


 , Tingting Xia 1,*
, Tingting Xia 1,*1 Center for Reproductive Medicine, the Third Affiliated Hospital of Sun Yat-sen University, 510630 Guangzhou, Guangdong, China
2 Department of Obstetrics, the Third Affiliated Hospital, Sun Yat-sen University, 510630 Guangzhou, Guangdong, China
†These authors contributed equally.
Abstract
Background: High responders are characterized by a large number of
retrieved oocytes and/or a high level of estradiol on the day of administration
of human chorionic gonadotropin. There is controversy in the literature regarding
live birth rates from fresh day-5 single blastocyst transfer (day-5 SBT) compared
to cleavage-stage fresh day-3 embryo transfer (day-3 ET) in high responders. The
aim of this study was therefore to compare reproductive outcomes between day-5
SBT and day-3 ET using high-quality embryos and gonadotropin-releasing hormone
(GnRH) antagonist protocols in high responders undergoing in vitro
fertilization/intracytoplasmic sperm injection (IVF/ICSI).
Methods: This was a single-center retrospective study of 282
high responders who underwent fresh day-5 SBT (day-5 SBT group, n = 142) or two
cleavage-stage fresh day-3 embryo transfer (day-3 ET group, n = 140) between 2015
and 2019. Results: No significant differences were observed between the
day-5 SBT and day-3 ET groups in terms of clinical pregnancy rate (51.41%
vs. 59.29%, p = 0.183) or live birth rate (41.55%
vs. 52.86%, p = 0.057). The incidence of multiple pregnancy
(1.37% vs. 36.14%) and of low birth weight (5.00% vs.
32.26%) were significantly less frequent in the day-5 SBT group than in the
day-3 ET group (p
Keywords
- high responder
- fresh cycle
- blastocyst transfer
- cleavage-stage embryo
- gonadotropin-releasing hormone antagonist
Since its advent almost 40 years ago, in vitro
fertilization/intracytoplasmic sperm injection (IVF/ICSI) has helped many
infertile couples to become parents. Controlled ovarian stimulation (COS) is an
essential step in IVF/ICSI treatment, with a subset of patients found to be
sensitive to COS. These patients are known as high responders and are
characterized by a total follicle count of 15 or more and/or an estradiol (E2)
concentration
Many studies have shown that frozen embryo transfer (FET) is preferable for high responders since it has a higher live birth rate (LBR) and a lower incidence of ovarian hyperstimulation syndrome (OHSS) compared to fresh embryo transfer (ET) [2, 3]. However, other studies have reported that FET had no advantage over fresh ET in terms of reducing OHSS in high responders [4]. Moreover, for infertile women with polycystic ovary syndrome (PCOS), it was reported that FET was associated with a higher risk of preeclampsia after the first transfer than fresh ET [2]. Furthermore, fresh ET can result in shorter times to pregnancy and live birth than FET, thus making it more cost-effective [5]. In addition, the use of gonadotropin-releasing hormone (GnRH) antagonists is associated with a reduced incidence of OHSS and does not seem to compromise ongoing pregnancy rates [6]. Therefore, fresh ET is worth considering for some high responders undergoing GnRH antagonist cycles.
To obtain an optimal clinical pregnancy rate (CPR), two cleavage-stage embryos are usually transferred. However, this can have adverse consequences related to multiple pregnancy in women and their new-borns [7]. Evidence shows that single blastocyst transfer (SBT) may be an effective way to lower the risk of multiple pregnancy without affecting the CPR [8, 9, 10]. Nevertheless, several retrospective studies on high responders in IVF/ICSI cycles have shown that fresh SBT was inferior to fresh day-3 ET (two embryo transfer) in terms of the CPR [3, 11]. Thus, clinicians face a dilemma between the use of day-3 ET or day-5 SBT during fresh cycles, especially when multiple high-quality embryos are available for high responders. Further studies are therefore needed to provide more reliable evidence when faced with this dilemma.
