







1 Clinic for Gynecology and Obstetrics, University Clinical Centre of Serbia, 11000 Belgrade, Serbia
2 Department of Obstetrics and Gynecology, Lebanese American University Medical Center-Rizk Hospital, 4505 Beirut, Lebanon
3 Faculty of Medicine, University of Belgrade, 11000 Belgrade, Serbia
4 Clinic for General and Pediatric Surgery, General Hospital Čačak, 32000 Čačak, Serbia
5 Department of Gynecology and Obstetrics, Pia Fondazione “Card. G. Panico”, 73039 Tricase (Lecce), Italy
6 Department of Obstetrics and Gynecology and CERICSAL (CEntro di RIcerca Clinico SALentino), “Veris delli Ponti Hospital”, Scorrano, 73020 Scorrano (Lecce), Italy
Abstract
Objective: The transvaginal natural orifice transluminal endoscopic surgery (vNOTES) is a kind of natural orifice transluminal endoscopic surgery in which the abdominal cavity is reached by using the natural orifices, such as the stomach, rectum, esophagus, and bladder. In comparison to traditional laparoscopic and robotic surgery, there are potential advantages of the vNOTES. This narrative review shows the use of vNOTES in contemporary gynecologic endoscopic surgery. Mechanism: MEDLINE, Scopus, and PubMed searches on these themes were conducted from 1990 to 2023 using a mix of keywords. Papers and articles were identified and included in this narrative review after the authors’ revision and evaluation. Findings in Brief: The vNOTES procedures allow a short surgery time, as well as estimated blood loss and postoperative pain. These procedures are safe and feasible in contemporary endoscopic gynecology surgery. Conclusions: The vNOTES procedures are beneficial for the patients, and to be added to other minimally invasive procedures, such as conventional laparoscopy and robotic surgery. However, further studies about the long-term outcomes of vNOTES procedures are still needed.
Keywords
- vNOTES
- gynecology
- endoscopic surgery
- laparoscopy
- minimally invasive surgery
Transvaginal natural orifice transluminal endoscopic surgery (vNOTES) is an endoscopic, minimally invasive surgical approach to be added to conventional laparoscopy or robotic surgery [1]. The vNOTES technique is a type of natural orifice transluminal endoscopic surgery, in which the abdominal cavity is reached by using natural orifices, such as the stomach, rectum, esophagus, and bladder [2]. In vNOTES methods, in gynecologic endoscopic surgery, the used natural orifice is traditionally the vagina. Vaginal access is preferred for the lower risk of postoperative infections, as well as improved visualization, closure and postoperative healing [2]. Although it is not a new approach, in comparison to traditional laparoscopic and robotic surgery, the potential advantages of the vNOTES are the shorter operative time, less pain, decreased operative risks, and improved cosmesis [3]. The vNOTES procedures are used for hysterectomy, adnexal urgent procedures (ovarian cystectomies, salpingectomies, oophorectomies), and uterosacral ligament suspension [3, 4, 5]. These procedures are also used in different settings such as: obese patients, nulliparous patients, large uteri, and prior hysterectomies [3, 4, 5, 6, 7, 8, 9, 10]. This narrative review aims to present the current utilization of vNOTES in contemporary gynecologic endoscopic surgery.
The authors searched the available data on the usage of vNOTES in current gynecologic endoscopic practice. Authors conducted a MEDLINE, Scopus, and PubMed search, for the years 1990–2023, using a combination of keywords, such as “vNOTES”, “minimally invasive surgery”, “gynecological endoscopic surgery”, “vaginal surgery”, “surgical treatment”, “complications”, “blood loss”, “surgical outcome”, “healing”, “obesity”, “management”, “infertility”, “hysterectomy”, “myomectomy”, “adnexal surgery”, “cystectomy”. Peer-reviewed articles concerning vNOTES were included in this paper. Additional articles were identified from the references of relevant papers. The results of the research have been divided into different paragraphs, with which we have illustrated what has been reported in the scientific literature.
