



 , Abdül Hamid Güler 1, Tolgay Tuyan İlhan 2, Feyza Nur Çintesun 3, Çetin Çelik 1, Mehmet Kulhan 1
, Abdül Hamid Güler 1, Tolgay Tuyan İlhan 2, Feyza Nur Çintesun 3, Çetin Çelik 1, Mehmet Kulhan 11 Department of Obstetrics and Gynecology, Selçuk University Medicine Faculty, 42250 Konya, Turkey
2 Department of Obstetrics and Gynecology, Mersin University Faculty of Medicine, 33110 Mersin, Turkey
3 Department of Obstetrics and Gynecology, University of Health Sciences, Konya City Hospital, 42010 Konya, Turkey
Abstract
Background: The main purpose of this study was to investigate the feasibility and safety of performing a laparoscopic intervention for the conservative management of uterine rupture (UR) during pregnancy. This study also provides a brief overview on the challenges and understanding of the management of UR in pregnancy. Methods: Patients diagnosed with UR between 2011–2021 at Selçuk University, Faculty of Medicine were evaluated, retrospectively. The reproductive history, clinical characteristics, UR symptoms and signs, predisposing factors, operative findings, complications and outcomes were assessed. The choice of treatment was determined according to the patients’ age, fertility desire, the severity of disease, and hemodynamic status. A variety of options ranging from surgical rupture repair, to hysterectomy via minimally invasive surgery or laparotomy, were employed. Laparotomy was preferred in all patients with viable fetuses, and in those with hemodynamic instability. Results: A total of 23 cases of UR were operated over a 10-year period. Nine of them underwent laparoscopic surgery and the remaining 14 underwent laparotomy. The presenting signs and symptoms of UR, in order of decreasing frequency were: abdominal pain, vaginal bleeding, fetal distress/demise, non-reassuring fetal status, signs of hemodynamic changes, elevation of the fetal presenting parts and/or the absence of station changes with contractions, and the early detection of hemoperitoneum on ultrasound. The primary risk factors for UR were a history of uterine surgery, use of misoprostol during abortion and labor, obstructed labor, curettage, congenital uterine malformations and trauma. Total ruptures included 17 in the lower segment (Kerr incision) and 6 outside the lower segment. There were considerable differences in the incidence of Kerr incision site ruptures and UR in other sites. The major complication rates were higher in ruptures outside the lower segment (6/6, 100%) than lower segment ruptures (5/17, 29.4%). Hysterectomy rates in lower segment ruptures and other rupture sites were 5/17 (29.4%) and 4/6 (66.6%), respectively. Kerr incision site ruptures are easier to manage and with less catastrophic complications compared to cases of UR after trauma, and those of unscarred uteri or those with a history of uterine scars other than from a Kerr incision. Conclusions: This study provides evidence of the safety and feasibility of laparoscopic management of UR, and this may encourage surgeons to consider minimally invasive surgery in hemodynamically stable patients prior to more aggressive and radical treatments. With the appropriate skill set, laparoscopy may be considered the preferred route of intervention, even in potentially life-threatening conditions such as UR.
Keywords
- complete uterine rupture
- laparoscopy
- scarred uterus
- unscarred uterus
Complete uterine rupture (UR) during pregnancy refers to a disruption of all uterine layers, including the visceral peritoneum and the direct interaction of the fetus or amniotic fluid with the maternal abdominal cavity. Although this event is very rare, it is well known to cause some catastrophic complications. The prevalence in patients with scarred uteri, which is mainly a consequence of Cesarean Section (C/S), is up to 1% and it can occur in 0.04% of patients without a history of C/S [1].
The most important risk factors are surgical procedures in which all layers of the uterus are incised as in C/S, which currently constitutes the majority of such procedures. UR may also be associated with all kinds of other uterine surgeries, labor induction, dystocia, and grant multiparity [2]. Additionally, the relationship between UR and smoking, maternal age, body mass index, birth weight, gestational age, operative vaginal delivery, and interpregnancy intervals have been reviewed elsewhere [3, 4, 5, 6]. However, to date, none of these predisposing factors were found to be sufficiently reliable and robust to be clinically useful for the prediction of UR. A prior vaginal birth significantly reduces, but does not eliminate, the risk of UR [7].
