

 , Keiyo Imaeda 1, Tomoko Yoshihama 1, Kanako Nakamura 2, Megumi Yokota 1, Shigenori Hayashi 1, Wataru Yamagami 1, Kouji Banno 1, Daisuke Aoki 1
, Keiyo Imaeda 1, Tomoko Yoshihama 1, Kanako Nakamura 2, Megumi Yokota 1, Shigenori Hayashi 1, Wataru Yamagami 1, Kouji Banno 1, Daisuke Aoki 11 Department of Obstetrics and Gynecology, Keio University School of Medicine, 160-8582 Tokyo, Japan
2 Department of Obstetrics and Gynecology, Tachikawa Hospital, 190-0022 Tokyo, Japan
Academic Editor: Christos Iavazzo
Abstract
Background: The Mayer–Rokitansky–Küster–Hauser (MRKH) syndrome is a rare disorder characterized by congenital vaginal defects and uterine traces. Because of its rarity, standardized management for MRKH syndrome is unavailable. This study reviewed the management of the patients with MRKH syndrome in our institution. Methods: Using medical records, we retrospectively reviewed the surgical techniques, outcomes, postoperative management methods, and outpatient follow-up of 17 patients with MRKH syndrome in Keio University Hospital. Results: Of the 14 patients who requested vaginoplasty, 12 underwent surgery with Davydov’s modified procedure after the Frank method, and it took 17 months to 34 months (median two years) for the vaginal cavity to enlarge by 5–6 cm. The Frank method is a non-surgical dilation with instrumental stretching of the vaginal vestibular mucosa. Davydov’s procedure is a surgical vaginoplasty in which the vesicoureteral space is coated by the peritoneum. Although one patient lost 3800 mL of bleeding from the plexus vein and four needed to remove the prosthesis under anesthesia about one month after surgery, all patients achieved anatomic success with a vaginal cavity length of 6 cm or more and could have sexual intercourse with their sexual partners. However, two patients interrupted their preoperative hospital visits, and three were lost to follow-up postoperatively. Two of the three patients who did not accept vaginoplasty presented myoma at uterine trace and underwent myomectomy. Another one was scheduled for surgery through psychological support. Conclusions: Davydov’s modified procedure is effective, and dilating the vaginal cavity adequately using the Frank method before surgery is needed to ensure sufficient vaginal length with less perineum. During the operation, attention is required to care for the plexus vein. Comprehensive psychological support, providing appropriate information to the patient for mental maturity, and planning surgery according to their life stages are essential for successful treatment.
Keywords
- clinical management
- congenital vaginal defects
- Davydov's modified procedure
- Frank method
- MRKH syndrome
- vaginoplasty
The Mayer–Rokitansky–Küster–Hauser syndrome (MRKH syndrome) is characterized by uterovaginal aplasia or aplasia of the uterus and vagina due to Müllerian duct dysgenesis [1]. It is a rare disease occurring approximately once in every 1/5000 female births [2, 3]. MRKH syndrome is classified into two types: Type I (56%–72%) with no associated malformations, and Type II (28%–44%) with related malformations affecting the nephrological system (47%), skeletal system (12%), heart, and auditory system resulting in deafness [4, 5]. Although a previous study identified genetic variations associated with the Type II cases of MRKH syndrome with renal malformations, the exact etiology remains unclear [6]. Patients are commonly diagnosed with MRKH syndrome in their teens or twenties when they visit an obstetrics and gynecology clinic for primary amenorrhea or apareunia [7]. Hence, vaginoplasty is an option to restore sexual function [8].
Additionally, due to the young age at which these patients were diagnosed and the unique nature of their conditions, they frequently have difficulty accepting the disease and deciding to undergo surgery. Moreover, outpatient care and surgical procedures are uncommon due to the rarity of the disease. Therefore, this study reviewed the cases and considered the factors to support the management of MRKH syndrome from the viewpoints of surgical techniques, postoperative management, and outpatient follow-up procedures.
This retrospective observational study reviewed the surgical techniques, surgical outcomes, postoperative management methods, and outpatient follow-up of 17 patients with MRKH syndrome using the medical records at Keio University Hospital. The Ethics Committee of our institution approved the study (Approval numbers: 20070081, 20150105).
The patients were 15–33 years (median 18 years) when they were first referred to our institution for consultation. Although eight patients were previously diagnosed with MRKH syndrome, they were under observation and referred to our institution for vaginoplasty. While four cases were referred to our institution for further management because of suspected MRKH syndrome, in which three cases were unclear, and two were suspected of having myoma.
