

1 Department of Obstetrics and Gynecology, Jinhua Municipal Central Hospital, 321000 Jinhua, Zhejiang, China
2 Department of Obstetrics and Gynecology, Wenzhou Central Hospital, 325100 Wenzhou, Zhejiang, China
3 Department of Obstetrics and Gynecology, Pujiang People's Hospital, 322200 Pujiang, Zhejiang, China
Abstract
Background: Adenomyosis is a gynecological benign lesion caused by the invasion of endometrium and stroma into normal myometrium. To further improve the treatment of adenomyosis, the objective of this study was to investigate the clinical effect of levonorgestrel-releasing intrauterine system, combined with gonadotropin-releasing hormone agonist (GnRH-a) drug-assisted focused ultrasound ablation, in the treatment of adenomyosis and its effect on phosphatidylinositol 3 kinase/phosphatase and tensin homolog (PI3K/PTEN) signal pathway. Methods: A study was conducted in subjects aged 28–54 years with adenomyosis, treated in our hospital. A total of 87 subjects were assigned to a control group (n = 41), which was given focused ultrasound ablation, and a study group (n = 46), which was given focused ultrasound ablation + GnRH-a + levonorgestrel-releasing intrauterine system, depending on the different treatment methods. The follow-up time was 12 months, and the treatment effect, adverse reaction, and PI3K/PTEN signal pathway related protein level were compared between the two groups. Results: After 12 months intervention, it was corroborated significant difference between focused ultrasound ablation group and the focused ultrasound ablation + GnRH-a + levonorgestrel group in uterine volume, visual analogue scale (VAS) score, pictorial blood loss assessment chart (PBAC) score, and serum cancer antigen 125 (CA125) levels. In terms of proteins level in the eutopic endometrial tissue, it was observed notably higher levels of PTEN and notably lower levels of protein kinase B (AKT) and p-AKT in the study group versus control group, 12 months after treatment. Conclusions: Levonorgestrel-releasing intrauterine system combined with GnRH-a drug-assisted focused ultrasound ablation is more effective in the treatment of adenomyosis, and its mechanism may be related to the regulation of the expression of molecules related to PI3K/PTEN signal pathway.
Keywords
- adenomyosis
- focused ultrasound ablation
- gonadotropin-releasing hormone agonist
- levonorgestrel-releasing intrauterine system
- PI3K/PTEN signal pathway
Adenomyosis is a gynecological benign lesion caused by the invasion of endometrium and stroma into normal myometrium, which is more common in women of childbearing age. It is characterized by enlarged uterus, excessive menstruation, and dysmenorrhea, which can affect women’s fertility [1, 2]. The prevalence rate of adenomyosis in infertile women under the age of 40 is about 20.0%, rising to 29.7% over the age of 40, and as high as 30% to 40% among women who use assisted reproductive technology [3]. Adenomyosis can be cured by total hysterectomy or subtotal hysterectomy, but it is not suitable for female patients with uterine preservation needs [4].
Focused ultrasound ablation is a non-invasive technique developed in recent years. It harnesses high penetration capability of ultrasound focus ultrasound unto a specific target under real-time imaging. This causes instantaneous high temperature, resulting in the necrosis of targeted tissue, and tissue ablation. Previous study has shown that focused ultrasound ablation can selectively ablate adenomyosis and relieve symptoms, such as dysmenorrhea and menorrhagia [5]. However, there are the following limitations: the boundary of the focus is not clear, the release of energy is not easy to control, there is the risk of recurrence, and the treatment effect is not very satisfactory. In addition to surgical treatment, drugs are also commonly used in the treatment of adenomyosis, including non-steroidal anti-inflammatory drugs, oral contraceptive, progesterone drugs, gonadotropin-releasing hormone agonist (GnRH-a), and mifepristone. Among them, GnRH-a inhibits estrogen secretion, thereby improving the clinical symptoms of patients. Levonorgestrel has a better effect on improving dysmenorrhea and menstrual volume [6, 7]. The specific pathogenesis of adenomyosis has not been fully understood yet.
