




1 Faculty of Pharmacy, King Abdulaziz University, 21589 Jeddah, Saudi Arabia
2 Department of Pharmacy Practice, Faculty of Pharmacy, King Abdulaziz University, 21589 Jeddah, Saudi Arabia
3 Department of Pharmacology and Toxicology, Faculty of Pharmacy, King Abdulaziz University, 21589 Jeddah, Saudi Arabia
Abstract
Background: The aim of this study is to assess female college students’ behavior in Jeddah, Saudi Arabia toward menstrual pain (dysmenorrhea) and their knowledge regarding the proper use of over-the-counter pain medications. Methods: A cross-sectional survey-based study that assessed 300 healthy females. The major points in the questionnaire were symptoms experienced during menstruation, pharmacological and nonpharmacological pain management, effects of participants’ menstrual periods on daily activity, locations of pain, menstrual pain severity, and exercise activity. Results: From the 300 participants who participated in the survey, pain was experienced by 256 (85%) of participants. Among those 256, 46.1% felt the pain was severe. The most reported pain was in abdomen (89.2%) and back (70%). Most participants (81.2%) experienced pain during the first 3 days. As for the management method, 69.9% managed their pain by nonpharmacological and 66.8% by pharmacological agents. Approximately 43% reported to practice physical activity during menstruation. Conclusions: Dysmenorrhea is common among female college students and affects their daily activity. Many students are suffering from menstrual pain and treating it with different methods. Most participants are not aware of the proper usage of pain killers. Pharmacists and other health care personnel can instruct on how to use analgesics during menstruation.
Keywords
- dysmenorrhea
- menstrual symptoms
- saudi
- college student
Dysmenorrhea is the most common etiology of pelvic pain which characterized by uterine painful cramps. It is the main cause of gynecological morbidity in female reproductive age worldwide. The burden of dysmenorrhea can extend beyond females to affect society productivity. Since mild dysmenorrhea is recognized as a normal part of the menstruation cycle and is quite tolerable by females, it has low reporting rate and majority of the female do not seek any medical help. On the other hand, some females have severe dysmenorrhea that affect their daily activity leading them to miss work and school days. This restriction in the daily activity may impact females’ live leading to lower their academic performance, low sleep quality and might cause depression and anxiety. Worldwide prevalence of dysmenorrhea in reproductive age female estimated to be ranges from 45% to 93%. With majority reported in the adolescents [1].
There are two types of dysmenorrhea: primary dysmenorrhea and secondary dysmenorrhea. Primary dysmenorrhea symptoms usually accompany within the start of menstrual cycle and symptoms include lower abdominal cramping as well as nausea, vomiting and headache in absence of pathologic disease. Pain usually decreases with older age. Secondary dysmenorrhea, however, is usually associated with chronic pelvic pain and midcycle pain and it usually develops later in life. Endometriosis is one of the most common causes of secondary dysmenorrhea [2].
Numerous articles discuss the impact of menstrual suffering on college students’ fulfilment, attendance, and degrees [3, 4, 5, 6, 7]. Adolescent females tend to lack appropriate and sufficient information about menstrual problems and how to manage them. They usually think that dysmenorrhea is a physiologic condition that does not need any medical consultation [8]. They also tend to depend on information gathered from family or friends and the internet to manage the pain [9]. There is a huge debate on the most reliable and effective treatment for menstrual pain [10]. Menstrual disorders may disturb the lives of adolescents and young women, and sometimes cause major problems that may lead to using medications or herbal products, such as chamomile or mint tea, that are of varying efficacy and safety [8, 9, 11, 12, 13]. Medications such as over-the-counter (OTC) and analgesics are often used in sub-or over-therapeutic doses [9, 11, 13].
Although menstrual pain can affect daily activities in young females and lead to the misuse of certain medications, there are limited data regarding menstrual pain management in college students in Saudi Arabia. The aim of this study is to assess female college students’ behavior in Saudi Arabia toward their menstrual pain and their knowledge regarding the proper use of OTC pain medications. Therefore, pharmacists and other health care personnel can give medical advice on how to use analgesics, including maximum doses, frequency of doses, and beneficial effects of physical activity (PA) on menstrual pain.
