





 , Andrzej Matyja 2, Czesław Osuch 2, Maciej Matyja 2
, Andrzej Matyja 2, Czesław Osuch 2, Maciej Matyja 21 Department of General Surgery, Regional Specialist Hospital, 42-218 Częstochowa, Poland
2 Department of General, Oncologic, Metabolic and Emergency Surgery, Jagiellonian University Medical College, 31-109 Kraków, Poland
Academic Editors: Laura Avagliano and Tengiz Charkviani
Abstract
Diastasis recti abdominis (DRA) is an acquired condition defined as a thinning, widening and protruding of the linea alba following an increase in intra-abdominal pressure. The aim of this review is to provide insight in the pathophysiology, risk factors, diagnostic methods and treatment modalities of DRA. DRA occurs in both women and in men, however, it is extraordinarily common and even expected condition affecting over half of women during pregnancy and one third 12 months after childbirth. There is no consensus of risk factors for DRA. Proposed risk factors include multiparity, maternal age and high age, caesarean section, macrosomia, multiple pregnancy, ethnicity, heavy lifting, body mass index (BMI) and diabetes. To diagnose the presence of DRA and its severity the interrecti distance (IRD) is measured. Palpation, caliper, ultrasound, computed tomography (CT) and magnetic resonance (MR) are applied to measure IRD and exclude concurrent hernias. DRA is mostly treated conservatively by physiotherapists. However, physiotherapy is unlikely to prevent or completely treat DRA. Over four fifth of patients are unsatisfied with the results of training programmes and opted for surgical intervention. Thereby the main purpose of physical training is to restore function, not to reduce the DRA. Physiotherapy may be an alternative for those who cannot undergo surgery. In case if severe cosmetic and functional impairment patients are referred for surgery. Patients with severe symptoms benefit more from surgery. Surgery is challenging since guidelines almost do not exist. Plication and mesh reinforcement are recommended by most authors, however whether it should be open or laparoscopic remains debatable.
Keywords
- diastasis recti abdominis (DRA)
- physiotherapy
- surgery
- abdominal wall reconstruction
- midline reconstruction
- midline plication
- abdominoplasty
Diastasis recti abdominis (DRA) is an acquired condition defined as an increase in width of the linea alba [1, 2]. Thinning, widening and protruding of the linea alba follow an increase in intra-abdominal pressure. It is combined with laxity of the ventral abdominal musculature [2, 3]. Two bellies of the rectus abdominis are separated along the midline of linea alba by an abnormal distance, but with no facia defect (Fig. 1) [2, 4]. It is debatable whether DRA is to be considered a pathological condition or a natural part of aging [2].
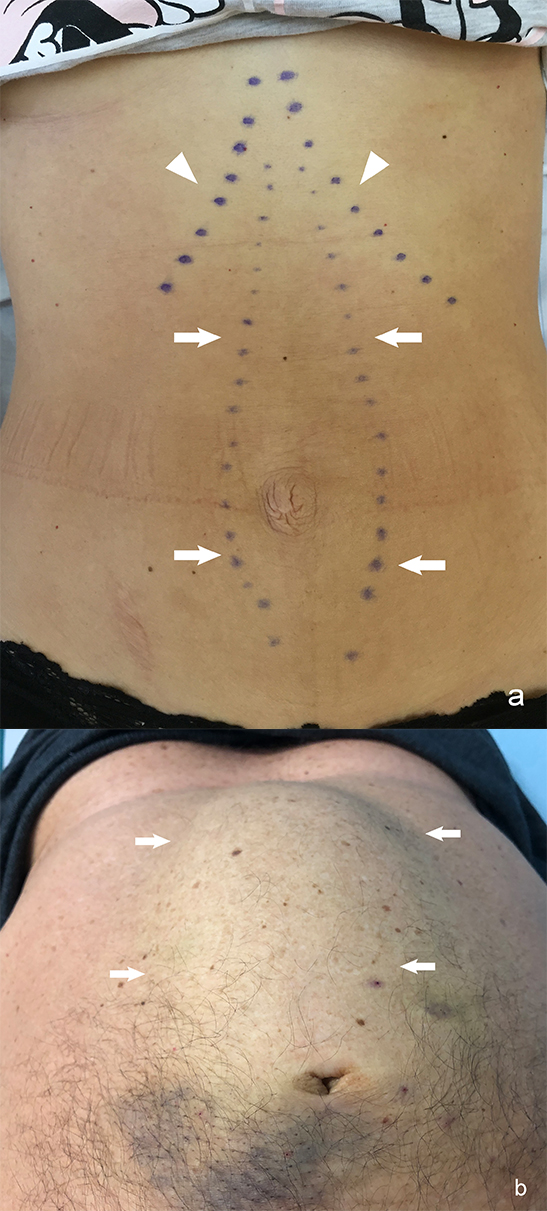 Fig. 1.