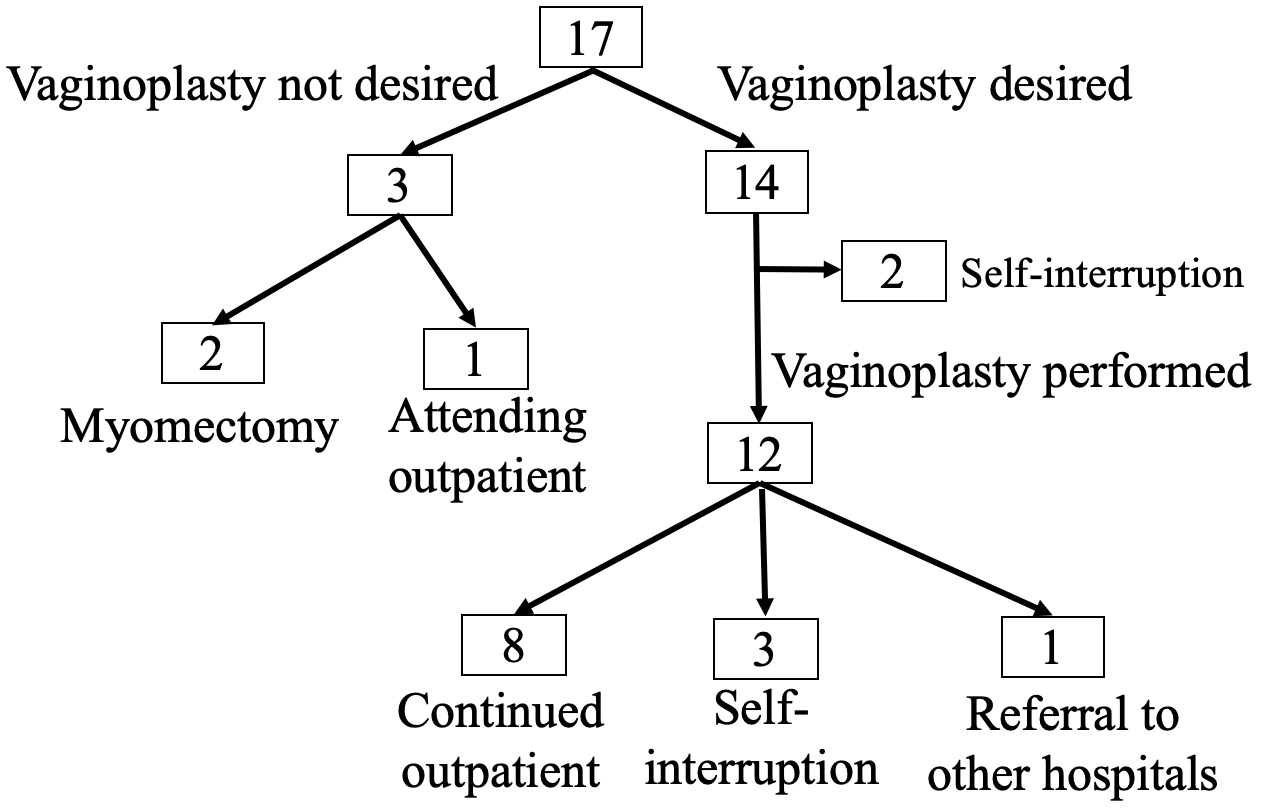
Fig. 1 presents the clinical course of the 17 cases. Pelvic magnetic resonance imaging and intra-venous pyelography revealed all cases were Type I of MRKH syndrome. Of the 14 patients who requested vaginoplasty, 12 underwent surgery, and two patients self-interrupted during outpatient visits for preoperative vaginal dilatation. Subsequently, while eight patients continued outpatient visits after vaginoplasty, three patients self-interrupted their outpatient visits, and we referred a patient to another hospital. Nevertheless, all patients achieved anatomical success with a vaginal cavity length of 6 cm or more (Fig. 2) and could have sexual intercourse with their sexual partners. Since two patients presented myoma at uterine traces, they underwent myomectomy.
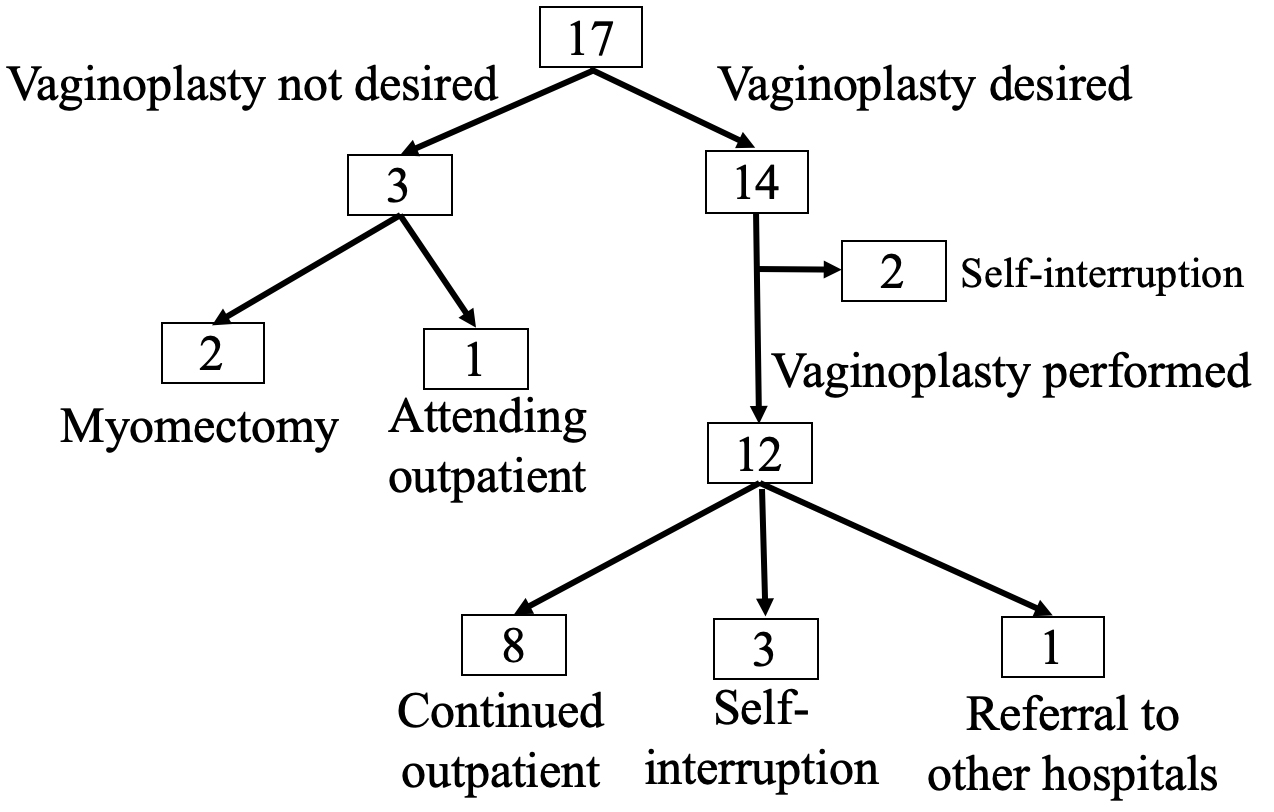 Fig. 1.
Fig. 1.The clinical course of the 17 cases of MRKH syndrome. Of the 14 patients who requested vaginoplasty, 12 underwent surgery, and two self-interrupted during outpatient visits for preoperative vaginal dilatation. Then, of the 12 patients who underwent surgery, eight continued outpatient visits after surgery, three self-interrupted outpatient visits, and one patient was referred to another hospital. One patient would be scheduled for surgery immediately after her work schedule settles. Furthermore, two patients underwent myomectomy for myoma in uterine traces.