We conducted a cross-sectional survey-based study. The survey was completed in Arabic by 300 healthy females from both the medical campus and the nonmedical campus at King Abdulaziz University, Jeddah, located in the Western region of Saudi Arabia, between September 2018 and December 2018. Only female participants who experienced menstrual pain were included in the final analysis. Ethical approval was obtained before distribution of the survey application number PH-1442-40 based on the Declaration of Helsinki.
The inclusion criteria included all female college students of child-bearing age (18–50 years old). We excluded any female younger than 18 years of age, non-Arabic speakers, anyone without a menstrual period, and those who rejected participation in the study. We eliminated female if they acknowledged that they never experienced pain during menstruation. The respondents were informed about the aim of the project and were willing to complete the questionnaire. Oral consent was given by the participants. The survey was interview-based, took 10–15 minutes, and participants were anonymized with code numbers.
The 14 Arabic questions included basic demographic information such as age and marital status. The questionnaire also asked about respondents’ healthcare-related education, symptoms experienced during menstruation, pharmacological pain management (dosage, duration, and adverse effects), nonpharmacological pain management (herbal and heat therapy), effects of participants’ menstrual periods on daily activity, locations of pain, menstrual pain severity, and exercise activity. Exercise activates included workout/cardio, swimming, waking/Jogging, martial arts. A visual scale of 0–10 was used to measure the severity of menstrual pain. Scores on the scale were categorized as mild (1–3), moderate (4–6), or severe (7–10). The survey questions were validated by 10 experts of clinical pharmacists who were also excluded from study participation. The study was conducted after obtaining consent from the King Abdulaziz University, Faculty of Pharmacy. Three researchers collected and coded the data and entered them in an Excel spreadsheet. Statistical analysis was performed using SPSS software. Descriptive statistics were used to summarize the data. Data were analyzed with SPSS software, version 24 (IBM, Chicago, IL, USA)
The survey was distributed to 300 women with 100% response rate. However, only 256 experienced pain during menstruation and were completed the survey. The female with pain free period were eliminated from the study. Most participants were single women between 18 and 25 years of age. Out of these 256 women who experienced the pain during menstruation, 114 (44.5%) were in nonmedical fields and 142 (55.5%) majored in medical fields (Table 1). Two hundred fifty-six women (85%) experienced pain during menstruation and were included in the final analysis. One hundred sixty-nine (66%) respondents experienced that pain every month (Table 2). Among participants, 118 (46.1%) felt the pain was severe, ranging from 7–10 on the pain scale. However, only 40 participants (15.6%) had visited the hospital in the previous year due to menstrual pain. Out of them, 25 visited the hospital 1–5 times during the previous year. Only 2 participants (5%) went 12 times (i.e., every month during the previous year). Moreover, 177 (69.1%) women claimed that the pain affected their daily activity. The most reported pain was in abdomen 232 (90.6%); back 182 (70%); head 44 (16.9%); thighs 87 (33.5%); legs 7 (2.7%); and breast area 6 (2.3%) (Fig. 1). Most participants (211, 81.2%) experienced pain during the first 3 days of menstruation; however, only (24, 9.3%) women experienced it through the fifth day of menstruation (Fig. 2). Tables 3,4 summarizes how the women usually managed their pain by pharmacological (OTC medications) or nonpharmacological methods (using herbal products, applying heat, or both). Regarding medication use, 73 respondents (28.5%) used non-steroids anti-inflammatory drugs (NSAIDs), 91 (35.5%) used acetaminophen, and only 7 women (2.7%) used hyoscine. Regarding the use of NSAIDs, 41 women (56.2%) were taking NSAIDS with food, 7 (9.6%) were taking them on an empty stomach, and 25 (34.2%) said they were taking NSAIDs without regard to food. Regarding NSAIDs dose, 27 (36.9%) thought that they knew the maximum doses; however, 21 (77.8%) stated incorrect dose. Moreover, 22 respondents (30.1%) claimed that they knew the contraindications of NSAIDs, but most of them 14 (63.6%) were incorrect. Among those who took acetaminophen, 26 women (28.6%) stated that they knew the maximum dose of the medication, but 20 (76.9%) of them stated incorrect doses.
