


1 Obstetrics Department, International Peace Maternity & Child Health Hospital, Shanghai Jiaotong University, 200025 Shanghai, China
2 Obstetrics Department, Shanghai First Maternity and Infant Hospital, Tongji University School of Medicine, 200126 Shanghai, China
†These authors contributed equally.
Academic Editor: Shigeki Matsubara
Abstract
Background: The aim of this study was to identify risk factors of Bakri balloon tamponade (BBT) failure for postpartum hemorrhage (PPH) and to evaluate the efficacy of BBT for PPH caused by different etiologies. Methods: All women who underwent BBT for PPH at International Peace Maternity & Child Healthcare Hospital, Shanghai, China were included. Univariate analysis and logistic multivariate models were used to identify prognostic factors for BBT failure. Results: Of 48,511 deliveries during the study period, 487 (1.0%) women underwent BBT for persistent PPH. The overall success rate was 91.8% (447/487). The individual success rates of BBT for PPH caused by uterine atony, placenta previa, placenta accreta spectrum (PAS), and coagulopathy were 95.9%, 90.6%, 50.0%, and 25.0%, respectively. Blood loss before BBT was remarkably higher in the failure group than in the success group. In addition, estimated blood loss (EBL) before BBT insertion, disseminated intravascular coagulation (DIC) development, in vitro fertilization (IVF) pregnancy, and PAS were considered to be independent risk factors of BBT failure. Conclusions: BBT is an effective method in the management of PPH resulting from uterine atony and placenta previa. Risk factors of BBT failure primarily include the EBL before BBT insertion, DIC development, IVF pregnancy and PAS.
Keywords
- Bakri balloon tamponade
- postpartum hemorrhage
- placenta accreta spectrum
- disseminated intravascular coagulation
Postpartum hemorrhage (PPH) is common and a leading cause of pregnancy-related death worldwide [1]. The factors that cause PPH are complex and mainly include uterine atony, abnormal placentation, genital tract lacerations, and retained placental product [2]. Most cases of PPH remain unpredictable; therefore, appropriate and timely management of excessive PPH is essential [3]. In recent years, guidelines for the management of PPH have involved a stepwise escalation of pharmacologic and eventual surgical approaches [4]. Primary management includes the use of uterotonic agents, fundal massage, manual exploration of the uterus, and suturing possible lacerations. If all of these techniques fail and bleeding persists, Bakri balloon tamponade (BBT) is becoming a widely suggested technique and is often regarded as a second-line procedure for the management of PPH [5, 6]. The efficacy of BBT in the management of PPH has been reported. Wang et al. [7] reported a success rate of 91.65% using BBT in a large retrospective study in South China. Suarez et al. [8] reported that the overall pooled uterine balloon tamponade success rate was 85.9% in a systematic review. Kumru et al. [9] reported that BBT was effective in 22 (88%) of 25 patients who had severe PPH with placenta previa. Soyama et al. [10] revealed that in women with placenta previa, routine rapid insertion of BBT significantly reduced intra- and post-operative hemorrhage and shortened the operative time. Therefore, BBT is effective in the treatment of PPH and has the value of clinical promotion. Factors for BBT failure mainly included pre-pregnancy obesity, maternal age, caesarean delivery, estimated blood loss before BBT insertion, long operation duration, and coagulopathy [11, 12]. To reduce massive hemorrhage more effectively, it is necessary to identify the risk factors of BBT failure.
In this study, we conducted a retrospective study and aimed to analyze the efficacy of BBT for the management of persistent PPH caused by different etiologies and to identify the specific risk factors related to an increased likelihood of BBT failure.
This retrospective study was conducted at International Peace Maternity & Child
Health Hospital, Shanghai Jiaotong University, China. Before analysis, the
information of all women were anonymized and de-identified. All women who
underwent BBT for persistent PPH from January 2014 to December 2016 were
reviewed. Our protocol of management of PPH was described in Fig. 1. Providers
could choose B-Lynch or BBT as an initial first step in cesarean deliveries.
