


1 Department of Obstetrics and Gynecology, Beijing Anzhen Hospital, Capital Medical University, 100029 Beijing, China
Abstract
Background: To investigate the value of the artificial intelligence cervical cancer screening system TruScreen (TS) in high-risk human papillomavirus (HPV)-positive patients in a clinical setting. Methods: Three hundred and eighteen patients positive for high-risk HPV in the gynecological clinic of our hospital from May 2020 to June 2021 were analyzed retrospectively. Colposcopy was performed when it was clinically indicated. Results: Among the 318 patients, 203 were TS negative and 115 were TS positive, of whom 84 were referred for colposcopy and possible biopsy. Among the 318 patents, 74.53% (237/318) had a single type of HPV infection, and 25.47% (81/318) had more than two types of HPV infection. In terms of HPV types, the top 5 types were 52, 58, 51, 56 and 16. HPV52 accounted for 27.4% (87/318), followed by HPV58, accounting for 17.30% (55/318). A total of 84 patients underwent colposcopy. The negative predictive values of TS and thinprep cytology test (TCT) screening for cervical cancer and precancerous lesions were 33.33% and 16.90%, respectively. The positive predictive values were 88.41% and 92.31%, respectively. The sensitivity was 85.92% and 16.90%, respectively. The specificity was 38.46% and 92.31%, respectively. Among 251 non-16/18 high-risk HPV-positive patients with TCT negative intraepithelial lesion or malignancy (NILM) 49 underwent colposcopy. The positive predictive value of TS for cervical cancer and precancerous lesions was 84.78% and the sensitivity was 92.86%. Conclusions: This study demonstrated that in a clinical setting, TS had a better sensitivity than TCT in cervical cancer screening, but less specificity than TCT. In the non-16/18 HPV-positive population with TCT NILM, TS screening can be considered as having potential for clinical management. However, the current research sample size was small, and further research needs to be performed with a larger sample size.
Keywords
- cervical cancer screening
- HPV
- TruScreen
- liquid based cytology
- triage
Cervical cancer is a common malignant tumor which seriously threatens the lives and health of women worldwide. The Global Cancer Report statistics in 2018 showed that the number of new cases of cervical cancer each year is about 570,000 and the number of deaths is about 311,000. The yearly number of new cases of cervical cancer in China accounts for about 25% of the world’s total, being approximately 131,500 cases [1]. However, the current rate of cervical cancer screening in China is only 19% [2], which is far from the accepted target of 90% of the population required for cervical cancer prevention and treatment [3]. Therefore, the efforts are underway to find alternative, reliable, cost-effective techniques to enhance screening coverage. At present, the traditional screening methods are liquid based cytology and human papillomavirus detection. Low sensitivity of liquid-based cytology technology may result in a missed diagnosis, and its success depends on the experience and technical level of the film reader [4]. The sensitivity for the preliminary screening of human papillomavirus (HPV) detection is high, but the results contain a large number of “transient” infected people, resulting in low specificity [5]. The appearance of an artificial intelligence cervical cancer screening system (TruScreen, TS) as a new screening method brings new technology to cervical cancer screening [4].
The principle of TS is a real-time artificial intelligence screening technology based on millions of data points from a standardized histopathological sample database. It transmits low-intensity light signals and electrical pulses to stimulate the cervix when it contacts the surface of the cervix through nano photoelectric biosensors. Based on the changes in tissue optical properties and impedance information caused by pathophysiological changes of cervical cancer and precancerous tissues, the system collects the original data information of photoelectric signal feedback, which will be filtered, sampled and computer analyzed to extract the most valuable data information for tissue classification. It is then compared with the standard histopathologic data in the system database through the unique core algorithm to simulate the discriminating process of top pathologists, identify and classify cervical tissues, and distinguish between abnormal and normal tissue. This technique can not only detect the epithelial tissue of the cervical surface, but also penetrate into the basal and stromal layers of the cervical epithelial tissue to detect changes in the deep layer. The technique focuses on cell morphology and tissue change. Because the TS technique does not require sampling and only obtains parameters through scanning, gynecologists can operate independently. TS has the advantages of being a simple procedure, objective, immediate and non-invasive. These attributes have attracted the attention of scholars to perform further research on the use of TS in cervical cancer screening [4].
According to the “Expert Consensus on Issues Related to Cervical Cancer Screening and Abnormal Management in China” published in the Chinese Clinical Journal of Obstetrics and Gynecology in 2017, if cytology and HPV combined screening is adopted, cytologically negative patients with HPV16/18 infection can be referred for colposcopy, and cytologically negative patients with non-16/18 infection are recommended to undergo repeat testing in 1 year. However, the clinical management of patients with non-16/18 HPV infection is more difficult [6]. The purpose of this study is to explore the advantages and disadvantages of TS versus traditional screening techniques, and whether TS technology can be considered as a basis for stratified management of non-16/18 HPV positive patients with thinprep cytology test (TCT) negative intraepithelial lesion or malignancy (NILM).
