

 , Vedi Loue 1, Virginie Angoi 1, Sophia Akinloye 1, Fatimata Ampoh 1
, Vedi Loue 1, Virginie Angoi 1, Sophia Akinloye 1, Fatimata Ampoh 11 Department of Gynecology and Obstetrics, University Hospital of Cocody, 00225 Abidjan, Cote d’Ivoire
Abstract
Background: Uterine fibroids are the most common form of benign uterine
tumors. African women of reproductive age usually present late with large and
numerous uterine fibroids. Conservative surgical treatment requires ways to
reduce intraoperative bleeding. This study attempts to describe innovative
methods in the efficient management of fibroids in low-and middle incomes
countries. We demonstrate the efficiency of the uterine tourniquet during
abdominal polymyomectomy in intraoperative bleeding reduction despite removal of
numerous myomas. Methods: A prospective, descriptive and analytical
review was conducted on 92 patients who underwent open myomectomy in the
gynecology department of the university hospital of Cocody (Côte d’Ivoire)
over 3 years (2019 to 2020). Intraoperative surgical steps include placing a
uterine tourniquet before removal of the myomas. The variations in mean
hemoglobin levels before and after myomectomies were compared. The significance
level was set at 5% (p
Keywords
- uterine myomas
- tourniquet
- abdominal myomectomy
- blood losses
- hemoglobin level
Uterine myomas are the most common benign disease of female genital tract, affecting 20 to 25% black women of reproductive age. Management of fibroids is challenging in low- and middle-income countries (LMICs) due to denial of the disease, late care due to socio-cultural beliefs, pre-conceived ideas concerning surgical treatment, multiple unsuccessful treatment attempts with traditional remedies, low literacy rates and financial constraints [1, 2]. It is frequently diagnosed in women desiring conception. In women requesting fertility preservation surgery, a myomectomy can be done by laparotomy, laparoscopy or hysteroscopy depending on the size, site and type of fibroid [3]. In our country, abdominal myomectomies are most often performed because of unavailability of laparoscopy or hysteroscopy [3]. Myomectomies however are risky procedures and can result in serious complications, such as, excessive intraoperative bleeding. It is therefore essential to implement a procedure to reduce blood loss during surgery, particularly in the African context where blood products are scarce unavailable [1, 2, 3]. The objective of these surgical procedures was to significantly reduce intraoperative blood loss [4]. The goal of this study was to examine the efficiency of uterine tourniquets in reducing blood loss during open myomectomies in a LMIC, where blood transfusion is unavailable.
A prospective descriptive and analytic study conducted was in the department of Obstetrics and Gynecology of the University Hospital of Cocody (Côte d’Ivoire) over 3 years (January 2019 to December 2021). It included 92 women of reproductive age who underwent an open myomectomy for uterine fibroids of any size, with initial placement of a urinary catheter as uterine tourniquet. Abdominal and endo-vaginal ultrasounds were used to map the uterine myomas (location, size and number). Magnetic resonance imaging (MRI) were requested but not done because our patients and their families had a limited income, thus unable to afford this relatively expensive examination income.
After laparotomy via the Pfannenstiel or Maylard approach, intraoperative evaluation of uterus, size and number of fibroids to enucleated was done. A securely tied uterine tourniquet was placed at the junction of the uterine body and isthmus before myoma enucleation (Fig. 1).
