate the effect of intradermal sterile water
injection (ISWI) on labor experiences of women who experience low-back pain
during labor. Methods: The sample group of the study was 120 pregnant
women with severe low-back pain during labor (30-sterile water, 30-saline
solution, 60-control). In the study, the baseline low back pain score (
Keywords
- experience
- labor
- low back pain
- pain relief
- satisfaction
- sterile water injections
Most of the obstetric studies about labor pain have focused on abdominal pain due to uterine contractions. However, there are important differences in severity and location of pain during labor [1, 2]. Melzack and Schaffelberg [2] reported that 33% of the women giving birth complained about constant back pain between contractions. Tzeng and Su [1] noted that the rate of the women having constant pain was 45.71%. The women described this pain as dreadful, tiring and agonizing [2]. It is clear that fear, tiredness and anxiety have negative effects on the labor process [3]. Therefore, it has been stated that women may need analgesia for the constant back pain [4, 5]. Not only women but also American College of Obstetricians and Gynecologists (ACOG) have considered labor pain as an indication for treatment [6, 7]. Nevertheless, pharmacological anesthesia has some side-effects and is expensive [3, 8, 9]. In addition, the fact that it is not required and may even be impossible to use in all women who give birth should be taken into account [3, 8]. For this reason, nonpharmacological pain management methods can be good alternatives [7]. There are many nonpharmacological pain management methods in the world. Intradermal sterile water injection is one of them. This method reduce back pain in labor [9].
The analgesic effect of sterile water injections were first described by an American surgeon Halsted in 1885 [10]. Although the mode of their action is not clear, it can be explained by gate control theory [4]. Intradermal or subcutaneous sterile water injections are performed on four different points around the sacrum and four water bubbles are created. Two of them are located on the posterior superior iliac spine and the others are located 3 cm below and 1 cm medial side of the first two bubbles [9, 10].
The literature includes various studies that aimed to determine the effect of sterile water injection on relieving low-back pain during labor using different procedures. The common point of the majority of these studies is that they are based on the comparison of sterile water injection and saline solution injection, and the results are in favor of sterile water injection [11, 12, 13, 14, 15, 16, 17]. Another common point of the studies is that injections were done in each side of the Michaelis Rhomboid [11, 12, 13, 14, 15, 16]. On the other hand, while a study reported that only one intradermal sterile water injection administered in the center of the Michaelis Rhomboid was effective, another study indicated that sterile water injection administered only on two sides of the Michaelis Rhomboid was effective [18, 19]. In addition, a recent multicenter study reported that four injections continued to be the preferred technique, whereas two injections were successful in relief pain [20]. Whether the tissue to be given sterile water injection will affect the targeted analgesic is another debated topic, and the majority of the studies focus on intradermal injections [11, 13, 21, 22]. On the other hand, some study samples showed that subcutaneous sterile water injection was also effective in relieving low-back pain [18, 23, 24, 25]. The literature includes studies that compared sterile water injection and other nonpharmacological pain control methods, yet while one study found sterile water injection more effective than transcutaneous electrical nerve stimulation (TENS), another study found it more effective than acupuncture [26, 27]. The literature includes metanalyses and systematic reviews on the technique. A meta-analysis reported that the technique had no adverse effects on maternal and fetal health [4]. Both systematic reviews concluded that the technique had a strong analgesic effect on relieving low-back pain during labor and thus should be used in labor rooms [10, 28].
In each intervention done during labor, it is important to measure its effects on perinatal outcomes as well as women’s labor experiences [29]. Because dissatisfaction with labor experience could have negative effects on the early postpartum adaptation process, breastfeeding, and maternal and baby attachment and cause postpartum depression and posttraumatic stress disorders [30, 31, 32]. In this regard, a meta-analysis investigating how to achieve a positive labor experience shows that many non-pharmacological pain control methods are ineffective in promoting a positive labor experience [33]. As mentioned above, intradermal sterile water has an analgesic effect. However, unlike many other nonpharmacological pain control methods, it is invasive even if it is minimal and causes pain when it is first done [4, 5]. Therefore, it is necessary to evaluate not only the effects of the method on pregnant women’s pain perception but also on satisfaction and labor experience [4]. However, while few studies in the literature were found to have investigated mothers’ satisfaction with the technique, no studies were found to have investigated its effects on labor experiences [15, 17, 24, 26, 34]. For this reason, this study aimed to investigate the effect of intradermal sterile water injection on pain perceptions and labor experiences of women who experience low-back pain during labor.