Previous research has identified high expression of the carcinogenic gene DJ-1 in ectopic endometrial tissues of patients with adenomyosis, suggesting it may participate in the biological behavior of ectopic endometrial cells (including proliferation, invasion and migration) through phosphatidylinositol 3 kinase/protein kinase B (PI3K/AKT) signal pathway, which may contribute to the development and progression of adenomyosis [8]. A recent study has also found that phosphatase and tensin homolog (PTEN) has a certain regulatory effect on PI3K/AKT signal unblocking [9]. To further improve the treatment of adenomyosis, this study used a combined method to explore the efficacy of levonorgestrel-releasing intrauterine system, combined with GnRH-a drug-assisted focused ultrasound ablation in the treatment of adenomyosis, and analyze the possible mechanism.
This was a retrospective study, from October 2019 to October 2020. The control group received only focused ultrasound ablation intervention. The study group received focused ultrasound ablation + GnRH-a + levonorgestrel intervention. In this study, uterine volume, visual analogue scale (VAS) score, pictorial blood loss assessment chart (PBAC) score, and serum cancer antigen 125 (CA125) level and phosphatidylinositol 3 kinase/phosphatase and tensin homolog (PI3K/PTEN) protein levels in the eutopic endometrial tissue were evaluated at baseline and at three follow-up points. Four assessments were conducted: at baseline, 3 months, 6 months, and 12 months after intervention.
The eligibility and exclusion criteria of subjects were evaluated according to the inclusion situation. After screening, the participants were assigned depending on the different treatment method. (1) The age of the subjects were 18–55 years old; (2) met the diagnostic criteria of adenomyosis [10]; (3) there was no need for fertility, but the uterus was required to be preserved; (4) there was no contraindication for ablation by aggregated ultrasound; (5) the clinical data were complete; (6) informed consent given. Exclusion criteria: (1) patients diagnosed with severe insufficiency of heart, liver and kidney; (2) patients diagnosed with malignant tumor; (3) patients diagnosed with mental illness and unable to communicate normally; (4) patients diagnosed with other uterine diseases; (5) patients were intolerant to the therapeutic drugs; (6) patients who failed to complete the treatment as required; and (7) loss of follow-up during the study period. Patients were sent to the control group or the study group depending on the different treatment method. The subjects were not dropped out.
The control group was only treated with
focused ultrasound ablation and did not take any drug treatment after operation.
The non-menstrual period was selected for the operation. Routine items were
checked before the operation. The afternoon before the operation, the compound
polyethylene glycol electrolyte (P5413, Sigma-Aldrich, St.
Louis, MO, USA) was taken orally for catharsis. The night
before the operation and the morning the day of the operation, the enema was
performed. The patient’s lower abdomen was degreased and degassed before the
operation. Before treatment,diclofenac sodium (D6899,
Sigma-Aldrich, St. Louis, MO, USA) was taken for analgesia and sedation. During
treatment, the patient was kept in prone position, points for scanning were
selected, and the power of 300–400 W was set. The distance
between the focal point and the endometrium was more than 1.5 cm, and about 1 cm
from the lower surface of the uterine serous membrane. Contrast-enhanced
ultrasound was performed immediately after treatment to evaluate the ablation and
supplement treatment if necessary. Ablation results in the control group:
irradiation time (s): 1118.45
The mode of focused ultrasound ablation (Hifu) in the study group was the same
as that in the control group. Ablation results: irradiation time (s): 1120.62
Before treatment, 3 months, 6 months, and 12 months after treatment, all patients were examined by ultrasound. The anterior and posterior diameter, transverse diameter, and long diameter of the uterus were measured, and the uterine volume was calculated according to the formula.
Clinical symptoms were evaluated, which included the symptoms of dysmenorrhea
and the amount of menstruation, in which the degree of dysmenorrhea was scored by
the VAS [11]. The score ranged from 0 to 10, with 0 representing no pain, 10
representing the most severe pain. The menstrual volume was evaluated by the PBAC
[12]. The total area of sanitary napkins with blood staining area
At each time point mentioned above, 5 mL was collected from patients’ fasting elbow vein blood in the morning. After centrifugation, the supernatant was taken, and the expression of serum CA125 was detected by enzyme-linked immunosorbent assay (ELISA, Proteintech, Wuhan, Hubei, China).
