


Clinical and Experimental Obstetrics & Gynecology (CEOG) is published by IMR Press from Volume 47 Issue 1 (2020). Previous articles were published by another publisher on a subscription basis, and they are hosted by IMR Press on imrpress.com as a courtesy and upon agreement with S.O.G.
 , M. Yalvaç 2, G. Vural 1
, M. Yalvaç 2, G. Vural 11 Faculty of Nursing, Obstetric-Women's Health and Diseases Nursing, Near East University, Nicosia, Northern Cyprus
2 Faculty of Health Sciences, Cyprus Science University, Kyrenia, Northern Cyprus
3 Faculty of Nursing, Obstetric-Women's Health and Diseases Nursing, Near East University, Nicosia, Northern Cyprus
Abstract
Purpose: The aim of this study is to analyze the effect of childbirth preparation training (education, Pilates, and breathing exercises) on the birth plans of primiparous women, as well as the effect of birth plans on the childbirth process. Materials and Methods: This is a quasi-experimental/non-randomized trials and prospective study. The population of the study included the primiparous women that came to two hospitals. Among these women, the sample of the study included 70 women (experimental group=35, control group=35). Results: The most common requests granted to the experimental group were having the support of the person they wanted during the birth process (80.6%) and being able to walk and change position (90.3%). The experimental group had a lower rate of planned cesarean, were more satisfied with their childbirth experiences, received more support during the birthing process, and used more techniques for coping with pain during labor (p < 0.05). The experimental group was earlier to have contact with their infants, to the first breast feed their infants (p < 0.05). Conclusion: Midwives and nurses play an active role in the realization of the birth plans that are within the framework of prenatal education courses.
Keywords
- Parturition
- Pregnancy
- Prenatal Education
- Midwife
- Nurse
A birth plan is one of the most important parts of prenatal childbirth education programs. It was first used in 1970 by childbirth preparation trainers [1-3].
In the U.S., Sheila Kitzinger was the one to make birth plans a current topic in 1980 [4]. The birth plan was first introduced in the Spanish Health Service in 2008 through the Strategy for the Care in Normal Childbirth by the National Health Service, which promotes woman-centered care, based on the latest scientific evidence. Birth plans were developed against a backdrop of medicalization of the childbearing process which was pushing maternity care provision away from those expectations and needs of the woman [5]. The American College of Obstetricians and Gynecologists (ACOG) and the American Academy of Pediatrics (AAP) endorse a majority of childbirth preparation training programs, and the birth plans created as part of these programs [6]. Prenatal trainers may encourage pregnant women to write a birth plan and share it with their physicians, midwives, and nurses, with the purpose of facilitating communication between parents and health professionals. A birth plan can be described as a written communication tool that is prepared by the pregnant woman in order to state her preferences about childbirth and childbirth management [3, 7].
A birth plan can assist to monitor women during their childbirth process, aid to support them during labor, encourage them to make their own decisions, and help them share their preferences with health professionals [1, 5, 8, 9-14].
A birth plan is supposed to include the management of the delivery, the participation of the partner, the delivery moment, and the practices of bonding with the infant right after the delivery. A birth plan may also include: a) the preferred delivery mode, b) preparations that should be made before coming to the hospital/clinics, c) the arrangements they want in the labor room, d) the movements and positions they prefer during the delivery, e) the methods they plan to use to cope with pain during labor, f) their preferences related to the management of delivery, and g) the persons from whom they want to receive emotional and physical support during labor and delivery. The other points that may be included in the birth plan are the interventions that the pregnant woman wants to avoid (e.g. intravenous feeding, continuous electronic fetal monitoring, routine episiotomy, and routine use of oxytocin). This can help ensure contact between the mother and the infant, and the start of breastfeeding right after the delivery. Avoiding unwanted interventions can also help the woman with providing initial care of the infant and the cord [1, 2, 5, 7, 9, 15]. Afshar et al. [3] suggested the use of the term “childbirth preferences” instead of “birth plan”, since this practice is related to sharing preferences about childbirth rather than planning it. Support can be given to these preferences, while ‘“plan” can be a restricting term. Childbirth preferences should be presented in an evidence-based manner and within the context of childbirth preparation training programs. Then, discussions about the benefits, risks, and options available during childbirth can help women deliver their infants as planned. Previous studies have found that women who have a written birth plan have preferences related to the childbirth process. They may also want to avoid some of the interventions that are routine during childbirth, which most of the time are completed [2, 4, 9].