H
H
H
A single-blinded randomized controlled design was used in the study.
The study population included all pregnant women presenting to the labor room of
a state hospital in Istanbul for vaginal labor between October 2015 and December
2016. During the study period, 1143 pregnant women who presented to hospital for
labor evaluated. Of 1143 women, 662 did not meet eligibility criteria, 349
declined to participate in the study and 132 accepted to take part in the study.
Then out of 132 pregnant women 32 were randomly assigned into the sterile water
group, 33 into the saline group and 67 into the control group. Since one woman in
the sterile water group, one woman in the saline group and four women in the
control group underwent cesarean section during follow-ups and since one woman in
the sterile water group, two women in the saline group and three women in the
control group gave birth before the ninetieth minute of their follow-ups, they
were excluded from the study. As a result, the study was completed on a total of
120 pregnant women, of whom 30 were in the sterile water group, 30 were in the
saline group and 60 were in the control group (Fig. 1). Whether pregnant women
divided into groups in the study had effects on the power of the study was
analyzed using the “G. Power 3.1.9.7” program (Franz Faul, Universität Kiel, Kiel, Germany). Analysis performed on 120
individuals (30 sterile water group, 30 saline group, and 60 control group) at
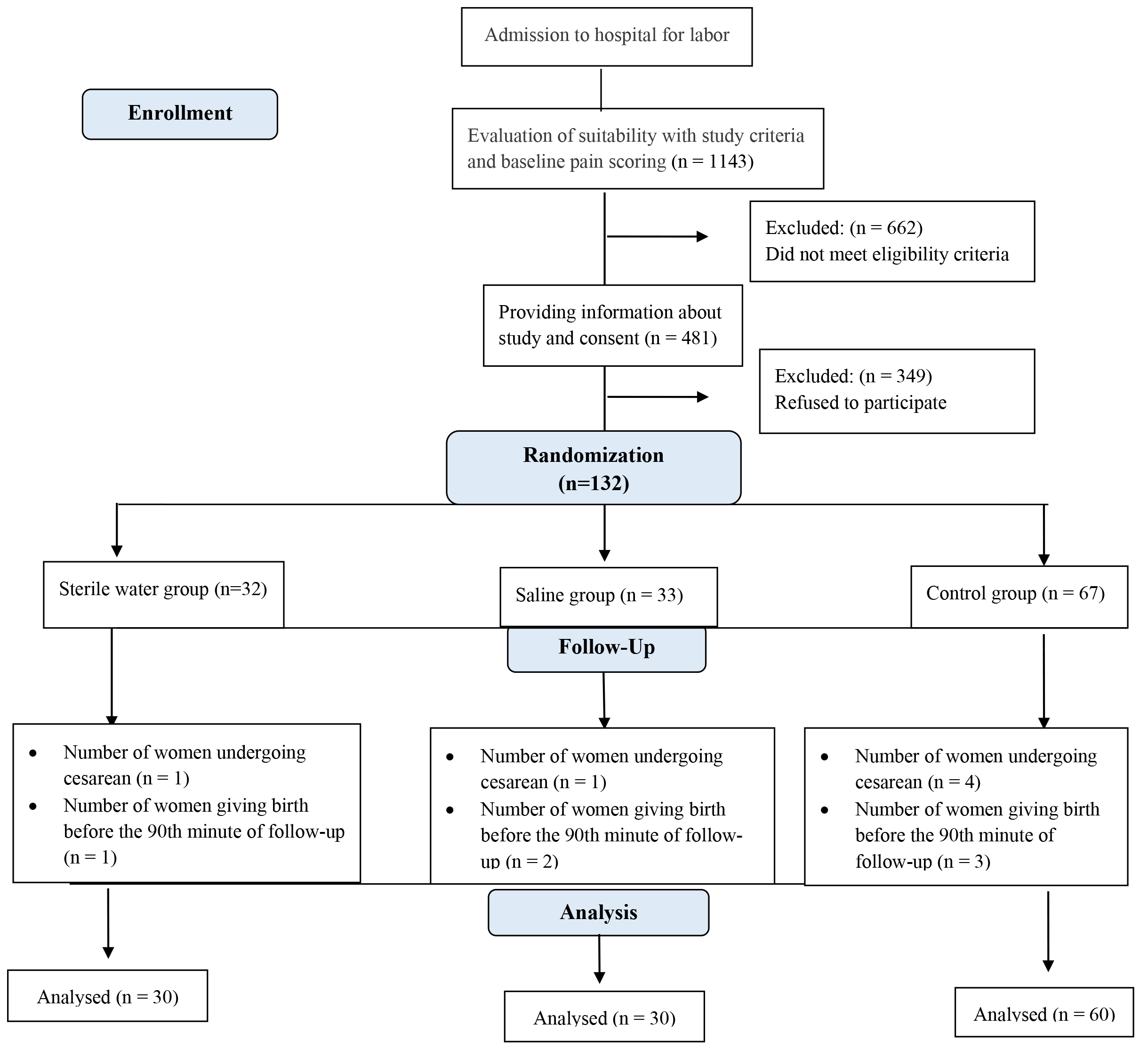 Fig. 1.
Fig. 1.Flow chart of the study participants.
Inclusion criteria of the study were age of 18 years or older, gestation weeks
of 37–42, fetal weight of 2500 gr–4000 gr on ultrasound examination (USG),
pregnancy without risk, having a single live fetus with vertex presentation,
experiencing the active phase of first stage of labor (4–7 cm cervical
dilatation) , severe low back pain (Visual Analogue Scale (VAS
The pregnant women were subjected to the following procedures
The back pain severity of
In these groups, after the basal back pain severity (VAS
This form, developed by the researchers, was composed of questions about age, education, gravida, parity, gestational week, and antenatal care status and body mass index.