Clinical data was collected for 318 high-risk HPV patients who underwent cervical screening at the Obstetrics and Gynecology Clinic of Anzhen Hospital from May 1, 2020 to June 30, 2021. The reasons for seeking medical treatment included routine health examination and gynecological diseases (including abnormal leucorrhea, vulva pruritus, contact bleeding, abnormal uterine bleeding, etc.). The exclusion criteria: (1) acute vaginitis; (2) acute cervicitis; (3) reproductive tract bleeding status; (4) within 3 months postpartum; (5) cervical coning/physical therapy within 6 months. The subjects were referred for colposcopy under the following conditions: (1) HPV16/18 positive; (2) TS positive; (3) TCT was low-grade squamous intraepithelial lesion (LSIL) or worse; (4) TCT was atypical squamous cells of undetermined significance (ASCUS) and HPV positive; (5) persistent HPV infection greater than 1 year. Patients referred for colposcopy were biopsied under colposcopic guidance, and the biopsy tissue was sent for histological examination (Fig. 1). The procedures were performed by different physicians, all of whom received formal training in the procedure and were not aware of other test results for these patients. This study was reviewed by the Ethics Committee of Beijing Anzhen Hospital, Capital Medical University (Batch number: 2021113X).
 Fig. 1.
Fig. 1.Clinical data collection procedure. TCT, thinprep cytology test; HPV, human papillomavirus; TS, TruScreen; ASCUS, atypical squamous cells of undetermined significance.
HPV typing was detected by fluorescent Polymerase Chain Reaction (PCR) (Shanghai ZJ Bio-Tech Co., Ltd., Shanghai, China). The study patients were examined using the TS cervical cancer screening facility (developed by Truscreen Pty Ltd., Sydney, Australia). The operator used disposable photoelectric sensors to align at least 20 cervical surface sites in the order specified in the equipment manual. The results were obtained in real time. The results were defined as: (1) normal (no abnormal cervical cells found) or (2) abnormal (abnormal cells found in the cervix).