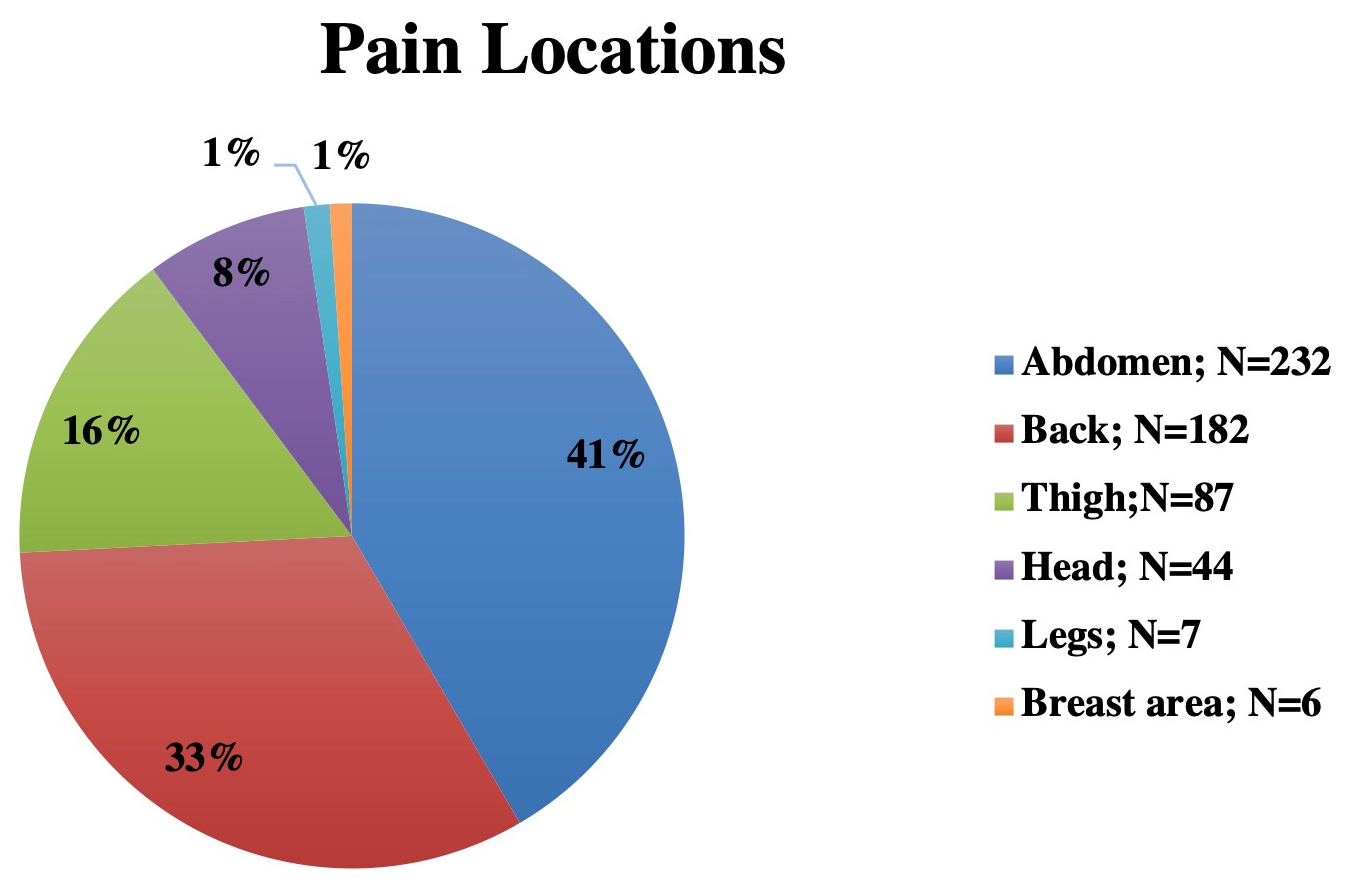 Fig. 1.
Fig. 1.Pain location during menstruation.