There are reported advantages of vNOTES surgery in the management of female infertility. In comparison to the laparoendoscopic single-site surgery, the vNOTES procedure is linked to less pain and shorter postoperative bowel movement time [11]. The vNOTES procedure is a less invasive, safe and practical procedure for the diagnosis and treatment of female infertility, especially suitable for patients who have special cosmesis requirements [11]. Moreover, the vNOTES are used as an ovarian drilling surgical procedure (Fig. 1) in patients with the dysovulatory polycystic ovarian syndrome, when the traditional medical treatment with clomiphene citrate, metformin, and/or letrozole is not effective [12]. Furthermore, some additional advantages of the vNOTES reported are an easier and a scarless access to the pelvic cavity (Fig. 2) [12]. Similar results were reported by Jegaden et al. [12], who reported that vNOTES is an easy technique, with minimal adverse effects, especially in obese patients. The vNOTES could be used in performing the isthmic retroperitoneal cerclage, even if Baekelandt [13] reported the first description of the technique of placement of permanent cerclage at the isthmic level of the cervix via the vNOTES procedure. Tavano et al. [14] performed a retrospective observational cohort study, which included 125 patients under 43 years, that underwent fertility-preserving vNOTES procedures such as vNOTES salpingectomy for ectopic pregnancy, vNOTES myomectomy, vNOTES cystectomy, and vNOTES unilateral adnexectomy. The authors observed a total of 26 pregnancies, of which 18 pregnancies were achieved within the period of the 1 year after the vNOTES procedure. The mean interval between surgery and pregnancy was 6 months. There were no vNOTES-related complications in all of the observed 26 pregnancies, and delivery at term was observed in all of these cases. The majority of these patients’ mode of delivery was a vaginal delivery. The authors showed that the vNOTES procedure did not influence the mode of consequent delivery, or cause of the delivery-related injuries. Also, they showed no adverse events related to the vNOTES in reproductive-age women. Posterior colpotomy as performed in all vNOTES procedures is by itself not an indication for an elective Caesarean section. On the other hand, vNOTES approach could be used for the permanent female sterilization [15]. Yassa et al. [15] conducted prospective cohort study to compare conventional laparoscopy and vNOTES approach in the bilateral salpingectomy. The use of vNOTES was associated with the lower 6-hour and 24-hour postoperative visual analog scale (VAS) scores, as well as less need for the postoperative analgesic administration. Also, authors reported the higher postoperative improvement in the vNOTES group. However, on the other hand there was similar postoperative decline in female sexual function in both groups [15]. There were no postoperative complications observed in both groups [15].
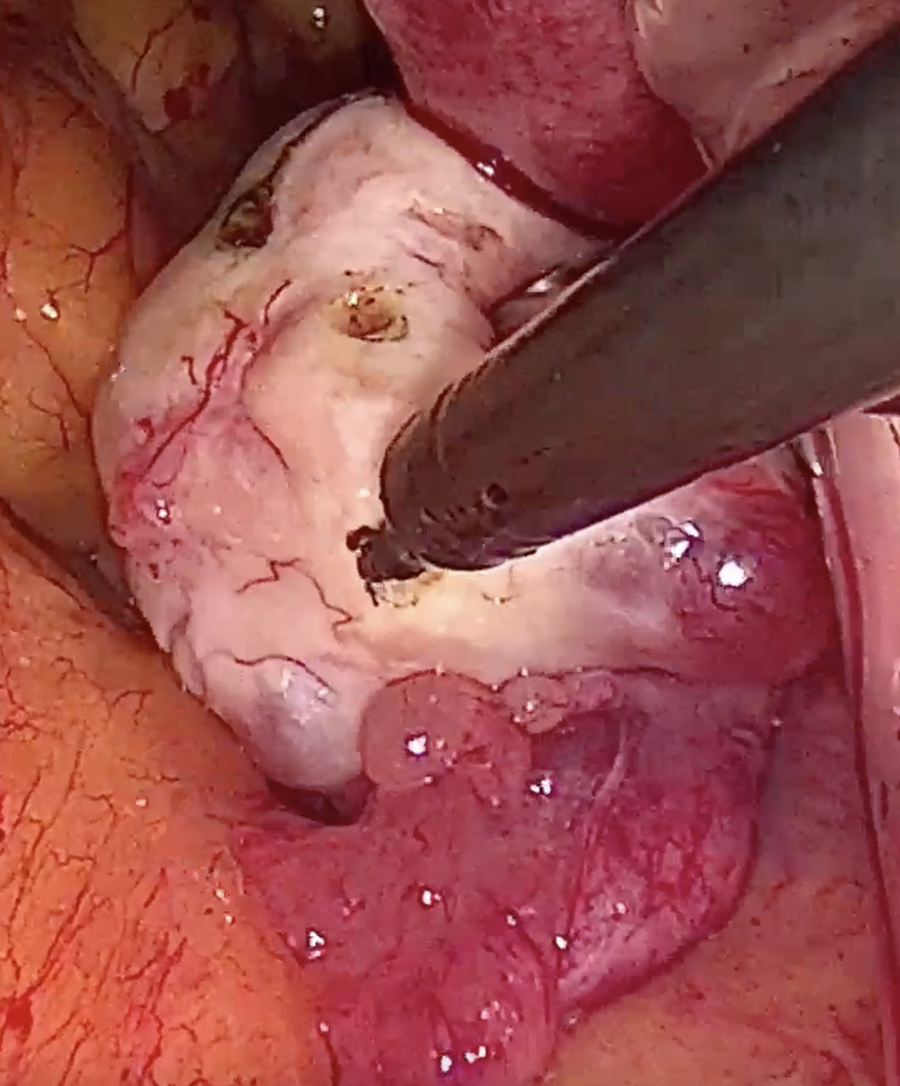 Fig. 1.