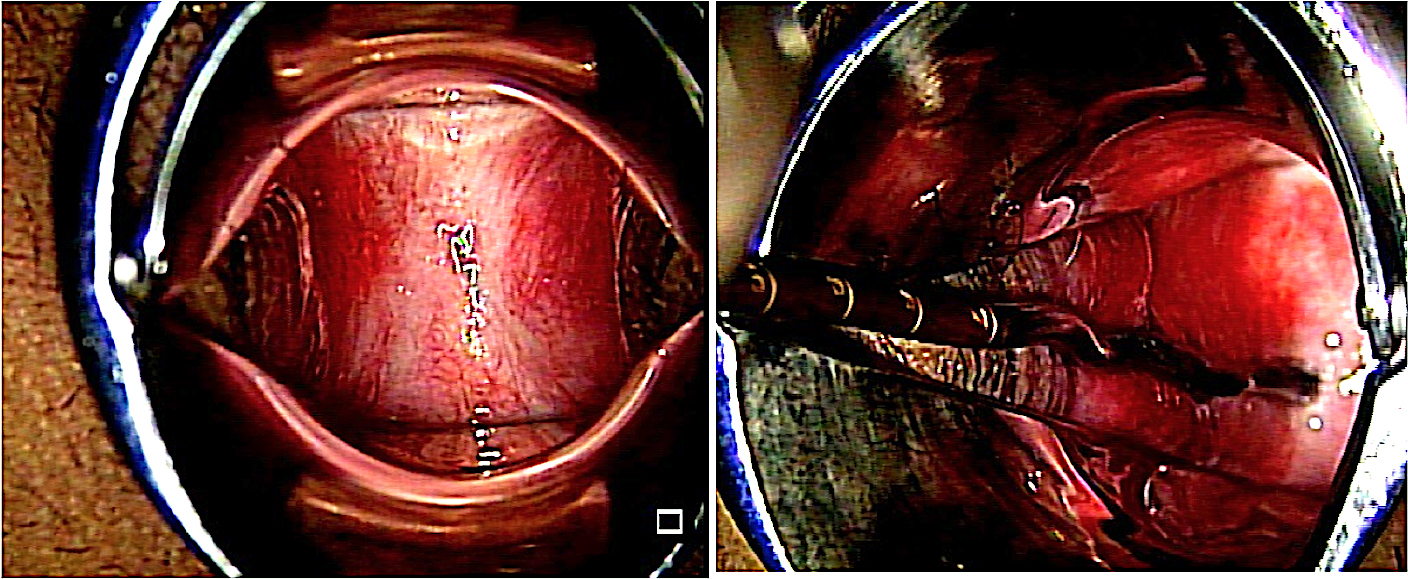 Fig. 2.
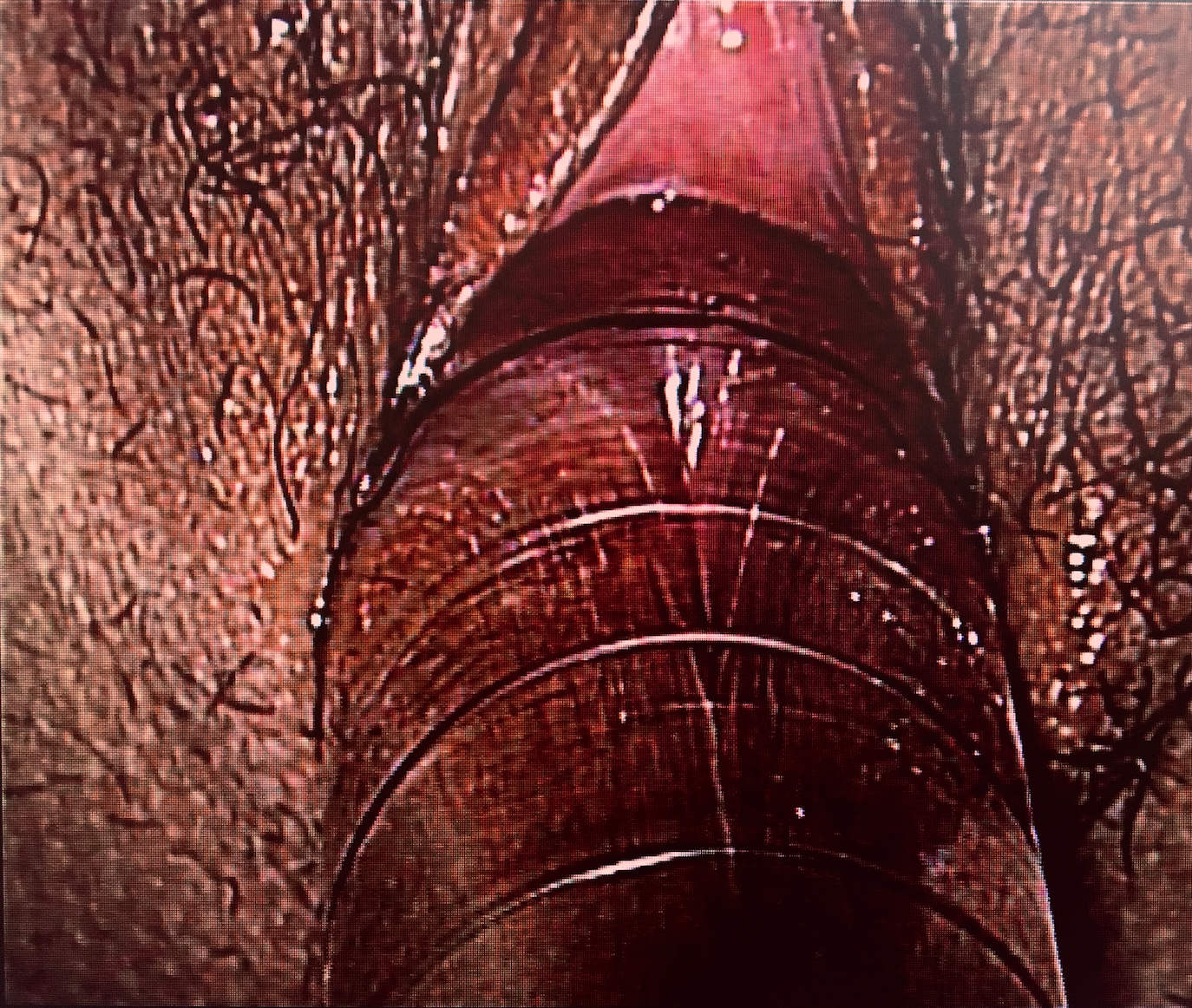
Fig. 2.The vaginal cavity 4 years and 9 months postoperatively. The length was about 7 cm.