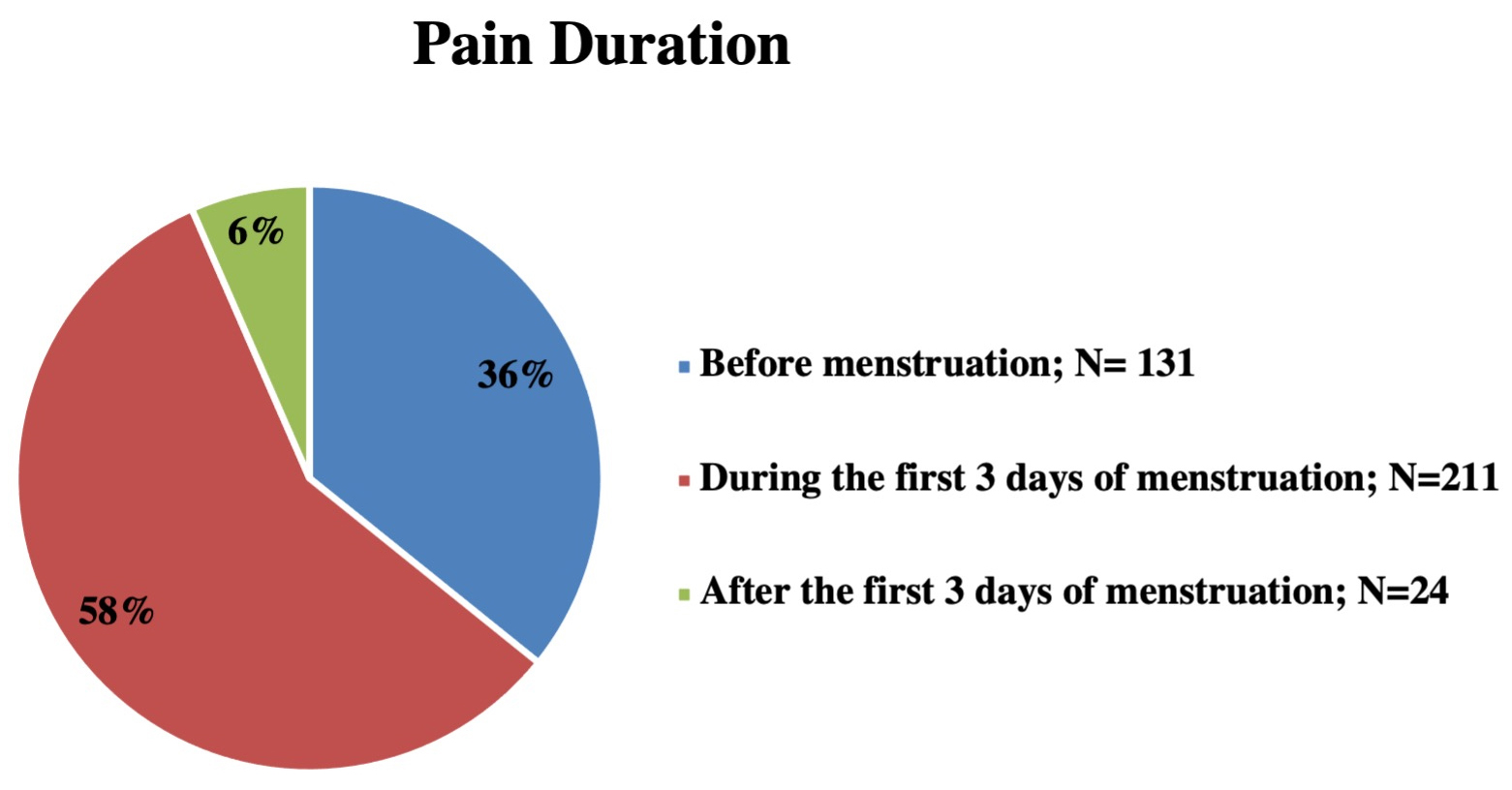 Fig. 2.
Fig. 2.Pain duration during menstruation cycle.
| Demographics | N = 256 | |
|---|---|---|
| Age | N (%) | |
| 18–25 years | 224 (87.5%) | |
| 26–30 years | 16 (6.3%) | |
| 31–40 years | 16 (6.3%) | |
| Social status | N (%) | |
| Married | 37 (14.5%) | |
| Single | 213 (83.2%) | |
| Separated | 6 (2.34%) | |
| Field of study | N (%) | |
| Medical | 142 (55.5%) | |
| Non-medical | 114 (44.5%) | |
N, number; %, percentage.