Fig. 1.Ovarian drilling by vNOTES. vNOTES, transvaginal natural orifice transluminal endoscopic surgery.
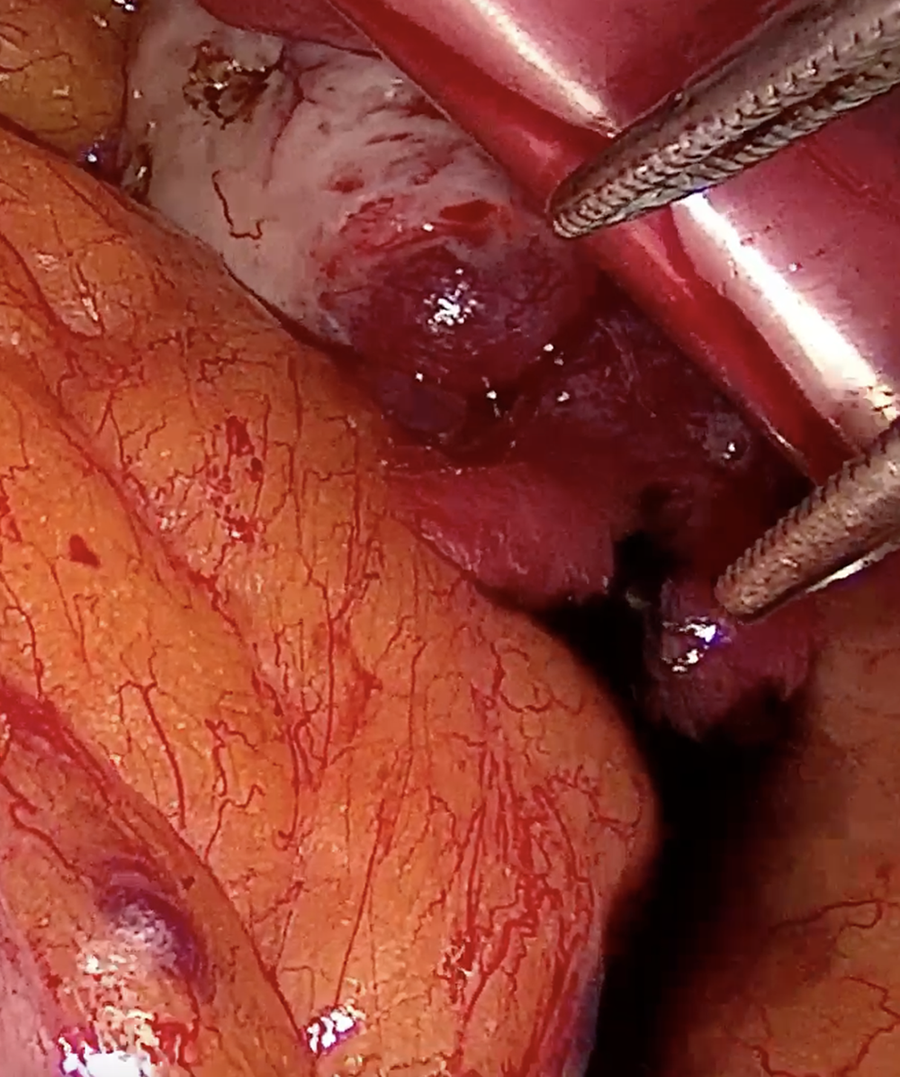 Fig. 2.
Fig. 2.Tubal patency test on the left side.
Comparing vNOTES to standard laparoscopy, vNOTES demonstrates additional positive pre, intra, and postoperative outcomes effects. It could be considered an alternative technique to conventional laparoscopy in emergent gynecologic surgery [16]. Karakaş et al. [16] performed a retrospective study to compare conventional laparoscopy and vNOTES procedures in the management of the emergency indications, such as ovarian torsion, acute abdominal pain, ovarian cyst rupture, and ectopic pregnancy. The authors reported a significantly shorter duration of surgery, allowing VAS scores at 6 h and after 12 h, and a shorter hospital stay in women operated by vNOTES method, in comparison to conventional laparoscopy [16]. Ozceltik et al. [17] described the vNOTES technique for the treatment of ectopic pregnancy. The authors used conventional laparoscopic equipment, with the addition of a self-constructed pessary port for management of the ectopic pregnancy in 21 women. The authors reported that the median duration of the hospital stay after surgery was 1 day. In the women who underwent vNOTES for the management of ectopic pregnancy were no complications within 30 days after surgery [17]. Kaya et al. [18] reported a significantly shorter duration of surgery and postoperative hospital stay, as well as a lower VAS pain score in women who underwent vNOTES for the management of emergent gynecological states, in comparison to the conventional laparoscopy. The experiences from the different centers worldwide showed that the vNOTES is a feasible and safe method for the management of ectopic pregnancy, and the most common emergent state in gynecology [19, 20, 21].