The adverse reactions related to the treatment of the two groups were observed and recorded.
After treatment, a little of eutopic endometrial tissue was scraped (1
mm
The data were analyzed by SPSS 22.0 statistical analysis software (IBM Corp.,
Armonk, NY, USA). The measurement data conformed to a normal distribution and
uniform variance, which was expressed by (
In the study group, the mean age was (42.50
| Classification | Study group | Control group | t | p |
| Age (years) | 42.50 |
43.15 |
0.424 | 0.673 |
| Body mass index (BMI) | 24.86 |
25.07 |
0.419 | 0.677 |
| Course of disease (years) | 3.17 |
3.20 |
0.176 | 0.861 |
| Number of pregnancies | 1.83 |
1.87 |
1.100 | 0.276 |
| Number of births | 1.07 |
1.00 |
0.361 | 0.719 |
Note: The baseline data between the two groups. BMI, body mass index; t, student’s t test; p, probability value.
| Grouping | n | Before treatment | 3 months after treatment | 6 months after treatment | 12 months after treatment |
| Study group | 46 | 256.37 |
178.51 |
140.33 |
108.77 |
| Control group | 41 | 252.08 |
203.27 |
176.10 |
131.84 |
| t | 0.280 | 4.793 | 8.728 | 6.530 | |
| p | 0.780 |
Note: The uterine volume between the two groups. In contrast with the same group before treatment,
Before treatment, the VAS score and PBAC score had no significant distinction
between the two groups (p
| Grouping | n | VAS score | PBAC score | ||||||
| Before treatment | 3 months after treatment | 6 months after treatment | 12 months after treatment | Before treatment | 3 months after treatment | 6 months after treatment | 12 months after treatment | ||
| Study group | 46 | 3.12 |
1.47 |
0.93 |
0.62 |
132.65 |
87.36 |
68.22 |
31.40 |
| Control group | 41 | 3.08 |
2.34 |
1.57 |
1.15 |
