


1 Department of Gynecology and Obstetrics, First Affiliated Hospital of Xiamen University, 361004 Xiamen, Fujian, China
2 Department of Gynecology and Obstetrics, Zhongshan Hospital Affiliated to Xiamen University, 361004 Xiamen, Fujian, China
Academic Editors: Elena Bernad and Marius Craina
Abstract
Background: To evaluate the safety and feasibility of single-handed
trans-umbilical single-site laparo-endoscopic surgery using the suspension-line
method for salpingectomy in ectopic pregnancy. Methods: This study
reviewed 54 patients with ectopic pregnancy who underwent salpingectomy in the
First Affiliated Hospital of Xiamen University from June 2018 to June 2019. The
control group (n = 29) was treated with routine two-handed trans-umbilical
laparoendoscopic single-site surgery (TU-LESS), while the study group (n = 25)
was treated with single-handed TU-LESS using the suspension line method.
Results: There were no significant differences in clinical indicators
such as operation time, postoperative recovery ventilation time, recovery time of
Keywords
- body image scale
- cosmetic scale
- ectopic pregnancy
- laparoendoscopic single-site surgery
- salpingectomy
Ectopic pregnancy refers to the failure of fertilized eggs to implant into the uterine cavity, of which tubal pregnancy accounts for ~95% of cases [1]. The typical clinical manifestations of ectopic pregnancy include abdominal pain and vaginal bleeding after menopause. Surgery is the most commonly used treatment method, while traditional laparotomy surgery is rarely applied due to larger trauma. With the arise and development of trans-umbilical laparoendoscopic single-site surgery (TU-LESS), it is widely used in ectopic pregnancy, but an obvious “chopstick effect” occurs during two-handed operations, that is difficult for inexperienced operators [2]. Our department improved TU-LESS for salpingectomy, and using a suspension line from the abdominal wall to exposed the oviduct, aiming to realize single-handed TU-LESS for salpingectomy. In this study, the feasibility and outcomes of this operation are evaluated.
60 cases of tubal ectopic pregnancy were diagnosed in our department from June
2018 to June 2019 and treated by the same doctor with salpingectomy. Patients
were randomly divided into study and control groups. The control group was
treated with routine two-handed TU-LESS, while the study group was treated with
single-handed TU-LESS using the suspension line method. After surgical
exploration, 6 patients had been diagnosed with severe pelvic adhesion and been
therefore changed to conventional porous laparo-endoscopic surgery, of which 1 in
control group, 5 in study group. The clinical indexes of these cases were not
included in the statistics, so the number of cases in the study group was 25, and
the number of cases in the control group was 29. Inclusion criteria: According to
the medical history, clinical examination, blood β-human chorionic gonadotropin (
| Group | Age (yr) | BMI (kg/m |
Lesion diameter (cm) | Pelvic surgery history (cases) |
|---|---|---|---|---|
| Study group (n = 25) | 27.80 |
22.85 |
4.52 |
9 (36%) |
| Control group (n = 29) | 27.10 |
22.32 |
4.12 |
13 (44.82%) |
| Statistical value | 0.502 |
0.707 |
0.983 |
0.433 |
| p value | 0.618 | 0.483 | 0.330 | 0.585 |
This study was discussed and agreed by the Hospital Ethics Committee, and then filed with the Medical Department.