Since UR requires urgent surgical intervention, intrapartum use of imaging methods is limited. However, if rupture is suspected and feto-maternal stability is confirmed, ultrasounografy (USG) is the initial imaging modality of choice. USG can not only be used to detect the site of perforation but also the presence and estimation of the volume of any associated hemoperitoneum [8].
The choice of treatment varies according to the patient’s age, fertility desires, the severity of disease, and hemodynamic status. The intervention may range from surgical rupture repair to hysterectomy. Management should, therefore, be decided on a case-by-case basis. Laparoscopy has been adopted in virtually all gynecologic surgeries, due to technological advancements and its many proven advantages. On the other hand, currently, there are only several case reports that laparoscopic surgery can be conducted for this purpose. To the best of our knowledge, our study appears to be the largest up-to-date case series of patients undergoing laparoscopic surgery. The main purpose of this study was to investigate the feasibility and safety of performing a laparoscopic intervention in the conservative management of UR in pregnancy. This study also provides a brief overview of the understanding of the management of UR, and addresses its pertinent challenges. It also includes a review of the clinical findings and risk factors associated with UR.
In this descriptive study, patients diagnosed with UR between 2011–2021 at Selçuk University, Faculty of Medicine were evaluated, retrospectively. Our study was conducted as a descriptive retrospective report of an aggregation of individual cases.
The demographic characteristics of the patients with the diagnosis of UR were retrieved from electronic medical records. The reproductive history, clinical characteristics, UR symptoms and signs, predisposing factors, operative findings, complications, and outcomes were assessed. Only cases of total UR, which was defined as the disruption of the entire uterine muscular layers and the visceral peritoneum regardless of the status of the fetal membranes, were included in the study. Partial ruptures (dehiscences, clinically occult uterine disruption with intact serosa), isthmoceles, uterine perforation secondary to an iatrogenic cause and non-pregnant cases were excluded.
The most important determinant in the selection of the surgical mode of management was the feto-maternal condition. The first priority was the mother, followed by the fetus, and the next priority was to preserve the uterus and if possible, to achieve this with minimally invasive methods.
Laparotomy was preferred in all cases with viable fetuses and in cases of hemodynamic instability. Although studies have shown that laparoscopy can be performed in up to 28 weeks of pregnancy, laparotomy was chosen for UR cases over 20 weeks. Laparotomy was preferred because of the prominent decrease in the laparoscopic panoramic view beyond 20 weeks, which may delay timely hemostatic intervention.
All patients were placed in a low dorsal lithotomy position to evaluate for vaginal bleeding. Unless other indications existed as in cases of previous non-Kerr incisions, the Pfannenstil incision was sufficient for almost all surgical manipulations. It may be necessary to be prepared for unexpected situations during laparotomy. Midline incisions may be preferred for wider exploration and faster abdominal access [9]. In cases of suspected large ruptures, extensive hemoperitoneum, UR after trauma, unscarred uteri and in uterine scars other than from a previous Kerr incision, midline incisions were usually preferred.
The surgical steps of laparotomy can be summarized as: the localization and determination of the site of rupture (Fig. 1), bleeding control, delivery of the fetus and placenta, repair of the defect including excision of the fibrotic tissue, and closure of the anterior uterine wall. A hysterectomy may be required in severely damaged cases when bleeding cannot be controlled, or the uterus is beyond repair.