Fig. 1.Diastasis recti abdominis (DRA) in relaxed state. (a) During curl up. (b) Arrows–medial margins of rectus muscles; arrowheads–costal arches.
DRA occurs in both women and in men [5]. However, it is extraordinarily common condition affecting a significant number of women during pregnancy and in the postpartum period [4, 6, 7]. The prevalence has been reported to be 60% and 30% six weeks and one year postpartum, respectively. Despite the high prevalence, the exact etiology and risk factors are still debatable [4].
DRA can be misclassified as a primary ventral hernia [3]. The musculofascial continuity of the linea alba and subsequent absence of a true hernia sac is what sets DRA apart from ventral hernia [2, 3]. Patients with DRA can experience similar complaints, such as functional and cosmetic impairment, and lower back pain as patients with ventral hernia [3]. DRA itself is associated with increased risk of developing epigastric and umbilical hernia [2, 7]. Muas [8] found that DRA was associated with midline hernias in 100% of their patients. Additionally in a series of small epigastric and umbilical hernias concomitant DRA was diagnosed in 45% of patients [9].
DRA may occur along the full length of the linea alba or be limited to the above-navel or below-navel segment [10]. Corvino et al. [1] found that the above-navel DRA is the most common presentation and even when diastasis is open completely, it is usually wider above the navel (Fig. 2). This may be explained by the smaller number of transverse fibers in the supraumbilical linea alba [2].
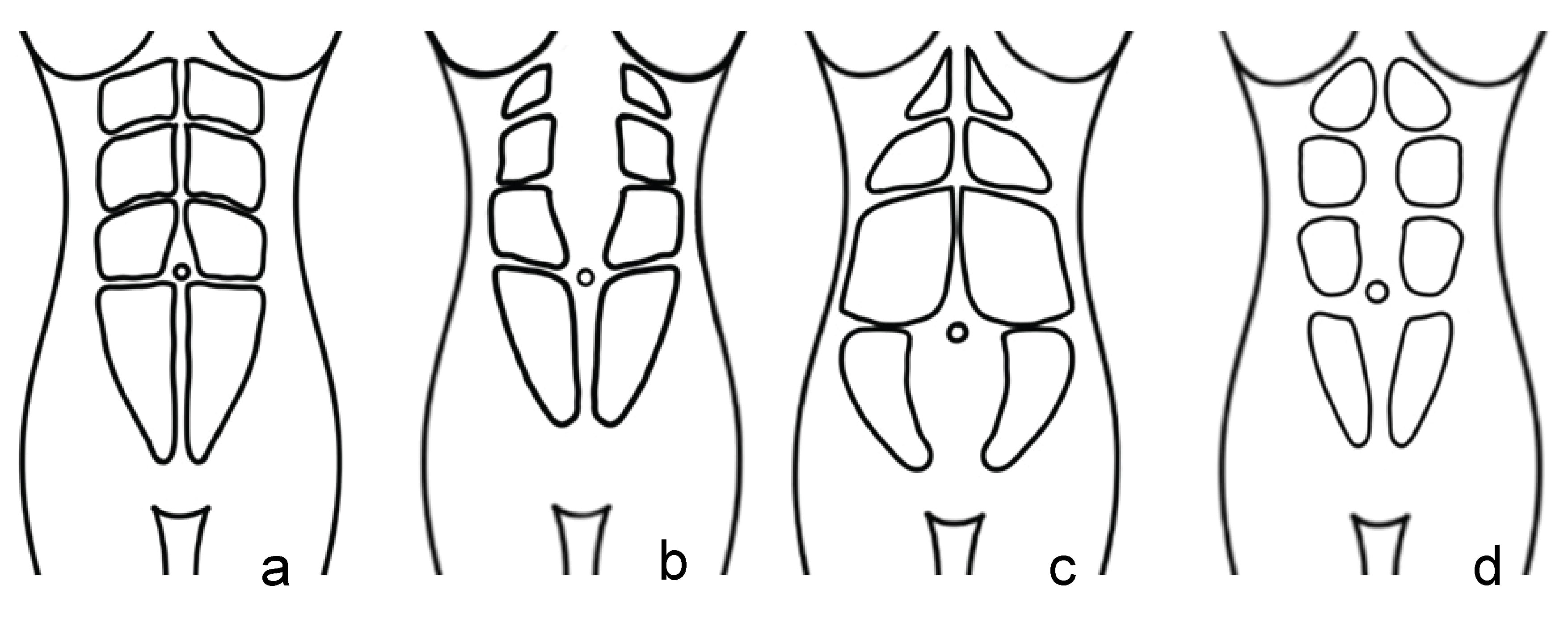 Fig. 2.
Fig. 2.Rectus abdominis muscles: correct position. (a) Above-navel DRA. (b) Below-navel DRA. (c) DRA along the full length of the linea alba. (d) DRA–diastasis recti abdominis.
The aim of this review is to provide insight in the pathophysiology, risk factors, diagnostic methods and treatment modalities of DRA and to point what the future studies could be focused on.