The TS result was defined as: (1) normal (no abnormal cervical cells found) or (2) abnormal (abnormal cells found in the cervix).
TCT negative refers to cytology
For the interpretation of examination results, biopsy pathological results LSIL or worse were defined as “abnormal”. Referring to the consensus of the American College of Pathologists and the American Society for Colposcopy and Cervical Pathology, the pathological results were divided into the following three types: (1) normal (including normal squamous epithelium, normal columnar epithelium, and chronic cervicitis); (2) cervical intraepithelial neoplasia, including low-grade cervical intraepithelial neoplasia (LSIL, i.e., primary CIN1), high-grade cervical intraepithelial neoplasia (HSIL, i.e., primary CIN3 and partial CIN2); (3) early invasive carcinoma and invasive carcinoma. The final pathological diagnosis was determined by an experienced pathologist who was not aware of the subject’s other findings. The classification of pathological findings included inflammation, CIN1, CIN2, CIN3, and cervical cancer.
Statistical analysis was performed using SPSS 23.0 (IBM Corp., Armonk, NY, USA) and Free Statistics analysis platform Description of rate was performed by SPSS 23.0. The sensitivity, specificity, positive predictive value, negative predictive value and area under curve (AUC) of each screening method were performed using R Statistical Software (Version 4.2.2, http://www.R-project.org, The R Foundation) and Free Statistics analysis platform (Version 1.8, FreeClinical Medical Technology Co., Ltd., Beijing, China).
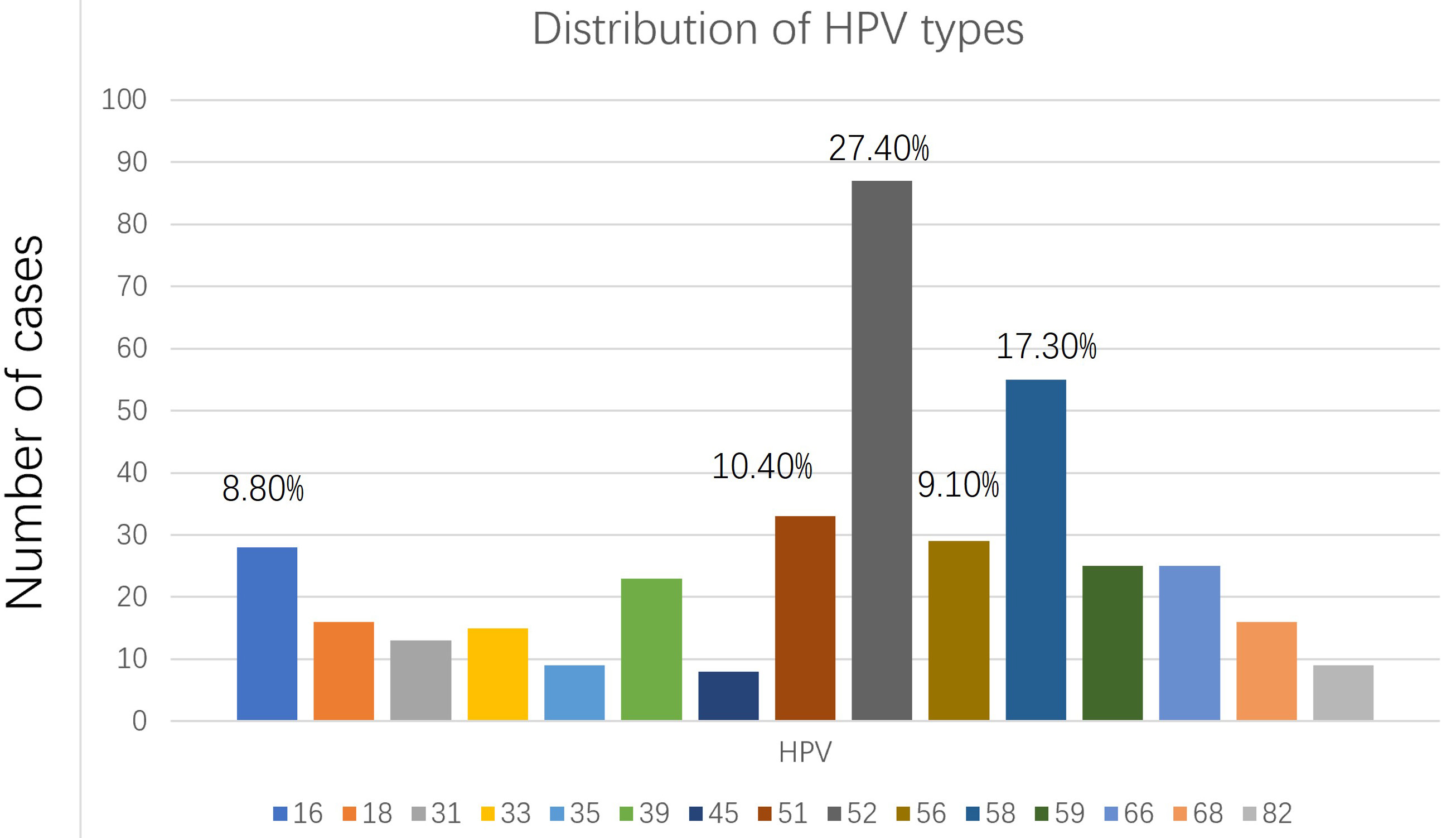
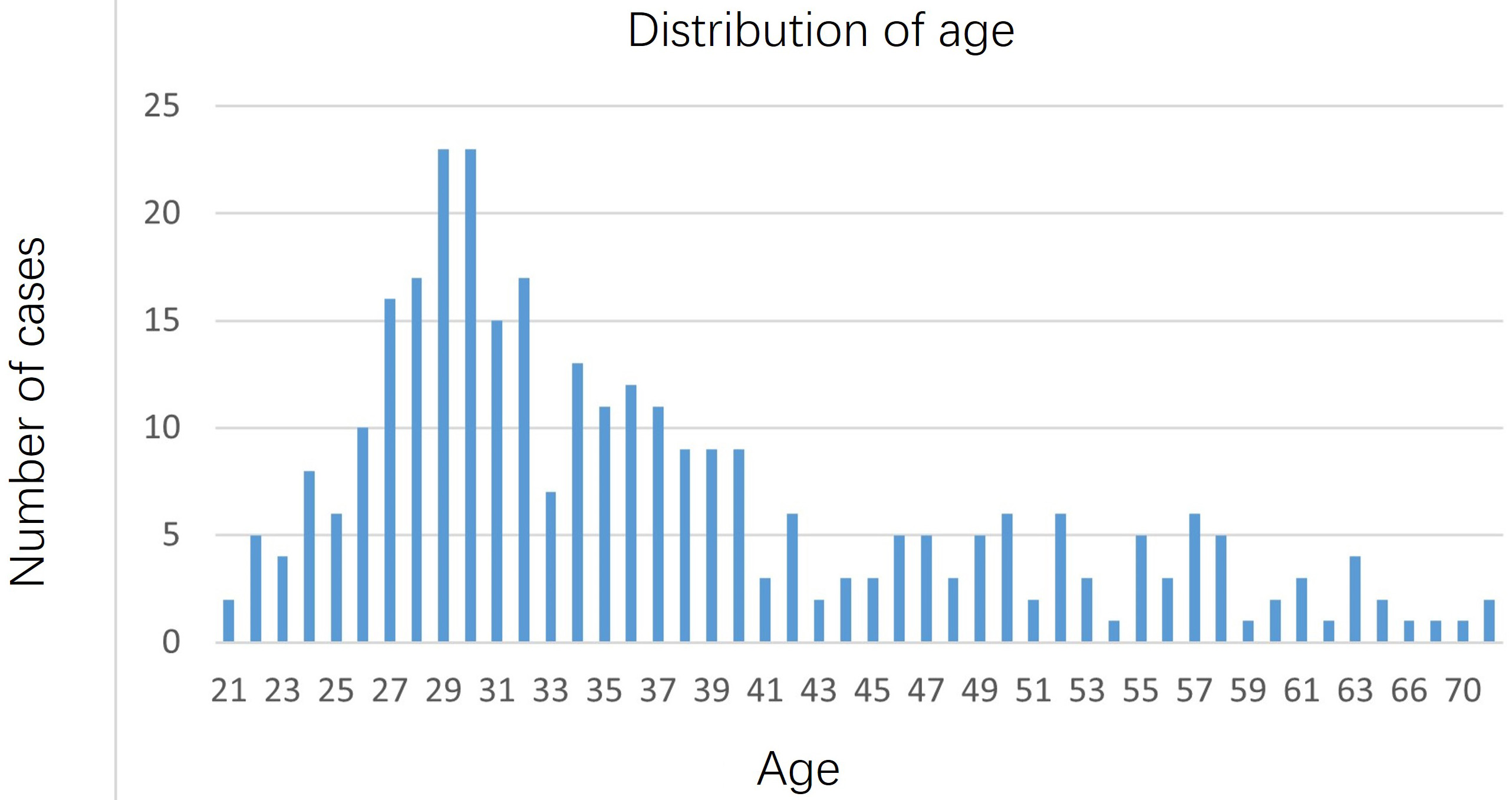
Patients ranged in age from 21 to 73 years, with an average age of 37.21 years. Among the 318 patients, 74.53% (237/318) were infected with a single HPV type, and 25.47% (81/318) were infected with more than two HPV types. In terms of HPV types, the top 5 types were 52, 58, 51, 56 and 16. The highest proportion was HPV52, accounting for 27.4% (87/318), followed by HPV58, accounting for 17.30% (55/318) (Fig. 2). In terms of age distribution, 27–32 year olds were at the peak (Fig. 3).