Both groups were examined prior to surgery, including routine blood analysis,
coagulation tests, complete biochemical tests, preoperative immunity,
Both groups of patients were treated with incision protector made by KANG JI™ (Batch number 20140056, Medical Holdings Limited, Hangzhou, Zhejiang, China). The patients were intubated after general anesthesia. The bladder lithotomy position was adopted and the catheter was retained, the towel was laid after disinfection. In the control group, a 2 cm longitudinal incision was made into the abdomen through the umbilical hole and the incision protector was positioned. Laparoscopic lens, separation forceps and bipolar were positioned to investigate the pelvic and abdominal cavity. According to the adhesions observed during operation, a simple uterine manipulator was selectively placed for assistance and the affected fallopian tube was clamped, and removed with scissors after bipolar electrocoagulation of the tubal mesosalpinx and isthmus. The study group routinely received simple uterine lifting devices, after disinfecting and spreading towel, 1 cm longitudinal incision was made through the upper edge of the umbilical hole. A 10 mm Trocar was routinely inserted to examine the abdominal cavity which was then removed. The fascia was then lifted and clamped, and the inner ring of the incision protector was inserted. We explored the pelvic and abdominal cavity and exposed the affected fallopian tube assisted by the uterine manipulator. A 1/0 VICRYL suture was inserted 2 cm medial of the anterior superior iliac spine from the abdominal wall of affected side to form the suspension line A. The ampulla of affected tube was sutured by one hand and tied with a knot. The 1/0 VICRYL was then stabbed out of the abdominal wall from the midpoint of the line between the umbilicus and the pubis to form suspension line B. The oviduct mesangial proximal to fimbrial portion was well exposed by pulling suspension line B, which was detached after bipolar electrocoagulation. Suspension line B was then relaxed and the isthmus of the fallopian tube was well exposed through the pulling of suspension line A, which was detached after bipolar electrocoagulation. The pelvic and abdominal cavity was washed with saline, and the specimens were placed in a specimen bag before removal through the umbilical hole (Fig. 1).
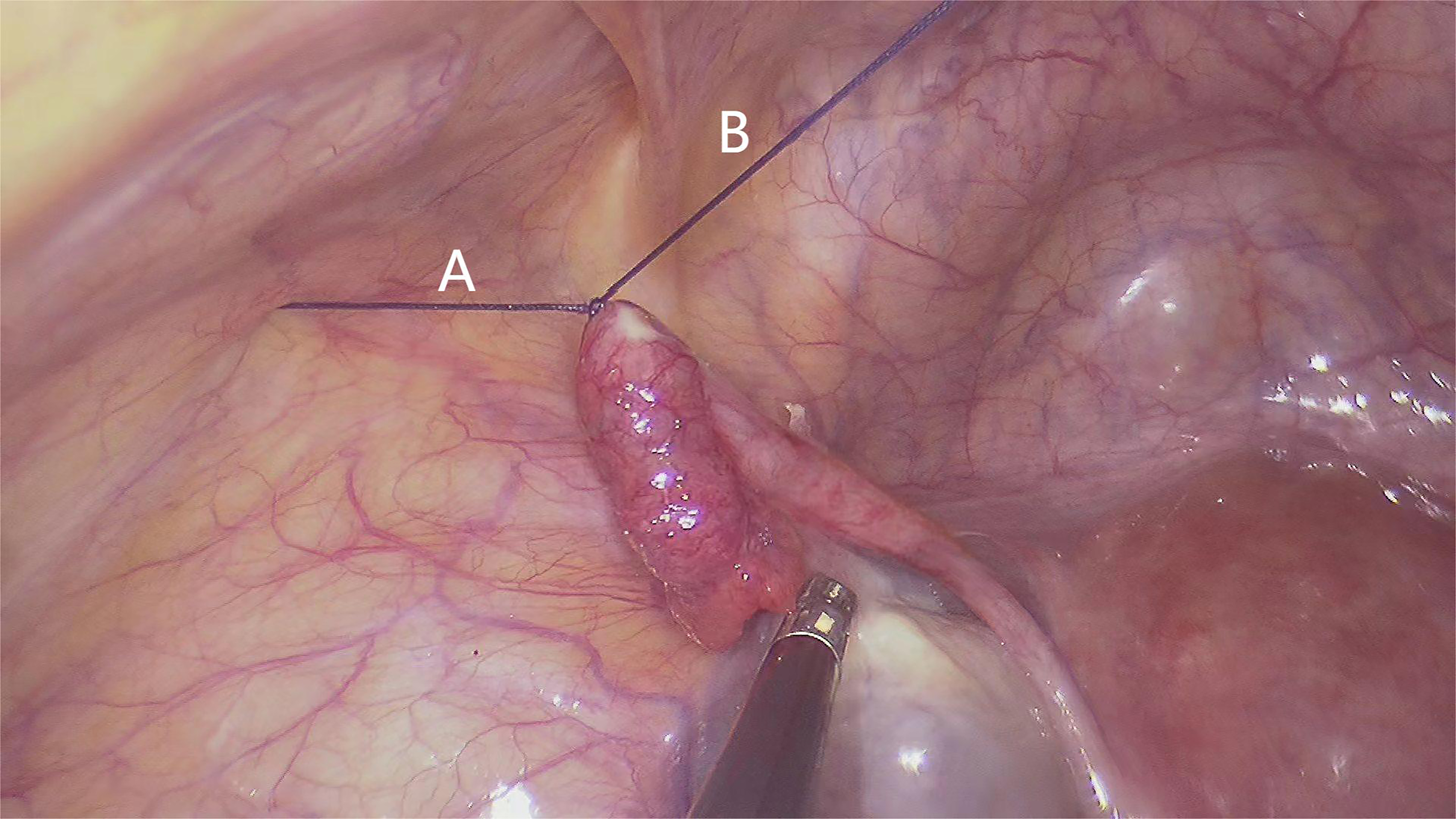 Fig. 1.