130.78 |
100.26 |
90.35 |
52.91 |
| t | 0.341 | 9.118 | 9.374 | 10.507 | 0.417 | 4.493 | 9.887 | 14.393 | |
| p | 0.734 | 0.678 | |||||||
Note: The VAS score and PBAC score between the two groups. In contrast with the same group before treatment,
The serum CA125 levels had no notable distinction between the two groups before
treatment (p
| Grouping | n | Before treatment | 3 months after treatment | 6 months after treatment | 12 months after treatment |
| Study group | 46 | 105.34 |
50.22 |
45.37 |
38.62 |
| Control group | 41 | 102.86 |
65.37 |
58.80 |
53.16 |
| t | 0.508 | 6.441 | 9.228 | 14.556 | |
| p | 0.613 |
Note: The serum CA125 level between the two groups. In contrast with the same
group before treatment,
| Grouping | n | Abnormal vaginal discharge | Fatigue and fatigue | Haemorrhage | Uterine infection | Total occurrence |
| Study group | 46 | 5 | 3 | 2 | 1 | 11 (23.91) |
| Control group | 41 | 6 | 1 | 1 | 0 | 8 (19.51) |
| 0.246 | ||||||
| p | 0.620 |
Note: The adverse reactions between the two groups. n, number;
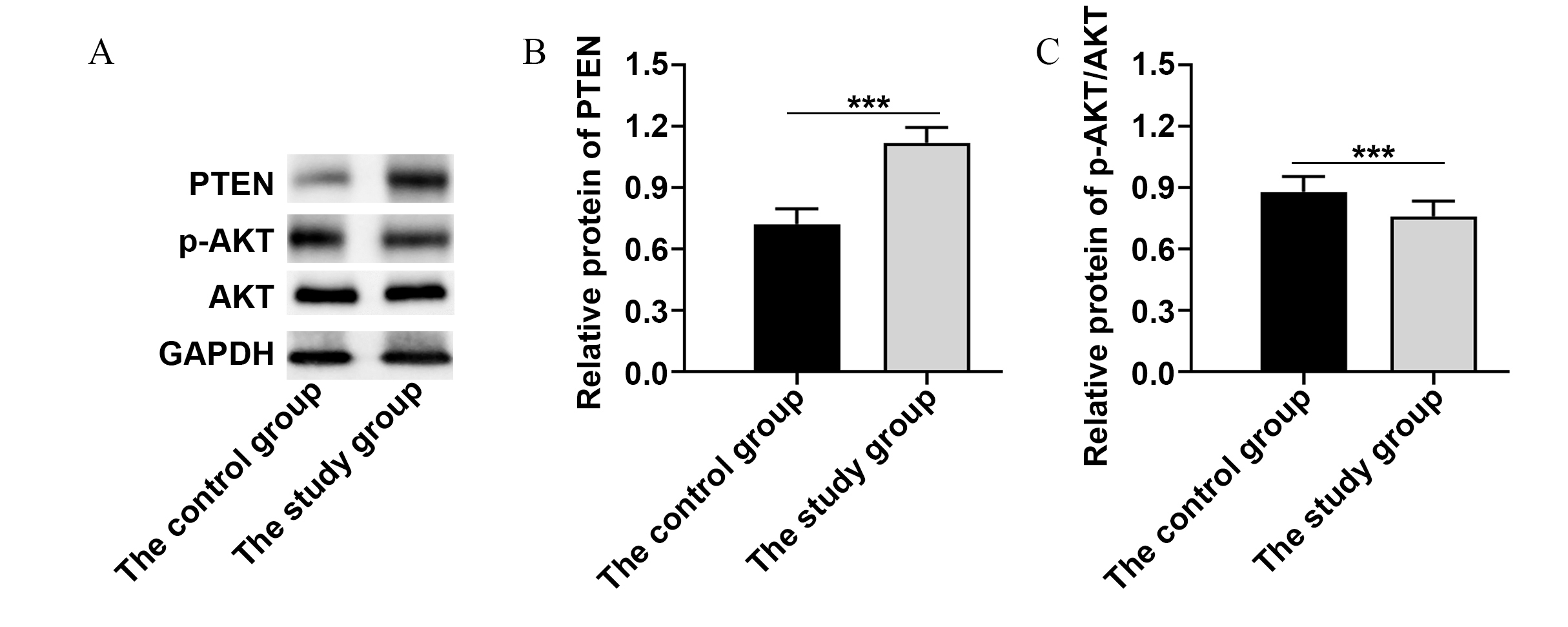
The level of PTEN in eutopic endometrium in the study group increased
significantly (p
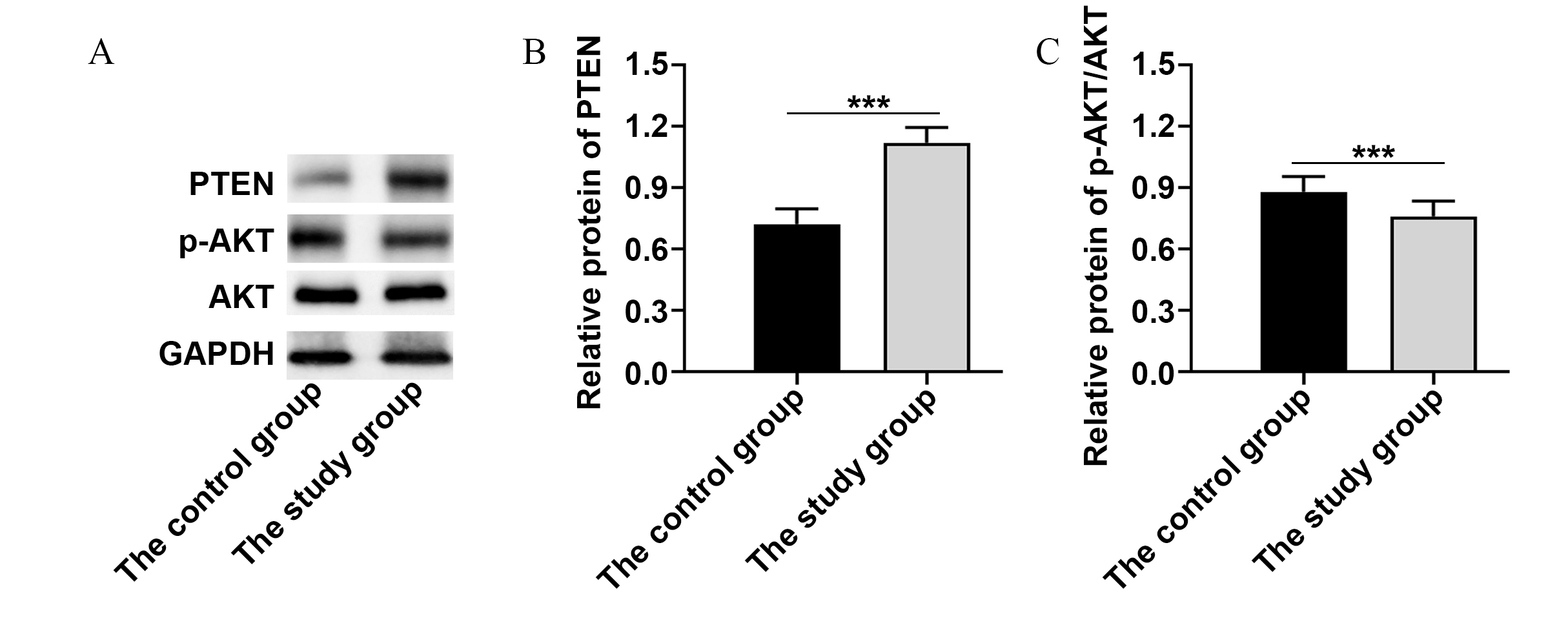 Fig. 1.
Fig. 1.The levels of proteins to PI3K/PTEN signal pathway. (A) Western
blot analysis of PTEN, p-AKT, AKT and GAPDH. (B) The relative protein of PTEN
between control group and study group. (C) The relative protein of p-AKT/AKT
between control group and study group. ***p