Although found in both males and females, DRA occurs most frequently during pregnancy [2, 3]. It is a common and even expected condition during pregnancy, caused by hormonal changes, increased intra-abdominal pressure and mechanical stretching of the abdomen [6, 7]. The linea alba expands and abdominal wall undergoes substantial changes as the pregnancy progresses [2, 11]. The bellies of rectus abdominis elongate and curve round while the abdomen expands to accommodate growing fetus [2, 11]. In most women DRA regresses spontaneously after childbirth [3]. Sparstad et al. [5] report prevalence of DRA was 33.1%, 60.0%, 45.4% and 32.6% at gestation week 21, 6 weeks, 6 months and 12 months after delivery, respectively. Moreover, DRA has been found in 52% of urogynecological menopausal patients [12]. Data for nonparturient woman and men are rare [2]. Altered collagen ratio, genetic predisposition and prolonged transverse stress on the linea alba may play a role in DRA etiology in males [3, 11].
DRA may affect physical function and quality of life [6, 8, 13]. It has been suggested that DRA is associated with urinary incontinence, lower back pain, lack of trunk strength, body dissatisfaction and significantly impaired quality of life [6, 10, 11, 14]. However, whether DRA actually causes these symptoms or coexists remains unclear [6]. There is only weak evidence that DRA severity is associated with impaired abdominal muscle strength and severity of low back pain [4]. Sparstad et al. [5] pointed that mild DRA is not associated with lumbopelvic pain and women with DRA were not more likely to report lumbopelvic pain 12 months postpartum compared with women without DRA [2, 5]. Benjamin et al. [15] distinguished no association between the presence of DRA and lumbopelvic pain and incontinence, while Braga et al. [16] excluded DRA as a risk factor for stress urinary incontinence.