Fig. 1.Sample picture of suspension line A and line B.
Perioperative and postoperative related indexes were compared between the
groups. (1) These included operation time, surgical complications, postoperative
exhaust time, postoperative recovery time of
| Not at all (1) | A little bit (2) | Quite a bit (3) | Extremely (4) | |
|---|---|---|---|---|
| Are you less satisfied with your body since the operation? | ||||
| Do you think the operation has damaged your body? | ||||
| Do you feel less attractive as a result of your disease or treatment? | ||||
| Do you feel less feminine/masculine as a result of your disease or treatment? | ||||
| Is it difficult to look at yourself naked? |
| 1. Could you give a score for the appearance of your scar on a scale from 1 (lowest score) to 10 (highest score)? Score = | ||||||
|---|---|---|---|---|---|---|
| 2. On a scale from 1 to 7, how satisfied are you with your (incisional) scar? | ||||||
| 1 = very unsatisfied | 2 | 3 | 4 = not unsatisfied/not satisfied | 5 | 6 | 7 = very satisfied |
| 3. On a scale from 1 to 7, how would you describe your (incisional) scar? | ||||||
| 1 = revolting | 2 | 3 | 4 = not revolting/not beautiful | 5 | 6 | 7 = beautiful |
SPSS 21.0 statistical software (IBM Corp., Armonk, NY, USA) was used for data
analysis. Measurement datas were represented by (
Surgery was successfully completed in the two groups. There were no significant
differences in clinical indicators such as operation time, postoperative recovery
ventilation time, and recovery time of
| Group | Operation time | Postoperative ventilation time | Recovery time of HCG to normal | Use of the uterine manipulator |
|---|---|---|---|---|
| Study Group (n = 25) | 42.92 |
15.44 |
14.68 |
25 (100%) |
| Control group (n = 29) | 39.45 |
17.41 |
13.90 |
6 (20.69%) |
| Statistical value | 0.993 |
–1.150 |
0.673 |
34.54 |
| p value | 0.325 | 0.255 | 0.504 | 0.00 |
There were no complications such as bleeding, acute pelvic inflammatory disease, incision infection, or incisional hernia after operation in the study group or the control group.
As shown in Table 5, the VAS score after 24 h of operation were lower in the
study group compared to the control group, with the differences showing
statistical significance (p
| Group | VAS score after 24 hours of operation | Postoperative BIS score | Postoperative CS score |
|---|---|---|---|
| Study Group (n = 25) | 1.80 |
6.08 |
21.60 |
| Control group (n = 29) | 2.52 |
7.00 |
20.00 |
| t value | –2.505 | –2.483 | 2.877 |
| p value | 0.015 | 0.016 | 0.006 |
Laparoscopic resection of the affected fallopian tube is the most commonly used treatment for ectopic pregnancy. With the continuous development of minimally invasive surgical techniques, current interventions are focused on rapid postoperative recovery whilst achieving the same therapeutic effects and ensuring patients safety [4, 5, 6]. Surgeons are continually adapting their procedures to minimize trauma and ensure incision beauty. TU-LESS uses the natural sunken of the umbilicus to mask the surgical incision, combining minimally invasive and aesthetics. Related studies have shown that TU-LESS is both safe and feasible for fallopian tube resection [7].