To the best of our knowledge, clinical outcomes with day-3 ET or day-5 SBT for high responders stimulated with GnRH antagonists in fresh cycles have not been reported to date. In the present study, we compared the CPR, LBR, OHSS and other IVF/ICSI-associated complications between fresh day-5 SBT and fresh day-3 ET using high-quality embryos in high responders. The European Society of Human Reproduction and Embryology (ESHRE) guidelines recommend the GnRH antagonist protocol for high responders due to its better safety and equivalent efficacy [12]. This comparative analysis therefore included only patients who were stimulated with GnRH antagonists.
The patient cohort for this retrospective study consisted of high responders [1]stimulated with a GnRH antagonist protocol. Between September 2015 and December 2019, these patients underwent IVF/ICSI cycles at the Reproductive Medical Center, Third Affiliated Hospital, Sun Yat-sen University.
As shown in Fig. 1, 1382 patients with high response to COS using the GnRH antagonist protocol were initially evaluated. Of these, 375 received fresh ET. The final study cohort consisted of 282 patients who underwent transfer with high-quality embryos. Of these, 142 received one fresh day-5 blastocyst ET and were assigned to the day-5 SBT group. The remaining 140 patients received fresh day-3 ET with two cleavage-stage embryos and were assigned to the day-3 ET group.
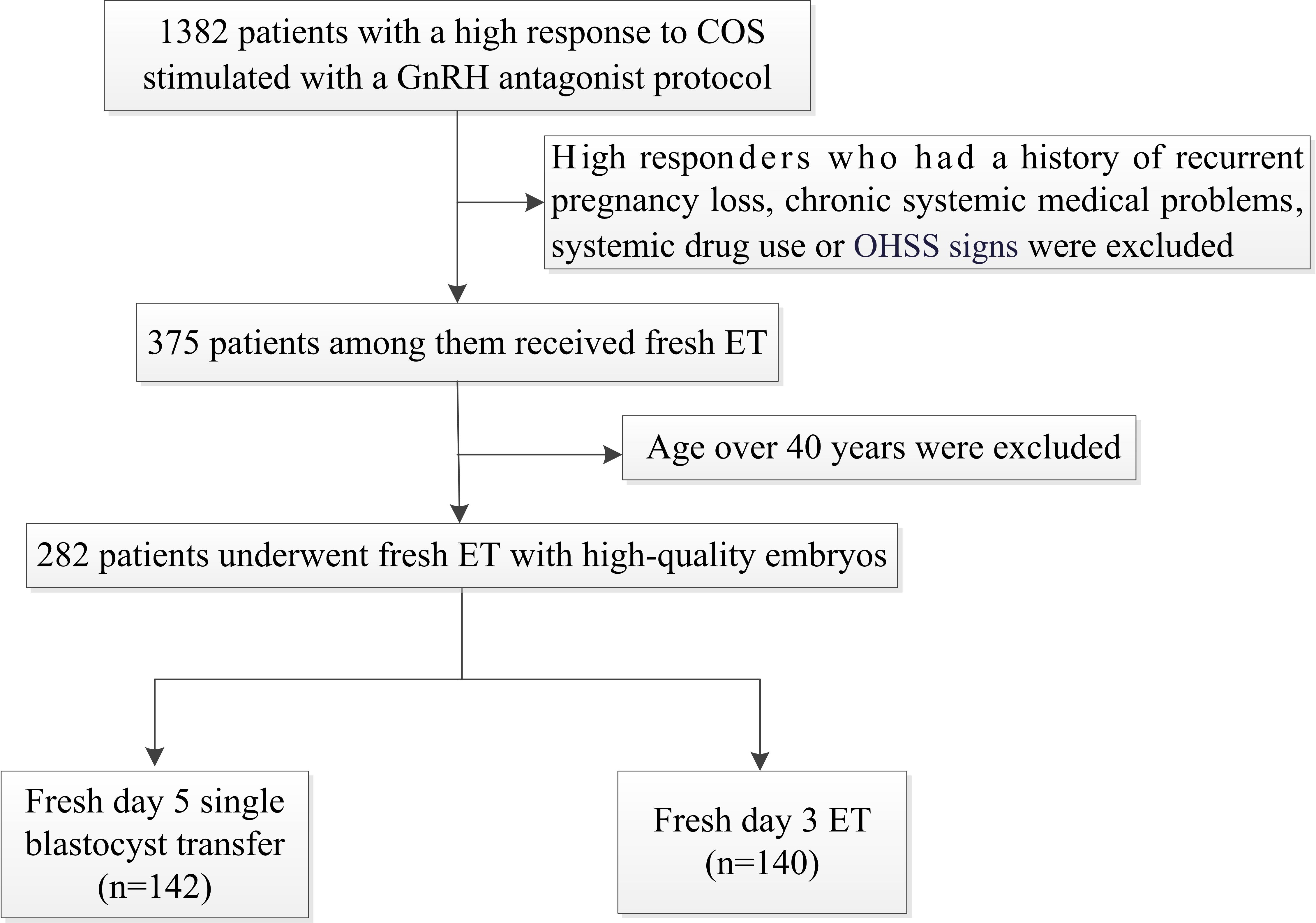 Fig. 1.
Fig. 1.Study flowchart. COS, controlled ovarian stimulation; OHSS, ovarian hyperstimulation syndrome; GnRH, gonadotropin-releasing hormone; ET, embryo transfer.
The inclusion criteria were as follows: (1) infertility caused by tubal factors,
endometriosis, anovulation, male factors, or unexplained reasons; (2) use of GnRH
antagonist protocol; (3) high responders [1], defined as patients with 15 or more
