
- Academic Editor
Background: The incidence and mortality of endometrial cancer (EC) have increased in recent years. The incidence of psychological disorders induced by EC is also increasing. Fluoxetine is a prescribed antidepressant drug for managing mental illnesses. We retrospectively explored the effect of fluoxetine intervention on symptom checklist 90 (SCL-90), quality of life, Hamilton anxiety scale (HAMA), Hamilton depression scale (HAMD), and nursing satisfaction in patients with EC undergoing surgery. Methods: One hundred patients with EC undergoing hysterectomy were selected. Based on the different clinical nursing intervention methods, the patients were categorized into a control group (n = 50) and an intervention group (n = 50). Patients in the control group were provided routine care, including nutrition guidance, basic psychological nursing, pain care, rehabilitation exercise, and complication prevention, whereas patients in the intervention group were only treated with fluoxetine based on routine nursing protocols. The differences in SCL-90, quality of life, HAMA, HAMD scores, and nursing satisfaction between the two groups were observed. Results: No significant difference was observed in the SCL-90, quality of life score, HAMA, and HAMD between the two groups before treatment. After treatment, all items in the intervention group differed from those in the control group. The SCL-90 scores of the intervention group decreased after treatment, and all subscales of SCL-90 in the intervention group were reduced. All dimensions of quality of life were elevated in the control group after treatment. The HAMA and HAMD scores of patients in the intervention group declined considerably after treatment. Conclusions: Fluoxetine intervention effectively improved the quality of life of patients with EC undergoing hysterectomy, and ameliorated signs of anxiety and depression, thus promoting the recovery of the disease.
Endometrial cancer (EC) is a malignancy of the endometrium that severely threatens the life and health of patients [1, 2]. This cancer mostly occurs in postmenopausal women residing in high-income countries with high obesity rates. Clinical manifestations of EC include irregular vaginal bleeding [3]. Treatment methods primarily used in EC mainly include surgery, radiotherapy, chemotherapy, and endocrine therapy [4]. Total hysterectomy is usually administered in clinical settings. Even though this procedure can prolong the survival of patients, because of the loss of normal uterine physiological functions, patients are prone to depression and anxiety after the surgery, which severely affects their postoperative rehabilitation or may even lead to several negative emotions, such as anxiety, depression, and annoyance [5, 6]. These negative feelings that occur post-surgery are closely correlated with the prognosis of patients [7]. Thus, how eliminating negative emotions after surgery has become a key task in postoperative care [8, 9]. Corresponding intervention measures are of great significance for reducing mood fluctuations in patients with EC post-surgery and improving their quality of life.
The pathogenesis of depression is complex, and changes in the expression of neurotransmitters have been proven to be an important mechanism in depression [10]. 5-hydroxytryptamine (5-HT) is a neurotransmitter in the pituitary gland and hypothalamus that is closely associated with behavior and emotion [11]. When the level of 5-HT is high, it tends to induce excitement. At low levels, 5-TH can cause people to develop symptoms of anxiety and depression symptoms. Fluoxetine, as a clinical drug used for the treatment of depression, can prolong and increase synaptic 5-HT levels and play the role of an antidepressant [12]. Fluoxetine is a type of so-called selective serotonin reuptake inhibitor with recognized clinical efficacy and safety [13]. Fluoxetine is a Food and Drug Administration (FDA)-approved medicine for obsessive-compulsive, panic disorder, and premenstrual dysphoric disorders [14]. Therefore, this investigation focuses on the clinical efficacy of fluoxetine in ameliorating depression.
Several evaluation systems are applied in assessing the mental state of patients. Symptom Checklist 90 (SCL-90) is a broad measurement of the severity of psychological symptoms [15]. Hamilton anxiety scale (HAMA) and Hamilton depression scale (HAMD) are both commonly applied in monitoring mood [16]. We focus on the change in assessment systems in patients with EC and compare the discrepancy among the various items. The study included patients with EC and categorized them into a control group and an intervention group to study the post-surgery effect of fluoxetine on patients. The clinical effect of fluoxetine on patients with EC was reflected by SCL-90, HAMA, HAMD, and quality of life score.