There is scant knowledge and no consensus of risk factors for DRA [2]. Proposed
risk factors include multiparity, maternal age and high age, caesarean section,
macrosomia, multiple pregnancy, ethnicity, heavy lifting, BMI and diabetes
[2, 5, 6, 15]. Cesarean section seems to be a risk factor only for women who have
given birth twice [2]. Diabetes causes loss of muscle mass and sarcopenia what
may lead to DRA [2]. Sparstad et al. [5] found no difference in risk
factors and reported lumbopelvic pain when comparing women with and without DRA.
They suggest a greater likelihood of DRA only among women reporting to be exposed
to heavy lifting
To diagnose the presence of DRA and its severity the interrecti distance (IRD) is measured [4]. Palpation, caliper, ultrasound (Fig. 3), CT (Fig. 4) and MR are used to measure IRD [2, 4]. To date there is no consensus which method should be applied. Swedish national guidelines recommend diagnosis using caliper or ruler for measurement. Ultrasound or other imaging modality is recommended when concomitant hernia is suspected [7]. Corvino et al. [17] promote the use of dynamic ultrasound in case of suspected hernia. They point that computed tomography is a static examination, while dynamic ultrasound could demonstrate the movement of abdominal contents [17]. The finger-width method is widely used, as it is economical and relatively convenient [2]. However, ultrasound, CT or MR to measure IRD are more accurate and may exclude any concurrent ventral hernia [2, 6].
 Fig. 3.
Fig. 3.Interrecti distance (IRD) measured by ultrasonography: correct IRD 8 mm. (a) Examples of diastasis recti abdominis (DRA). (b–e) IRD 66 mm. (b) IRD 74 mm. (c) IRD 82 mm during curl up. (d) IRD 52 mm in pregnant woman. (e) Arrows–medial margins of rectus muscles, arrowheads–protruded linea alba during curl up.
 Fig. 4.
Fig. 4.Interrecti distance (IRD) measured by computed tomography: IRD 56 mm.
There is no consensus on the exact cut-off point to diagnose DRA and where
exactly IRD should be measured [2, 4, 6, 7]. DRA is defined in the literature by
different authors as IRD greater than 22–30 mm [6, 11, 18]. Additionally, IRD is
measured on different levels, above or below the umbilicus. Some authors report
IRD during a curl-up, while the majority of authors measure it in relaxed state
[4]. Due to these discrepancies, to date there is scant knowledge on exact
prevalence of DRA [5, 11]. According to the prevalent classification by Beer
et al. [18] DRA is defined as an IRD of
DRA is mostly treated conservatively. Patients referred to a physiotherapist receive training programmes that specifically target reducing IRD [3]. Frequency of the recommended training programmes varied between studies. Some studies recommend training with physiotherapist, while others let patients train on their own [3, 20]. Recommended frequency of training sessions varied from one to five sessions per week [3]. There is limited scientific knowledge of which exercises to recommend in the treatment of DRA [19]. The exercise intervention was focused on various core trainings, breathing technique and mindfulness teaching [10]. The most recommended exercises by women’s physiotherapists were exercises targeting the transversus abdominis and pelvic floor muscles, like curl-up leading to an immediate decrease in IRD [4]. Gluppe et al. [19] found that head lift, twisted curl-up and curl-up exercises decreased the IRD both above and below the navel. However, though all studies reported a decrease of IRD, follow-up was performed directly after the training programme end [3]. Whether the exercises may cause a permanent reduction in IRD is unknown [19].
Furthermore, despite decrease of IRD Emanuelsson et al. [21] reported that 87% of patients were unsatisfied with the results of training programmes and opted for surgical intervention. Mommers et al. [3] found in the literature no strong evidence of the successful treatment of DRA following a physiotherapy training programme what explains why over 80% of patients in the training group were unsatisfied and opted for surgical intervention. It is suggested that physiotherapy can moderately reduce IRD only during muscle contraction. However, impact of this finding on function outcome, cosmesis, satisfaction or quality of life is unclear [3]. Gluppe et al. [4] concluded in randomized controlled trial of 381 women that there is very low-quality scientific evidence to recommend specific exercise programs in the treatment of DRA postpartum. Therefore, physiotherapy may be a useful addition to surgery or an alternative to surgery for those who are unable to undergo surgery.