The use of a birth plan may have positive effects on the pregnant woman’s satisfaction with the delivery, as well as on the delivery process and results [1, 2, 4, 7, 9, 14]. Relevant studies have found that the women who developed birth plans had a lower rate of cesarean section than those who did not [7, 16], used fewer analgesics [16], and experienced fewer incidence of amniotomy, and the use of oxytocin [17]. Afshar et al. [17] found that some women who had developed birth plans were less satisfied with their childbirth experience since the birth did not fulfill their expectations, which results in a negative experience concerning birth plans. The study by Aragon et al. [8] looked at women’s opinions related to birth plans. This study found that these plans were effective at an acceptable level, although the participants stated that they were disappointed if their plans were not implemented. There are a number of studies proving that the use of birth plans have both positive and negative effects on childbirth; however, there are few evidence-based studies among them [1, 5, 10, 18]. Health professionals may ignore and avoid implementing birth plans due to the lack of evidence regarding their effect on childbirth, or because they find them to be unrealistic [1]. On the other hand, childbirth preparation education programs help pregnant women learn about medical practices, and possible outcomes. These programs also help women identify their wishes related to childbirth. Prenatal training classes encourage pregnant women to think about the type of delivery they prefer and help them develop realistic expectations about their birth plans.
The researchers believe that birth plans that are prepared considering these benefits will often lead to more positive childbirth and delivery experiences. According to the latest data from 150 countries, currently 18.6% of all births occur by cesarean section ranging from 6% to 27.2% in the least and most developed regions, respectively [19].
The World Health Organization (WHO) has asserted that the rate of cesarean sections should not exceed 15% [20]. In 2013, the rate of cesarean sections was 53.1% in public hospitals [21]. The researchers estimated that this rate was higher in private hospitals. The rates of planned cesarean sections may be reduced if fewer women list it as a preference in the birth plans that they develop during childbirth preparation training. This study examines the reasons that prenatal training classes are not conducted in a systematic manner in 2015, and the reasons that birth plans are not applied equally in hospitals/clinics as well. Prenatal education is a new term for this country. Another main consideration in the design of this study was that there are few studies focusing on the birth plans of women who receive childbirth preparation education. The researchers also believe that this study is unique since it is the first in 2015 to address this issue. It is expected that the study will play a leading role for the midwives and nurses in hospitals/clinics, as they help women develop birth plans. Based on all of these points, the purpose of this study is to analyze the effect of the childbirth preparation education programs on the birth plans of primiparous women, as well as the effect of birth plans on the childbirth process. The research questions are: “Of the primiparous women that had received childbirth preparation training and made birth plans, how successful were they in implementing their plans related to the childbirth process?”, and “Is there a difference between the women that had received childbirth preparation training and made birth plans, and those that had neither received this training, nor made birth plans regarding the mode of delivery, the interventions during the delivery, the support received during the delivery, use of coping techniques for pain, satisfaction with the delivery, and the time of first breastfeeding and first contact with the infant?”
This is a quasi-experimental/non-randomized trial and a prospective study conducted with irrelevant groups using the pretest-posttest method. The study was conducted in two Hospitals, both of which are located in Nicosia, the capital of Northern Cyprus. These hospitals were selected for the study because they had a high number of deliveries annually, and they were the largest-scale public and private hospitals. A Hospital has a capacity of 500 beds, one gynecology unit, and one labor and delivery unit, in addition to an outpatient clinic that provides antenatal care. The other Hospital has a capacity of 360 beds, one gynecology unit and one labor and delivery unit, and three outpatient clinics for antenatal care.
The population of the study included the pregnant women that came to the antenatal clinics of these two hospitals between January 1 and June 1, 2015. Among these women, the sample of the study included 70 women (35 in the experimental group and 35 in the control group) that fit the sampling criteria, and who participated in the study on a voluntary basis that came to the two hospitals between January 1 and June 1, 2015. The researchers applied a statistical power analysis to determine the sample size. The aimed power in the study was 0.80, the effect size was 0.2, and the significance level was 0.05.
Based on these analysis results, the researchers anticipated including 31 individuals in each group. Considering the effects of possible power-reducing factors that might appear during the study process, the researchers decided to include 35 subjects in each group. The inclusion criteria for the experimental group were: being between 18 and 35 years of age, being in the 28th to the 32nd week of pregnancy, being primiparous, having only one fetus, having no pregnancy complications or systemic diseases, not in the habit of exercising regularly or doing pregnancy Pilates, having completed the educational part of the childbirth preparation program, as well as at least 75% of pregnancy Pilates sessions, and having given birth in term. The inclusion criteria for the control group were being 18 to 35 years of age, being in 28th to the 32nd week of pregnancy and being primiparous, having only one fetus, having no pregnancy complications or systemic diseases, having a close education level to the experimental group, and not having performed any regular exercise or pregnancy Pilates during pregnancy, not having a birth plan, and having given birth in term.