The VAS is a unidimensional scale developed for pain assessment. In the scale, individuals are asked to rate their pain between 0 (not at all) and 10 (very much) [36, 37]. In this study the women were asked to rate the pain they had on their backs without having uterine contractions.
The scale developed by Dencker et al. [29] in Sweden in 2010 has four sub-scales and 22 items to measure women’s labor experiences from different dimensions. The own capacity sub-scale assesses women’s pain as well as their feelings and sense of personal control. The professional support sub-scale assesses midwifery care and information. The perceived safety/memories sub-scale includes questions about mothers’ feelings of safety and labor-related memories. Participation in the decisions sub-scale includes questions about women’s participation in decisions such as movements during labor, labor position, and elimination of labor pain. While the first 19 items of the scale are rated on a 4-point Likert scale, the last three items are assessed using VAS. The first 19 items in CEQ are scored between 1 and 4, including responses I strongly agree = 1, I agree = 2, I partly agree = 3, and I strongly disagree = 4. Scores in VAS are categorized as 0–40 = 1, 41–60 = 2, 61–80 = 3, 81–100 = 4. Items 3, 5, 8, 9 and 20 include negative statements, so they are scored reversely. Higher scores indicate better labor experiences of the mother. The scale was adapted to Turkish society and its reliability and validity were assessed by Mamuk et al. [38]. The Turkish version of the scale was reported to have Cronbach’s alpha of 0.76.
This form was developed by the researchers to determine satisfaction with intradermal injections and opinions about effectiveness of these injections. The form has six questions. The responses to the items are: Yes, No or undecided. These questions are: “Were you satisfied with Intradermal injections at labor?”, “Did Intradermal injections reduce your lower back pain at labor?”, “Did intradermal injections increase your resistance to pain at labor?”, “Was the intradermal injections at labor a good experience for you?”, “Would you requesting application of the same technique at your next labor?”, “Would you recommend intradermal injections to another pregnant woman?”.