retrieved oocytes and/or an E2 concentration
All patients in this study received the GnRH antagonist protocol. The starting
dose was 50–300 IU of gonadotrophin (Merck Serono, Modugno, Italy; MSD,
Ravensburg, Germany; Lizhu Pharmaceutical Trading, Zhuhai, Guangdong, China) on
days 2–3 of the menstrual cycle. Follicular development was assessed by both
transvaginal ultrasonography and analysis of the serum hormone profile.
Cetrorelix (Merck Serono, Halle, Germany) or ganirelix (Organon, Ravensburg,
Germany; Zhengdatianqing Pharmaceutical Group, Nanjing, Jiangsu, China) was added
from day-5 of stimulation, or when the dominant follicle was
After informing patients of the advantages and disadvantages of blastocyst
culture, they were given the choice of either day-3 ET or day-5 SBT. In the SBT
group, one blastocyst was selected for transfer. High-quality blastocysts on
day-5 after oocyte retrieval were defined as 4BB grade or better according to the
Gardner and Lane criteria [13]. In the day-3 ET group, two high-quality embryos
were selected for transfer. These were defined as
All baseline and clinical data were collected from the hospital records. Serum
levels of anti-Müllerian hormone (AMH), follicle stimulating hormone (FSH),
luteinizing hormone (LH), E2 and progesterone (P) were measured using
chemiluminescence methods. The primary outcome parameters were CPR and LBR.
Secondary outcome parameters were OHSS development, implantation rate (IR), and
multiple pregnancy status. Clinical pregnancy was defined as the presence of a
gestational sac on transvaginal ultrasound approximately four to five weeks after
ET. IR was defined as the number of observed gestational sacs divided by the
number of embryos transferred. LBR was defined as the delivery of any viable
infant at
All data were analyzed using SPSS (version 20.0, IBM, Armonk, NY, USA).