The experimental group included the women that volunteered for the study and fit the inclusion criteria. The study was not able to utilize randomization since the researchers could not access the numbers and lists of all the pregnant women coming to the antenatal clinics of the two hospitals within the scope of the study.vThe experimental group consisted of 24 women in one of the hospitals, and 11 women in the other hospital. Similarly, the control group constituted of 24 women in one of the hospitals and 11 women in the other hospital. Figure 1 presents the steps followed in the implementation stage of the study.
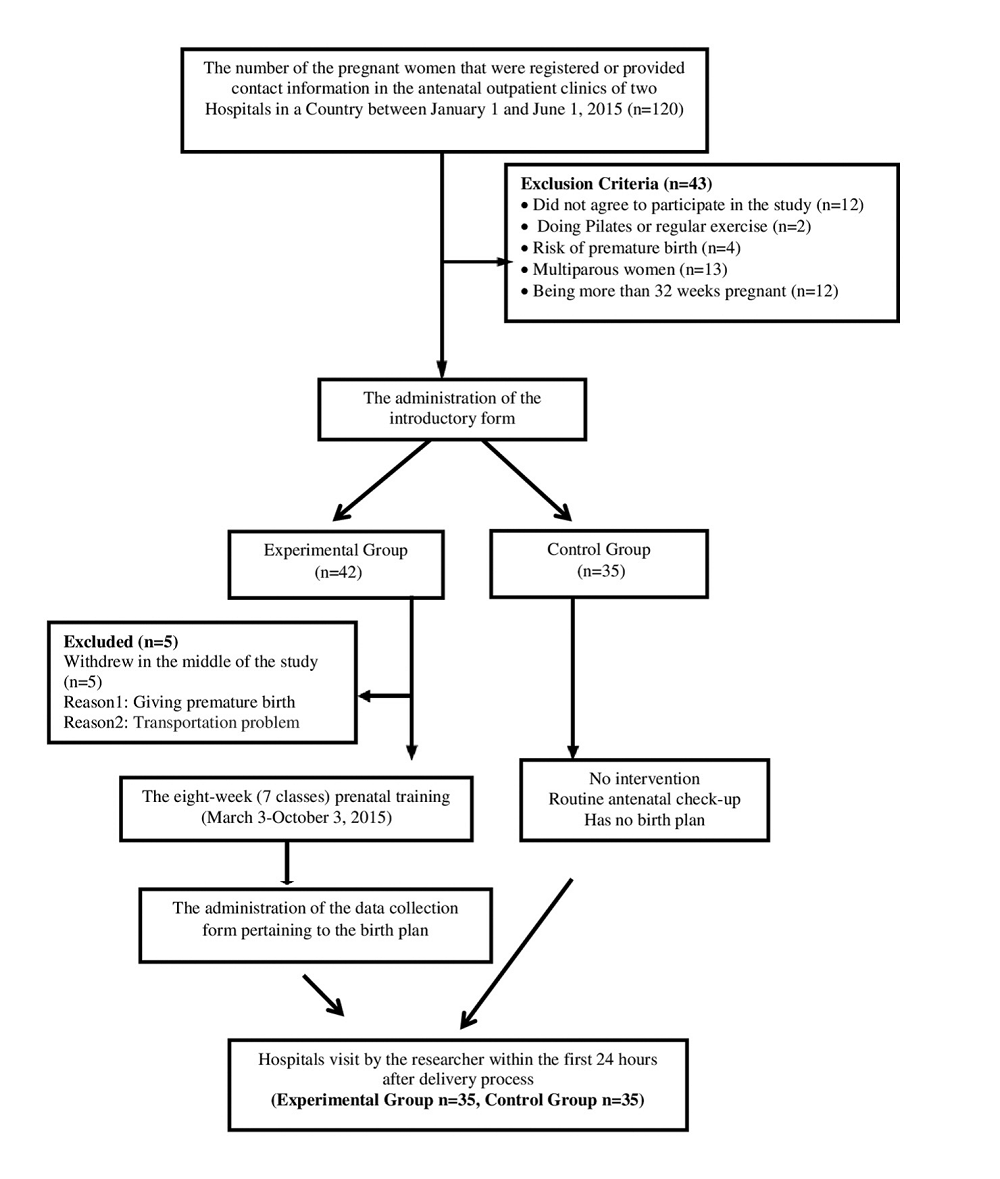 Figure 1.
Figure 1.— Flow chart demonstrating the implementation stage.
The study data were collected by the researcher during personal interviews. The study data were collected using an introductory form, and a data collection form investigating birth plans and process. The introductory form included five questions about the pregnant women’s age, nationality, marital status, education level, and employment status. The data collection form on birth plans was created by the researcher based on a literature review [1, 10-12, 14, 15]. The questions in this form were about the mode of delivery, pregnant women’s plans for the process before coming to the hospital, as well as the arrangement of the delivery room, their wishes about the management of the delivery, the interventions they wanted to avoid during the delivery, and their expectations about the infant in the postpartum period. This form included 12 open- and closed-ended questions. The control group was asked about the existence of birth plans. The control group did not have any birth plans. The data collection form investigating the childbirth process included nine questions.