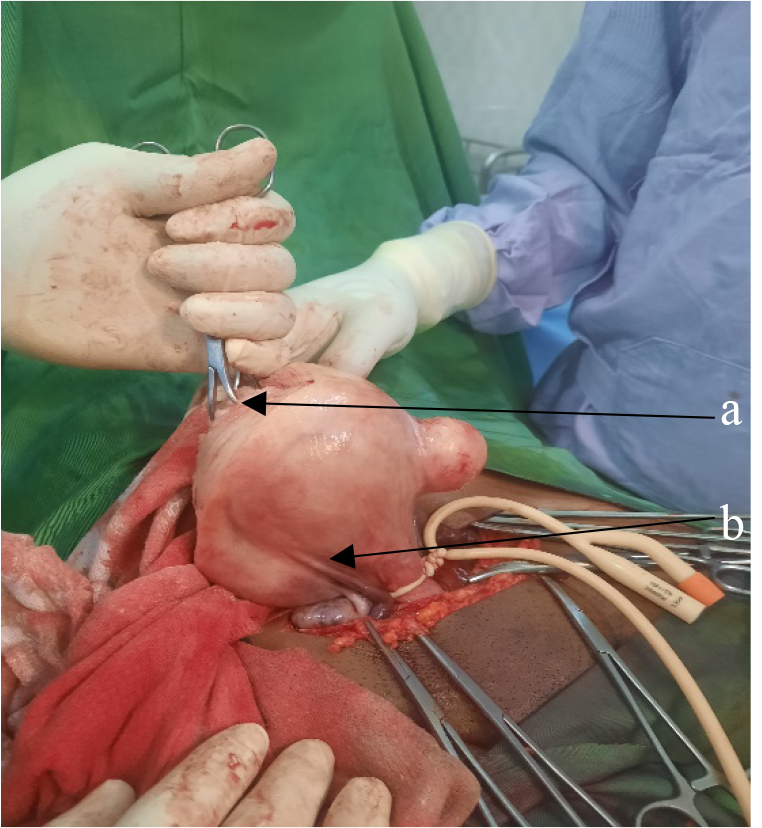 Fig. 1.
Fig. 1.Intraoperative view of uterine tourniquet placement. (a) Polymyomatous uterus. (b) Foley catheter tied at the uterine isthmus.
The operating time with the uterine tourniquet was 90 minutes. The tourniquet was discontinued as soon as the anatomical uterine structures appeared blue.
The tourniquet was re-applied 15 minutes later if continuation of surgery was
necessary. After enucleation of all fibroids, simple or “U” uterine stitches were
performed. Following removal of the tourniquet, hemostasis was checked and
established with additional safety stitches as necessary. A hemoglobin level was
checked before, and 48 hours after the surgical procedure to assess blood loss.
Sociodemographic and clinical parameters, hemoglobin level, postoperative course,
duration of hospitalization and need for blood transfusion were studied.
Statistical analyze was performed using Epi Info 3.5.1 2008 software (centers for
disease control and prevention (CDC), Atlanta, GA, USA) and Fischer
exact test for comparison of average hemoglobin levels with a significance level
of 5% (t
The average age was 38.5 years, with extremes of 23 and 48 years. Nulliparous women represented 39%. The main reason for consultation was menstrual cycle disorders (67.4%). Table 1 shows the reasons for consultation.
| Variables | Number (n) | % | |
|---|---|---|---|
| Reasons for consultation | n | % | |
| Cycle disorders (metrorrhagia, menorrhagia) | 62 | 67.4 | |
| Pelvic pain | 24 | 26 | |
| Pelvic mass and heaviness | 23 | 25 | |
| Infertility | 7 | 17.9 | |
| Constipation and pollakiuria | 9 | 9.8 | |
| Hydrorrhea | 9 | 9.8 | |
| Surgical features | n | min–max | |
| Mean number of fibroids (n) | 10 | 3–30 | |
| Average size of fibroids (cm) | 8 | 5–30 | |
| Average duration of intervention (min) | 155 | 55–180 | |
| Average blood loss (mls) | 250 | ||
The intraoperative mean uterine size was 30 cm with the smallest and largest being 16 and 35 cm, respectively. The uteri varied in size between: 20–28 cm (44%), 28–30 cm (35%) and 16–20 cm (21%). The number of enucleated myomas, duration of surgical procedure, and blood loss are summarized in Table 1.
The postoperative evaluation of hemoglobin levels, and the number of transfused
patients is summarized in Table 1. There was no significant variation between the
mean hemoglobin levels before and after surgery (t
The average of hemoglobin level varied from 12.78 g/dL before surgery to 11.19
g/dL after with no significant difference (t
Uterine myomas are the most common benign disease of the female genital tract, particularly affecting of black women [1, 2, 3, 4]. No medical treatment has proven to be effective so surgical management for symptomatic uterine fibroids is the treatment of choice [4]. Hysterectomy would eliminate the possibility of recurrence but this procedure is not readily accepted by women with a desire for pregnancy [3, 4]. Conservative treatment (myomectomy) is very often associated with a significant risk of bleeding that may be life-threatening [3, 4, 5, 6]. Nowadays there are several conservative surgical approaches that reduce intraoperative bleeding significantly [3]. Most of these procedures are not available in our countries despite the large fibroids observed in our patients.