Kamel et al. [22] found that neuromuscular electrical stimulation helps to reduce DRA in postnatal women, if combined with abdominal exercises. However, there is no strong evidence that DRA severity is associated with impaired abdominal muscle strength [4]. There is no difference in the fulfilling the recommendations for general exercise, strength training or specific floor muscle training when comparing women with and without DRA [5]. Sparstad et al. [5] report no association between regular exercise and DRA. There is only weak evidence that training during pregnancy and during postpartum period can decrease risk of DRA [6].
The exercise intervention on DRA may play a role in treating the laxity of abdominal musculature affecting body weight and core function [9, 23]. Women who perform more physical training have greater endurance and trunk strength [11]. Training programs lead to significant increases in physical function, although cosmetic improvement is limited [4, 7, 21]. It is not likely that rehabilitation would have had any significant impact on DRE improvement. Conservative management including training and weight loss is generally advised first-line treatment [6]. Swedish national guidelines [7] recommend physiotherapy as a firsthand treatment for DRA. Evidence in the literature supporting physical training for DRA is inconclusive. Thereby the main purpose of physical training is to restore function, not to reduce the DRA [6].
Although associated with both functional and cosmetic disability, DRA poses no risk of strangulation [3, 7]. In case if severe cosmetic and functional impairment patients are referred to surgeons [3]. Patients with severe symptoms benefit more from surgery [6]. Olsson et al. [6] found that surgical reconstruction results in significant improvement in abdominal trunk function, urinary incontinence and quality of life. However, the indication for surgical treatment of DRA in the absence of concomitant ventral hernia is debatable [7]. Swedish national guidelines [7] recommend surgery in patients with functional impairment, but not until the patient has undergone a standardized 6-month abdominal core training program. Surgery may be recommended at least 2 years since last childbirth and future pregnancy should not be planned. These guidelines recommend to undertake surgery for DRA at least 5 cm wide [7]. In case of pronounced bulging or concurrent hernia, surgery may be considered for smaller DRA [7].
Several surgical techniques ranging from laparoscopic and endoscopic to open repairs may be considered [24, 25, 26]. There is no consensus on the preferred surgical management [3]. Mommers et al. [3] distinguish plication-based and hernia repair techniques. There is no clear difference in postoperative complications between them [3]. To minimize risk of recurrence Olsson et al. [6] instruct patient to wear a girdle day and night in weeks 1–8 and daytime only in weeks 9–12 postoperatively. Swedish national guidelines [7] recommend plication of the linea alba as the firsthand surgical technique. Plication could be either laparoscopic or open. Authors using laparoscopic plication technique used mesh reinforcement. Most of them used interrupted sutures instead of continuous ones. However, the difference in suture technique did not lead to difference in reported recurrence rates, which were 0% [25, 27, 28]. Open plication technique studies describe plication of different layers of the abdominal wall. In most studies open plication was combined with a sublay mesh, however open plication without mesh reinforcement was also described. Patients had undergone plication of anterior or posterior rectus fascia, combined with mesh reinforcement or not [24, 25, 26]. Some patients that suffer from excess skin should be referred for plication of linea alba combined with simultaneous abdominoplasty [3].
Postoperative complications of plication techniques were reported not in each study. Postoperative pain was reported in 10% of patients [28]. The plication techniques, in particular the laparoscopic ones, may leave a surplus of soft tissue clustered at the midline, which is a main limitation of these procedures [3, 29]. Carrara et al. [29] suggest not to correct skin excess at the time of abdominal wall reconstruction. A few months after surgery a skin fold is reduced due to scar remodelling and surgical correction of skin excess postponed to that time allows to avoid over- or under-treatment [29]. Olsson et al. [30] reported no recurrences after suture plication of the linea alba and functional improvement of this surgical reconstruction persisted for 3 years. Authors describe recurrences after open plication or laxity of the abdominal wall with protrusion of linea alba, what should be interpret as recurrent DRA [3]. Kerckhoven et al. [31] distinguish two kinds of recurrences. First is recurrence of DRA examined by ultrasound, while the second is abdominal wall protrusion assessed by clinical examination However the recurrences that require a reoperation are rare [31].