This form investigated the mode of delivery, the analgesics and/or anesthetics used in the childbirth process, the individuals who served as support partners during birthing, and the techniques used to cope with pain during labor.
It also included questions about the interventions made during the delivery, the time when they first held their infants, and the time they first breast fed their infants. It also questioned whether the women were satisfied with the delivery.
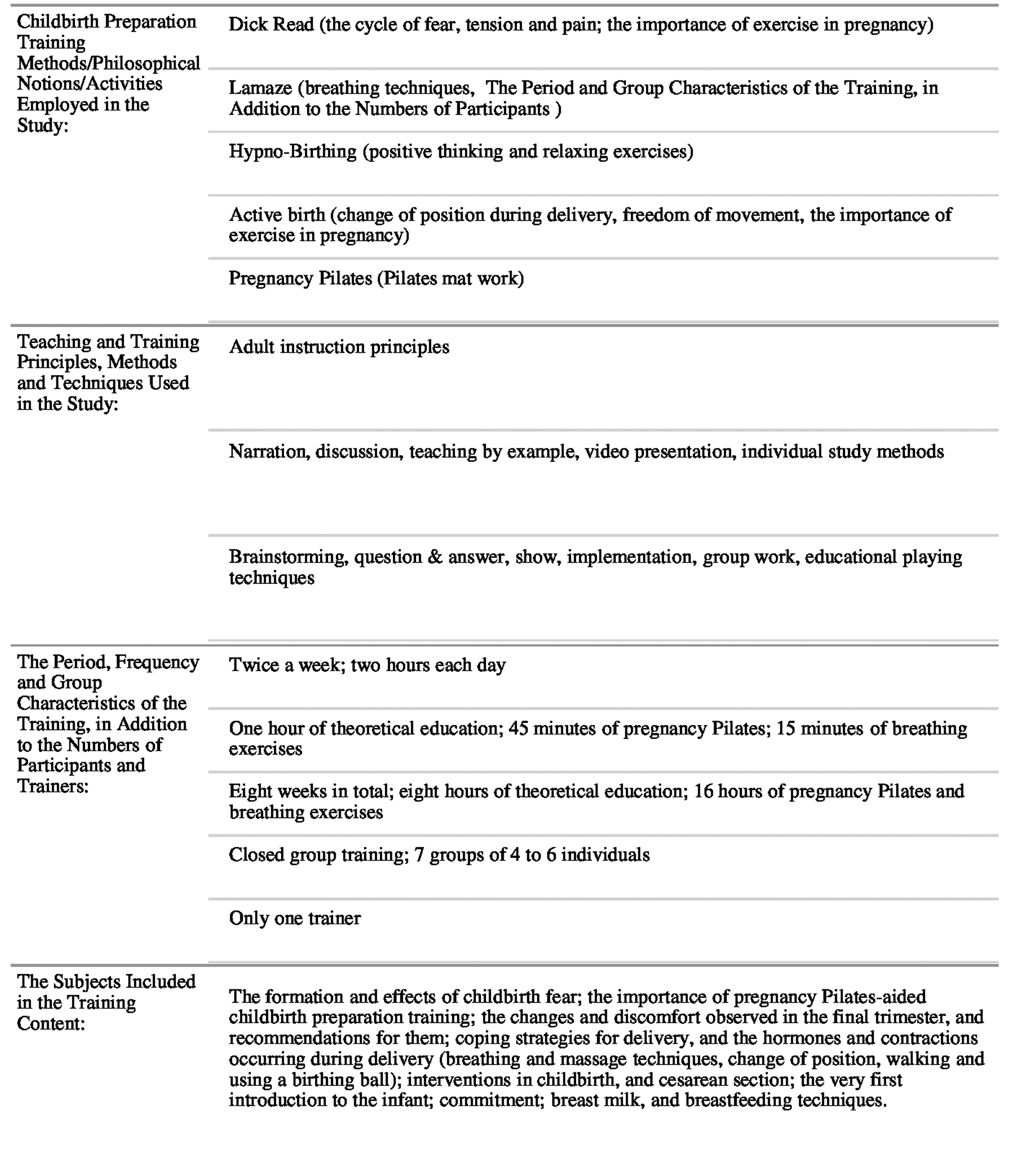
The experimental group was provided with childbirth preparation training, while there was no intervention in the control group. The childbirth preparation training program lasted for eight weeks. During the first phase of the study, this program was executed twice a week for two hours each day comprising one hour of theoretical education, 45 minutes of pregnancy Pilates session, and 15 minutes of breathing exercises in the first four weeks. The final four weeks of this training program consisted of only pregnancy Pilates and breathing exercises. Table 1 summarizes the other information related to the features of the training program. The researcher provided the theoretical instruction for the childbirth preparation program in addition to instruction for pregnancy Pilates.