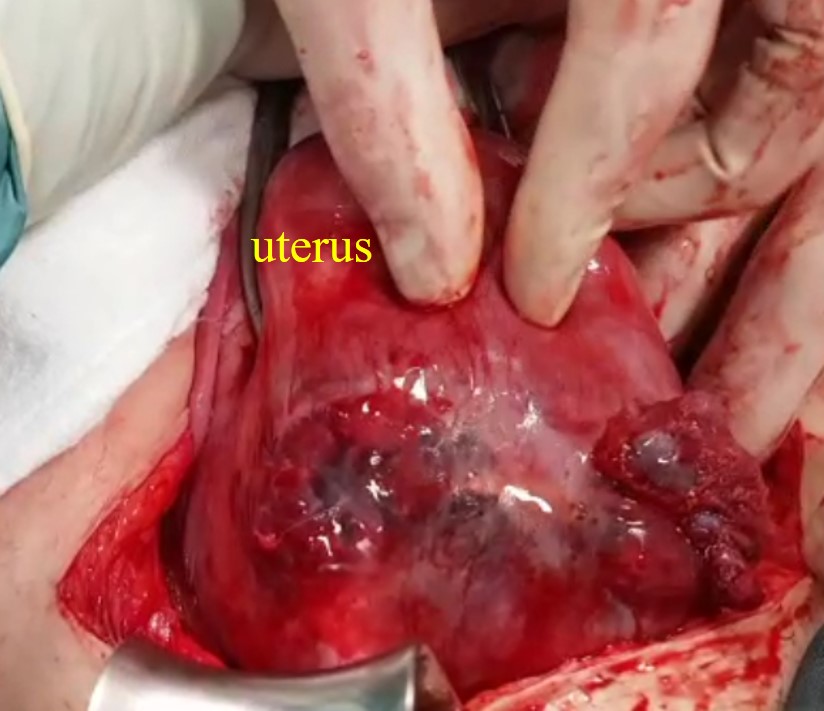 Fig. 1.
Fig. 1.Rupture at the site of a previous Cesarean Section (C/S) scar at 17 weeks of pregnancy (Case 5 in Table 1).
All patients in the laparoscopy group were operated on by the senior author. Patients were placed in low dorsal and steep Trendelenburg positions for the expulsion of an embryo or fetus, for the evaluation of bleeding, and uterine manipulation. Appropriate shoulder support was placed to prevent the patient from slipping off the table. After laparoscopic abdominal entry and the establishment of pneumoperitoneum, management for anatomical restorations included the utilization of avascular spaces and identification of size, depth, extent, and location of the rupture line. Homeostasis of active bleeding foci was performed with bipolar energy (Fig. 2A,B). Direct laparoscopic visualization was employed for the assessment of the uterine cavity after the expulsion of an embryo/fetus or for curettage via the vaginal route. The endometrial cavity was assessed with transvaginal sonography, under sterile conditions, to confirm complete clearance of the uterus from fetal and placental appendages. A bladder flap was made to mobilize the bladder inferiorly by opening the vesicovaginal and vesicocervical space, for improved access to the lower uterine segment(Fig. 2C). At this stage, a uterine manipulator or vaginal tampon facilitated bladder dissection. Excision of the fibrotic tissue (Fig. 2D) and full-thickness closure of the uterus with polyglactin sutures similar to the traditional methods of uterine closure were employed (Fig. 2E,F). Closure of the visceral peritoneum is not essential, but may be helpful for hemostasis in low flow bleeding (Fig. 2G,H).