Numerical data are presented as the mean
As shown in Table 1, no significant differences in age, body mass index (BMI),
duration of infertility, primary cause of infertility, AMH, and baseline LH or E2
level were detected between the day-5 SBT and day-3 ET groups (p
| Day-5 SBT | Day-3 ET | p value | ||
| (n = 142) | (n = 140) | |||
| Age (years) | 30.50 (27.00–33.00) | 31.00 (28.00–34.00) | 0.624 | |
| BMI (kg/m |
20.30 (19.25–23.27) | 20.58 (19.09–22.85) | 0.744 | |
| Duration of infertility (years) | 3.00 (2.00–4.75) | 3.00 (2.00–5.00) | 0.442 | |
| Primary cause of infertility | 0.701 | |||
| Male | 40 (28.17) | 35 (25.00) | ||
| Female | 91 (64.08) | 93 (66.63) | ||
| Both | 6 (4.23) | 9 (6.43) | ||
| Unexplained | 5 (3.52) | 3 (2.14) | ||
| AMH (ng/mL) | 5.01 (3.46–7.12) | 5.44 (2.75–8.59) | 0.889 | |
| Baseline FSH (IU/L) | 6.19 |
6.42 (5.75–7.59) | 0.002 | |
| Baseline LH (IU/L) | 5.49 (4.43–8.44) | 5.18 (4.31–7.49) | 0.479 | |
| Baseline E2 (pg/mL) | 35.87 (27.11–50.16) | 37.17 (27.06–50.23) | 0.514 | |
SBT, single blastocyst transfer; ET, embryo transfer; BMI, body mass index; AMH, anti-Mullerian hormone; FSH, follicle stimulating hormone; LH, luteinizing hormone; E2, estradiol.
As shown in Table 2, no significant differences were observed between the two
groups in terms of the FSH, LH, E2 and P levels on the hCG trigger day, the
trigger rate for GnRH agonist plus hCG, the number of oocytes, or the incidence
of moderate/severe OHSS (p
| Day-5 SBT | Day-3 ET | p value | |
| (n = 142) | (n = 140) | ||
| FSH on hCG trigger day/(IU/L) | 10.94 (8.99–13.54) | 11.99 (9.95–14.13) | 0.288 |
| LH on hCG trigger day/(IU/L) | 3.09 (2.11–4.68) | 2.51 (1.80–3.86) | 0.129 |
| E2 on hCG trigger day/(pg/mL) | 3353.35 |
3318.0 (3002.0–3720.5) | 0.981 |
| P on hCG trigger day/(ng/mL) | 0.78 |
0.79 |
0.736 |
| GnRHa + hCG trigger rate | 39 (27.46) | 36 (25.71) | 0.739 |
| Oocytes | 15.50 (11.00–17.75) | 15.00 (11.00–17.00) | 0.258 |
| Moderate/Severe OHSS | 3 (2.12) | 3 (2.14) | 0.986 |
SBT, single blastocyst transfer; ET, embryo transfer; FSH, follicle stimulating hormone; LH, luteinizing hormone; E2, estradiol. P, progesterone; hCG, human chorionic gonadotrophin; GnRHa, gonadotropin-releasing hormone agonist; OHSS, ovarian hyperstimulation syndrome.
Table 3 compares the outcomes between the day-5 SBT and day-3 ET groups. No significant differences were found with regard to the incidence of CPR, LBR, early pregnancy loss, ectopic pregnancy, prematurity, macrosomia, congenital anomalies, or neonatal gender. The day-5 SBT group had a significantly higher IR than the day-3 ET group, but lower incidence of multiple pregnancy and LBW.