One hundred patients with EC who underwent treatment at the First Hospital of Xingtai between April 2021 and September 2022 volunteered in this research. All patients met the following criteria: diagnosed with EC by pathological examination; underwent hysterectomy without surgical contraindications; had complete clinical data; had clear consciousness and no communication barriers. Patients with other liver and kidney diseases, heart and brain diseases, mental diseases, other tumors, and a history of surgery were ineligible. The patients had no clinical manifestations of depression before the surgery but showed symptoms of depression after the surgery. The clinical manifestation of depression refers to the third edition of Chinese diagnostic criteria for mental disorders [17]. These volunteers were categorized into a control group (n = 50) and an intervention group (n = 50) based on different nursing design plans. This grouping method was based on patient preference, and patients who were unwilling to take medication were assigned to the control group. This study was retrospective and performed in line with the principles of the Declaration of Helsinki. The Ethics Committee of the First Hospital of Xingtai approved this plan, and the patients were informed and signed the consent form.
The routine postoperative care included dietary care, basic psychological care, pain management, rehabilitation exercise, and complication prevention. (1) Nutritional support involves the guidance and supervision of patients’ daily diet, the formulation of scientific diet conditioning plans for patients, and the reasonable arrangements for the daily nutritional intake of patients. (2) Psychological care requires positive and face-to-face communication with patients and their families every day, attending to each patient’s psychological feelings of patients promptly, helping patients resolve negative emotions, and helping them get adequate sleep. The attention of patients was diverted and pain perception was alleviated by positive guidance and psychological recommendations. Familial pressure on patients was reduced by training and guiding their family members. (3) Pain management involves asking patients about their pain every day and administering active treatment to help them alleviate their pain. In addition, patients were also guided to shift their focus to a pain alleviation method. (4) Rehabilitation nursing includes massage of lower limbs, increasing limb activity, and rehabilitation training guidance of the pelvis. (5) Complication care includes informing the patient of possible complications after surgery and managing them promptly and appropriately when they occur.
All patients in the control group and the intervention group were administered active treatment methods, including psychotherapy and positive self-adjustment. Patients in the intervention group were administered fluoxetine (J20170022, Bourgoin Jallieu, Isere, France) twice a day based on the prementioned active treatment methods. The dose of fluoxetine was 20 mg at each instance of administration. The dose was adjusted after 2 weeks of dosing. The whole treatment course was of two months.
After the 2-month treatment, the scale was assessed independently for each participant. Before the evaluation, the staff explained the general scoring method and requirements. Participants provided self-ratings that were not influenced by anyone and filled the forms out independently. At the end of the assessment, the scales were checked and recorded by clinicians.
The degree of depression of patients was evaluated using the HAMD score [18]. The HAMD score is the sum of the scores of 24 items. Most HAMD projects adopt a five-level scoring method with 0–4 points, and a few projects adopt a three-level scoring method with 0–2 points. The criteria for each level were as follows: 0 = none; 1 = mild; 2 = medium; 3 = severe; 4 = extremely severe. The scoring criteria of the three-level scoring method were as follows: 0 = none; 1 = mild to moderate; 2 = severe. When the score was greater than or equal to 8, it implies that there is depression, and the higher the score, the more serious the situation is.
The anxiety symptoms of patients were estimated using the HAMA score [19]. Higher the HAMA score, the more severe the anxiety symptoms. All HAMA items were scored on a five-point scale from 0 to 4. The criteria for each level were: 0 = no symptoms; 1 = light; 2 = medium; 3 = heavy; 4 = extremely heavy.
Somatization, compulsion, interpersonal sensitivity, depression, anxiety, terror, paranoia, and psychosis constitute of the SCL-90 scoring system [20]. SCL-90 has nine 9 categories, and each category has some items. Each patient scored the item according to five grades. In the SCL-90 table, each item was considered negative if it is less than 2, and positive if the value was greater than or equal to 2. In this study, the average value of positive items in each category was counted. The lower the level, the better the conditions.
Quality of life was assessed using the quality of life questionnaire (QLQ-C30) in a questionnaire survey [21]. Some items are graded on a scale of 1–7, whereas others were graded on a scale of 1–4 and converted into values between 0 and 100.