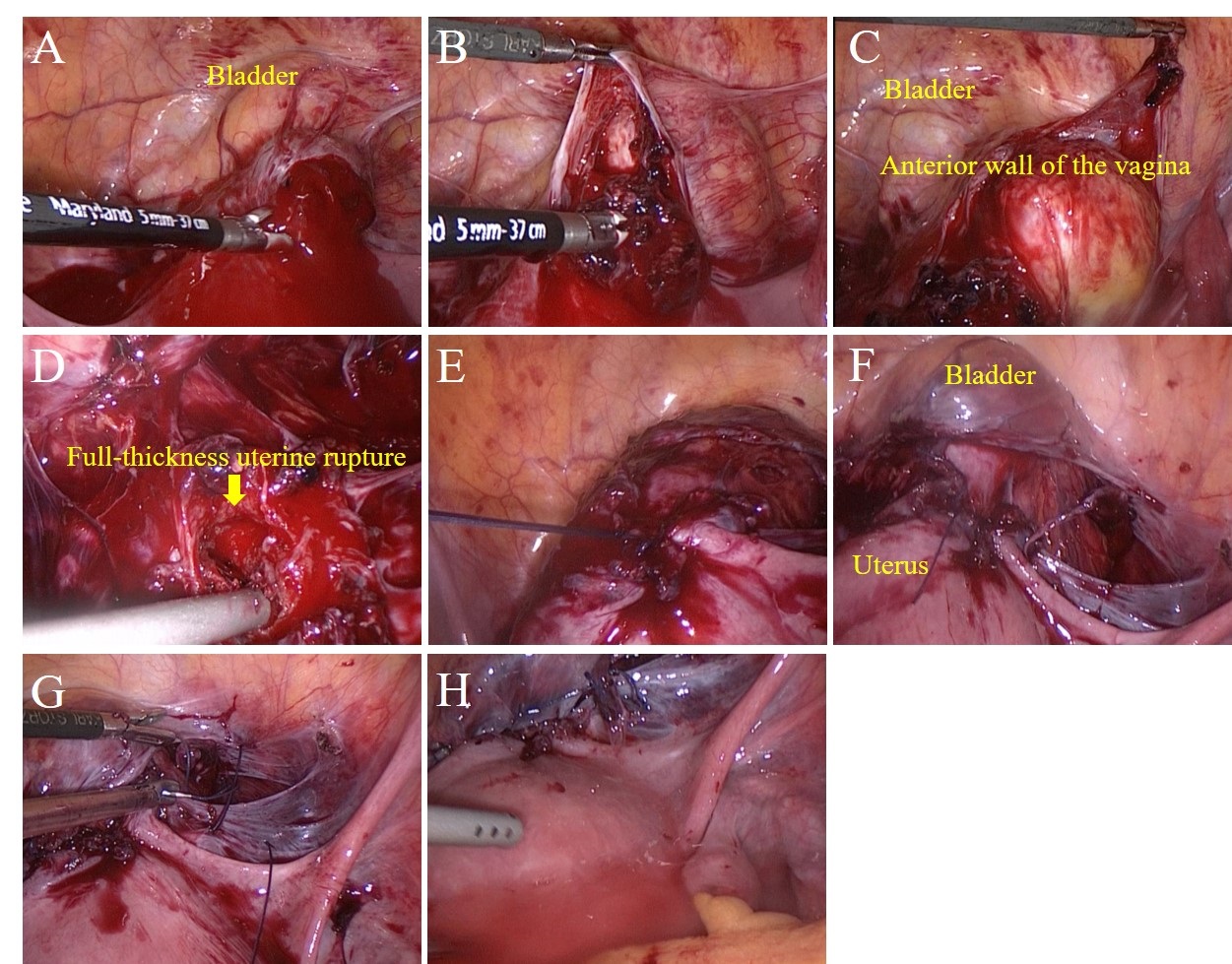 Fig. 2.
Fig. 2.Laparoscopic surgical steps. (A) Identifying rupture at 13 weeks of pregnancy (Case 1 in Table 2). (B) Control of bleeding. (C) Establishing a bladder flap and dissecting the peritoneal lining to separate the urinary bladder from the lower uterine segment. (D) Excision of the fibrotic tissue and removal of the separated chorionic villi. (E) The figure-of-eight suture technique used for wound closure. (F) Suturing until achieving complete hemostasis. (G) Visceral peritonization. (H) Aspiration, irrigation, and final review.
As our case numbers were nonetheless limited, we performed no statistical comparisons of risk factors and outcomes in association with scar location, complete versus partial rupture or perinatal outcome. However, based on percentages, there were considerable differences between outcomes of ruptures in scars in or outside the lower segment.