|
The skills laboratory of a university was prepared for this training education. Before commencing childbirth preparation training, the researchers contacted the experimental group via phone calls to determine the days and hours of training based on women’s opinions. Subsequently, seven courses consisting of four to eight participants were organized and conducted from 16.30 to 20.30 every day. The experimental group completed the training and made their birth plans between March 3 and October 3, 2015. The training program and interviews were conducted out of the hospital to ensure that the control group was not affected. The researchers prepared a birth calendar based on the women’s predicted dates of childbirth. They contacted the groups approximately a week before the childbirth dates and reminded the women to inform the researchers about the commencement of birth. During the second phase of the study, researchers visited groups at Hospital within the first 24 hours after delivery to collect data about childbirth process.
The study data were analyzed using the Statistical Package for Social Sciences (SPSS) version17.0 statistical package. Descriptive qualities and the data related to the birth plans of the experimental group were analyzed using a percentage calculation. The descriptive qualities and childbirth process data of the experimental and control groups were compared using chi-square tests (Fisher’s exact and Pearson’s chi-square). Homogeneity with reference to general characteristics and outcome variables at baseline between the experimental and control groups were examined with chi-square test. All calculations related to the power analysis were made using G*power (version 3.1.7) software.
The researchers obtained written permission before the study from the Ministry of Health Directorates, Gynecology and Childbirth Service Clinical Manager, and the Head Physician Office. The study procedures were approved by the institutional review board (IRB) of the authors’ university (IRB No. 2015-27-171). Informed consent was confirmed by the IRB. Before the study began, the researcher also obtained the written informed consents of the participants.
The general characteristics investigated were homogeneity among the experimental and control groups. Therefore, the experimental and control groups were considered homogeneous at the baseline except employment status (Table 2).
| Characteristics | Experimental |
Control |
Significance test | ||||
|---|---|---|---|---|---|---|---|
| (n=35) | % | (n=35) | % | X2 | p | ||
| Age(years) | |||||||
| Under-24 | 4 | 11.5 | 6 | 17.1 | 4.945 | 0.293* | |
| 25-27 | 14 | 40.0 | 12 | 34.3 | |||
| 28-30 | 11 | 31.4 | 10 | 28.6 | |||
| 31 and over | 6 | 17.1 | 7 | 20.0 | |||
| Nationality | |||||||
| TRNC | 18 | 51.4 | 8 | 22.9 | |||
| TR | 8 | 22.9 | 17 | 48.6 | 8.086 | 0.088* | |
| TRNC-TR | 9 | 25.8 | 10 | 5.8 | |||
| Marital status | |||||||
| Married | 35 | 100.0 | 35 | 100.0 | |||
| Education level | |||||||
| Under-High school | 6 | 17.1 | 11 | 31.4 | 3.052 | 0.549* | |
| Graduate | 21 | 60.0 | 19 | 54.3 | |||
| Postgraduate | 8 | 22.9 | 5 | 14.1 | |||
| Employment status | |||||||
| Employed | 27 | 77.1 | 16 | 45.7 | |||
| Nonemployed | 8 | 22.9 | 19 | 54.3 | 9.559 | 0.008* | |
* Pearson’s chi-square test.
In the study, 88.6% of the experimental group desired to have a vaginal birth, while 62.9% underwent cesarean section (Figure 2). The most common activities in the experimental group were taking a shower (35.4%), leaving for the hospital when they had contractions every five or ten minutes (35.4%), and consuming food or drinks that would energize them (35.4%). In the experimental group that desired to have a vaginal birth, the majority (93.5%) stated that they wanted support \ from their husbands during the birthing process, and 80.6% managed to do this (Table 3). The women mostly made their own plans to cope with the delivery pain using inhaling exercises (87%), a birth ball (77.4%), and walking and/or changing position (67.7%). They planned that was most widely implemented was walking and/or changing position (90.3%) (Table 3). In the experimental group, 60% stated that they shared their birth plans only with their physicians. Of the women that shared their plans, 38.1% received positive reactions from their physicians, and 42.9% were informed that their pregnancy was normal, and they would be able to have a vaginal birth. However, 19.1% of the pregnant women had their plans rejected, and were told that caesarean section was healthier for them, and vaginal birth was at risk. In the experimental group, 37.1% had a vaginal birth, and this rate was 17.1% in the control group (X2 = 3.54, p = 0.06).