The values were analyzed using the SPSS 20.0 statistical software (IBM Corp.,
Armonk, NY, USA). t-test was conducted to analyze the measurement data,
and
This study collected the demographic information, marital status, education, and
childbearing age of all recruited patients. As documented in Table 1, no
significant discrepancy was observed between the control group and the
intervention group (p
| Factors | Control (n = 50) | Intervention (n = 50) | p value | |
| Age (years) | 45.68 |
45.72 |
0.982 | |
| BMI (kg/m |
24.02 |
24.76 |
0.188 | |
| Marriage | 0.182 | |||
| Yes | 47 (94.00%) | 43 (86.00%) | ||
| No (spinsterhood, divorce, widowed) | 3 (6.00%) | 7 (14.00%) | ||
| Education | 0.072 | |||
| Secondary or below | 21 (42.00%) | 30 (60.00%) | ||
| Post-secondary education | 29 (58.00%) | 20 (40.00%) | ||
| Age of childbearing (years) | 0.646 | |||
| 47 (94.00%) | 48 (96.00%) | |||
| 3 (6.00%) | 2 (4.00%) | |||
Note: Data are presented as mean
In this research, we estimated the psychological status of patients using the
SCL-90 rating system. In this rating method, all aspects were evaluated to
evaluate the mental health status of patients. All patients showed no obvious
difference in the various parameters before
treatment (p
 Fig. 1.
Fig. 1.Detection of symptom
checklist 90 (SCL-90). (A) The discrepancy in the SCL-90 score before treatment.
(B) The difference in SCL-90 score after treatment. **p