A total of 23 cases of UR were operated in a single academic tertiary center over a 10-year period. Nine of them underwent laparoscopic surgery and the remaining 14 underwent laparotomy. The mean age was 31.4 (25–41), the mean gravidity 3.7 (2–6), and the mean parity 2.7 (2–4). The demographic data, clinical characteristics and the modes of management are summarized in Tables 1,2.
| N | Age | G/P | GW | Signs and symptoms | Predisposing factors | Management | Operative findings | Complications | |
| Incision types | Operation type | ||||||||
| 1 | 38 | 6/4 | 41 w | Abdominal pain, vaginal bleeding, fetal distress, the elevation of the fetal presenting part | Dystocia, kristeller maneuver, oxytocin | Midline, TAH | Active bleeding tear extending from the uterine isthmic region to the right uterine artery | Requirements of NICU, blood transfusion | |
| 2 | 32 | 5/4 | 15 w 4 d | Abdominal pain, vaginal bleeding, hemoperitoneum | PGE2-induced abortion, two prior C/S | Pfannenstiel, surgical abortion, rupture repair | Rupture at the site of a prior C/S | Blood transfusion | |
| 3 | 36 | 5/3 | 40 w 5 d | Abdominal pain, non-reassuring fetal status, elevation of the fetal presenting part | PGE2 induced labor, obstructed labor, curettage | Midline, C/S, rupture repair, İnternal iliac artery ligation | Long irregular tear in the posterior wall with active bleeding foci | Blood transfusion, hospital stay longer than 1 week | |
| 4 | 35 | 4/4 | 36 w 1 d | Vaginal bleeding, signs of hemodynamic changes, demise, hematuria | Trauma (traffic accident) | Midline, C/S, TAH, bladder rupture repair | Curved tear extending from uterus cervix to fundus, with elongated boundary of the bladder | Fetal demise, blood transfusion bladder injury prolonged bladder drainage, hospital stay longer than 1 week | |
| 5 | 28 | 3/3 | 17 w 1 d | Vaginal bleeding, hemoperitoneum | PGE2-induced abortion, two prior C/S, congenital uterine malformations | Mini-Pfannenstiel, rupture repair | Rupture at the site of a prior C/S | ||
| 6 | 32 | 4/4 | 38 w 2 d | Abdominal pain, non-reassuring fetal status, signs of hemodynamic changes | Three prior C/S | Pfannenstiel C/S, TAH, bladder rupture repair, ureteral stenting | Rupture at the site of a prior C/S involving the base of the bladder | Blood transfusion, bladder injury, prolonged bladder drainage, hospital stay longer than 1 week | |
| 7 | 29 | 2/2 | 35 w | Abdominal pain, fetal distress | Prior C/S, inverted T incision, preterm labor | Pfannenstiel C/S, rupture repair, internal iliac artery ligation, Bakri Balloon placement | Rupture at the site of a prior C/S involving the superior branches of the right uterine artery | Blood transfusion, requirements of NICU, requirements of ICU | |
| 8 | 33 | 4/4 | 35 w 5 d | Vaginal bleeding, fetal distress, signs of hemodynamic changes | Three prior C/S, placenta accreta | Pfannenstiel C/S, TAH, BSJ | Rupture at the site prior to C/S | Blood transfusion, requirements of NICU | |
| 9 | 33 | 4/3 | 32 w 3 d | Abdominal pain, vaginal bleeding, hemoperitoneum, non-reassuring fetal status | Myomectomy and preterm labor | Midline C/S, supracervical hysterectomy, BSJ | long irregular tear in the anterior wall with active bleeding foci | Blood transfusion, hospital stay longer than 1 week, requirements of NICU | |
| 10 | 27 | 4/3 | 34 w 5 d | Abdominal pain, vaginal bleeding, signs of hemodynamic changes | Myomectomy and preterm labor | Midline C/S, supracervical hysterectomy | Long-large irregular tear in the anterior wall with active bleeding foci | Blood transfusion, requirements of NICU | |
| 11 | 28 | 2/2 | 35 w 1 d | Abdominal pain, vaginal bleeding | Two prior C/S | Pfannenstiel C/S, rupture repair | Rupture at the site of a prior to C/S | Requirements of NICU | |
| 12 | 27 | 4/2 | 17 w 1 d | Abdominal pain, vaginal bleeding, hemoperitoneum, failed induction with PGE2 | Two prior C/S induced abortion, curettage | Pfannenstiel, rupture repair | Rupture at the site of a prior to C/S | ||
The “N” indicates the number of patients; G/P, gravidity and parity, GW, gestational weeks; C/S, cesarean section; TAH, total abdominal hysterectomy; BSJ, bilateral salpingectomy; NICU, neonatal intensive care unit, ICU, intensive care unit; PGE2, prostaglandin E2.