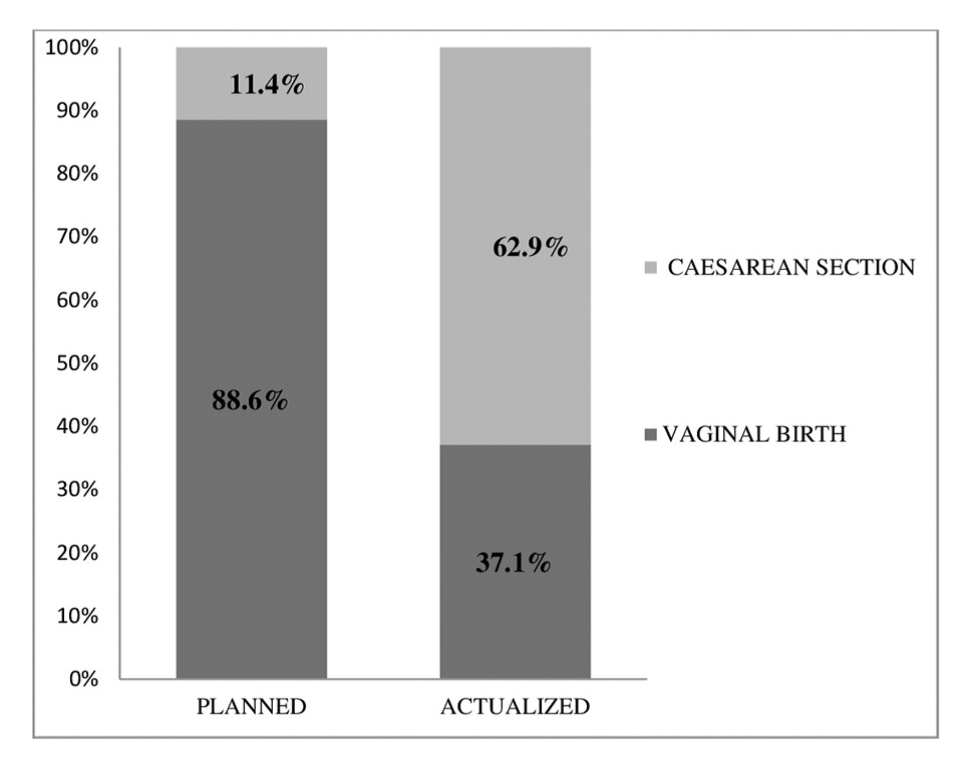 Figure 2.
Figure 2.— Distribution of the delivery modes that were planed by the experimental group and of those that were applied (n=35).
| Plans | Planned | Launched | |||
|---|---|---|---|---|---|
| n=31* | % | n=31* | % | ||
| Persons that gave support during delivery | |||||
| Spouse | 29 | 93.5 | 25 | 80.6 | |
| Mother | 16 | 51.6 | 10 | 32.2 | |
| Sibling | 3 | 9.6 | 3 | 9.6 | |
| Friend | 1 | 3.2 | 2 | 6.4 | |
| Nurse | 0 | 0.0 | 2 | 6.4 | |
| Coping techniques against birthing contractions | |||||
| Inhaling exercises | 27 | 87.0 | 17 | 54.8 | |
| Using birth ball | 24 | 77.4 | 9 | 29.0 | |
| Walking and/or changing position | 21 | 67.7 | 28 | 90.3 | |
| Praying | 0 | 0.0 | 1 | 3.2 | |
| Interventions related to vaginal birth that were not preferred but still applied | |||||
| Vulva shave | 26 | 83.8 | 0 | 0.0 | |
| Episiotomy | 19 | 61.2 | 6 | 19.3 | |
| Cessation of oral food and fluid intake | 16 | 51.6 | 6 | 19.3 | |
| IV induction | 15 | 48.3 | 10 | 32.2 | |
| Continuous electronic fetal monitoring | 13 | 41.9 | 3 | 9.7 | |
| Epidural analgesics for delivery pain | 12 | 38.7 | 1 | 3.2 | |
| Early amniotomy | 9 | 29.0 | 1 | 3.2 | |
| Enema | 5 | 16.1 | 8 | 25.8 | |
* The number of pregnant women that were planning to give vaginal birth. The percentages were calculated considering the n value since there were multiple responses.