To-date, fallopian tube resection by TU-LESS is performed using both hands. Compared to conventional porous laparoscopic surgery, the problems associated with TU-LESS include mutual interference and collision among the laparoscopic lens, two-handed operation instruments, trocar, exposure of the operative field, and cooperation with the surgical assistant. These procedures require extensive training and adaptation. The auxiliary hand is used for the exposure, lift, and clamping of the fallopian tube during the procedure of salpingectomy using two-handed TU-LESS. If the affected fallopian tube is suspended using a suture and the mesosalpinx is exposed, then the single-handed removal of the fallopian tube can be achieved. Based on the above studies, there are no differences in the clinical efficacy indicators of the two surgical methods in terms of surgical time, complications, and postoperative recovery, while the single-handed LESS using the suspension line method shows advantages as following: (1) Smaller incision (1 cm rather than 2–3 cm) and maintains aesthetics. When the incision protector is placed and tightened, the incision was expanded modestly. The single surgical instrument can then be squeezed through the gap between the laparoscopic lens and the incision protector. (2) Single-handed TU-LESS using the suspension line method reduces instrument interference and improves the comfort of the operation. Two-handed TU-LESS requires the placement of two instruments in addition to the laparoscopy lens which may lead to hand-to-hand operations. This means that the size of the incision and “external field” instruments such as cameras and optical fibers may interfere with each other, increasing the difficulty of surgery. During one-handed operations when the fallopian tube is overhung and exposed, the removal of the fallopian tube required longitudinal “stretching” action of the single instrument, so as to avoid mutual interference between the instruments and lens. Even when the incision is small, the laparoscopic lens fits closely with the instrument, and the operating experience is very comfortable, making it easier to complete the operation. (3) Reduction of incision complications. The umbilicus is the weakest area of the abdominal wall, and the contents of the abdominal cavity can easily protrude from its site to form the umbilical hernia. Studies have shown that the probability of an incisional hernia increases when the abdominal wall incision is greater than 1 cm [8]. To accommodate the instruments, a two-handed TU-LESS often requires a longitudinal 2–3 cm incision, which destroys the integrity of the umbilical ring. The single-handed TU-LESS using the suspension line method is located 1 cm above the umbilical ring so to avoid umbilical damage. Although no complications such as incisional bleeding, infection, and incisional hernia were observed in any cases in this study, longer term observations are required as the number of cases increases. (4) The instrument and the laparoscopic lens typically interfere during the two-handed operation, so it is necessary for the assistant to adjust the lens and fibers skillfully, while the TU-LESS using the suspension line method can be operated by a single person, holding the lens in one hand, and the surgical instruments in the other, and the cooperation is more tacit.
It should be noted that single-handed TU-LESS using the suspension line method has some limitations. When serious pelvic and abdominal cavity adhesion are encountered, the suspension line is difficult to replace the auxiliary equipment for exposure. In 5 cases, the pelvic and abdominal cavity adhesion were serious after laparoscopic exploration using the single-handed LESS with suspension line method. In these patients, a 5 mm incision was added to the lateral abdomen for auxiliary operation. In addition, when removing the pelvic hemorrhage, the single-handed operation in the study group struggled to expose the posterior region of the uterus. Therefore, the study group must place a simple uterine manipulator in position to assist the exposure, while the exposure of the control group is completed by the auxiliary instruments, and a uterine manipulator is only active when the pelvic adhesion is serious. Laparoscopic salpingectomy is an aseptic operation. Although no infections occurred after surgery in either groups, the placement of a simple uterine manipulator can increase the chance of postoperative infections, which requires further studies.
In summary, after mastering basic skills such as single-handed knotting with the needle, single-handed TU-LESS using the suspension line method can be safely and effectively applied to salpingectomy, with less trauma, more beautiful incision, and more comfortable operation, which is worthy of clinical popularization and widespread application.
Study conception and design—ML, DW; Acquisition of data—ML, ZC; Analysis and interpretation of data—ML; Critical revision—ML, ZC, DW. All authors read and approved the final manuscript.
All subjects gave their informed consent for inclusion before they participated in the study. The study and the protocol were approved by the Ethics Committee of the First Affiliated Hospital of Xiamen University (Approval number: XMYY-2019-XJS1130).
Special thanks to Jianing Li for his help of the video editing.
This study was funded by “Medical Treatment and Public Health major project of Xiamen (2019S2766)”.
The authors declare no conflict of interest.