| N | Age | G/P | GW | Signs and symptoms | Predisposing factors | Management | Operative findings | Complications | |
| Incision types | Operation type | ||||||||
| 1 | 28 | 4/3 | 13 w 2 d | Abdominal pain, vaginal bleeding, hemoperitoneum | Two prior C/S, PGE2 induced abortion | Umbilical 10 mm camera port, 1 |
Rupture at the site prior to C/S | ||
| 2 | 29 | 3/2 | 15 w 1 d | Abdominal pain, vaginal bleeding | Two prior C/S, PGE2 induced abortion | Umbilical 10 mm camera port, 1 |
Rupture at the site prior to C/S | ||
| 3 | 41 | 4/3 | 14 w 5 d | Abdominal pain, vaginal bleeding, hemoperitoneum, | Three prior C/S curettage | Umbilical 10 mm camera port, 2 |
3 cm. rupture at the site of a prior C/S | ||
| 4 | 26 | 3/2 | 14 w 2 d | Vaginal bleeding, hemoperitoneum | Two prior C/S, PGE2 induced abortion | Umbilical 10 mm camera port, 1 |
Rupture at the site of a prior to C/S | ||
| 5 | 27 | 3/2 | 14 w 5 d | Abdominal pain, vaginal bleeding, hemoperitoneum, failed induction with PGE2 | Two prior C/S induced abortion | Umbilical 10 mm camera port, 2 |
Rupture at the site of a prior to C/S | ||
| 6 | 25 | 3/2 | 17 w 2 d | Abdominal pain, vaginal bleeding | Two prior C/S | Supraumbilical 10 mm camera port, 1 |
Rupture at the site of a prior to C/S | ||
| 7 | 34 | 4/3 | 12 w 6 d | Abdominal pain, vaginal bleeding, hemoperitoneum, failed induction with PGE2 | Three prior C/S induced abortion | Umbilical 10 mm camera port, 2 |
Rupture at the site o C/S f a prior | ||
| 8 | 28 | 3/2 | 11 w 4 d | Vaginal bleeding, hemoperitoneum | Two prior C/S | Umbilical 10 mm camera port, 1 |
Rupture at the site of a prior C/S | ||
| 9 | 36 | 4/2 | 15 w 1 d | Asymptomatic, hemoperitoneum | Two prior C/S, induced abortion, curettage | Umbilical 10 mm camera port, 1 |
Rupture at the site of prior C/S, intestinal adhesion at the rupture line, and low-flow bleeding | ||
| Patients converted to laparotomy | |||||||||
| 1 | 39 | 4/4 | 18 w | Abdominal pain, vaginal bleeding, hemoperitoneum, failed induction with PGE2 | Three prior C/S induced abortion | Laparoscopy converted to Pfannenstiel TAH, BSJ | Large rupture at the site of a prior C/S beyond the repair | Blood transfusion, conversion to laparotomy | |
| 2 | 32 | 4/4 | 19 w 4 d | Abdominal pain, vaginal bleeding, failed induction with PGE2 | Two prior C/S, PGE2 induced abortion | Laparoscopy converted to Pfannenstiel, supracervical hysterectomy | Large rupture at the site of a prior cesarean incision and intestinal adhesion to the rupture line | Conversion to laparotomy | |
The “N” indicates the number of patients; G/P, gravidity and parity, C/S, cesarean section; TAH, total abdominal hysterectomy; BSJ, bilateral salpingectomy; NICU, neonatal intensive care unit, ICU, intensive care unit; PGE2, prostaglandin E2.