Study data were analyzed using SPSS (Statistical Package for Social Sciences) for Windows 21.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics including frequency, median, minimum, maximum, mean, and standard deviation were used in the analysis of the data. Conformity to normal distribution was analyzed by the Kolmogorov-Smirnov test. One-way ANOVA, Chi-square test, independent groups t-test and Kruskal Wallis - H test were used to compare the groups. The Tukey Test was used to determine which group caused the difference in more than one group. The statistics were analyzed with a 95% confidence interval and the significance was tested with the determined alpha value of 0.05.
In the present study, descriptive characteristics of pregnant women and the
comparison of these characteristics according to groups are shown in Table 1.
Groups were found to be similar terms of age, education, body mass index (BMI),
number of pregnancies, parity, gestational week, frequency of receiving prenatal
care, newborn weight, and time from injections to labor (p
| Obstetric characteristics | Sterile water group (n: 30) | Saline group (n: 30) | Control group (n: 60) | F | p |
|---|---|---|---|---|---|
| Mean |
Mean |
Mean | |||
| Age (year) | 25.04 |
25.46 |
26.05 |
0.312 | 0.732 |
| Duration of education (year) | 6.36 |
5.53 |
6.46 |
0.758 | 0.471 |
| BMI (kg/m |
23.97 |
24.44 |
24.09 |
0.099 | 0.910 |
| BMI during Pregnancy (kg/m |
28.64 |
29.32 |
29.11 |
0.224 | 0.800 |
| Number of pregnancies | 1.90 |
2.40 |
2.00 |
1.199 | 0.305 |
| Number of labor* | 0.63 |
0.90 |
0.66 |
0.842 | 0.434 |
| Gestational week | 39.10 |
39.50 |
39.30 |
0.752 | 0.474 |
| Frequency of prenatal care | 10.20 |
10.60 |
10.55 |
0.056 | 0.946 |
| Newborn weight (gr) | 3217.5 |
3162.0 |
3234.3 |
0.333 | 0.718 |
| APGAR score (1st min) | 8.76 |
8.46 |
8.78 |
2.027 | 0.136 |
| Time from injections to labor (min) | 173.66 |
226.40 |
245.38 |
2.192 | 0.116 |
*Women who had not given birth before were not included. F = One way ANOVA test.
APGAR, Score of appearance, pulse, grimace, activity and respiration of newborn.
Table 2 shows the distribution of mean VAS scores by the groups. According to
one-way variance analysis for independent groups, there was no difference in mean
VAS scores before injections between the groups, but there was a significant
difference in mean VAS scores in the 10th, 30th, 60th and 90th minutes after
injections in favor of the sterile water group (p
| VAS administration time | Sterile water group (n: 30) | Saline group (n: 30) | Control group (n: 60) | Test value | p | diff |
|---|---|---|---|---|---|---|
| Mean |
Mean |
Mean | ||||
| Before injections | 7.54 |
7.51 |
7.77 |
F = 1.383 | 0.255 | |
| At the time of injections | 9.01 |
7.02 |
- | t = 4.575 | 0.000* | |
| 10th minutes after injections | 4.81 |
6.68 |
7.85 |
F = 56.955 | 0.000* | c |
| c | ||||||
| 30th minutes after injections | 5.05 |
6.98 |
8.24 |
F = 48.097 | 0.000* | c |
| c | ||||||
| 60th minutes after injections | 5.42 |
7.61 |
8.60 |
F = 46.180 | 0.000* | c |
| c | ||||||
| 90th minutes after injections | 5.60 |
7.98 |
8.80 |
F = 43.294 | 0.000* | c |
| c | ||||||
| 120th minutes after injections | 5.50 |
8.19 |
8.92 |
KW = 24.05 | 0.000* | c |
| c |
F = One-Way ANOVA Test, t = Student t Test, KW = Kruskal Wallis - H
Test, VAS = Visual Analogue Scale, a = Sterile water group, b = Saline group, c =
Control group, *p
Table 3 reveals a comparison of mean scores for CEQ and its subscales between
the groups. One-way variance analysis showed no significant difference in mean
scores for the own capacity and perceived safety subscales (p
| The Childbirth Experience Questionnaire | Sterile water group (n: 30) | Saline group (n: 30) | Control group (n: 60) | F | p |
|---|---|---|---|---|---|