There is a wide spectrum of indications for the vNOTES use in elective
gynecological surgery (Fig. 3). Farah et al. [1] reported the
experiences of vNOTES performed hysterectomies and uterosacral ligament
suspension performed on 23 women. The authors reported that hysterectomy (Fig. 4)
and uterosacral ligament suspension is a feasible and safe procedure when
performed via vNOTES [1]. Liu et al. [22] described the operative
technique, as well as short-term outcomes of 26 women treated for pelvic organ
prolapse with the vNOTES sacrocolpopexy. The authors conducted a retrospective
case series study that included women with stages II to IV of pelvic organ
prolapse. In this study group, the median operative time duration was 184 minutes
(interquartile range, 158.5–202.5). Also, the mean estimated blood loss was
30.87
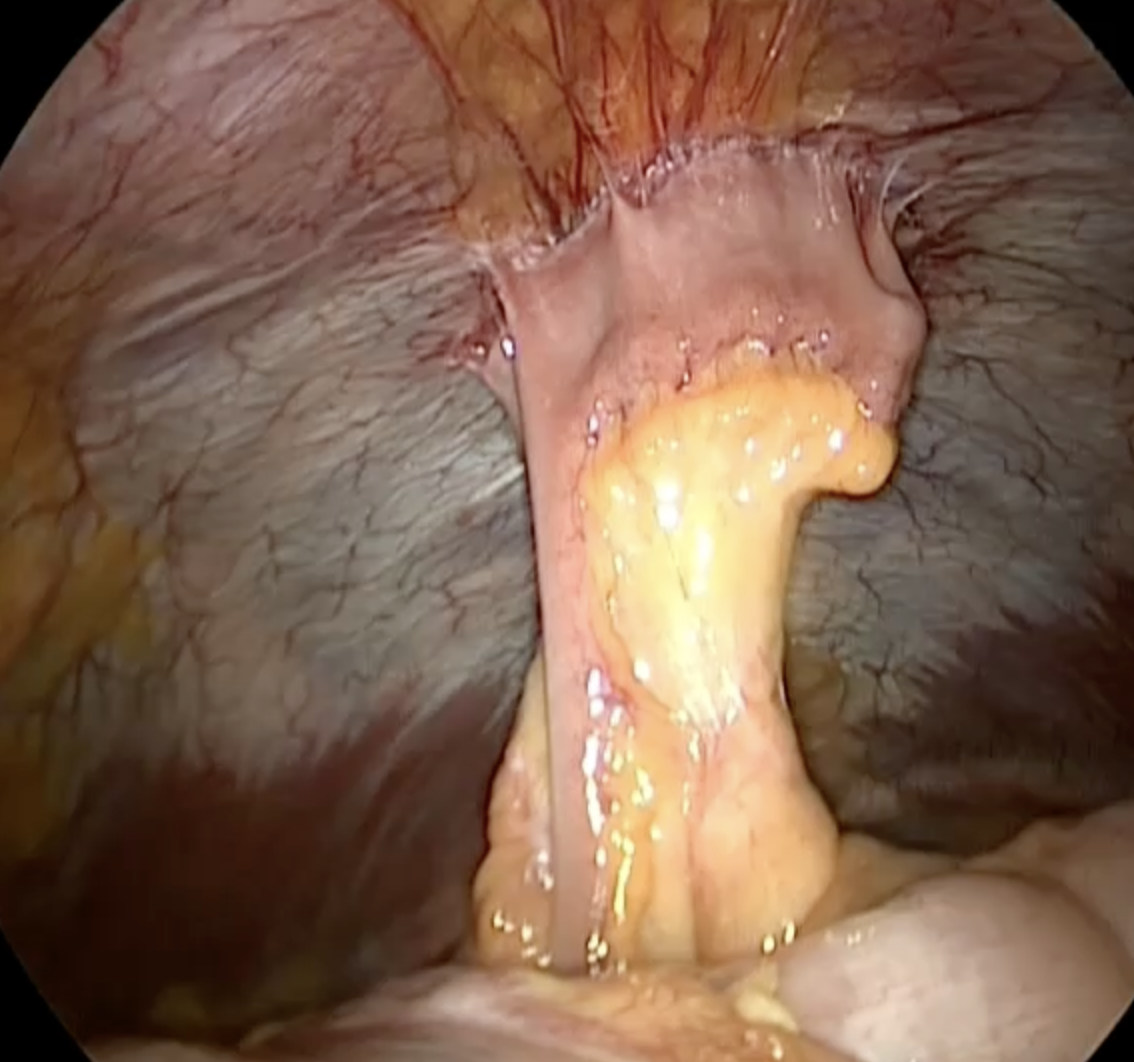 Fig. 3.