| Characteristics | N = 256 | |
|---|---|---|
| Frequency of pain | N (%) | |
| Every period | 169 (66%) | |
| Every 2 periods | 54 (21.1%) | |
| Less than that | 33 (12.9%) | |
| Pain severity | N (%) | |
| Mild | 32 (12.5%) | |
| Moderate | 106 (41.4%) | |
| Severe | 118 (46.1%) | |
| Pain affect the daily activity | 177 (69.1%) | |
N, number; %, percentage.
| Modality | N = 256 | |
|---|---|---|
| NSAIDs use | 73 (28.5%) | |
| NSAIDs frequency (N = 73) | ||
| Once daily | 43 (58.9%) | |
| Twice daily | 21 (28.8%) | |
| Three times daily | 9 (12.3%) | |
| NSAIDs administration (N = 73) | N (%) | |
| With food | 41 (56.2%) | |
| On empty stomach | 7 (9.6%) | |
| Without regards to food | 25 (34.2%) | |
| NSAIDs maximum dose (N = 73) | N (%) | |
| Claimed knowing the maximum dose | 27 (37.0%) | |
| Stated the correct maximum dose | 6 (8.2%) | |
| NSAIDs contraindications (N = 73) | N (%) | |
| Claimed knowing the contraindications | 22(30.1%) | |
| Stated the correct contraindications | 8 (11.0%) | |
| Acetaminophen use | 91 (35.5%) | |
| Acetaminophen frequency (N = 91) | ||
| Once daily | 49 (53.8%) | |
| Twice daily | 31 (34.1%) | |
| More than twice | 11 (12.1%) | |
| Acetaminophen maximum dose (N = 91) | N (%) | |
| Claimed knowing the maximum dose | 26 (28.6%) | |
| Stated the correct maximum dose | 6 (6.6%) | |
N, Number; %, percentages; NSAIDs, Non-steroidal Anti-inflammatory Drug.
| Modalities | N = 256 | |
|---|---|---|
| Non-pharmacological modalities | 179 (69.9%) | |
| Herbal | 64 (25.0%) | |
| Heat | 63 (24.6%) | |
| Both | 52 (20.3%) | |
| Satisfaction to non-pharmacological modalities (N = 179) | 162 (90.5%) | |
| Physical activity* | 108 (42.2%) | |
| Cardio | 8 (3.1%) | |
| Lifting | 31 (12.1%) | |
| Walking | 52 (20.3%) | |
| Another physical activity | 55 (21.5%) | |
| Frequency (N = 108) | N (%) | |
| 5–7 times weekly | 38 (35.2%) | |
| 2–4 times weekly | 36 (33.3%) | |
| Once weekly or less | 34 (31.5%) | |
| Satisfaction to physical activity (N = 108) | 75 (69.4%) | |
N, Number; %, percentages.
*, Some of the physical activities were practiced simultaneously by women.
Regarding the nonpharmacological methods, 179 (69.9%) women used both herbal drinks and heat application, whereas 63 (24.6%) applied heat only, and 64 (25.0%) used herbal products only. The most common herbal teas used were cinnamon in 56 women followed by ginger in 29 women and mint in 27 women, whereas 38 women acknowledged drinking mixed or any hot herbal tea available during to relieve their pain. One hundred sixty-two women (90.5%) felt that herbal products and heat helped in alleviating their menstrual pain. Simulations use of non-pharmacological and pharmacological modalities were acknowledged in 110 (43.0%) of the women. Regarding PA, 108 women (42.2%) claimed they were engaging in PA, most of them in the form of walking. As for PA frequency, 38 women (35.2%) said they practiced it 5–7 times weekly, 36 (33.3%) said they practiced 2–4 times weekly, and 34 (31.5%) said they practiced PA once a week or less. As a result, 75 women (69.4%) confirmed that practicing PA lowered the intensity of their pain. Only 21 women (8.2%) acknowledged that they were using contraception, while 235 (91.8%) denied any contraceptive use.
This study showed that period pain is a major issue among the young adult population in Saudi Arabia that requires significant attention. We focused on assessing how the young female population manages its pain and how dysmenorrhea affects daily life in Saudi Arabia using a cross-sectional survey. In this study, the total prevalence of menstrual pain was 85.33%, which is similar to the findings of previous studies [5, 6, 14]. In those studies, the prevalence of menstrual pain was 71.7%, 79%, and 84.1%, respectively.