| Subscales | Mean |
Mean |
Mean | ||
| Own capacity | 19.90 |
19.26 |
18.08 |
1.589 | 0.209 |
| Professional support | 16.23 |
16.06 |
14.11 |
5.079 | 0.008*; c |
| Perceived safety | 18.70 |
18.13 |
16.96 |
2.620 | 0.077 |
| Participation | 8.20 |
7.23 |
6.36 |
5.164 | 0.007*; c |
| CEQ total | 63.03 |
60.70 |
55.53 |
4.876 | 0.009*; c |
F = One-Way ANOVA Test, a = Sterile water group, b = Saline group, c = Control
group, *p
As presented in Table 4, opinions of the sterile water group and the isotonic
(saline) group about intradermal injections were compared by using Chi-square
test and a significant difference was found between the groups (p
| Characteristics | Sterile water group (n: 30) | Saline group (n: 30) | p | ||
|---|---|---|---|---|---|
| N (%) | N (%) | ||||
| Were you satisfied with Intradermal injections at labor ? | |||||
| Yes | 26 (86.7) | 15 (50.0) | 11.819 | 0.001* | |
| No | 4 (13.3) | 15 (50.0) | |||
| Did Intradermal injections reduce your lower back pain at labor ? | |||||
| Yes | 28 (93.3) | 15 (50.0) | 15.256 | 0.000* | |
| No | 2 (6.7) | 15 (50.0) | |||
| Did intradermal injections increase your resistance to pain at labor ? | |||||
| Yes | 25 (83.3) | 12 (40.0) | 10.253 | 0.001* | |
| No | 5 (16.7) | 18 (60.0) | |||
| Was the intradermal injections at labor a good experience for you? | |||||
| Yes | 22 (73.3) | 11 (36.7) | 6.734 | 0.009* | |
| No | 8 (26.7) | 19 (63.3) | |||
| Would you requesting application of the same technique at your next labor? | |||||
| Yes | 24 (80.0) | 15 (50.0) | 4.689 | 0.015* | |
| No | 6 (20.0) | 15 (50.0) | |||
| Would you recommend intradermal injections to another pregnant woman? | |||||
| Yes | 27 (90.0) | 19 (63.3) | 4.565 | 0.009* | |
| No | 3 (10.0) | 11 (36.7) | |||
This randomized-controlled study that included women who experienced low-back pain during labor found that pregnant women who were administered sterile water injection (SWI) demonstrated a decrease in their low-back pain scores until the 120th minute after the injection; mothers were highly satisfied with the method; and they had a more positive labor experience. The study groups were similar in terms of the characteristics that are considered to affect labor pain such as age, duration of education, BMI, gestational week, number of labor, frequency of receiving antenatal care, and newborn weight. Besides, the duration from the injection to the labor and APGAR mean scores (Score of appearance, pulse, grimace, activity and respiration of newborn) were similar between the groups, which indicated that the injections did not affect the natural course of labor. These findings are in line with the literature [4, 13, 14, 15, 16, 22].
Severe back pain that could accompany together with or independently from uterine contractions could cause pregnant women to experience fatigue, anxiety, and stress and thus affect the course of labor negatively. Therefore, back pain needs to be controlled [1, 22, 25]. The literature includes several studies showing that intradermal or subcutaneous sterile water injection is effective in relieving low-back pain. A multi-centered randomized-controlled study on the issue reported a 30–50% decrease in low-back pain of pregnant women who were administered sterile water injection until the 90th minute following injection [22]. Two systematic reviews also reported that sterile water injection had a strong analgesic effect in eliminating low-back pain during labor and it was concluded that it should be used in labor rooms [10, 28]. This study also found that pregnant women who were administered SWI had a decrease in their low-back pain until the 120th minute following injection compared to the other two groups, indicating its effectiveness in line with the literature.