It was therefore important to propose myomectomy techniques that prevent intraoperative hemorrhage [6].
One of these techniques has been used in our department for decades for
generally very large uterine fibroids (
On the other hand, some of our patients have expressed fear of the surgical procedure due to concern of uterine removal, complications of surgery, socio-cultural beliefs presenting uterine fibroids as a mystical issue [5, 6, 7].
These large uterine fibroids, present a risk of hemorrhage estimated at 6% during their removal especially in the case of open polymyectomy [5].
Reduction of intraoperative bleeding requires use of several drugs, such as,
gonadotrophin agonists, androgens and multiple inhibitors of steroidogenesis
(Danatrol) for reducing the volume of fibroids prior to surgery [6]. Surgical
primary ligation of the hypogastric arteries has even been proposed [7, 8]. Some
drugs have also shown effectiveness in reducing myomas size by 40–50%, for
instance, mifepristone (anti-progestogen), and raloxifene (selective estrogen
receptor modulator) [9]. However, progestin-based medical treatment has not shown
any effect on uterine myoma size. Preoperative embolization consists of bilateral
obliteration of the uterine arteries after selective catheterization. It is the
reference technique in developed countries, allows “bloodless surgery”, and can
be carried out only 3 hours before the operation [9, 10]. Preoperative
embolization allows obliteration of uterine arteries and significant reduction of
arterial blood flow that result in bloodless surgery [10, 11, 12]. Embolization
prevents necrosis from creating significant adhesions with neighboring organs and
causes cleavage planes to disappear [13]. The indications for preoperative
embolization are still poorly defined. However, it ought to be the preferred
procedure for fertility preservation, although it exposes the patient to risks of
ovarian alteration and adhesions with myomectomy. Moreover, histological studies
[6] show that embolization reduces perfusion of the myometrium around the
fibroid, a reduction that could compromise adequate uterine healing and increase
the risk of uterine rupture in the event of pregnancy. Embolization use is
relatively new in our country and still unavailable because it is very expensive.
In our country the evaluation of embolization, in definitive/selective
embolization of uterine fibroids was published only in 2019 [14]. Myomectomies by
conventional surgery after placing a tourniquet at the uterine isthmus allowed
bloodless removal of several myomas. In fact, there no variations in pre- and
postoperative of hemoglobin levels (t
This is a definite advantage because of the of transfusion products in our practice (4.3%). Indeed, ordered but undelivered transfusions are a health security problem in our country [5]. The uterine tourniquet technique allows reduction of both intraoperative hemorrhage, and transfusion needs during abdominal myomectomies better than use of misoprostol [15, 16, 17, 18], oxytocics [13], gonadotrophin releasing hormon (GnRH) agonists [10] and tranexamic acid [19, 20, 21]. The uterine tourniquet has also shown its superiority over bilateral primary ligation of hypogastric arteries, which is reserved for experienced surgeons [15].
Some authors systematically recommend this technique during abdominal myomectomies [19] as an alternative to arterial embolization in countries with limited resources [19, 20, 21]. Uterine ischemia is a risk with use of the uterine tourniquet, but it is not significant if the procedure lasts less than 90 minutes [22]. To reduce ischemia risk, when procedures are too long, it is necessary to remove, and reapply the tourniquet after at least 15 minutes [20, 21, 22].
A short average of hospital stay was observed in this study (3 days). The time of hospitalization was modified by the presence of a postoperative complication such as anemia, and a delay in return of bowel function. Other complications have been described in the literature [23] and the possibility of pregnancy after abdominal myomectomies [24, 25].
The uterine tourniquet significantly reduces intraoperative hemorrhage in abdominal myomectomies. It is readily available, simple to use and effective in reducing intraoperative bleeding. It could be an alternative to arterial embolization in low- and middle-income countries, and thus should be widely promoted.
The data that support the findings of this study are available from corresponding author but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of Dehi Boston Mian et al.
All authors (DBM, VL, VA, SA and FA) have contributed in extraction and drafting of the manuscript. DBM and VL have made the analysis of data, manuscript revision, design and revision, final statistical analysis. All authors read and approve this final manuscript.
We have obtained the approval (N 234554-CI/2020) of the Felix Houphouet Boigny University for the publication of this manuscript.
We acknowledge any support given which is not covered by any author contribution.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.