Several surgical techniques for vaginoplasty have been adopted (Table 1). Although each method has its advantages and disadvantages [7, 8], we conducted Davydov’s modified procedure, a laparoscopic-assisted pelvic peritoneal approach. We adopted this procedure because of the relatively short period of peritoneum epithelialization. We also performed vaginal dilatation before surgery using the Frank method [9], which involved compression and stretching of the vaginal mucosa using an instrument (Figs. 3,4) in an outpatient setting and waiting 17 months to 34 months (median two years) for the vaginal cavity to enlarge by 5–6 cm.
| Frank | Mclndoe | Ruge | Davydov | Vecchietti | |
|---|---|---|---|---|---|
| Vaginal formation tissue | Vestibular mucosa | Skin, Artificial dermis | Sigmoid colon | Peritoneum | Vestibular mucosa |
| Advantage | Minimally invasive | Relatively minimally invasive | No vaginal stenosis and shortening | Early sexual intercourse possible | Vaginal formation in a short period |
| Disadvantage | Long treatment period | Postoperative self-dilation | Unpleasant discharge, High infection rate | Postoperative self-dilation | Special equipment required |
 Fig. 3.
Fig. 3.Hegar Cervix Dilator. Start around #20 and gradually work up to #30.
 Fig. 4.
Fig. 4.Schematic presentation of the Frank method. Compression and stretching of the vaginal mucosa using a Hegar Cervix Dilator.
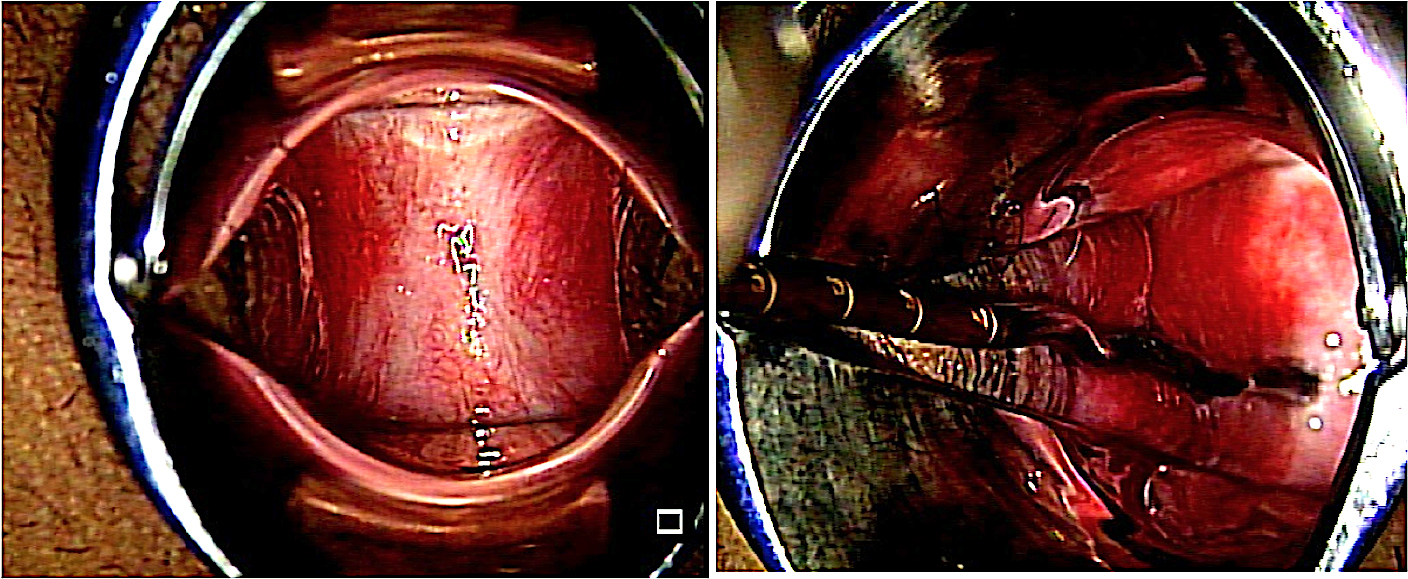
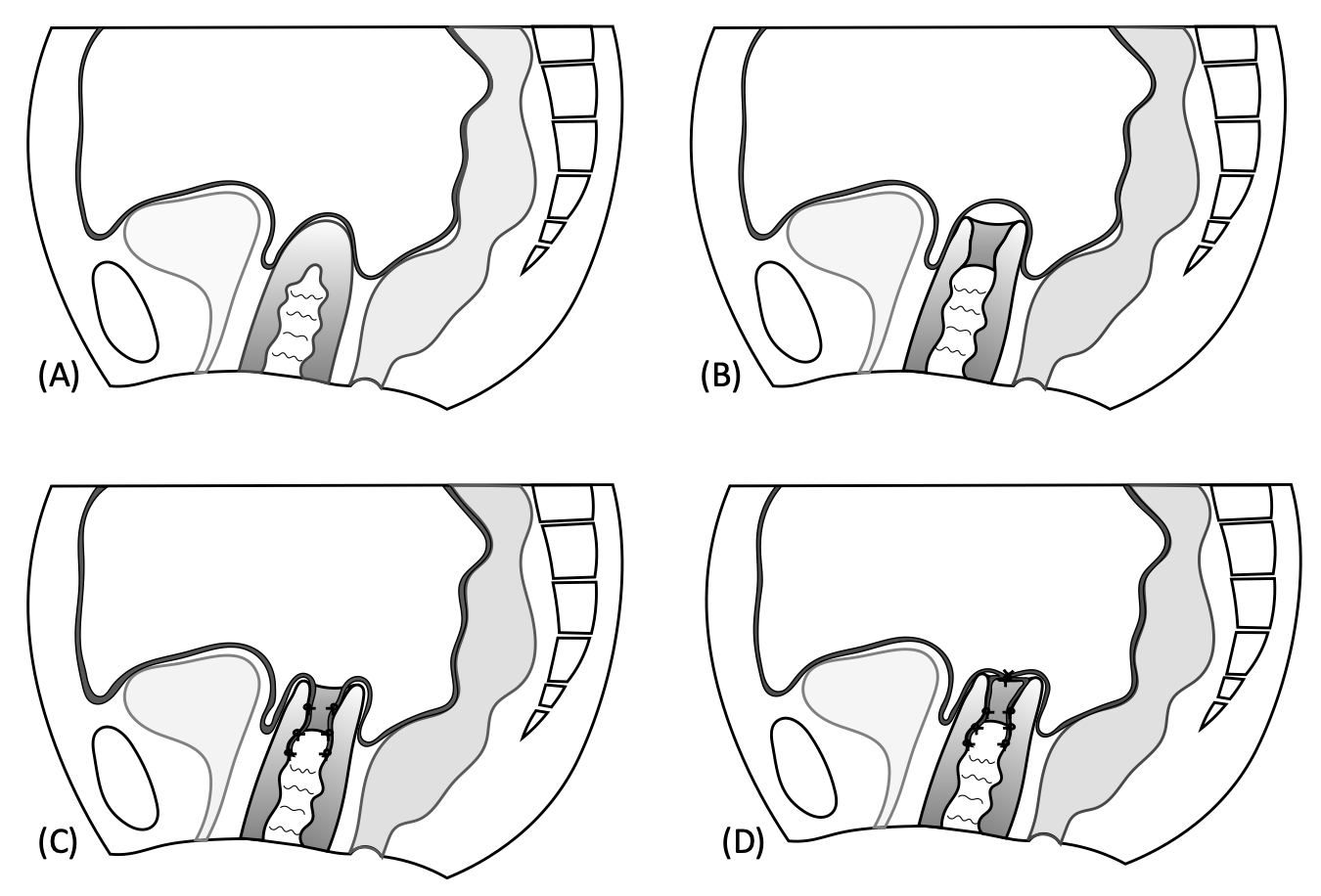
Below is the schematic presentation of Davydov’s method (Fig. 5) and intraoperative findings of Davydov’s modified procedure (Fig. 6). Initially, we observed the abdominal cavity through laparoscopy. Then, vaginal manipulation was performed to form a vaginal cavity. Later, a 1 cm lateral incision was made at the back of the vaginal wall, resulting in connective tissue expansion with Kelly forceps, after which the peritoneum, identified at the back of the cavity and estimated to be the Douglas fossa, was detached so that it became a single peritoneum. After confirming the position laparoscopically, the peritoneum was perforated through vaginal manipulation, and the pelvic peritoneum was sutured and fixed at the vaginal entry site. Additionally, after the prosthesis was inserted into a new vaginal cavity, the vaginal end was formed laparoscopically. Finally, the uterine serosa was sutured from both sides to the anterior rectal serosa at the midline.
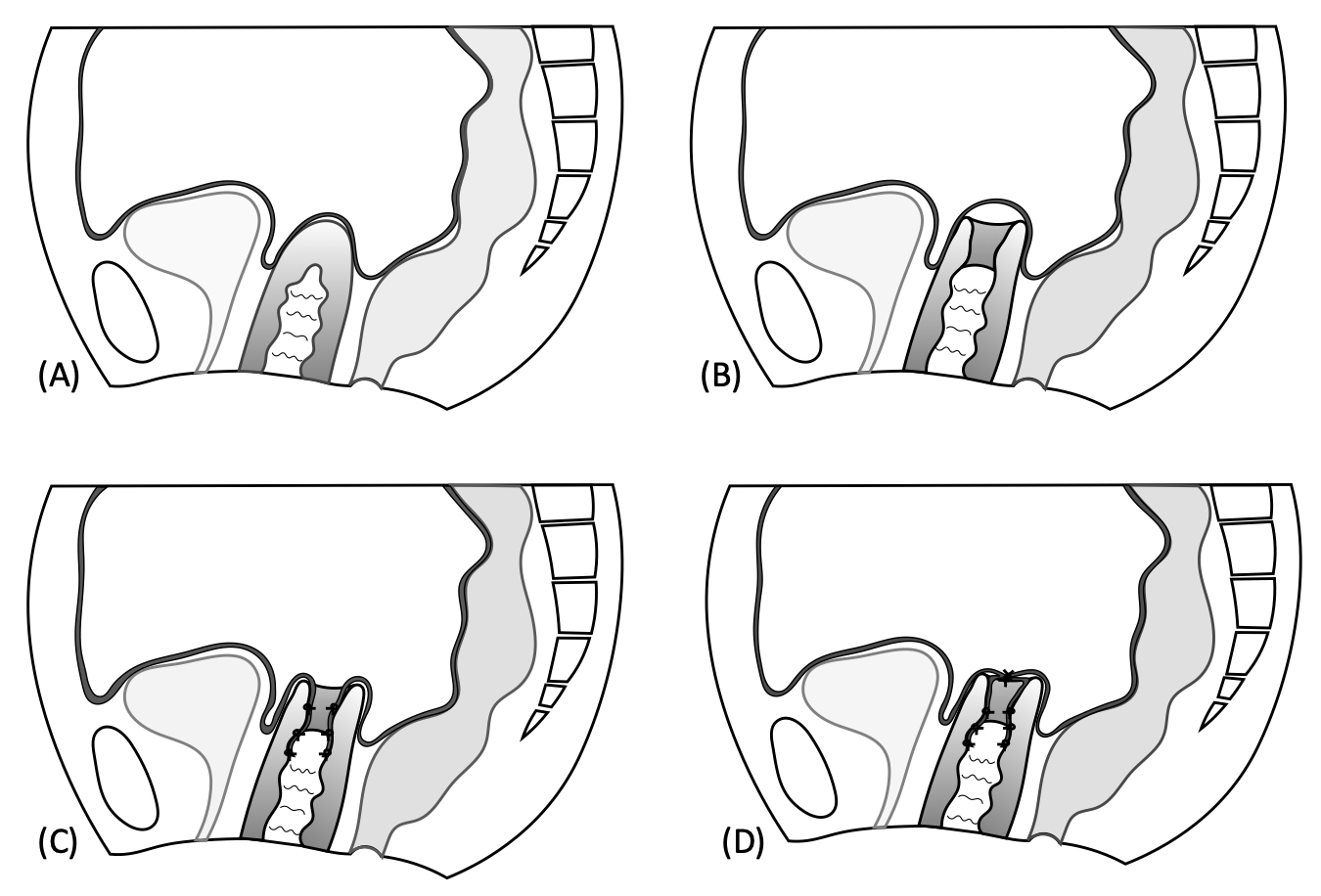 Fig. 5.