In the experimental group, 86.4% had unplanned cesarean sections (both urgent and non-urgent included), and 55.2% of the control group had a planned cesarean section (the operations were preferred by the pregnant women and the physicians) (X² = 12.59, p = 0.002). Of the women that had cesarean sections, 68.1% of those in the experimental group had this operation with spinal analgesics, and this rate was 68.9% among those in the control group (X2 = 3.57, p = 0.303). As seen in Table 4, 91.4% of the experimental group received support during delivery, while this rate was 37.1% in the control group (p < 0.05). In the experimental group, 54.3% of the participants used techniques to cope with the pain during labor, and 14.3% used coping techniques in the control group (p < 0.05) (Table 4).
| Characteristics | Experimental group | Control group | Significance test | |||||
|---|---|---|---|---|---|---|---|---|
| (n=35) | % | (n=35) | % | X² | p | |||
| Receiving support during delivery | ||||||||
| Yes | 32 | 91.4 | 13 | 37.1 | 22.46 | 0.000* | ||
| No | 3 | 8.6 | 22 | 62.9 | ||||
| Using coping techniques | ||||||||
| Yes | 19 | 54.3 | 5 | 14.3 | 12.42 | 0.000* | ||
| No | 16 | 45.7 | 30 | 85.7 | ||||
| Interventions | ||||||||
| Enema | 8 | 22.9 | 8 | 22.9 | 0.00 | 1.000* | ||
| Amniotomy | 2 | 5.7 | 1 | 2.9 | 0.34 | 1.000** | ||
| Episiotomy+ | 9 | 69.2 | 6 | 100.0 | 2.33 | 0.255** | ||
| IV Induction | 12 | 34.3 | 10 | 28.6 | 0.26 | 0.607* | ||
| Cervical Induction | 1 | 2.9 | 2 | 5.7 | 0.34 | 1.000** | ||
| Epidural analgesics | 1 | 2.9 | 0 | 0.0 | 1.01 | 1.000** | ||
| IV analgesics | 3 | 8.6 | 0 | 0.0 | 3.13 | 0.239** | ||
| Vacuuming | 2 | 5.7 | 0 | 0.0 | 2.05 | 0.493** | ||
| Fundal pressure | 1 | 2.9 | 1 | 2.9 | 0.00 | 1.000** | ||
* Pearson’s chi-square test.
** Fisher’s exact test.
+ The frequency of episiotomy was calculated considering the number of women that gave vaginal birth; the women that had caesarean sections were not included in the analysis.
There was no statistically significant differences among the experimental and control groups regarding the interventions that were made (p > 0.05) (Table 4). In the experimental group, 71.4% of the women made physical contact with their infants during the first 30 minutes in the delivery room, and this rate was 22.9% in the control group. In addition, 40% of the experimental group and 8.6% of the control group began to breast feed in the first 60 minutes (X2 = 18.01, X2 = 30.24, p < 0.001). In the study, 80% of the experimental group was satisfied with their birthing experience, while only 28.6% of the control group was satisfied (X2 = 19.23, p < 0.001).
The high rates of cesarean section in the country have been reflected in the study as well. Yam et al. [2] conducted a study with nine women using the interview method and found that all nine women excluded cesarean section from their birth plans, while four of them had this operation. The high cesarean rate implies there is a serious problem that needs to be dealt with.
Prenatal training is an important area in which nurses and midwives can work independently. It provides information to pregnant women about the ways to cope with delivery pain, and the interventions and initiations they may encounter during the birthing process. Among the techniques used to cope with delivery pain, the ones that were most preferred by the experimental group were performing inhaling exercises, using the birthing ball, and walking and/or changing position, respectively. A majority of the women realized their wish to walk and/or change position during labor. The study by Suárez-Cortés et al. [4] found that 62.5% of the women that had made birth plans desired their preferred position during the delivery, and 48.1% of them realized this plan. The first step of the Mother-friendly Care Guide in Ten Steps, which was created based on evidencebased medical information, included the instruction ‘The pregnant woman should be free to move about during the delivery’ and ‘The pregnant women should be supported in having different positions rather than only lying on her back’ [15]. In this study, the preference with the highest rate of realization among all birth plans was walking and/or changing position. Also, slightly more than half of those who wished to use a birthing ball managed to do this.
The researchers believe that the pregnant women in the study received positive support from their partners, or from the healthcare professionals, in walking and/or changingpositions. The Guide includes a number of statements such as ‘Avoiding all types of unnecessary interventions’ and ‘Making no use of the practices and procedures that are not supported by scientific evidence’ [15].
The interventions that should never be made during the delivery process include vulva shave, enema, feeding by IV, and/or establishing vascular access, cessation of oral food intake, rupturing the membrane at an early stage, and continuous electronic fetal monitoring [15].
Nurses and midwives have an important responsibility concerning the interventions that should never be made. This study determined that the most undesired interventions in the experimental group were vulva shave (83.8%), cessation of the oral intake of fluid and food (51.6%), and continuous fetal monitoring (41.9%). The most common interventions made during the birthing process were (25.8%) and cessation of the oral intake of fluid and food (19.3%). In contrast with the present study, 16.6% of the women in the study by Suárez-Cortés et al. [4] who had made birth plans said that they wished to have a vulva shave, and 12% of these women were given a vulva shave during the childbirth process. All of the nine women that made birth plans said that a vulva shave was not a problem for them, and six of these women were given a vulva shave [2]. The researchers believe that this difference in the study resulted from cultural factors. The thought of having their genital area shaved by another person probably made them embarrassed, as they desired their privacy; that is why they did not prefer this procedure.