| Factors | Control (n = 50) | t | p | Intervention (n = 50) | t | p | F | p | ||
| before | after | before | after | |||||||
| Somatization | 5.14 |
5.16 |
–1.06 | 0.916 | 5.86 |
3.42 |
4.73 | 15.17 | ||
| Obsessive-compulsive symptoms | 4.90 |
4.52 |
0.82 | 0.415 | 4.98 |
3.52 |
4.17 | 7.23 | 0.008 | |
| Interpersonal relationships | 5.08 |
4.98 |
0.17 | 0.869 | 5.60 |
3.50 |
4.57 | 8.89 | 0.004 | |
| Depression | 5.98 |
7.06 |
–1.77 | 0.083 | 6.92 |
2.26 |
11.11 | 140.97 | ||
| Anxiety | 6.18 |
6.92 |
–1.26 | 0.215 | 7.04 |
1.80 |
15.10 | 180.57 | ||
| Hostility | 2.42 |
1.80 |
3.97 | 2.38 |
1.46 |
8.67 | 8.23 | 0.005 | ||
| Terror | 5.66 |
5.48 |
0.32 | 0.754 | 5.78 |
1.94 |
9.05 | 87.40 | ||
| Paranoia | 5.64 |
5.06 |
1.29 | 0.204 | 5.86 |
2.90 |
6.47 | 55.71 | ||
| Psychoticism | 4.92 |
4.72 |
0.60 | 0.551 | 4.75 |
2.90 |
5.46 | 48.47 | ||
Note: SCL-90, Symptom Checklist 90. Data are presented as mean
Six aspects were performed to assess the quality of life of patients. No
difference was observed in all aspects before treatment (p
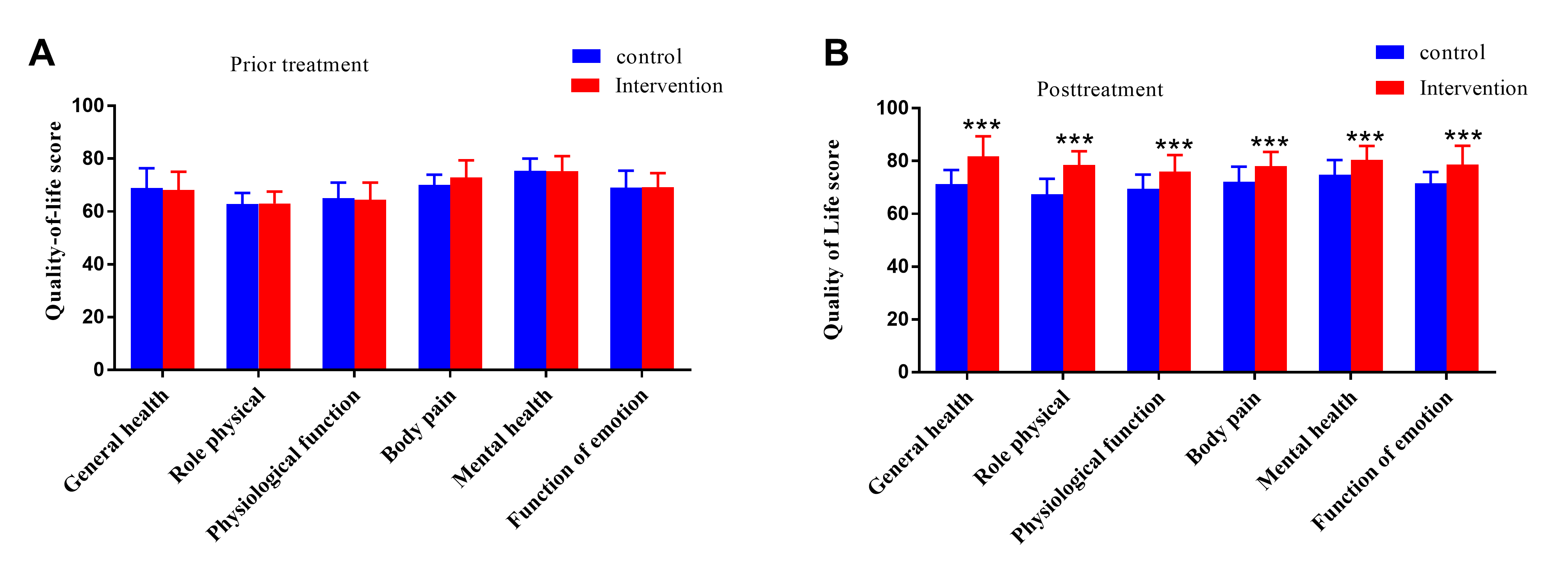 Fig. 2.
Fig. 2.Comparison of the quality-of-life score. (A) No difference in
quality-of-life scores prior treatment. (B) All dimensions were elevated in the
intervention group after treatment. ***p
| Factors | Control group (n = 50) | t | p | Intervention group (n = 50) | t | p | F | p | ||
| before | after | before | after | |||||||