However, BBT was the only initial step in the vaginal delivery group. BBT was
used when blood loss was
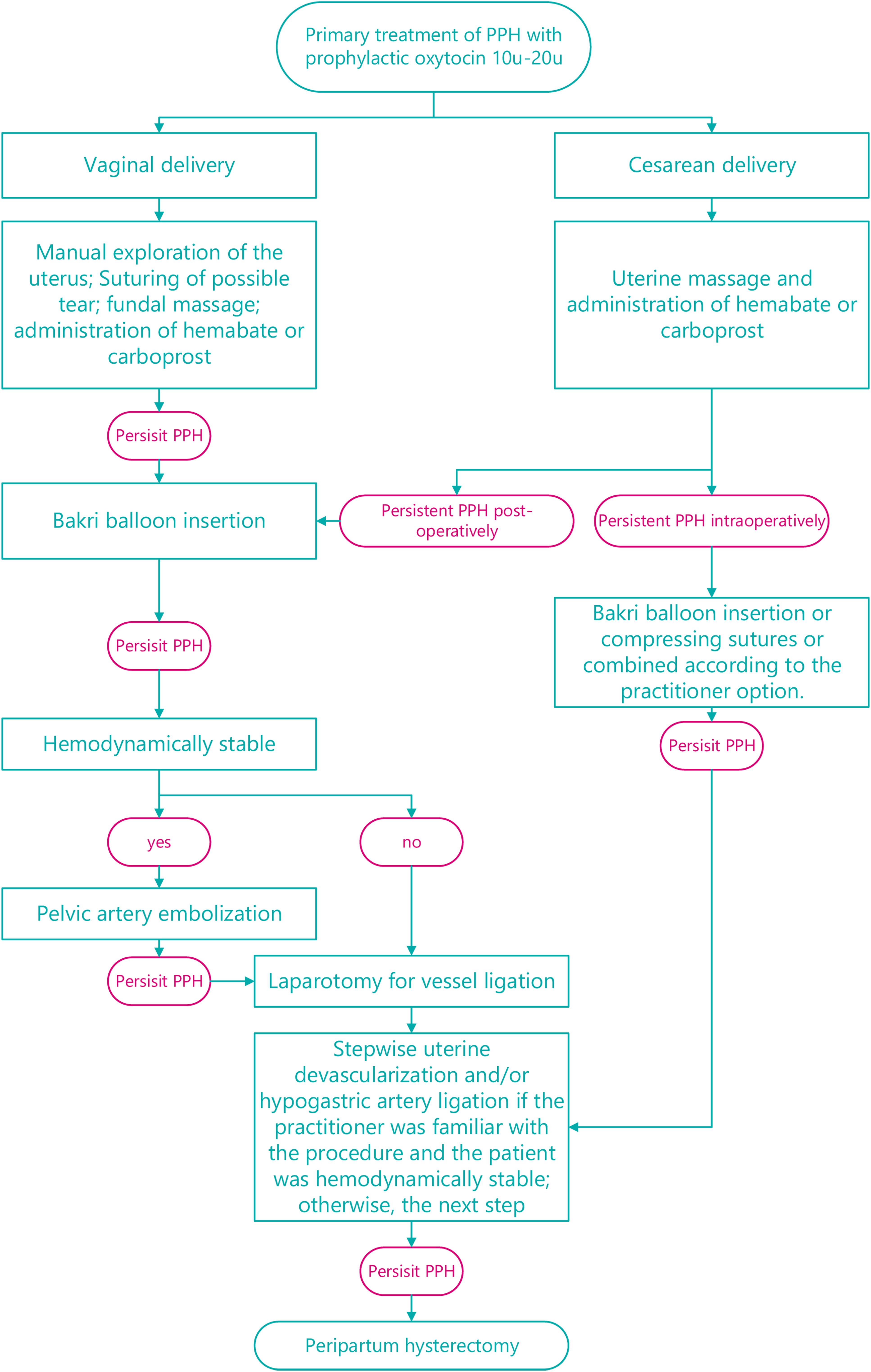 Fig. 1.
Fig. 1.Management for patients with postpartum hemorrhage.