Adenomyosis is a common gynecological disease in women of childbearing age, and it is one of the main causes of female infertility. At present, most studies believe that the invasion of the basal endometrium into the myometrium is the basis of adenomyosis, and it is related to angiogenesis, abnormal secretion of progesterone and its receptor, cell proliferation and invasion, immunity, heredity, and other factors. The proliferation of inflammatory cells, neuroangiogenesis and abnormal secretion of sex steroid hormones are the key factors leading to dysmenorrhea, menorrhagia, and infertility [13]. Whether adenomyosis is genetically determined or microenvironmentally induced, and whether dysregulation of local factors causes changes in endometrial gene expression, is not yet clinically clear. Furthermore, more in-depth studies are needed to elucidate its pathogenesis, and to discover effective treatments to improve patients’ quality of life [14]. The treatment of adenomyosis includes surgery and drug therapy, each of which has its own advantages and disadvantages. Hysterectomy is needed to achieve the purpose of radical cure, whenever conservative drug treatment is not a feasible option of cure, nor taken for a long time. At the same time, investigations in recent years have shown that the incidence of adenomyosis is increasing year by year, in younger patients, and the older the age, the more limited the effect of conservative drug treatment [15]. At present, the proportion of late marriage and late childbearing in China has increased significantly, so there is an urgent need to find an efficient treatment with less uterine damage. Focused ultrasound ablation is one of the minimally invasive and innovative techniques in the field of surgery, which has the advantages of safe, non-invasive and reproducible operation, and has become a commonly used surgical treatment for uterine fibroids, adenomyosis, and various other gynaecological diseases [16].