| General health | 68.84 |
71.28 |
–1.82 | 0.075 | 68.12 |
81.82 |
–9.39 | 64.32 | ||
| Role physical | 62.84 |
67.48 |
–4.97 | 63.00 |
78.58 |
–15.66 | 103.00 | |||
| Physiological function | 65.02 |
69.56 |
–3.89 | 64.44 |
76.08 |
–8.87 | 31.87 | |||
| Body pain | 70.07 |
72.18 |
2.51 | 0.016 | 72.90 |
78.16 |
–4.79 | 76.90 | ||
| Mental health | 75.34 |
74.86 |
0.41 | 0.687 | 75.22 |
80.46 |
–4.09 | 27.05 | ||
| Function of emotion | 69.00 |
71.56 |
–2.10 | 0.041 | 69.22 |
78.66 |
–8.14 | 36.37 | ||
Note: Data are presented as mean
The HAMA score and HAMD score were decreased in the intervention group than
control group after the treatment (p
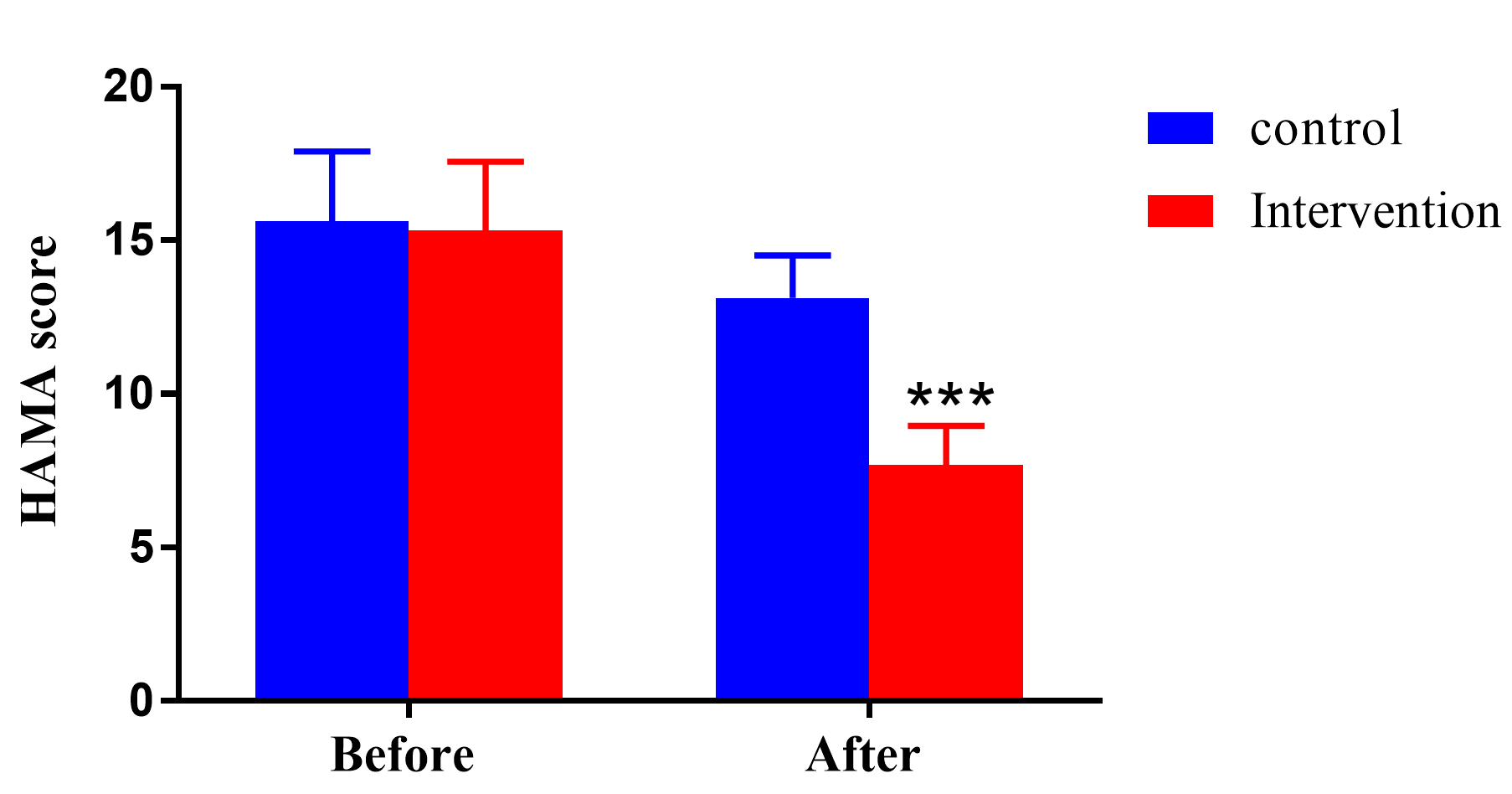 Fig. 3.
Fig. 3.The Hamilton anxiety scale (HAMA) score in the two groups showed
no difference before treatment, while it decreased in the intervention group
after treatment. ***p
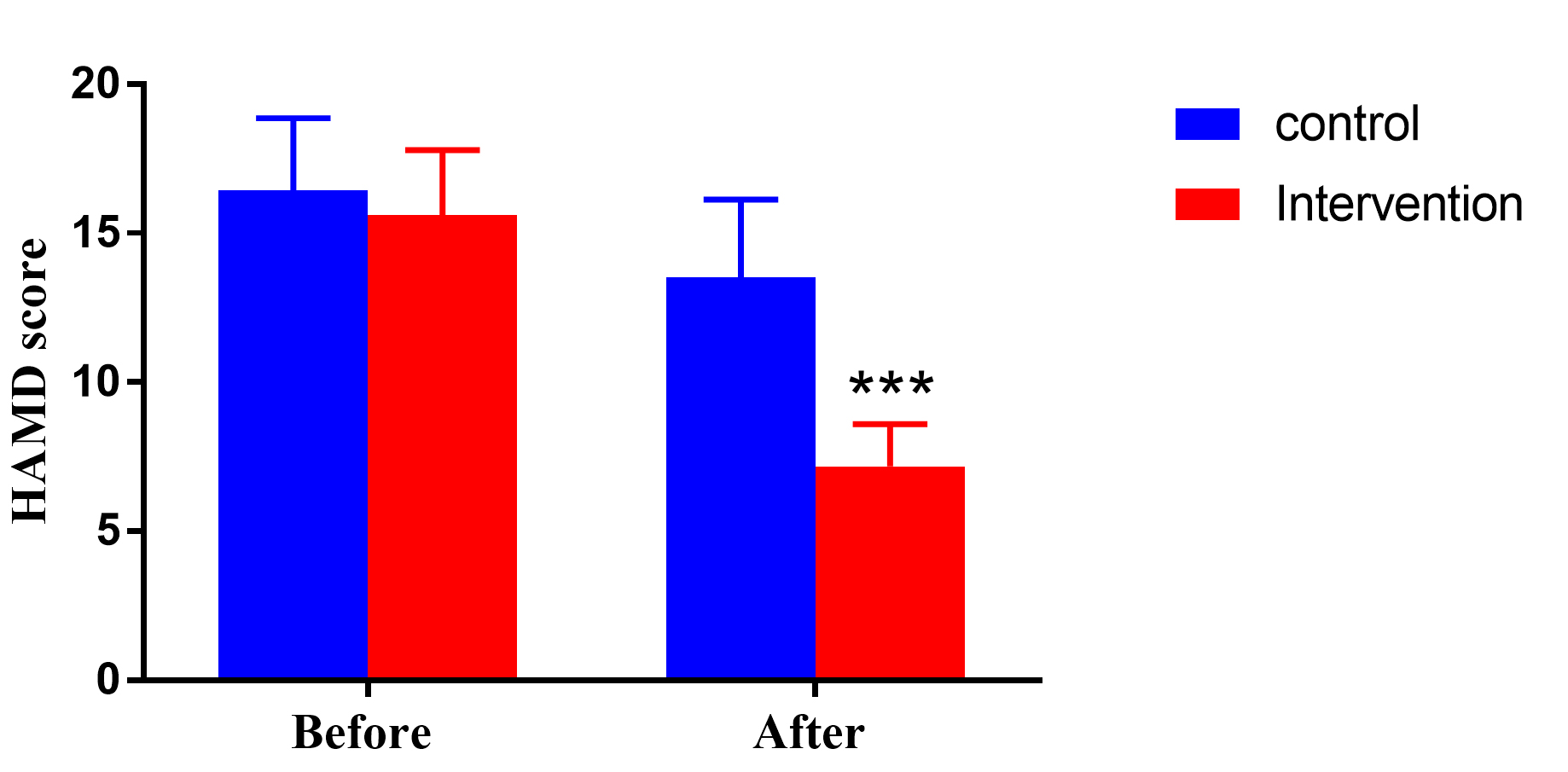 Fig. 4.
Fig. 4.The depression degree was reflected by the difference in
Hamilton depression scale (HAMD). ***p
| Factors | Control (n = 50) | t | p | Intervention (n = 50) | t | p | F | p | ||
| before | after | before | after | |||||||
| HAMA | 15.62 |
13.12 |
6.20 | 15.32 |
7.68 |
20.40 | 421.15 | |||
| HAMD | 16.44 |
13.52 |
5.90 | 15.60 |
7.18 |
22.02 | 229.10 | |||
Note: HAMA, Hamilton Anxiety Scale; HAMD, Hamilton Depression Scale. Data are
presented as mean
Nursing satisfaction was divided into five grades. As shown in Table 5, the