Of the women participating in this study, 41.9% said that they did not want to use continuous fetal monitoring. In the study by Yam et al. [4]. all of the participants desired to have a continuous Non-stress Test (NST), and they all went through this process. This led to a different result from the present study. This difference might have been caused by the fact that the experimental group of the present study were aware of the benefits of having freedom of movement, thanks to the childbirth preparation training they had received, as well as being aware of the negatives of being connected to NST continually. The study by Suárez-Cortés et al. [4]. found that 42% of the women that had made birth plans wished to take fluids and food orally during the delivery, and 33% of them realized this plan.
A number of evidence-based studies have proved that physical contact has a positive effect on breastfeeding [22] Suárez-Cortés et al. [4]. found that 60.4% of the participants desired to make physical contact right after giving birth, and 27.4% realized this preference. In the present study, four participants planned to make early physical contact, while only two participants managed to do this (Table 5). The researchers estimate that the small number of participants wishing to make physical contact right after delivery was due to the lack of this practice in these Hospitals. Thus, the women might not have listed these preferences on their birth plans.
| Plans | Planned | Launched | ||
|---|---|---|---|---|
| n | % | n | % | |
| The Time of first physical contact with the infant | ||||
| In the first 30 minutes after delivery | 35 | 100.0 | 25 | 71.4 |
| In the first 30 to 60 minutes after delivery | 0 | 0.0 | 3 | 8.6 |
| In the first 1 to 2 hours after delivery | 0 | 0.0 | 4 | 11.4 |
| In the first 3 hours or later | 0 | 0.0 | 3 | 8.6 |
| The Time of first breastfeeding | ||||
| In the first 30 minutes after delivery | 34 | 97.1 | 7 | 20.0 |
| In the first 30 to 60 minutes after delivery | 1 | 2.9 | 7 | 20.0 |
| In the first 1 to 2 hours after delivery | 0 | 0.0 | 15 | 42.9 |
| In the first 3 hours or later | 0 | 0.0 | 6 | 17.1 |
| Other plans (n:8)+ | ||||
| Early physical contact | 4 | 50.0 | 2 | 25.0 |
| Early physical contact with the father | 2 | 25.0 | 2 | 25.0 |
| Keeping the cord and cord blood of the infant | 2 | 12.5 | 1 | 12.5 |
*This is the number of responses to this question. The percentages were calculated considering the n value.
The midwives and nurses working in childbirth services have an important responsibility in supporting women regarding breastfeeding and physical contact. The experimental group of this study had a lower rate of planned cesarean section than the control group, they received more support during the delivery, used more techniques to cope with pain during labor, and breast fed and made their first contact earlier (p < 0.05). In consistency with the present study, the relevant studies found that there was no significant difference between the women who did and did not have birth plans regarding cesarean section and episiotomy applications, spontaneous or intervened initiation of the delivery, and oxytocin use [16, 17]. The study by Burke et al. [18] found that birth plans are associated with a significant prolongation of labor and possibly an increase in cesarean delivery rate. In contrast with this study, the previous studies found that the women with birth plans had lower rates of cesarean section, as well as lower rates of the use of IV analgesics [16] and epidural analgesics, amniotomy, and oxytocin applications [17].
The study by Berger [9], women who followed their birth plans had fewer interventions. Of the women in the experimental group, only 60% shared their birth plans with their physicians, and 19.1% did not receive any support for their childbirth preferences. Both of these results indicate that women’s opinions about the interventions and initiations made during the delivery were not considered.
A previous study found that the pregnant women with birth plans were less satisfied, since their deliveries did not meet their expectations [17]. Similar to the studies by Farahat et al. [7] and Berger [9], the present study determined that the women that had birth plans were more satisfied with their delivery than those who did not have birth plans. The researchers believe that the mothers in this study who had childbirth preparation training developed their birth plans in a more realistic manner; this might have affected the study results. This study was determined that birth plans mostly had a positive effect on women’s preferences concerning the childbirth process except for rates of cesarean section and interventions and on the level of their satisfaction with their delivery. If communication is improved among the pregnant women visiting the outpatient clinics and the midwives and nurses working there, as well as an increase in trust between them, birth plans will be shared with midwives and nurses. This sharing will help midwives and nurses play an active role in the development of birth plans. In this regard, the study suggests that midwives and nurses play an active role in prenatal training classes, and gain awareness regarding the development of birth plans. The use of birth plans has shown contradictory results about cesarean section and interventions in published literature. It is also suggested that the study is repeated using a larger sample and taking into consideration the effect of using birth plans on birth results.
The researchers acknowledge Associate Professor Doctor O.T. for his guidance and contribution to the statistical analysis of this study.