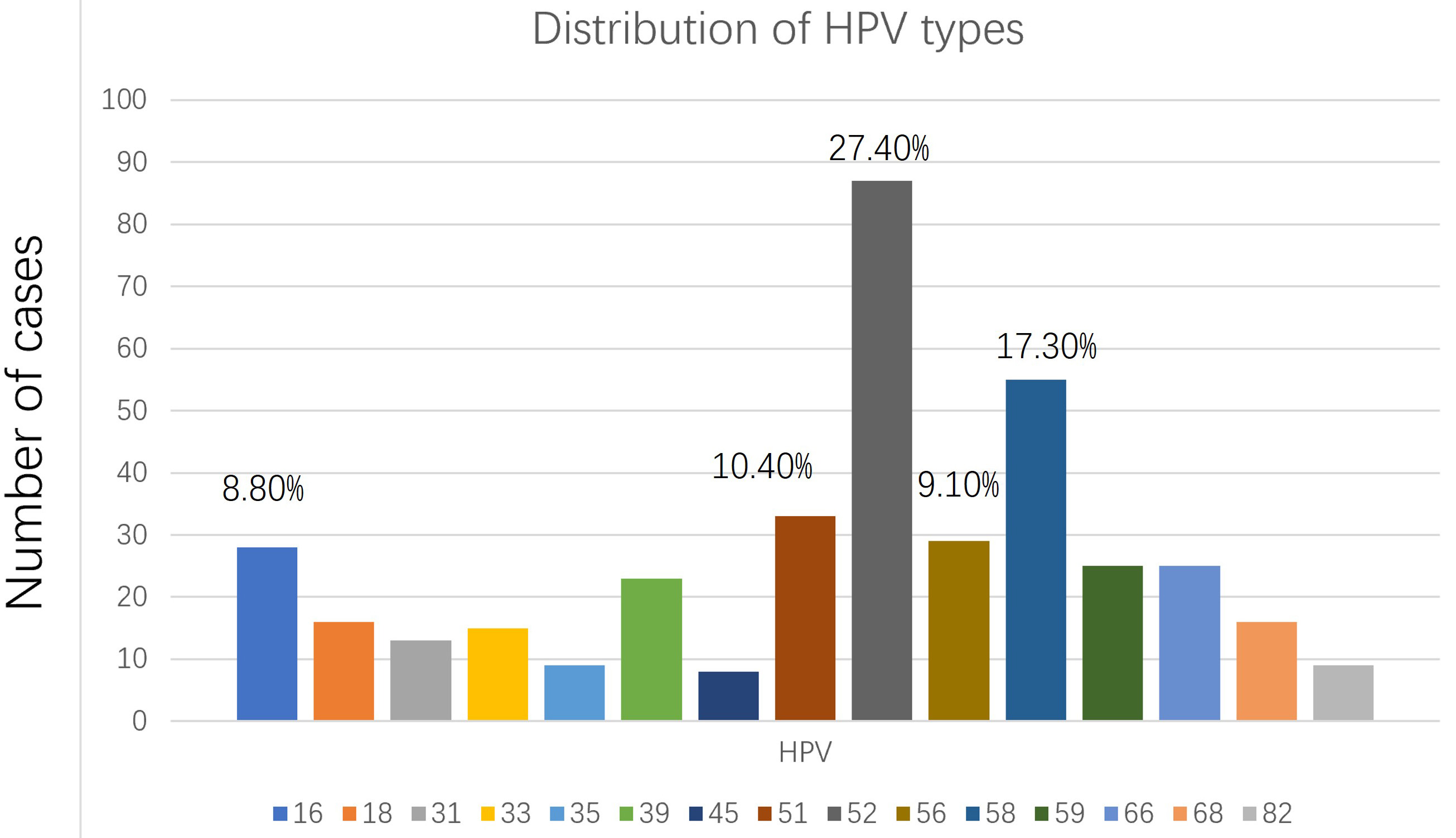 Fig. 2.
Fig. 2.Distribution of human papillomavirus (HPV) types.