Fig. 3.Umbilical hernia seen from vNOTES.
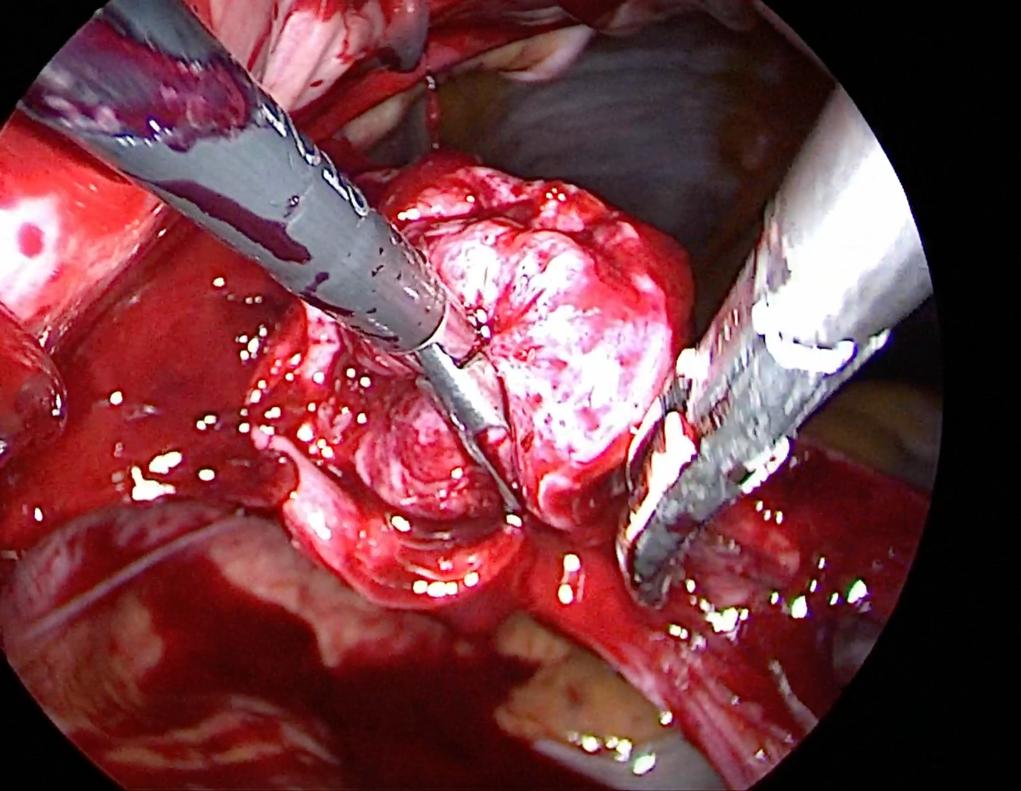 Fig. 4.
Fig. 4.vNOTES hysterectomy, the first step.
Raquet et al. [23] reported their initial experience in the usage of vNOTES for the treatment of benign gynecologic diseases. In a group of 32 patients who underwent the vNOTES procedure, no one required conversion to laparotomy or conventional laparoscopy. Although the vNOTES allows the management of the adnexal pathologies, the authors observed limitations of the vNOTES procedure, such as their usage in a history of the previous cesarean section and the existence of the large uterus.
Huang et al. [24] compared the safety, feasibility, advantages, as well as disadvantages of vNOTES with conventional vaginal surgery for sacrospinous ligament fixation. They analyzed data from 82 patients, of which 31 underwent vNOTES and 51 underwent conventional vaginal surgery. The authors reported that the two groups had similar general characteristics. There were higher rates of anatomical success and bilateral salpingo-oophorectomy in the vNOTES group than conventional vaginal surgery group. However, there was a shorter postoperative stay in the vNOTES group than in the conventional vaginal surgery group. There were no statistically significant differences in bilateral salpingectomy rate, operation time, colporrhaphy rate, postoperative visual analog scale score, estimated blood loss, hemoglobin decreases at 72 h postoperative, maximum body temperature at 72 h postoperative, complication rate, buttock pain, or Pelvic Floor Impact Questionnaire-7, and Pelvic Floor Distress Inventory Questionnaire-20 scores at 1 year postoperative between two groups of patients
Lu et al. [25] analyzed short-term outcomes of transvaginal vNOTES
procedures for uterosacral ligament suspension in women diagnosed with severe
prolapse. They conducted a retrospective study that included 35 patients with
severe prolapse (
Alay et al. [26] compared the intraoperative characteristics and
surgical outcomes of the classic vaginal hysterectomy, vNOTES sacrocolpopexy, and
vNOTES high uterosacral ligament suspension in the treatment of the symptomatic
apical pelvic organ prolapse. The authors observed shorter mean operative time
for vNOTES sacrocolpopexy, and vNOTES uterosacral ligament suspension in
comparison to the classic vaginal hysterectomy, 46
Interdonato et al. [27] performed a study that included 46 patients who
underwent vNOTES surgery for different gynecological indications, such as myomas
Jung et al. [28] presented the results of the pilot study in which authors compared the operative outcomes between vNOTES and single-port access adnexectomy. The study included 12 women who underwent vNOTES adnexectomy and 55 patients who underwent single-port access adnexectomy. Although the lower postoperative pain score and less required use of analgesic medications postoperatively were observed in the patients who underwent vNOTES, other surgical outcomes were comparable between these two groups.