An obstetrical chart review of each woman was done to collect data including
demographic and obstetric characteristics of the study population, causative
factors of PPH, mode of delivery, pretamponade treatment, amount of estimated
blood loss (EBL) before insertion, timing and method of placement, amount of
saline used to inflate the balloon, blood transfusion, and immediate
complications. The diagnostic criteria for disseminated intravascular coagulation
(DIC) were based on the International Society on Thrombosis and Hemostasis (ISTH)
score and patients were diagnosed with DIC according to the diagnostic criteria
of ISTH score
SAS version 9.4 (SAS Institute, Cary, NC, USA) was used for
statistical analyses. The Pearson chi-square or Fisher exact test was used to
analyze the categorical variables between the groups with BBT failure and
success, and the Student’s or Wilcoxon test was used for the analysis of
continuous variables. The mean value was used for missing data when applicable.
Factors related to BBT failure with p
Among the 48,511 women who delivered during the study period, 498 with persistent
PPH underwent BBT. The records of 487 patients were studied and analyzed. Table 1
presents the demographic and pregnancy factors of the 487 women with BBT success
and BBT failure. There was no significant difference in maternal age, body mass
index, percentage of nulliparity, previous cesarean delivery, prior curettage,
and birth weight between the success and failure groups. In addition, there was
no remarkable difference between the two groups with regard to preeclampsia,
complicated with myoma or mode of delivery. Interestingly, the percentage of
pregnancies via in vitro fertilization (IVF) in the failure group was
significantly higher than that in the success group (35.0% versus 21.0%,
p
| Characteristics | Success (N = 447) | Failure (N = 40) | p | |
| Maternal characteristics | ||||
| Age, years, median | 32 (29.0–35.0) | 33 (31.5–36.0) | 0.07 | |
| Previous uterine surgery, n (%) | 0.67 | |||
| Previous cesarean section | 101 (22.6) | 9 (22.5) | ||
| Previous myomectomy | 13 (2.9) | 2 (5.0) | ||
| Others | 16 (3.6) | 2 (5.0) | ||
| Body mass index at first prenatal visit, kg/m |
22.4 (20.6–24.7) | 22.45 (20.6–24.4) | 0.75 | |
| Complicated with myoma, n (%) | 42 (9.4) | 5 (12.5) | 0.57 | |
| Pre-labour HB (g/L), median | 115.0 (108.0–123.0) | 110.5 (106.0–115.0) | 0.02 | |
| Peripartum HB (g/L), mean |
101.3 |
79.8 |
0.00 | |
| Nulliparity, n (%) | 304 (68.0) | 26 (65.0) | 0.70 | |
| History of prior curettage, n (%) | 0.70 | |||
| 0 | 257 (57.5) | 22 (55.0) | ||
| 1 | 123 (27.5) | 10 (25.0) | ||
| 67 (15.0) | 8 (20.0) | |||
| Obstetric characteristics | ||||
| Twin pregnancy, n (%) | 74 (16.6) | 12 (30.0) | 0.03 | |
| Pre-eclampsia, n (%) | 37 (8.3) | 7 (17.5) | 0.08 | |
| IVF pregnancy, n (%) | 94 (21.0) | 14 (35.0) | 0.04 | |
| Gestational age (wks), median | 37.6 (37.0–39.0) | 36.6 (35.3–38.0) | 0.00 | |
| Birth weight (g), median | 3445.0 (3080.0–3900.0) | 3485.0 (3022.5–4075.0) | 0.94 | |
| Mode of delivery, n (%) | 0.78 | |||
| Cesarean | 405 (90.6) | 36 (90.0) | ||
| Vaginal delivery | 42 (9.4) | 4 (10.0) | ||
| DIC development, n (%) | 6 (1.3) | 23 (57.5) | 0.00 | |
| ICU admission, n (%) | 188 (42.1) | 37 (92.5) | 0.00 | |
| PPH characteristics | ||||
| Causes of PPH, n (%) | 0.00 | |||
| Uterine atony | 282 (63.1) | 12 (30.0) | ||
| Placenta previa | 155 (34.7) | 16 (40.0) | ||
| PAS | 9 (2.0) | 9 (22.5) | ||
| Coagulopathy | 1 (0.2) | 3 (7.5) | ||
| Blood loss before insertion of Bakri balloon (mL), median | 500 (200.0–2000.0) | 1612.5 (600.0–5500.0) | 0.00 | |
| EBL |
390 (87.2) | 5 (12.5) | ||
| EBL 1000 mL–2000 mL, n (%) | 57 (12.8) | 20 (50.0) | ||
| EBL |
0 (0) | 15 (37.5) | ||
| Red blood cell units transfused (units), median | 0 (0.0–0.0) | 6 (4.0–9.5) | 0.00 | |
| Data are presented as n (%), mean | ||||
The overall success rate of BBT was 91.8% (447/487), with a success rate of 91.3% and 91.8% among vaginal and cesarean deliveries, respectively. Uterine atony was the most common reason for PPH (294/487 cases, 60.4%), followed by placenta previa (171/487 cases, 35.1%). The success rate of BBT was 95.9% (282/294) for women with uterine atony and 90.6% (155/171) for women with placenta previa. In contrast, the success rate of BBT was only 50.0% (9/18) for women with PAS and 25.0% (1/4) for women with coagulopathy (Table 1).