total satisfaction rate in the intervention group was elevated compared with the
control group (p
| Factors | Control (n = 50) | Intervention (n = 50) | p value | |
| Very satisfied (n/%) | 17 (34.00) | 22 (44.00) | 5.01 | 0.025 |
| Satisfied (n/%) | 16 (32.00) | 20 (40.00) | ||
| Generally satisfied (n/%) | 8 (16.00) | 6 (12.00) | ||
| Unsatisfied (n/%) | 9 (18.00) | 2 (4.00) | ||
| Total satisfaction rate (n/%) | 41 (82.00) | 48 (96.00) |
EC has shown a continuous and rapid growth trend among gynecological tumors in recent years. The condition severely affects the overall physical and psychological health of women, making patients very prone to negative emotions and affecting their quality of life [22, 23]. Psychological factors are inseparable from the process of the disease [24]. When the body is in a state of stress, there will be negative emotions, such as anxiety and tension, are bound to occur. These negative emotions also weaken the immune function of the body, thus reducing its ability to resist external invasion. It leads to poor prognosis for patients and is not conducive to their quality of life in the future [25]. Many women with cancer experience severe anxiety and depression after undergoing surgical resection [26]. Therefore, it is necessary to adopt effective nursing measures to eliminate the negative emotions of patients and improve life quality.