Karkia et al. [29] evaluated the operative outcomes of the hysterectomy
Tekin et al. [30] reported that the implementation of the vNOTES technique in hysterectomy, myomectomy, diagnostic procedure in gynecology, and the adnexal procedure is feasible (Figs. 5,6), satisfactory and safe. Gündoğdu et al. [31] conducted a study to evaluate the safety and outcomes of the use of spinal anesthesia in the vNOTES procedure. In their study on six patients, there were no observed conversions to laparotomy, or conventional laparoscopy. The authors concluded that the vNOTES procedure could be safely performed under spinal anesthesia. In comparison to the trans-umbilical laparoscopic single-site surgery, the vNOTES technique for hysterectomy showed a shorter operative time, a quicker gas passage by the anus, and a shorter length of hospital stays, with lower pain scores [32]. The vNOTES procedure for hysterectomy offers a patient faster recovery and less postoperative pain. Similar outcomes were observed by Yang et al. [33]. Merlier et al. [34] performed a retrospective cohort study to compare the surgical outcomes of vNOTES hysterectomy and vaginal hysterectomy in outpatient surgery. The study analyzed the outcomes of the 50 vNOTES hysterectomies and 50 vaginal hysterectomies. The authors observed no differences in the surgical characteristics between the two management approaches, except the rates of salpingectomies and adnexectomies which were higher in the vNOTES group. In a study by Kaya et al. [35], authors observed significant surgical differences in women with undescended-enlarged uteri between laparoscopic hysterectomy, and vNOTES hysterectomy. Although there were no differences in age, parity, and body mass index (BMI), a group of vNOTES surgery for hysterectomy authors observed significantly shorter durations of surgery, and hospitalization, as well as a lower VAS score, than in the group who underwent a laparoscopic hysterectomy. On the contrary, in a study by Park et al. [36], it was reported significantly higher postoperative vaginal pain in the women who underwent vNOTES hysterectomy than in women who underwent laparoendoscopic single-site hysterectomy. Badiglian-Filho et al. [37] conducted a retrospective study which include 86 women who underwent hysterectomy with salpingectomy/salpingo-oophorectomy via vNOTES or standard laparoscopic access. They compared the main outcomes of these two procedures. The authors reported that there are no statistically significant differences in age, BMI, the prevalence of smoking, obstetric history, the prevalence of arterial hypertension or diabetes, number of abdominal previous surgeries, menopausal status, or preoperative hemoglobin level in these two groups. Also, the authors observed no statistically significant differences in the mean operative times as well as in the indications for surgery, specific and unspecific surgery complications, conversions to the open surgery, reoperations, need for the blood transfusion, and hospital stay between these two groups.
 Fig. 5.
Fig. 5.Endo bag extraction of ovarian dermoid cyst.
 Fig. 6.
Fig. 6.vNOTES cystectomy on the left side (on the right side, the normal ovary).
In addition, the vNOTES procedure takes its place in the ovarian cystectomy. Baekelandt [38] reported a series of 15 patients who underwent transvaginally ovarian cystectomy for removing benign ovarian cysts. The authors reported the successful ovarian cystectomy in all patients without need for the conversions to standard laparoscopy, as well as no complications. In all of these patients, vNOTES ovarian cystectomy was performed as a fertility-sparing procedure, and no ovariectomies were performed. The authors concluded that benign ovarian cysts can be managed by the vNOTES procedure. Huang et al. [39] analyzed retrospectively the 296 patients to compare the surgical outcomes of the vNOTES ovarian cystectomy and conventional laparoscopy ovarian cystectomy. The authors reported significantly lower visual analog scale scores in the group of patients who underwent of vNOTES procedure. Hence, the cosmetic scores were significantly higher in the vNOTES group. The time of flatus and postoperative stay was shorter in patients who underwent the vNOTES procedure. However, there were no significant differences between the two groups in the estimated blood loss, operation time, postoperative hemoglobin decreases at 48 h, hospital costs as well as maximum body temperature in 48 h after surgery.
Ameta-analysis on a set of limited studies showed that vNOTES hysterectomies in comparison to conventional laparoscopy have lower operation time, lower estimated blood loss, and shorter hospital stay [39, 40].