The pre-labour hemoglobin level of the
success group was higher than that of the failure group (median, 115.0 g/L versus
110.5 g/L, p
No patients died during the study. Among all patients, 18 women in the success group developed puerperal fever with no specific infection detected. All patients experienced resolution and recovered well after antibiotic treatment. Five patients developed endometritis in the success group and were treated with antibiotics. They all recovered favorably as well. Three patients in the success group suffered from incision infection or dehiscence, which required re-suturing. In addition, BBT failed to control bleeding in 40 women. Among them, one woman had central placenta previa with placenta implantation. The woman had a history of cesarean section twice, and the blood loss was 3900 mL. One woman had central placenta previa and was premature with 1450 mL of bleeding. One woman had central placenta previa with 5500 mL of bleeding. These three women ultimately required peripartum hysterectomy after all conservative interventions. A total of 35 pelvic arterial embolizations were attempted and succeeded. Laparotomy was performed in only one woman who had pelvic inflammation. The balloon was then removed, and B-Lynch sutures were applied. One woman was managed by massive blood transfusion plus clotting factors after BBT failure.
Finally, we constructed the multivariate logistic model on those variables with
p
| Variable | S.E | Wald x |
p | OR (95% CI) | ||
| Pre-labor HB | –0.04 | 0.02 | 4.50 | 0.03 | 0.96 (0.93–1.00) | |
| EBL before insertion | ||||||
| 2.58 | 0.63 | 17.05 | 0.00 | 13.25 (3.89–45.18) | ||
| 1 | ||||||
| IVF | 1.33 | 0.64 | 4.30 | 0.04 | 3.77 (1.08–13.19) | |
| DIC | 2.15 | 0.67 | 10.40 | 0.00 | 8.59 (2.33–31.72) | |
| PAS | 2.33 | 0.91 | 6.55 | 0.01 | 10.29 (1.73–61.35) | |
| Placenta previa | 1.40 | 0.61 | 5.21 | 0.02 | 4.04 (1.22–13.40) | |
| BBT, Bakri balloon tamponade; HB, hemoglobin; OR, odds ratio; CI, confidence interval; IVF, in vitro fertilization; DIC, disseminated intravascular coagulation; PAS, placenta accreta spectrum. | ||||||
Our large retrospective study of 487 patients who underwent BBT for persistent PPH at our tertiary center demonstrated two key findings: (1) the risk factors of BBT failure included EBL before insertion, DIC development, IVF pregnancy and PAS. (2) BBT was an effective method in the management of PPH resulting from uterine atony and placenta previa, with success rates of 95.9% and 90.6%, respectively.
BBT was first reported in 2001 for the management of persistent bleeding from the lower uterine placental site [13]. The mechanism of BBT had been possibly attributed to the intrauterine pressure, which is greater than the systemic arterial pressure, created by the balloon. BBT has become a popular management method because it is simple to use and has a success rate of 80%–100%. Alkıs et al. [2] found that BBT was effective in 14 (87.5%) patients with PPH caused by placenta previa. Similarly, the success rate of BBT was 90.6% (155/171) for persistent PPH caused by placenta previa in this study. In addition, uterine atony is also a main cause of PPH. Previous studies have reported that BBT was effective in cases of PPH caused by uterine atony [16, 17]. In the present study, 60.4% (294/487) of patients were complicated with persistent PPH caused by uterine atony, and the success rate of BBT was 95.9%. These results indicate that BBT is effective in the management of PPH caused by placenta previa and uterine atony.