Fig. 5.Schematic presentation of Davydov’s method. (A) Vaginal canal along the anterior wall of the rectum. (B) Once the peritoneum was reached, peeled off the peritoneum to form a single piece. (C) Dissected pelvic peritoneum was suture-fixed to the vaginal opening. (D) A prosthesis was inserted, and the cysto-uterine fossa peritoneum and Douglas fossa peritoneum were sutured to form the vaginal end.
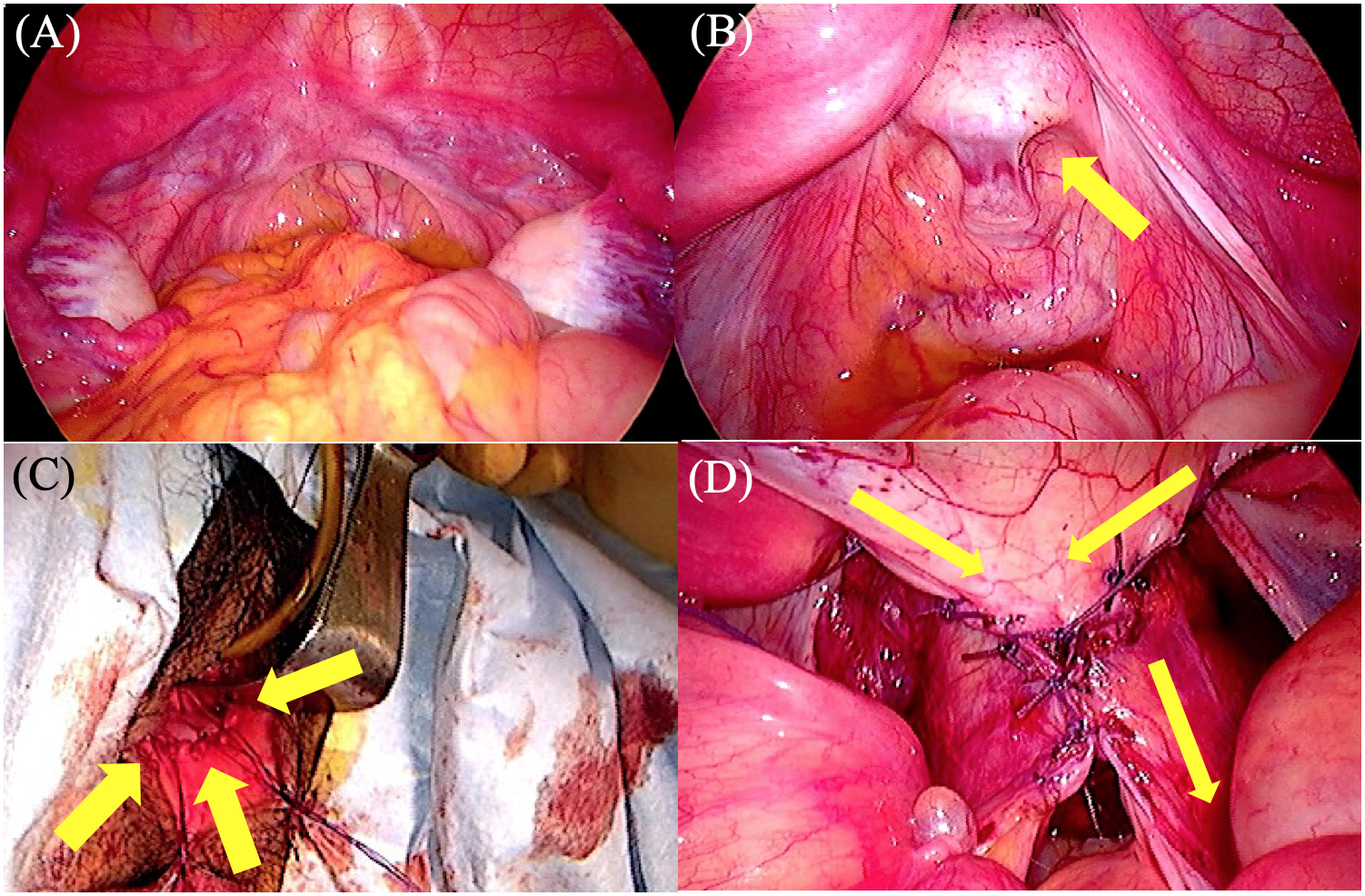
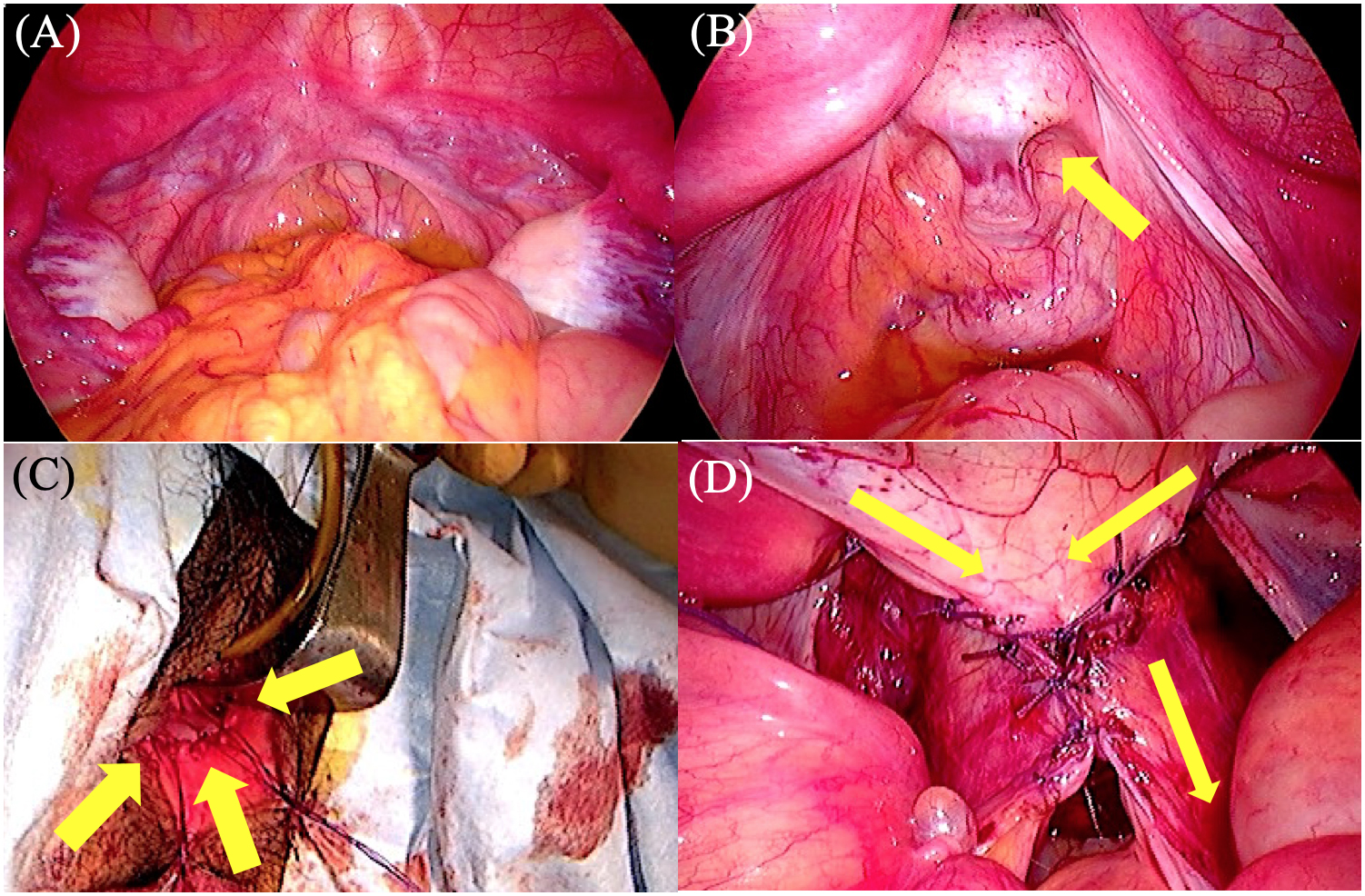 Fig. 6.
Fig. 6.Intraoperative findings. (A) Uterine traces were observed on the right and left pelvic walls, as a cord-like tissue on the pelvic floor and normal bilateral adnexa. (B) The vaginal cavity was formed through vaginal manipulation. The peritoneum, estimated to be the Douglas fossa (arrow), was identified at the back of the cavity. (C) Suturing and fixation of the pelvic peritoneum at the vaginal entry site (arrows). (D) Suturing of the uterine serosa from both sides to the anterior rectal serosa in the midline as the direction of the arrows.
The age at surgery was 18–27 years (median 22 years), the operative time was 3 h 24 min–6 h 5 min (median 3 h 51 min), and the bleeding was small–3800 mL (median 112 mL) (Table 2). One patient lost 3800 mL of bleeding from the 9 o’clock plexus vein, which is the hypervascular area around the rectum and between the bladder and rectum, and she needed a blood transfusion during vaginal formation.
| Period required for the preoperative Frank method | 2 Y (1 Y 5 M–2 Y 10 M) |
|---|---|
| Age (years) | 22 (18–27) |
| Surgery time | 3 h 51 min (3 h 24 min–6 h 5 min) |
| Bleeding (mL) | 112 (Small amount–3800) |
| Intraoperative complications | Bleeding (3800 mL) that needed blood transfusion: 1case |
| Postoperative complications | Difficult to remove the prosthesis that needed to be removed under anesthesia: 4 cases |
| Note: Data are shown as median (range).
Abbreviations: Y, year; M, month. | |
The postoperative management of MRKH syndrome is essential. At our institution, we began vaginal lavage and disinfection 2–3 d after surgery. Then, we tried rotating the prosthesis. Immediately after discharge, patients visited the hospital once or twice weekly to remove granulation and rotate the prosthesis to prevent adhesions. Subsequently, the patients were subjected to intermittent dilatation with a dilator at 2–3 months after surgery when the peritoneum became squamous, and intermittent hospital visits were encouraged afterward. Once her condition became stable, she was advised to visit the hospital every six months. Although we replaced the prosthesis to a smaller size under anesthesia in four cases (lumbar anesthesia in three and intra-venous anesthesia in one) due to narrowing of the vaginal entry or partial adhesions to the prosthesis within one month after surgery, all cases could achieve anatomical success.