Hernia repair techniques for DRA are often modifications of the Chivrel and Rives-Stoppa techniques [3, 32, 33, 34, 35, 36]. Access to linea alba in a particular patient depends on body figure, surplus of excessive skin and anatomical conditions, and involve midline incision, low transverse incision and abdominoplasty including resection of excessive skin [6]. The complications are associated predominantly with abdominoplasty [31]. The most frequent complication was seroma (7%), followed by abdominal hypoesthesia (6%), chronic pain (4%), surgical site infection (2%). Mesh reinforcement may increase chronic postoperative pain [31]. Studies using a hernia repair technique reported no recurrences [3]. For surgical treatment for DRA associated with small midline hernia, including umbilical and epigastric hernias, most studies described suture closure of the hernia sac combined with mesh reinforcement [3]. However, laparoscopic plication of the midline in the anatomical plane between the subcutaneous tissue and the anterior rectus fascia, and onlay mesh reinforcement was also described [37, 38, 39, 40]. If reported, postoperative complications were seromas (2.5–23%) and only one recurrence [36].
Although cosmetic result of a surgical intervention is of high importance, it is not yet evaluated which surgical technique has the most satisfying cosmetic outcome [3, 13, 30, 41]. To date, despite the importance of cosmetic results, the majority (85%) of published cases are open ones [3]. Though new minimally invasive techniques have been also described. There are also reported some minimally invasive variation of classic procedures that leave minimal scaring, without abdominal cavity opening and risk of incisional hernia (Fig. 5) [3, 7, 27, 28, 39]. Malcher et al. [42] identified nine endoscopic techniques for DRA and ventral hernia repair, including Full Endoscopic Suprapubic Subcutaneous Access (FESSA) [43], Subcutaneous Onlay Endoscopic Approach [44], Pre-Aponeurotic Endoscopic Repair (REPA) [8], Total Endoscopic-assisted Linea Alba Reconstruction [45]. These techniques were differently named, but the surgical concept of subcutaneous endoscopic approach for both DRA and hernia repair was the same [42]. Under endoscopic vision the supra-aponeurotic space is dissected to expose linea alba [46]. Therefore Malcher et al. [42] proposed term Endoscopic Onlay Repair (ENDOR) to unify these procedures. These techniques were effective and safe, allow to resolve the defect without entering abdominal cavity, with good functional and cosmetic results [8]. The most common complication was seroma, pain requiring intervention, hematoma, and surgical site infection [42]. Endo-laparoscopic reconstruction of DRA is safe, effective [29]. Manetti et al. [47] published a pilot study of fully laparoscopic technique, which is a modification of Rives-Stoppa technique. However, two of seventy-four patients had recurrence after six months [47]. Whether these techniques have any functional or cosmetic advantage over open surgery is unclear [3].