Our findings indicated that the risk factors of BBT failure included EBL before insertion, DIC development, IVF pregnancy and PAS. In agreement with our results, Wang et al. [7] also reported that DIC development is one of the risk factors in the BBT failure. Ruiz Labarta et al. [11] found that EBL before insertion was associated with BBT failure. In addition, PAS is associated with life-threatening maternal PPH. In a systematic review and meta-analysis, Suarez et al. [8] examined the efficacy of uterine balloon tamponade and discovered that the success rate for PAS was 66.7%. Mathur et al. [18] reported that the failure rate of BBT reached 50% in PPH caused by placenta increta. In Grönvall’s cases series of 50 patients, BBT failure was noted in two of five cases of placenta accreta/increta, both of which required hysterectomy [19]. Similarly, in our study, there were 18 cases of PPH caused by PAS, with nine failures (success rate: 50.0%). Interestingly, we found in the study that patients of IVF pregnancy would have higher risk of BBT failure, which was not identified in previous studies. This may be due to the high rate of twin pregnancy with IVF pregnancy. Furthermore, patients of IVF pregnancy may have some potential hormonal disorders, which may lead to unresponsiveness to medication and severe bleeding before further intervention deployed.
Meanwhile, 15 of the 40 failed cases had a blood loss of
This study has several strengths. First, it is one of the largest studies to address the issue of the success and failure rates of BBT. The large number of included patients also makes the results more convincing. Second, participants from our single medical center had the same diagnostic criteria and underwent similar management for PPH, which resulted in the limitation of potential confounders. Third, the overall success rate of BBT was 91.8%, which was consistent with that reported in previous studies [22, 23]. In addition, this study has several limitation. First, the sample size of the outcomes of interest was small (n = 40, with only four PPH cases caused by coagulopathy), this series might not have the ability to detect some other predictive factors. Second, we could choose either B-Lynch or BBT as the initial first step in cesarean deliveries, which was not standardized and might have caused bias. However, BBT was the only initial step in the vaginal delivery group, and the success rate of BBT was similar to that of cesarean deliveries. This suggests that randomness in cesarean deliveries is unlikely to have a significant effect on the main results we were concerned about. Third, our study lacked a control group, which may have resulted in overestimation of the efficacy of BBT. Only a randomized study could assess the true efficacy of BBT.
Our results regarding the risk factors of BBT failure have important clinical significance because they may assist caregivers in optimizing the management of PPH. Notably, although BBT is not effective in some situations with risk factors of failure, it may be used as a temporary tamponade, which permits practitioners to prepare for the next intervention or patient transfer. For example, at our tertiary center, BBT in combination with pelvic artery embolization can enhance the treatment effectiveness of BBT failure and lower the risk of peripartum hysterectomy. In addition, other treatment options instead of Bakri and embolization such as ligation of the ampulla tubae uterinae or the application of a Celox tamponade can be used for PPH.
We demonstrated that BBT is an effective treatment method for PPH caused by uterine atony and placenta previa. The risk factors of BBT failure primarily include EBL before insertion, development of DIC, IVF pregnancy and PAS. In addition, timely intervention of BBT for patients at high risk of PPH may result in a high success rate.
XL designed the study. YC and WC contributed to experiment and methodology. EM collected and analyzed the data. TT wrote the manuscript. All authors read and approved the final manuscript.
This study was approved by the Ethics Committee of International Peace Maternity & Child Health Hospital, Shanghai Jiaotong University. The ethical approval number is GKLW2017-113. Informed consent was obtained from all subjects involved in the study.
We thank Cheng Lei, the information engineer of IPMCHH for his support of the data collection, the midwives in the labor and delivery room for the detailed delivery records.
This work was supported by Shanghai Science and Technology Commission, grant number 17441902900. The sponsor has no role involvement in the study or the submission of the manuscript.
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/j.ceog4911255.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.