Yang et al. [41] settled a meta-analysis that included the clinical trials with 1340 patients which compare vNOTES and traditional laparoscopy risk of postoperative complications, as well as the pain on the first, second, and third postoperative day, risk of intraoperative complications, the duration of surgery time needed for full recovery, and hospital stay. The authors observed no statistical differences in the risk of intraoperative, as well as the postoperative complications between vNOTES and traditional laparoscopy. Also, there was the lower pain score was lower in vNOTES procedure first, second, and third postoperative day, compared to the traditional laparoscopy. According to the results observed in this meta-analysis, the vNOTES procedures are recommended for women who had adnexectomy, cholecystectomy, and/or appendectomy (Table 1, Ref. [1, 4, 12, 13, 14, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42].
| Study | vNOTES using |
| Jegaden et al. [12], review, 2023. | vNOTES are used as an ovarian drilling surgical procedure in patients with the dysovulatory polycystic ovarian syndrome. |
| Baekelandt [13], stepwise explanation of the surgical technique, 2023. | vNOTES could be used as mode for the placement of permanent cerclage at the isthmic level of the cervix. |
| Tavano et al. [14], retrospective observational cohort study, 125 patients under 43 years old, 2021. | vNOTES is used as fertility-preserving procedures in salpingectomy for ectopic pregnancy, myomectomy, cystectomy, and unilateral adnexectomy. |
| Karakaş et al. [16], retrospective study, 90 patients, 2022. | vNOTES procedure is feasible and safe method for the treatment of ectopic pregnancy, and the most common emergent state in gynecology. In addition, these procedures are not inferior in comparison to the analog laparoscopic procedures. |
| Ozceltik et al. [17], retrospective study, 21 patients, 2022. | |
| Kaya et al. [18], cross sectional study, 114 patients, 2021. | |
| Baekelandt et al [19], stepwise explanation of technique, 15 patients, 2017. | |
| Ozceltik et al. [20], explanation of technique, 2021. | |
| Lamblin et al. [21], explanation of technique, 2021. | |
| Farah et al. [1], case series, 23 patients, 2023. | vNOTES procedure is feasible and safe method for the management of the uterine prolapse. |
| Liu et al. [22], retrospective case series study, 26 patients, 2019. | |
| Huang et al. [24], retrospective study, 82 patients, 2023. | |
| Lu et al. [25], retrospective study, 35 patients, 2021. | |
| Alay et al. [26], retrospective study, 11 patients, 2021. | |
| Raquet et al. [23], case series, 23 patients, 2023. | vNOTES approach in gynecologic surgery such as hysterectomy, myomectomy, cystectomy are the safe procedures, and with satisfactory surgical outcomes. |
| Interdonato et al. [27], retrospective study, 46 patients, 2022. | |
| Jung et al. [28], retrospective study, 67 patients, 2022. | |
| Karkia et al. [29], case series, 33 patients, 2019. | |
| Tekin et al. [30], retrospective study, 105 patients, 2023. | |
| Gündoğdu et al. [31], case series study, 6 patients, 2022. | |
| Yan et al. [32], retrospective study, 361 patients, 2022. | |
| Yang et al. [33], retrospective study, 86 patients, 2020. | |
| Merlier et al. [34], retrospective cohort study, 56 patients, 2022. | |
| Kaya et al. [35], cross-sectional study, 78 patients, 2022. | |
| Park et al. [36], prospective controlled-trial, 26 patients, 2021. | |
| Badiglian-Filho et al. [37], retrospective study, 151 patients, 2021. | |
| Baekelandt [38], stepwise explanation of surgical technique, 14 patients, 2018. | |
| Huang et al. [39], retrospective study, 296 patients, 2021. | In comparison to the conventional laparoscopy hysterectomy, vNOTES hysterectomy led to the lower operation time, lower estimated blood loss, and shorter hospital stay. |
| Michener et al. [40], meta-analysis included 26 studies, 2021. | |
| Yang et al. [41], systematic review and meta-analysis included 13 studies, 2019. | There are no statistical differences in the risk of intraoperative as well as the postoperative complications between vNOTES and traditional laparoscopy. However, there is the lower pain score in vNOTES procedure in first, second, and third postoperative day in comparison to the traditional laparoscopy. |
| Housmans et al. [42], systematic review and meta-analysis included 6 studies, 2020. | In comparison to the conventional laparoscopic hysterectomy, vNOTES hysterectomy had significantly shorter duration of the operation time, shorter length of stay in hospital as well as lower blood loss. There are no differences in difference in intra and postoperative complications, pain scores at 24 h postoperative, readmission and change in hemoglobin on firs postoperative day. |
| Aharoni et al. [4], retrospective cohort study, 135 patients, 2021. | vNOTES procedure for the hysterectomy with the uterosacral ligament suspension leads to the lower mean operative time, as well as lower mean anesthesia time. On the other hand, it has longer median hospital staying in comparison to the conventional vaginal hysterectomy with the uterosacral ligament suspension. It is observed less estimated blood loss and lower incidences of intraoperative complications and intraoperative ureteral obstruction in vNOTES hysterectomy with uterosacral ligament suspension, comparing to the conventional vaginal hysterectomy with the uterosacral ligament suspension. |
vNOTES, transvaginal natural orifice transluminal endoscopic surgery.