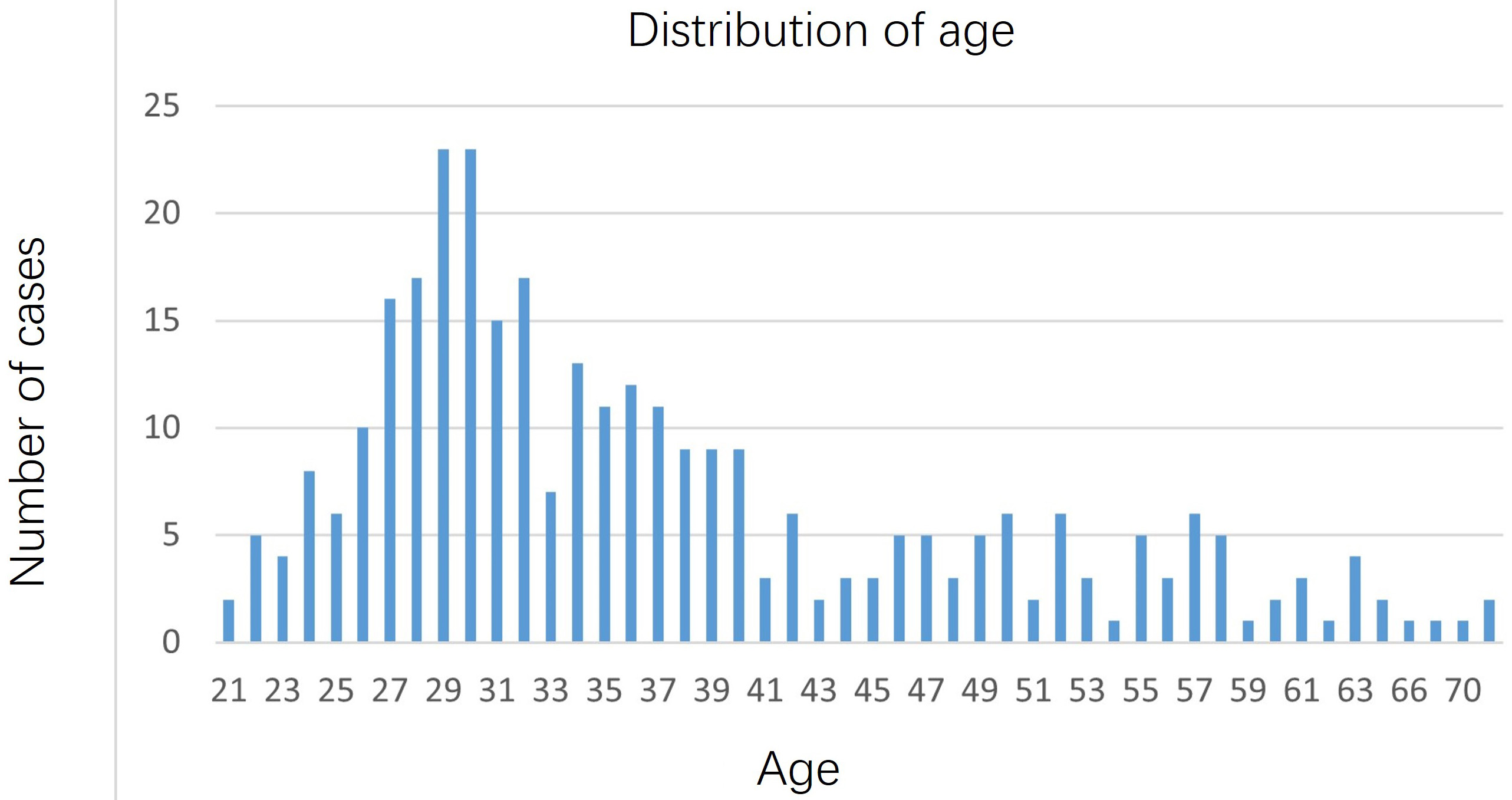 Fig. 3.
Fig. 3.Distribution of age.
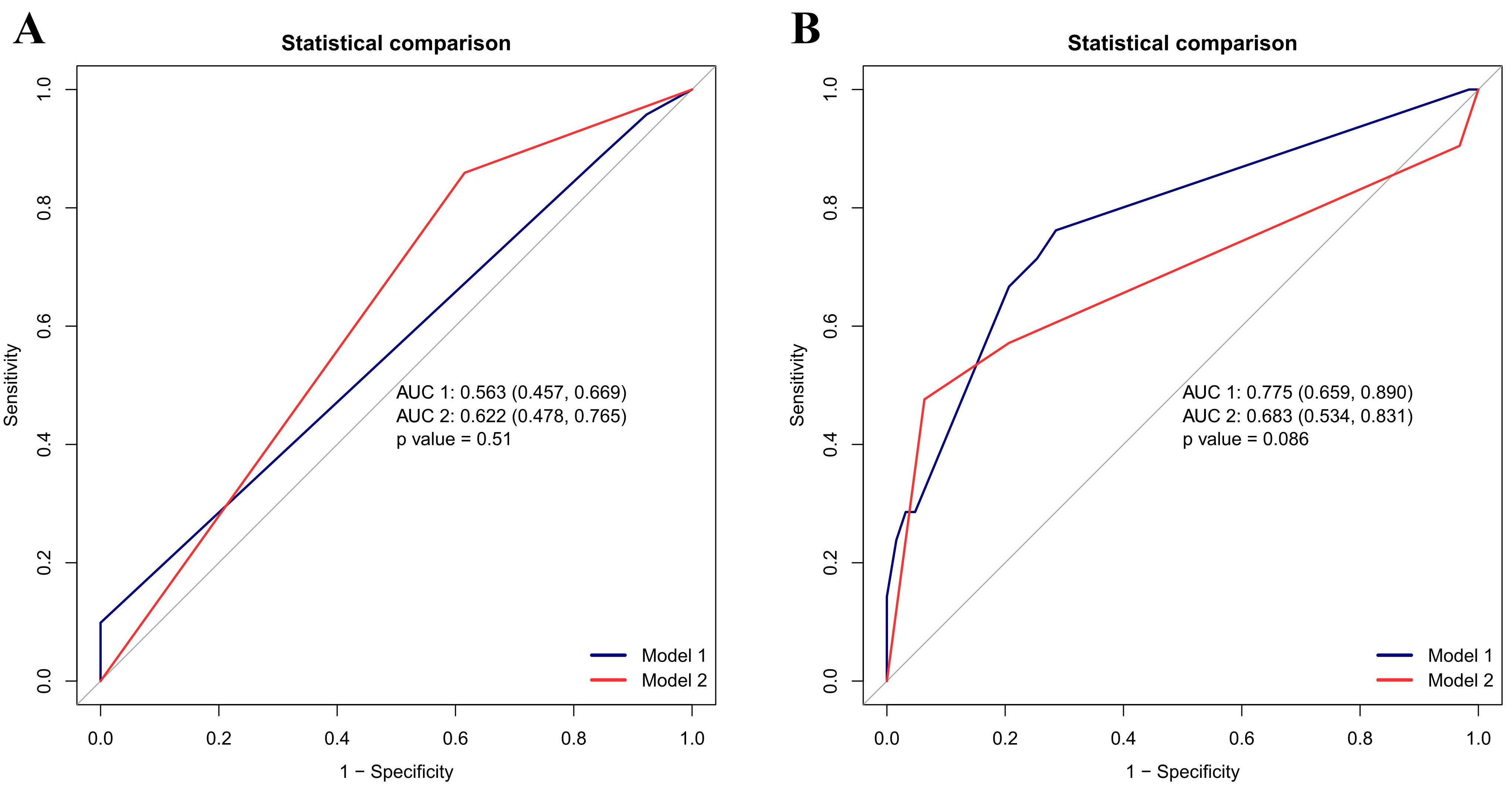
Among the 318 patients studied, 39 patients were 16/18 high risk HPV (hrHPV) and 279 patients were non 16/18 hrHPV. All the 318 patients underwent TS, 115 were TS positive and 203 were TS negative. 84 patients were referred to colposcopy, and the colposcopy biopsy results showed that 13 patients had chronic inflammation, 15.48% (13/84), 51 patients had LSIL, 60.71% (51/84), and 20 patients had CIN2–3, 23.81% (20/84) (Table 1). The negative predictive values of TS and TCT screening for cervical cancer and precancerous lesions were 33.33% and 16.90%, respectively. The positive predictive values were 88.41% and 92.31%, respectively. The sensitivity was 85.92% and 16.90%, respectively. The specificity was 38.46% and 92.31%, respectively. The AUC of TS was 62.19% (62.2–76.54%) and that of TCT was 53.74% (53.7–64.2%). If CIN2+ was used as the end point, the sensitivity (76% vs. 48%) and