Depression medication is a commonly used choice in clinical practice. Fluoxetine is an antidepressant and anxiety drug and a potent and highly selective serotonin reuptake inhibitor [27]. Oral fluoxetine is completely absorbed in the gastrointestinal tract and not affected by food intake or the combination of antacids. It is distributed rapidly and widely distributed in various tissues. Fluoxetine is one of the oldest drugs applied for managing some mental illnesses, like major depressive disorder, hypochondria, anxiety, bulimia nervosa, and obsessive-compulsive disorder [28]. A systematic review reported that fluoxetine is effective in treating psychological symptoms in patients with premenstrual and infertility disorders [29]. Another investigation by Alenko et al. [30] indicates that an 8-week treatment with fluoxetine helps reduce psychological symptoms in patients with major depressive disorder. In addition, the peripheral changes may influence the central nervous system, thus inducing depression [31, 32]. The receptors of fluoxetine are widely distributed in the peripheral nervous systems, thus, fluoxetine may affect depression by regulating peripheral effects [33]. In an animal trial, fluoxetine is proven to exert antidepressant and analgesic effects [34]. The analgesic effects of fluoxetine may also enhance its lowering effect on depression. Thus, this research focused on the efficacy of fluoxetine in patients with EC.
The SCL-90 phobic anxiety scale is a valid measure of psychiatric manifestations and extensively applied in psychogenic research [35]. This scoring system is utilized for patients with frontotemporal depression, affective disorders, and mental manifestations of allergic rhinitis [36, 37, 38]. This current research reported that the SCL-90 score was decreased after treatment and the intervention group had a lower level than the control group, suggesting that fluoxetine could improve the mental health status of patients. In the control group, only hostility was decreased, while in the intervention group, all parameters, including SCL-90, declined obviously, reflecting that fluoxetine improved the psychosomatic symptoms. Then, we further estimated the quality of life through QLQ-C30. After treatment, all subscales in the QLQ-C30 scale were elevated in the intervention group relative to that in the control group, providing that fluoxetine could improve life quality and accelerate the rehabilitation process. Thirdly, the HAMA and HAMD systems were conducted to assess mental sickness. After treatment, the HAMA and HAMD scores of the two groups were decreased, and the scores in the intervention group were lower, indicating that fluoxetine in the treatment of depression can not only effectively improve depression but also significantly relieve anxiety. Finally, nursing satisfaction was improved in the intervention group, indicating that the combination of fluoxetine and routine nursing is more easily accepted and welcomed by patients.
Totally, fluoxetine treatment along with routine care could effectively reduce the overall psychological complaints, ameliorate anxiety and depression, and reduce the pain of patients with EC, thus improving their quality of life. This method of aftercare for patients with EC undergoing hysterectomy is functional and worth adopting in clinical settings.
EC, endometrial cancer; HAMA, Hamilton anxiety scale; HAMD, Hamilton depression scale; QLQ-C30, quality of life questionnaire; SCL-90, symptom checklist 90; 5-HT, 5-hydroxytryptamine.
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by WJY, LLW, JW and LW. The first draft of the manuscript was written by NS and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. All authors contributed to editorial changes in the manuscript. All authors have participated sufficiently in the work to take public responsibility for appropriate portions of the content and agreed to be accountable for all aspects of the work in ensuring that questions related to its accuracy or integrity.
This study was performed in line with the principles of the Declaration of Helsinki. The Ethics Committee of the First Hospital of Xingtai approved this plan (approval number: 2020-015), and the patients were informed and signed the consent form.
Not Applicable.
This research was funded by Medical Science Research Project of Hebei Province, grant number: 20232008.
The authors declare no conflict of interest.
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.