Because of the need for prolonged outpatient visits before and after surgery, regular outpatient follow-up visits are also essential. Five cases self-interrupted their hospital visits, in which two were preoperative and three postoperative. Of the two preoperative cases, one started the Frank method at 18 years as an outpatient. However, she visited again at her 22 years since she had a partner and resumed the Frank method. Still, she self-interrupted again after two months. In another case, although MRKH syndrome was suspected in high school, she did not visit a higher institution and did not consult with her parents or others around her. Nevertheless, she visited her previous doctor at age 33 for primary amenorrhea. Therefore, she was referred to our institution for further management, after which she started the Frank method for surgery. However, she self-interrupted after six months.
Moreover, we observed the three postoperative loss-to-follow ups patients who had been receiving the treatment for several years and had achieved anatomical success. Among the patients, one patient was scheduled for surgery as soon as her work schedule settled. She was diagnosed with MRKH syndrome at 15 years old after a visit to the hospital for primary amenorrhea. Since she was a junior high school student, the condition was explained only to her mother and then to her 19 years old after graduating high school.
Notwithstanding, the patient could not face the condition directly and was reluctant to undergo vaginoplasty. Therefore, we took time for nursing consultations and shared information, which resulted in continuing the Frank method with regular outpatient visits and planning the surgery after her work became more settled. Additionally, a case had a baby by surrogate conception abroad since no way had been discovered for patients with MRKH syndrome to conceive and give birth in Japan.
The vaginoplasty in MRKH syndrome aims to create a sexually viable vagina through the safe and uncomplicated procedure. The enlargement procedures reported for vaginal hypoplasia included surgical vaginoplasty and non-surgical dilation therapy. A systematic literature review reported that the non-surgical dilation therapy has success rates of 78% and complication rates were significantly lower than the vaginoplasty techniques [8]. Another paper repoted that only 4 of 60 (7%) patients treated with self-dilation, that later needed surgery [10]. Since 2002, the American College of Obstetricians and Gynecologists has recommended non-invasive dilation as a first-line treatment due to the low risk of complications and lack of hospitalization [11]. However, the Frank method (one of the non-surgical dilation) may result in comparatively shorter vaginas than surgery [8, 12, 13], and there are also reported that 61% of the patients needed an additional surgical vaginoplasty [14].