specificity (71% vs. 94%) of HPV typing combined with TCT compared to HPV typing combined with TS demonstrated the AUC being 77.48% and 68.25%, respectively (p = 0.086) (Fig. 4).
| Histological diagnosis | Normal | CIN1 | CIN2 | CIN3 | Total | |
| Cytological examination | ||||||
| NILM | 12 (16.90) | 45 (63.38) | 5 (7.04) | 9 (12.68) | 71 (84.52) | |
| ASCUS | 1 (16.67) | 3 (50) | 1 (16.67) | 1 (16.67) | 6 (7.14) | |
| ASC-H | 0 | 1 (100) | 0 | 0 | 1 (1.19) | |
| LSIL | 0 | 2 (33.33) | 0 | 4 (66.67) | 6 (71.43) | |
| TS examination | ||||||
| positive | 8 (11.59) | 45 (65.21) | 6 (8.70) | 10 (14.49) | 69 (82.14) | |
| negative | 5 (33.33) | 6 (40) | 0 | 4 (26.67) | 15 (17.86) | |
Note: NILM, negative intraepithelial lesion or malignancy; ASCUS, atypical squamous cells of undetermined significance; ASC-H, atypical squamous cells cannot exclude an high-grade squamous intraepithelial lesion; LSIL, low-grade squamous intraepithelial lesion; CIN, cervical intraepithelial neoplasia; TS, Truscreen.