Although patients with UR may rarely be asymptomatic, clinical symptoms are overt in the majority of patients within a short onset of time. The presenting signs and symptoms of UR, in order of decreasing frequency were: abdominal pain, vaginal bleeding, fetal distress/demise, non-reassuring fetal status, signs of hemodynamic changes, elevation of the fetal presenting parts, and/or the absence of station changes with contractions, and the early detection of hemoperitoneum on ultrasound. The primary risk factors for UR were a history of uterine surgery, labor or abortion induction, trauma, curettage, congenital uterine malformations, and placental invasion anomalies. The distribution of risk factors, signs, symptoms, operative findings, and complications are summarized in Tables 1,2.
Total ruptures included 17 in the lower segment (Kerr incision) and 6 outside the lower segment. As our case numbers were limited, statistical comparisons of risk factors and outcomes in association with scar location could not be performed. However, there were considerable differences in the percentages of respective outcomes of Kerr incision site ruptures compared to other sites of rupture. The major complication rates were higher in rupture sites outside the lower segment (6/6, 100%) than lower segment ruptures (5/17, 29.4%). Hysterectomy rates in lower segment scar ruptures and other rupture sites were 5/17 (29.4%) and 4/6 (66. 6%), respectively. Kerr incision site ruptures were easier to manage and with less catastrophic complications than UR after trauma, UR cases associated with unscarred uteri and in uterine scars other than from Kerr incisions.
UR during pregnancy is a rare event and frequently results in life-threatening feto-maternal complications. However, more awareness regarding UR has emerged only in the last decade, with the highest UR rate among all women, probably due to increasing C/S rates, repeated C/S, and better documentation [10, 11]. UR is perceived as a major health burden in developing countries [12]. Considering the rising C/S rates globally, it is clear that higher UR rates and management challenges will be observed in the future. Cases that were encountered very rarely in the recent past, such as C/S scar pregnancies, isthmoceles, and placental invasion anomalies, are now increasingly common.
The primary risk factors for UR in patients with a history of C/S are previous UR and previous fundal or high vertical uterine incisions, which include an inverted T or J incision or extension of a low transverse incision into the upper uterine segment and the use of induction [13]. The incidence of rupture is higher in patients who undergo induction than in those who experience spontaneous labor [14], and it is noticeably higher with the use of misoprostol than oxytocin [15]. There are some hypotheses that UR after uterine surgery results from poor vascularisation, electro-coagulation, and deficient healing processes, and this defect may therefore render the uterus vulnerable to forceful influences and rupture [16]. In our series, the primary risk factors for UR were previous C/S, use of misoprostol in abortion, uterine surgery, obstructed labor, and trauma, in order of decreasing frequency.
There is no reliable method for predicting UR in patients with a prior C/S birth. Familiarity with the symptoms and signs and the maintenance of a high index of clinical suspicion for UR seem to be very important for its correct and early management, especially in patients with risk factors. UR must be excluded in all cases of vaginal bleeding during pregnancy.