The results of this study showed that the uterine volume, dysmenorrhea, and menstrual volume of the two groups were improved after treatment. Moreover and, the uterine volume, VAS score and PBAC score of the study group versus the control group were significantly lower at 3 months, 6 months, and 12 months after treatment. It is suggested that levonorgestrel combined with GnRH-a drug-assisted focused ultrasound ablation can improve the therapeutic effect of adenomyosis and further improve the clinical symptoms of patients. The therapeutic mechanism of focused ultrasound ablation is to cause coagulative necrosis of the focus tissue by physical method. On the one hand, the unclear boundary of the focus may affect the therapeutic effect. On the other hand, this method will not reduce the level of estrogen in patients. Therefore, there is a risk of recurrence after operation. It is reported that after focused ultrasound ablation, the recurrence rate of adenomyosis can be as high as 20% [17]. In this study, the adjuvant uses of GnRH-a and levonorgestrel-releasing intrauterine system after focused ultrasound ablation can effectively inhibit the estrogen level in patients and improve the therapeutic effect. Adenomyosis is an estrogen dependent disease. GnRH-a has a certain regulatory effect on the hypothalamus-pituitary-gonadal axis. It can reduce the expression of progesterone and estrogen by inhibiting the secretion of follicle hormone and luteinizing hormone, thus causing transient amenorrhea, shrinking the uterine volume, and reducing pelvic pain [18]. A previous relevant study [19] has showed that GnRH-a treatment after focused ultrasound ablation can reduce the recurrence rate of adenomyosis after surgery. Estrogen drugs are also commonly used in the treatment of adenomyosis. Long term use of levonorgestrel can make the endometrium subject to the effect of persistent progesterone, which will reduce menstrual flow [20]. Combined application of focused ultrasound ablation with levonorgestrel-releasing intrauterine system and GnRH-a can supplement the shortcomings of single method and ensure the therapeutic effect. In this study, the serum CA125 levels of the study group versus the control group at each timepoint after treatment was notably lower, which also showed that the combined application had better effect. CA125 is a glycoprotein secreted by epithelial tissue cells. A study has shown that the serum CA125 levels in patients with adenomyosis is abnormally high, which can be used as an index to evaluate the curative effect of the disease [21]. The comparison of this study showed that the incidence of adverse reactions had no notable distinction between the two groups, indicating that the combination therapy has higher safety, which is consistent with the results of previous similar study [22].
In order to explore the mechanism of combined therapy, the levels of PTEN, AKT and p-AKT in eutopic endometrium were contrasted between the two groups. It was found that the level of PTEN increased, and the levels of AKT and p-AKT decreased. It suggests that PI3K/PTEN signal pathway is involved in the occurrence and development of adenomyosis, and levonorgestrel-releasing intrauterine system and GnRH-a may play a therapeutic role by upregulating the expression of PTEN. A previous study [23] has shown that the level of PTEN in eutopic and ectopic endometrium of patients with adenomyosis decreased, and the levels of AKT and p-AKT protein increased, which confirmed that PI3K/PTEN/AKT signaling pathway was involved in the pathogenesis of adenomyosis. In relevant animal experiments, by building a mouse model of adenomyosis, it was also found that Neiyi Kangfu Tablets could treat and control the symptoms of adenomyosis by upregulating PTEN and downregulating p-P65 protein expression [24].
In conclusion, it is safe and feasible to use levonorgestrel-releasing intrauterine system and GnRH-a combined therapy after focused ultrasound ablation, which can notably reduce the uterine volume of patients and improve clinical symptoms. Its mechanism may be related to the upregulation of PTEN protein expression.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
HF and XG designed the research study. HF and CH performed the research. HF and XG analyzed the data. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
As this study was a retrospective cohort study with no specific interventions, only anonymized medical record data and clinical information that were pooled to produce the results were used and did not allow the identification of participants, ethical approval was waived according to the Ethics Committee of Jinhua Municipal Central Hospital.
We would like to express our gratitude to all those who helped us during the writing of this manuscript. Thanks to all the peer reviewers for their opinions and suggestions.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.