vNOTES procedure present some advantages in comparison to the traditional laparoscopic surgery. The vNOTES procedure gives a surgeon better insight into the identification of the ureter, and accordingly, lowers the risk for injuries to the ureter [42]. In comparison to the conventional laparoscopic procedure, vNOTES had significantly lower values for operation time and length of stay in hospital, as well as lower blood loss. When it compares with the conventional laparoscopic procedures, there is no significant difference in intra and postoperative complications, pain scores at 24 h postoperative, readmission and change in hemoglobin on firs postoperative day [42]. Also, the vNOTES procedure enables a more complete exploration of the pelvic cavity and easier manipulation in cases of the large uterus or adnexal masses than classic vaginal surgery [5, 43, 44]. The vNOTES procedure allows endoscopic surgery when there is an umbilical hernia or previous umbilical surgery the situations where the traditional trocar placement is a disadvantage [45].
When it compares the vNOTES procedure for the hysterectomy with the uterosacral ligament suspension with the conventional vaginal surgery, the vNOTES procedure leads to the lower mean operative time as well as mean anesthesia time. On the contrary, longer median hospital stays to women who underwent conventional vaginal hysterectomy with the uterosacral ligament suspension. The women who underwent vNOTES hysterectomy with uterosacral ligament suspension had less estimated blood loss and lower incidences of intraoperative complications and intraoperative ureteral obstruction, in comparison with the women who underwent conventional vaginal hysterectomy with the uterosacral ligament suspension [4].
Moreover, the vNOTES is safe and suitable procedure in obese women. Mat
et al. [46] conducted the study aimed to assess the feasibility and
efficacy of vNOTES staging surgery in extreme obese patients diagnosed with
early-stage type-1 endometrial cancer. In this study, six extreme obese patients
were included ,with mean BMI of 51.4 kg/m
In addition, the vNOTES give opportunity for the diagnosis of the ascites of the unknown cause. Indeed, studies reported seven patients with ascites of unknown cause. After peritoneoscopy and pathological examination, different pathologies were diagnosed, such as peritoneal carcinomatosis, abdominal tuberculous, ovarian fibroma, ovarian mature cystic teratoma and stomach cancer. One year after vNOTES procedure follow-up, there was no adverse events observed in these patients. In these patients, the vNOTES procedure for the early differentiative diagnostic tool in some gynecologic disease is suitable [47].
Although there is a lack in the studies about the long-terms’ outcomes of the vNOTES procedures, there are pilot studies about long-terms outcomes and recurrences after vNOTES. Lu et al. [48] conducted a retrospective cohort study to analyze the results of mesh exposure and prolapse recurrence after vNOTES procedure for sacrocolpopexy, after more than 24 months of postoperative follow-up. In this study, the 55 women were follow-up for a duration period of 24 and 46 months. In the study, the incidence of the prolapsed recurrence was 3 of 55 (5.5%) and the total incidence of mesh exposure was 3 of 55 (5.5%) [48].
Although there are numerous advantages of the vNOTES procedures in comparison with the classic vaginal surgery, and or classic laparoscopic procedures, there are some limits to the vNOTES procedure. There is a consensus about contraindications for the vNOTES performing, such as rectovaginal endometriosis and a previous pelvic radiotherapy [49, 50]. There are limited data about the safety of the vNOTES in patients with a history of previous surgery, but there if are severe adhesion and/or obliteration in the cul-de-sac, vNOTES are a contraindication due to the higher risk for pelvic organ injury, especially rectum [10, 51, 52].
Lastly, most of the studies that analyzed the outcomes of the vNOTES approach in the different gynecological procedures are pilot studies, which include a relatively small number of patients. There are commonly retrospective, observational studies and there is a lack of randomized, control trial studies. Also, the follow-up period of most prospective studies is about one year, which is not enough for the estimation of the risk for rare surgical complications and long-term surgical outcomes.
The vNOTES procedures are safe, reproducible, and feasible in contemporary gynecologic surgery. They have some advantages in comparison to conventional laparoscopy surgery. Nevertheless, further studies on a large number of patients should analyze the long-term outcomes of the vNOTES procedure, comparing the outcomes of the vNOTES and conventional laparoscopy procedures.
AT, RS, MA, ZS, ĐT designed research study. AT, RS, MA, AM analyzed data. AT, MA, RS wrote and revised the manuscript. All authors contributed to editorial changes in the manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work. All authors read and approved the final manuscript.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest. Andrea Tinelli is serving as one of the Editorial Board members/Guest editors of this journal. We declare that Andrea Tinelli had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Michael H. Dahan.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.