In the case of UR, one of the most important questions that the surgeon should answer immediately is whether the uterus can be repaired or not. Unfortunately, the most accurate answer to this question in most cases can be given only at the time of surgery. A UR may range from a small defect of uterine layers to a wide and deep defect involving the entire myometrium, and even nearby pelvic organs. The choice of treatment should be determined not only by the characteristics of the rupture, but also by the patient’s hemodynamic status and desire for fertility. Due to the rarity of UR, the variability in the location and extent of the injury, and the scarcity of long-term follow-up data, there is no consensus on the optimal repair technique. Exploratory laparotomy is the most commonly used method to confirm UR in clinical practice [17] and hysterectomy has been the treatment of choice for decades [18]. The advantages of laparoscopic surgery, including smaller scars, fewer wound complications, faster recovery, decreased pain, and shorter duration of hospital stay are well established. Recently, with the continuous development of laparoscopic technology and improvements in surgical training, studies have shown that laparoscopy can also be used for this purpose [19, 20, 21, 22]. Unfortunately, almost all are case reports. A case of postpartum UR and laparoscopic repair is reported by Rottenstreich et al. [19] and Cai et al. [17]. Namazov et al. [20] reported a video presentation, of UR after early second-trimester medical abortion, and a special case of uterine and bladder rupture after vaginal birth after cesarean (VBAC) and laparoscopic repair is reported by Lua et al. [21]. Stern et al. [22] compared operative data and patient satisfaction between open and laparoscopic surgery for postpartum-diagnosed UR in a questionnaire-based cohort study, and emphasized that laparoscopy is a viable surgical option for patients with UR, and may result in better patient recovery and satisfaction. We did not compare the patients who underwent laparotomy and laparoscopic surgery in this study because we often treat high-risk patients with open surgery in our surgical practice. Therefore, since the groups were not similar, it is obvious that bleeding and blood transfusion, complications, and hysterectomy rates will be higher, and the hospital stay will also be longer in these high-risk patients. In this study, 9 of 23 cases were successfully treated with laparoscopic surgery. With the appropriate skill set, laparoscopy was considered the preferred route in selected patients, even in potentially life-threatening conditions such as UR.
Generally, uterine midline small ruptures were more easily repaired than cases of long, wide, and irregular ruptures with lateral extention involving the uterine arteries. Although our sample size was not big enough for a statistical analysis, according to our study, Kerr incision site ruptures were easier to manage than cases of UR after trauma in those with unscarred uteri and in uterine scars formed from incisions other than Kerr incisions. At the same time, the major complication and hysterectomy rates were higher in scars outside the lower segment. In addition to the scar characteristics, a delayed diagnosis could be independently associated with a hysterectomy and significantly higher rates of blood transfusions and puerperal fever [23]. This is consistent with several studies that confirm a worse outcome when the ruptured uterus is not previously scarred [24, 25]. Sayed Ahmed et al. [18] found cervical/parametrial involvement is more evident in the unscarred uterus group but in this study, there was no important difference in the maternal and fetal outcomes in the scarred and unscarred UR groups. Non-complicated Kerr incision site ruptures are easily managed by laparoscopy with basic laparoscopic skills such as hemostasis, suturing and standard laparoscopic equipments. However, extra care may be required to avoid bleeding of the uterine artery during bladder dissection in Kerr incision site ruptures. Overall, our study provides evidence of the safety and feasibility of laparoscopic management. Therefore, in hemodynamically stable cases it should be considered prior to more aggressive and radical treatments, especially in patients with fertility desires prior to or at the 20th week of gestation.
The major limitations of the study are its retrospective design, limited number of patients with no statistical comparisons, lack of long-term follow-up, and the data collection from a single tertiary center. A nationwide population-based multicenter study with a prospective design would provide a better overview of the understanding of this matter, and address the questions related to the challenges in the management of UR. However, to the best of our knowledge, our study appears to be the largest contemporary case series of patients undergoing laparoscopic surgery with this purpose.
The study highlights the feasibility and safety of the laparoscopic management of UR, and this may encourage surgeons to consider minimally invasive surgery in certain conditions before attempting radically aggressive treatments. Laparoscopy may be considered in the suspected UR in stable patients up to early second trimester before the fetal viability and postpartum period.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
MGU, ÇÇ and MK designed the research study. MGU, MK performed conception and design. MGU, AHG, FNÇ contributed towards the data acquisition, analyses and revised the manuscript. MGU and FNÇ performed the research. MGU, ÇÇ, TTİ, MK involved in drafting the manuscript. ÇÇ and AHG provided help. TTİ analyzed the data. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
All patients gave informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Selçuk University, Faculty of Medicine (approval number: 2023/251).
We would like to express our gratitude to Serra Akar M.D and all those who helped us during the writing of this manuscript. Thanks to all the peer reviewers for their opinions and suggestions.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.