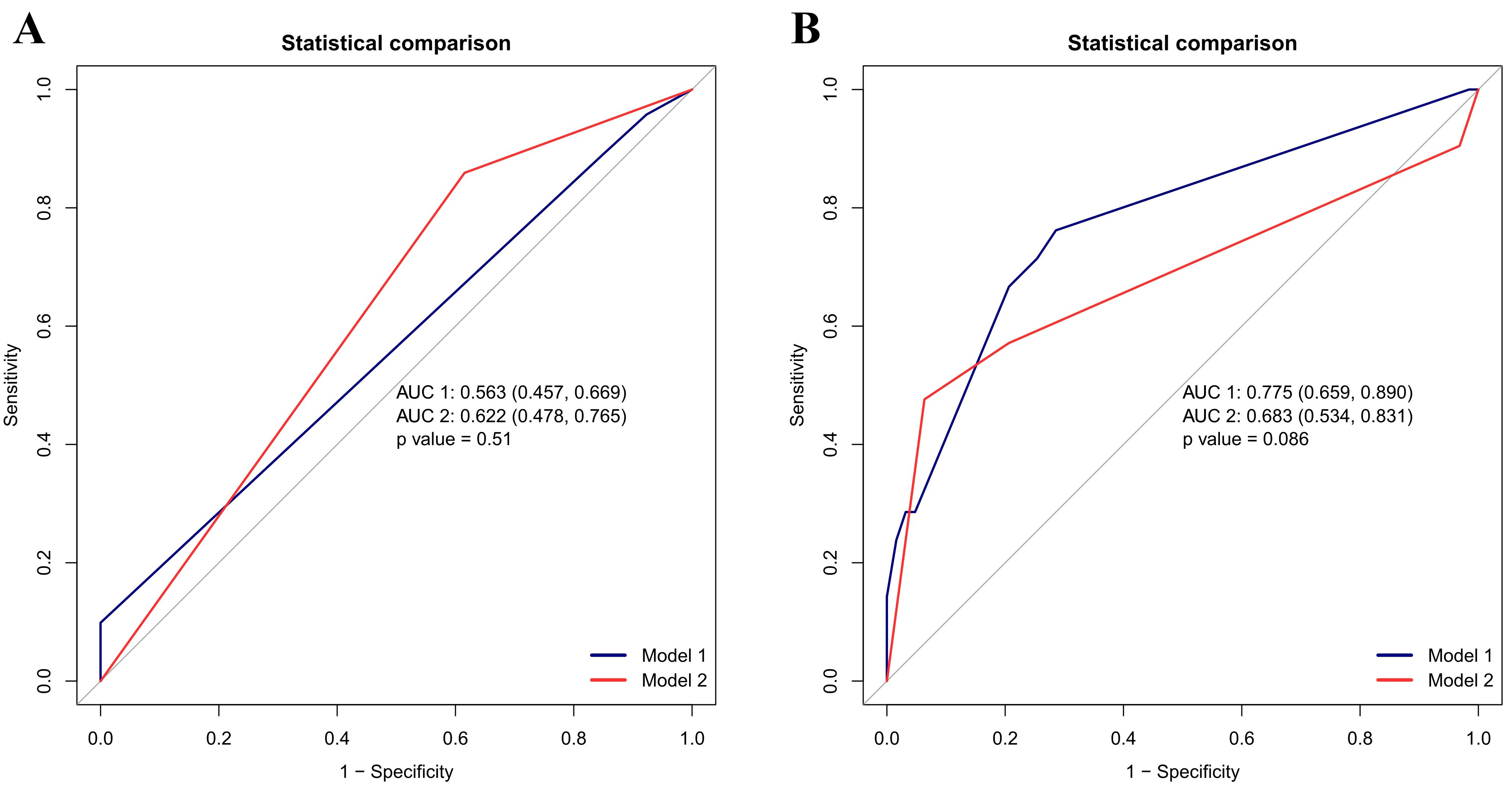 Fig. 4.
Fig. 4.Area under receiver operating characteristic (ROC) curve of thinprep cytology test (TCT) and TruScreen (TS) screening for cervical cancer and precancerous lesions. (A) The area under curve (AUC) of TS curve was 62.19% (62.2–76.54%) and that of TCT was 53.74% (53.7–64.2%). (B) Using cervical intraepithelial neoplasia (CIN) 2+ as the end point, the sensitivity (76% vs. 48%) and specificity (71% vs. 94%) of HPV typing combined with TCT compared with HPV combined with TS demonstrated the AUC being 77.48% and 68.25%, respectively (p = 0.086).
Among the 33 patients whose TCT results were less than ASCUS and HPV16/18 positive, 19 underwent colposcopy, of which 9 were TS positive and 10 were TS negative. Among the 9 positive patients, 3 were CIN1 (33.33%) and 6 were CIN2–3 (66.67%). Biopsy results were normal in 4 cases (40%), 4 cases were CIN1 (40%), and 2 cases were CIN2–3 (20%) (Table 2). The sensitivity and specificity of TS for the diagnosis of CIN3 and above lesions were 67.7% and 80%, respectively.
| HPV grouping | 16/18 HPV | Non-16/18 HPV | ||
| Biopsy result | TS positive | TS negative | TS positive | TS negative |
| Normal | 0 | 4 (40%) | 7 (15.22%) | 0 |
| CIN1 | 3 (33.33%) | 4 (40%) | 36 (78.26%) | 1 (33.33%) |
| CIN2–3 | 6 (66.67%) | 2 (20%) | 3 (6.52%) | 2 (66.67%) |
| Total | 9 (47.37%) | 10 (52.63%) | 46 (93.88%) | 3 (6.52%) |
Among the 251 non-16/18 high-risk HPV-positive patients with TCT results less than ASCUS, 85 were TS positive and 166 were negative. They were referred for colposcopy as TS positive or HPV persistent infection, but only 49 underwent colposcopy. Among the 46 patients whose TCT results were less than ASCUS and non-16/18 HPV positive but TS positive, 7 patients had chronic inflammation (15.22%, 7/46), 36 patients had CIN1, 78.26% (36/46), and 3 patients had CIN2–3, 6.52% (3/46). Among the 3 patients whose TCT results were less than ASCUS and non-16/18 HPV positive but TS negative, 2 patients had CIN2–3, accounting for 66.67% (2/3). The positive predictive value of TS for cervical cancer and precancerous lesions was 84.78%, and the sensitivity was 92.86% (Table 2).