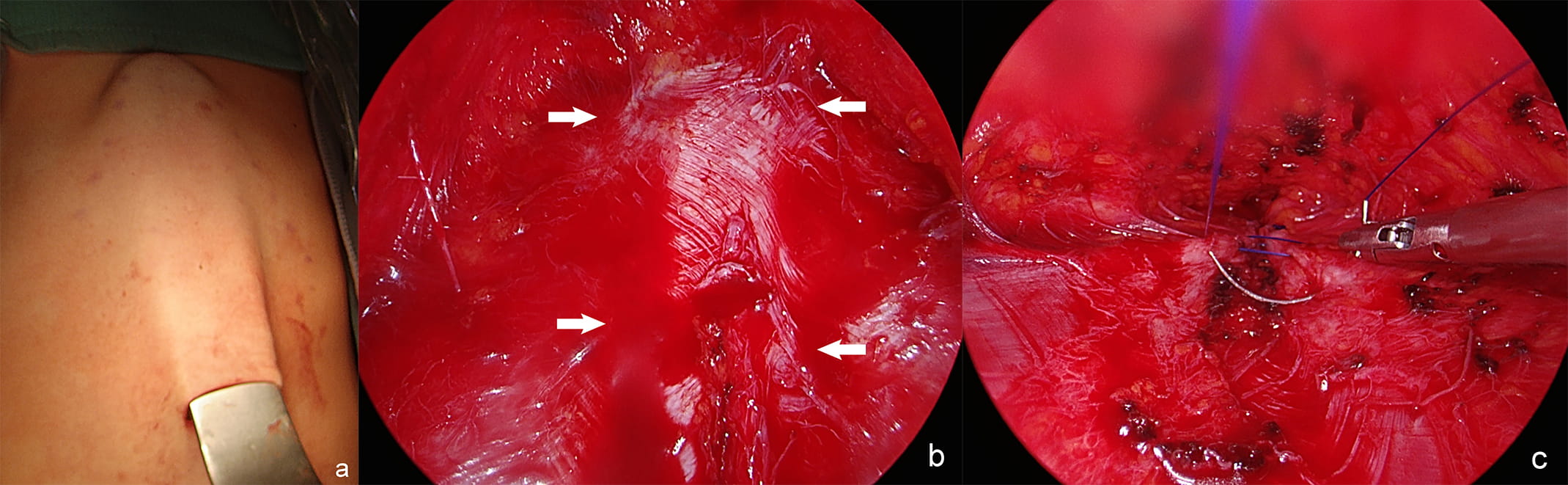 Fig. 5.
Fig. 5.Endoscopic assisted approach for DRA: the retractor lifts the skin above the linea alba. (a) Endoscopic view of the supra-aponeurotic space and exposure of the linea alba. (b) Plication of the anterior rectus sheath with continuous suture. (c) DRA–diastasis recti abdominis, arrows–medial margins of rectus muscles.
The physical deformity of the abdomen wall can result in reduced quality of life [41]. The impact of surgery of quality of life has not yet been established [41]. Surgical reconstruction of DRA is safe, durable and effective, improves function and could possibly provide increased quality of life [30, 31, 41]. Although Kerckhoven et al. [31] showed a high rate of patient satisfaction after surgical correction of DRA, they did not favour any treatment method. They noted, that IRD should not be an indicator for a particular surgical technique. They emphasized that abdominal wall protrusion may determine patient satisfaction and could be an indicator for treatment [31].
The prevalence of DRA is unknown as the prevalence rate varies according to
measurement method, measurement site and cut-off point for DRA diagnose. However,
DRA is an exceptionally frequent condition. IRD measurement 3 centimeters above
the navel and 22 millimeters as a cut-off point for DRA diagnose are recommended
by most authors. The above-navel DRA is the most common one. Most studies are
focused on women with mild and moderate DRA and there is little knowledge on
women with severe DRA
There is lack of consensus on the preferred treatment of DRA. Physiotherapy is unlikely to prevent or completely treat DRA. Surgical repair is challenging since guidelines almost do not exist. Plication is recommended by most authors, however whether it should be open or laparoscopic remains debatable. There are only limited national recommendations.
There is a great need for further large sample studies including nulliparous, primiparous and pluriparous women, and men. Prevalence, effects of abdominal training in prevention and treatment of DRA need to be evaluated along with what is important for the patients: cosmetic or functional outcome.
LS designed and performed the study. LS, AM, CO and MM analyzed the data. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript.
Not applicable.
We would like to thank Zofia Sułkowska for preparing Fig. 2 and editing the remaining figures.
This research received no external funding.
The authors declare no conflict of interest.