Pregnant women’s acceptance of the method to be used for pain and having positive labor experiences are as important as controlling pain during labor [39, 40]. Except for the study conducted by Labrecque et al. [26], the literature includes findings similar to the present study, indicating satisfaction with SWI [14, 17, 22]. Labrecque et al. [26] concluded that low satisfaction despite the effects on pain control could be associated with the temporary pain felt during injections.
Labor is a multidimensional experience that affects women not only physically but also psycho-socially, and it is affected by many factors [40, 41]. Labor experience could be positively affected by women’s feeling of safety, maintenance of control, perceived level of pain, benefitting from intrapartum analgesia, being informed, professional support received, support of relatives, and participation in decision-making [41, 42, 43, 44]. Therefore, unlike the related literature, this study included hypotheses to determine the effect of the technique on the labor experience as well as the satisfaction of pregnant women with SWI using a standard measurement tool. The mean score of CEQ, which was used to determine the labor experience of women in the study, was found to be significantly higher in favor of the SWI group, indicating that the practice had a positive effect on the labor experience of women. The same group of pregnant women were more satisfied with the injection, which strengthens the conclusion that sterile water injection affects women’s labor experiences positively. Like the present study, the related literature also indicates that some non-pharmacological pain control methods also improve women’s labor experiences. For instance, the study conducted by Kaçar and Keser [45] reported that pregnant women who received massage had a more positive labor experience in comparison to pregnant women who did not. Werner et al. [46] also reported that hypnosis improved the labor experience. In their systemic review, Thomson et al. [47] concluded that non-pharmacological methods might not always be effective in reducing pain or facilitating labor, yet they could increase the adjustment and coping capacity of pregnant women. Another study that compared pharmacological and non-pharmacological pain control methods indicated that labor experience and satisfaction associated not only with the level of pain experienced, but also with the care provided to the mother [48]. As stated by the World Health Organization, all women have the right to have a positive labor experience. The quality of care provided can be measured by the obstetric outcomes [40]. However, how women evaluate the labor they have experienced and the determination of factors that contribute to a positive labor experience should be important for care givers [49]. In this regard, determination of the positive effect of intradermal sterile water injection in this study on mothers’ labor experience is considered to be very important.
It can be concluded that intradermal sterile water injections can decrease perceived back pain in labor and have a positive effect on labor experiences and that women can be satisfied with them. Based on these results, it is recommended to assess low back pain at certain intervals during labor and to provide women who have low back pain with ISW option. In addition, multicenter studies are recommended to evaluate the effect of intradermal sterile water injection on the labor experience of women.
In the literature, there are studies reflecting the sterile water injections can relieve back pain during labor. Contrary to other studies, this is the first study to examining the effect of intradermal sterile water injection on labor experiences of women who experience low-back pain during labor. On the other hand the results of this study cannot be generalized to all pregnant women since it was a single-center study and had a small sample size.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Conception and design—RM, NHŞ; Data collection—RM; Data analysis—RM; Manuscript writing—RM, NHŞ; Critical revisions for important intellectual content—RM, NHŞ. All authors read and approved the final manuscript.
Ethics committee approval was obtained from the Medipol University (approval number: 2014/232). A written permission was taken from Bağcılar Training and Research Hospital Directorate (approval number: 95273397/770) so that the study could be performed. In accordance with Helsinki Declaration, oral and written informed consent was obtained from all the participants.
This article is a product of a PhD thesis completed in the İstanbul University Institute of Health Sciences. Authors gratefully thanks Bağcılar Education and Research Hospital administrators and staffs who work in the delivery clinics, as well as women who are participating in the study.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.