A large amount of epidemiological evidence has confirmed that HPV testing is an accurate primary screening method [7]. A recent systematic review has suggested [8] that the overall infection rate of high-risk HPV infection in China is about 19%, with the 5 most common types being 16, 52, 58, 53 and 18. This is consistent with the results obtained in our study. However, HPV infection has a certain degree of natural clearance, being approximately 90% [9, 10]. This supports the idea that referring all HPV infected patients for colposcopy is unnecessary and is a huge waste of medical resources. Therefore, it is a more economical and reasonable method to select an appropriate triage scheme after HPV has been used for primary screening. At present, many studies have discussed the feasibility of TCT triage, but the results of TCT are closely related to the expertise of cytologists.
The purpose of this study was to explore the application value of TS in the clinical setting and whether it can be used as a triage strategy for cervical cancer screening.
This study showed that in HPV-positive patients, with pathological abnormalities of LSIL as the end point, the sensitivity of TS examination was higher than that of TCT, with the specificity being poorer than that of TCT. The sensitivity was 85.92% and 16.90%, respectively. The specificity was 38.46% and 92.31%, respectively. If CIN2+ was used as the endpoint, the sensitivity (76% vs. 48%) and specificity (71% vs. 94%) of HPV typing combined with TCT compared with TS combined with an AUC demonstrated 77.48% vs. 68.25% (p = 0.086). In 251 non-16/18 high-risk HPV-positive patients with TCT results less than ASCUS, the positive predictive value of TS for cervical cancer and precancerous lesions was 84.78% and the sensitivity was 92.86%. Therefore, TS can be considered as one of the tools for stratified management of such patients. If TS is positive, patients with a TCT result less than ASCUS and who are non-16/18 high-risk HPV-positive should be referred for colposcopy examination. If TS is negative, follow-up observation may be considered. In HPV16/18 positive patients with TCT results less than ASCUS, the TS values of 2 patients (20%) were negative, but CIN3 was found on colposcopy. Therefore, in patients with HPV16/18 infection, TS is not recommended as a stratified management tool, and referral to colposcopy is recommended. Previous studies have shown that TS has high accuracy in detecting cervical cancer and precancerous lesions [11, 12]. In a systematic review in 2018 [13], TS’s pooled test features were as follows: sensitivity was 76%, specificity was 69%, with AUC being 0.7859 (Q = 0.7236). The TS screening triage strategy for HPV16/18 and 12 other high-risk HPV types showed the highest sensitivity for CIN2+ (92.5%), but slightly lower specificity (54.7%) [11]. A recently published study showed that in high-risk HPV-positive women using CIN2+ as the study endpoint, the specificity of HPV detection in combination with TS was significantly higher than that in combination with TCT (50% vs. 39.9%, p = 0.004). The sensitivity of HPV testing combined with TS was comparable to that of the HPV test combined with TCT (93.94% vs. 87.88%, p = 0.625) [14]. Other studies have shown that there is no significant difference in the detection rate of HPV positivity between the two triage strategies [15].
There are many factors that may affect the research results. For example: (1) The cytology expertise of pathology departments in different hospitals was variable. (2) In clinical practice, the contraindications for TS examination were not clear, such as within 3 months postpartum or following a cervical cone procedure, which may interfere with the results of the TS examination. (3) The accuracy of TS examination results depended to a certain extent on whether the procedure is standardized. During the detection process, the probe needed to contact the cervical surface. If the cervical surface secretions were excessive or there was inflammation, the stimulation signals could not be received, which may result in false negative or false positive results. (4) Whether the point used for detection could fully cover the cervix. If the full coverage of the cervical surface was not guaranteed, or there were lesions in the cervical canal and vaginal wall, it may cause potential false negative or false positive results.
In general, many research results indicate that this is a promising technology for its good sensitivity and specificity. In addition, the TS test has several other advantages in that it can give real-time results during gynecological outpatient visits, it is easy to use, the procedure is non-invasive, and patient satisfaction is high. Although the current research sample size was small, this study may provide some basis for the triage strategy for cervical cancer screening. The next plan is to conduct a larger population study for the value of TS in the real clinical setting.
TS examination can be considered as one of the stratified management methods for non-16/18 HPV-positive patients with TCT value less than ASCUS. For these patients, if TS is positive, it is recommended to immediately refer them to colposcopy to reduce missed diagnosis of CIN. If TS is negative, it is recommended to have a follow-up examination after 1 year. Furthermore, for areas with difficult to follow-up patients, TS can be considered as one of the methods for cervical cancer screening due to its real-time and fast response. However, the applicable population and standardized operating procedures should be considered. In summary, patients’ age, previous screening history and fertility requirements should be considered in clinical decision-making and further analysis of large-scale clinical study data is still needed.
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
LML and JZ designed the research study. LML performed the methodology and analysis. LML drafted the manuscript, and JZ contributed to the critical revision of the manuscript. Both authors read and approved the final manuscript. Both authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Beijing Anzhen Hospital (Anzhen 2021113X).
We would like to express our gratitude to all those who helped us during the research and writing of this manuscript. Thanks to all the peer reviewers for their opinions and suggestions.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.