Although there are several surgical vaginoplasty methods, no one is perfect. Differences between these methods are the vaginal forming tissue that replaces the vaginal mucosa, such as using a skin valve or artificial dermis in the McIndoe procedure [15], using the sigmoid colon like in the Ruge method [16], using the pelvic peritoneum like in Davydov’s procedure [17], then the Vecchietti procedure [18] where traction of the vaginal vestibular mucosa is conducted. Each facility adopts a method that they are accustomed to conducting. We adopted Davydov’s modified procedure because of the easy procedure with no risk of peritoneal flap necrosis and rejection. Moreover, this procedure takes a relatively short period of peritoneum epithelialization, allowing patients to have early sexual intercourse.
We made the following contrivances in performing Davydov’s modified procedure; first, peritoneum extension procedure; second laparoscopic usage; and finally, postoperative management.
As the peritoneum has high regenerative powers and can undergo squamous metaplasia when exposed to the external environment, metaplasia to the normal squamous epithelium is almost complete by three months after surgery [19]. However, to obtain and move adequate peritoneum to cover the wall of the neovagina, Davydov’s modified procedure requires the mobilization of a relatively wide range of pelvic peritoneum. Therefore, we performed vaginal dilatation before surgery using the Frank method to 5–6 cm to ensure sufficient vaginal length with less perineum. Moreover, the pelvic peritoneum was detached on both sides to ensure the length of the peritoneum. Subsequently, the uterine serosa was sutured from both sides to the anterior rectal serosa at the midline to allow room for the vaginal canal and provide adequate strength.
Using laparoscopy prevents damage to other organs and facilitates surgical operations. We use a laparoscope with several points in mind. When forming the vaginal cavity, the point is to expand along the anterior wall of the rectum under the light source of the laparoscope and be careful not to damage the lateral “venous plexus”, which is hypervascular areas around the rectum and between the bladder and rectum. It is not an anatomical name as the anatomy of MRKH syndrome is different from the usual in the first place. The previous study has reported that the blood vessels are clustered around the uterine traces in patients with MRKH syndrome, so it is essential to carefully evaluate the running of the vessels in close proximity [20]. Notably, before perforating the peritoneum vaginally, grasping the point with laparoscopic forceps helped to identify the area. Subsequently, when fixing the pelvic peritoneum to the vaginal entry site, threads were spun to the peritoneal end laparoscopically, after which they were pulled from the vaginal entrance and sutured at the vaginal entry site. This step made the procedure more accessible, rather than performing all procedures vaginally. Nevertheless, one case required a blood transfusion due to bleeding from the venous plexus, which was due to the difficulty with hemostasis, included an injury to the venous plexus in the lateral vaginal area, the narrow field of view for vaginal manipulation, and the enlargement of the laceration due to the vaginal speculum.
A previous study on Davydov’s procedure reported 92% anatomical success with
postoperative complications such as granulation of the vaginal canal (8.7%),
vaginal stenosis (5.1%), urethral injury (3.8%), rectovaginal or vesicovaginal
fistula (1%), urinary retention (1%), and prosthesis loss into the abdominal
cavity (
Postoperative management of vaginoplasty is essential to prevent vaginal narrowing and shortening, which determines the success or failure of the treatment. Infection prevention is more critical than conventional surgery, as vaginal infections can lead to scarring or adhesions due to granulation. Our hospital prevented the infections by frequent vaginal lavage and disinfection. However, four outpatients for whom the prosthesis could not be removed as an outpatient due to severe pain when attempting to remove the prosthesis and narrowing or partial adhesion of the vaginal entry site. In these cases, the peritoneum got epithelialized without recurrent adhesion after we replaced the prosthesis with a smaller size (M to S) under anesthesia. Eventually, they could move to the next phase, where they dilate intermittently using a dilator. Frequent removal of the granulation is needed to prevent partial adhesion, which occurs immediately after the surgery. As for the length of time of prosthesis implantation, previous studies have reported that continued dilatation with a dilator after three months of prosthesis implantation can prevent the shortening of the vaginal canal and maintain sufficient vaginal canal length [21]. Since sexual intercourse is associated with maintaining the length of the vaginal cavity, patients without a sexual partner should continue self-expansion.
The problems regarding outpatient discovered in this study were the difficulty of accepting the disease and making treatment decisions, including self-interruption of intermittent outpatient visits due to the long period before and after surgery. Previous studies have shown a positive effect of psychosexual interventions on MRKH syndrome patients [22, 23]. In the case of our institution, nurses took time to ask about the life background, such as study and work, understanding and acceptance of the disease or treatment, and provided information as needed during outpatient visits. Through this study, we consider the importance of providing information appropriate to patients’ mental maturity, providing mental support concurrently with treatment, and planning surgery according to their life stages, such as study and work. Thus, they could maintain motivation for successful treatment.
Concerning pregnancy and childbirth, adoption is the only option in Japan. Besides, although surrogate conception is possible abroad, many ethical and social issues have been observed. Nevertheless, some techniques, such as uterine transplantation, are under study [24]. It is hoped that future medical advances or changes in ethical and social attitudes toward reproductive medicine will lead to the favorable consideration of these methods.
Since this is a single-institution case series, we hope for a national approach in the future. Currently, we evaluated the effect of the operation by asking patients in an outpatient setting whether they have anatomical success and whether they can have sexual intercourse with their partners. In the future, it is desirable to evaluate these patients more objectively using the Female Sexual Functioning Index and the revised Female Sexual Distress Scale (FSDS-R) with a long-term follow-up survey.
We can consider that Davydov’s modified procedure is effective and that dilating the vaginal cavity using the Frank method adequately before surgery and taking care of the plexus vein during the operation is essential. Comprehensive psychological support at outpatient is also necessary.
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
These should be presented as follows: YK designed the research study. AM, YK, KI, TY MY, SH and WY acquired the data. AM and YK analyzed the data. AM wrote the manuscript. KN created Fig. 5. YK, KB and DA provided help and advice. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript.
This study was conducted with approval from the Ethics Committee of Keio University School of Medicine. (Approval numbers: 20070081, 20150105).
We would like to express our gratitude to all those who helped us during the writing of this manuscript.
This research received no external funding.
The authors declare no conflict of interest.