| Day-5 SBT | Day-3 ET | p value | ||
| (n = 142) | (n = 140) | |||
| CPR | 73 (51.41) | 83 (59.29) | 0.183 | |
| IR | 71 (50.00) | 111 (39.64) | 0.042 | |
| Early pregnancy loss | 11 (15.07) | 6 (7.22) | 0.117 | |
| Ectopic pregnancy | 2 (2.74) | 1 (1.20) | 0.911 | |
| LBR | 59 (41.55) | 74 (52.86) | 0.057 | |
| Multiple pregnancy | 1 (1.37) | 30 (36.14) | ||
| Prematurity | 8 (13.56) | 14 (18.92) | 0.409 | |
| LBW | 3 (5.00) | 30 (32.26) | ||
| Macrosomia | 0 (0.00) | 3 (3.23) | 0.280 | |
| Congenital anomalies | 0 (0.00) | 0 (0.00) | ||
| Neonatal gender | 0.187 | |||
| Boy | 34 (56.67) | 42 (46.16) | ||
| Girl | 26 (43.33) | 51 (54.84) | ||
SBT, single blastocyst transfer; ET, embryo transfer; CPR, clinical pregnancy rate; IR, implantation rate; LBR, live birth rate; LBW, low birth weight.
Table 4 shows the comparison of outcomes between day-5 SBT and day-3 ET groups
according to patient age. For both age groups, no significant differences were
observed between day-5 SBT and day-3 ET groups with regard to CPR, LBR, early
pregnancy loss, ectopic pregnancy, prematurity or macrosomia, congenital
anomalies or neonatal gender. For patients aged
| Day-5 SBT | Day-3 ET | p value | Day-5 SBT | Day-3 ET | p value | ||
| (n = 66) | (n = 73) | (n = 76) | (n = 67) | ||||
| CPR | 29 (43.94) | 40 (54.79) | 0.201 | 44 (57.89) | 43 (64.18) | 0.442 | |
| IR | 29 (43.94) | 55 (37.67) | 0.388 | 44 (57.89) | 56 (41.79) | 0.025 | |
| Early pregnancy loss | 5 (17.24) | 2 (5.00) | 0.122 | 6 (13.64) | 4 (9.30) | 0.739 | |
| Ectopic pregnancy | 0 (0.00) | 1 (2.50) | 1.000 | 2 (4.55) | 0 (0.00) | 0.494 | |
| LBR | 23 (34.85) | 35 (47.95) | 0.118 | 36 (47.37) | 39 (58.21) | 0.195 | |
| Multiple pregnancy | 0 (0.00) | 17 (42.50) | 1 (2.27) | 13 (30.23) | |||
| Prematurity | 3 (13.04) | 8 (22.86) | 0.499 | 5 (13.89) | 6 (15.38) | 0.855 | |
| LBW | 0 (0.00) | 16 (36.36) | 0.001 | 3 (8.11) | 14 (28.57) | 0.014 | |
| Macrosomia | 0 (0.00) | 1 (2.27) | 1.000 | 0 (0.00) | 2 (4.08) | 0.504 | |
| Congenital anomalies | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | |||
| Neonatal gender | 0.494 | 0.202 | |||||
| Boy | 13 (56.52) | 21 (47.73) | 21 (56.76) | 21 (42.86) | |||
| Girl | 10 (43.48) | 23 (52.27) | 16 (43.24) | 28 (57.14) | |||
SBT, single blastocyst transfer; ET, embryo transfer; CPR, clinical pregnancy rate; IR, implantation rate; LBR, live birth rate; LBW, low birth weight.
This study found that day-5 SBT and day-3 ET showed similar CPR and LBR following fresh transfer of high-quality embryos in high responders stimulated with a GnRH antagonist protocol. Moreover, day-5 SBT showed significantly higher IR and lower incidence of multiple pregnancy and LBW than day-3 ET.