In general, the pain and inflammation that happened during menstrual hormonal changes leads to the release of prostaglandins, which have a role in triggering muscle contractions in the uterus. In this study, most women stated that their pain was severe, with 46.1% of the study subjects rating it as 7 out of 10 or above. Previous study found that most Lebanese students (60.3%) evaluated their pain as severe [4]. The difference in the degree of pain severity may be related to cultural and ethnic attitudes toward pain perception and variability in pain thresholds [15]. The study found a low rate of contraception use in the sample and only 8.2% acknowledged that they were using contraception. This low rate maybe due to the fact that about 83% of the sample are singles, and culturally in Saudi Arabia only married people are sexually active and may use contraception regularly.
In this study, 69% of participants stated that the pain affected daily activity. This point was with statistically significant difference with a previous study that found reductions of women’s quality of life during the menstrual period (26%) [16]. In this study, most participants (89.2%) experienced menstrual pain in the abdomen and 70% in the back. These findings are also similar to previous study that found most participant pain was in the lower abdomen (36.6%) and lumbar region (33.9%), representing the entire lower abdominal region [17].
Women in Saudi Arabia use various modalities to relieve their pain through pharmacological and nonpharmacological methods. We found that 66.7% used medication for pain management, which is similar to Cakir et al.’s results [10]. They found 50% of women used medication for their pain. This might be due to the medications’ ability to rapidly control the release of prostaglandin and inflammatory biomarkers that are responsible for this pain. Seventy-three of the respondents (28.5%) in this survey reported using NSAIDs for pain relief. This was an interesting finding. Comparable results were acquired by Oman [18]. We found 91 (35.5%) of the participants used acetaminophen, which was the most common analgesic used for the management of dysmenorrhea as reported in previous studies [19]. Acetaminophen has a preferable safety profile compared to NSAIDs for managing painful menstruation, especially in patients who are at higher risk for peptic ulcers [20]. The majority of participants in this study admitted using nonpharmacological pain management techniques such as heat pads and herbal drinks. Among participants who used nonpharmacological methods, 45.3% applied heat only, 44.9% used herbal products only, and 69.9% preferred to use both herbal remedies and heat at the same time. A similar study found that heat pads were used in 36.5% of their participants and sleep in 31.0% of the participants [17].
There has been an increase in the overuse of OTC pain medications. This has prompted Food and Drug Administration (FDA) to instruct pharmacological companies to clearly label the active ingredients on bottles and indicate the adverse reactions likely to be caused by the medicines. Therefore, pharmacists should also take center stage to ensure that they take every possible opportunity to educate and assist patients in the proper use of OTC analgesics. Acetaminophen is hepatoxic at doses more than 4 g/day or with chronic use. Moreover, NSAIDs should be taken with food to avoid gastrointestinal upsets. They are contraindicated in specific cases such as for patients who take warfarin or have renal or hepatic issues [21]. Health awareness campaigns should be undertaken regularly in middle and high schools to increase knowledge and awareness. Basic information regarding dysmenorrhea and proper management may also be included as part of school subjects in high school.
This study has several strengths. The response rate was complete (100%). We specifically targeted college students with both medical and nonmedical majors, and the survey questions were tailored according to our community practice. The study also has some limitations. It has across-sectional design, so its results cannot be generalized. The sample size was not very large and was from one city in the western region of Saudi Arabia. Despite these limitations, this study showed the need to increase knowledge among women regarding dysmenorrhea and pain management methods. Larger multicenter studies are still needed to compare effects between different types of PA as well as various herbal products used to alleviate dysmenorrheal pain.
Dysmenorrhea is common among female students and can affect their daily activity. Most students are not aware of the proper usage of pain killers. Therefore, pharmacists and other health care personnel can give medical advice on how to use analgesics, including the maximum doses, frequency of dosing, and the beneficial effects of PA on menstrual pain.
All data and materials will be available upon request.
SA, KE and MA designed the study. RA, LH, ML collected the data. SA, MN and KE double-checked the data collection. RA and MN managed and analyzed the data, and all authors helped interpret it. RA drafted the manuscript and all co-authors contributed to its revision and final approval.
All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Research Ethics Committee of King Abdulaziz University, faculty of Pharmacy (PH-1442-40).
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.