Extended culture to the blastocyst stage is considered a useful tool for embryo
selection, since it allows only high-quality embryos to develop into blastocysts
[18]. A meta-analysis of 5 randomized clinical trials (RCTs) found that SBT was
associated with a higher rate of ongoing pregnancy and LBR than single
cleavage-stage transfer [19]. A recent publication involving 15 studies and 2219
women also found the LBR was higher in blastocyst transfer patients than in
cleavage-stage ET patients (odds ratio (OR) 1.27, 95% confidence interval (CI)
1.05 to 1.51) following fresh ET [10]. However, in the present study with
high-quality embryos we observed a trend (p = 0.057) for day-3 ET to
have higher LBR than day-5 SBT. This trend was observed in both the younger and
older patient groups. Moreover, the CPR with day-3 ET was reported to be
significantly higher than SBT in high responders with the GnRH agonist protocol
and fresh cycles [3]. A previous study reported no significant difference in the
LBR between SBT and two cleavage-stage ET [20]. Because blastocysts have good
developmental potential, blastocyst transfer with high-quality embryos should
result in better clinical outcomes than cleavage-stage ET. However, in the
present study blastocyst transfer did not result in significantly better LBR
compared to cleavage-stage ET (41.55% vs. 52.86%, p = 0.057). This may
be due to the fact that two embryos were transferred in the cleavage-stage ET
group, and a high serum E2 level (
The day-5 SBT group was observed here to have a higher IR than the day-3 ET
group, indicating the rate of successful implantation between the two groups was
different. The IR was not significantly different when the patients were aged
It has been proposed that GnRH antagonists have the advantage of reducing the risk of OHSS in women with PCOS [6]. Moreover, a GnRH agonist for oocyte triggering resulted in a lower incidence of OHSS in normal patients [24, 25]. In the present study, the number of oocytes induced by GnRH agonist plus hCG was almost identical in the day-5 SBT and day-3 ET groups. Since all patients in the current study were stimulated with the GnRH antagonist protocol, the incidence of OHSS was already rather low in high responders due to the beneficial effect of this protocol.
Numerous studies have recommended that SBT be considered first in routine practice when high-quality blastocysts are available, as this reduces the risk of multiple pregnancy and has no effect on the LBR [7, 26]. In accordance with these studies, our analysis also found the multiple pregnancy rate with day-5 SBT was markedly lower than with day-3 ET. Multiple pregnancy is considered an important risk factor for LBW and is associated with increased medical, psychological, economic and social costs [27, 28]. As expected, the incidence of LBW in the current study was found to be markedly higher in the day-3 ET group than in the day-5 SBT group. Advanced age is an important risk factor for female infertility, pregnancy loss, fetal anomalies, stillbirth, and obstetric complications [29]. Patients who have a good response to COS and undergo fresh ET are usually young [1]. The median age of patients in the day-5 SBT and day-3 ET groups in the current study was very similar at around 30 years. There was no evidence of any differences between the two groups in terms of the incidence of early pregnancy loss, ectopic pregnancy, prematurity, macrosomia, congenital anomalies, or in terms of neonatal gender. These results concur with those of previous studies [30].
This study was limited by its retrospective design and the use of data from a single-center. The inclusion and exclusion criteria were strictly obeyed in order to minimize the risk of bias in the selection of patients. In view of its limitations, this was a preliminary study to examine the outcome of two fresh ET strategies, day-5 SBT and day-3 ET, for high responders in GnRH antagonist cycles.
In conclusion, when considering the CPR, IR, LBR and various complications such as LBW and multiple pregnancy, day-5 SBT appears to be preferable over day-3 ET for high responders undergoing IVF/ICSI cycles with GnRH antagonist in fresh ET cycles with high-quality embryos. However, further RCTs are needed to determine more accurately which fresh ET strategy is best for high responders with high-quality embryos.
The raw data generated in this study are available upon reasonable request from the corresponding author.
Conceptualization: TX, YZ, JO, WX. Data curation: FY, XL, WX. Formal analysis and investigation: TX, FY, JO. Methodology: WX, FY, XL. Resources: FY, XL. Supervision: JO. Writing – original draft: WX, JO. Writing – review & editing: WX, JO, TX. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study was approved by the Institutional Review Board of the Third Affiliated Hospital of Sun Yat-sen University ([2021]02-143-01). All patients in this study signed informed consent forms to undergo IVF/ICSI treatments in our center, and the anonymity of the patients has been strictly protected.
Not applicable.
This project was supported by the Medical Scientific Research Foundation of Guangdong Province of China (Grant No.: A2020575).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.