

 , Henrique Lima de Oliveira 1, Khissya Beatryz Alves de Lima 1
, Henrique Lima de Oliveira 1, Khissya Beatryz Alves de Lima 11 Department of Medicine, Federal University of Goiás, Goiânia, GO 74605-050, Brazil
2 Medical Department, Medical Sciences and Life School, Pontifical Catholic University of Goiás, Goiânia, GO 74605-050, Brazil
Abstract
Hypertrophic cardiomyopathy (HCM) is genetically heterogeneous and characterized by left ventricular hypertrophy, myocardial fibrosis, and diverse clinical manifestations. Although circulating microRNAs (miRNAs) are promising biomarkers of pathological cardiac remodeling, the correlation of these miRNAs with specific clinical characteristics of HCM remains unclear. Therefore, we systematically reviewed and quantified the correlation between circulating miRNAs and structural and functional cardiac parameters in HCM.
This systematic review and meta-analysis of observational studies evaluated the association between circulating miRNA expression levels and Echocardiography, magnetic resonance imaging, and histological parameters for HCM. We comprehensively searched the PubMed, Embase, Scopus, and Web of Science databases, and extracted and transformed correlation coefficients into Fisher’s Z-scores. The study was registered with PROSPERO under registration number CRD420251058653. Meta-analyses were conducted using random-effects models, and heterogeneity was assessed using the I2 statistic. Sensitivity analyses, meta-regression, and publication bias were also assessed.
A total of 11 studies comprising 633 patients were included. Pooled analysis showed moderate-to-strong positive correlations between miRNAs (miR-21, miR-29a, miR-199a-5p, and miR-27a) and myocardial fibrosis, wall thickness, and left ventricular mass (r = 0.53; 95% confidence interval 0.40–0.64; I2 = 60.1%). Sensitivity and meta-regression analyses confirmed the robustness of the results, with no significant publication bias. The risk-of-bias assessment (Quality Assessment of Diagnostic Accuracy Studies 2) revealed moderate concerns, primarily related to patient selection and index-test blinding.
Circulating miRNAs were significantly correlated with structural and functional cardiac changes in HCM, supporting the potential role of these miRNAs as noninvasive biomarkers. However, further high-quality studies are needed to validate their clinical applicability.
Keywords
- biomarkers
- correlation
- hypertrophic cardiomyopathy
- microRNA
- diagnostic
Hypertrophic cardiomyopathy (HCM), one of the most common autosomal-dominant cardiomyopathies with an estimated prevalence of 1:200–1:500 [1], is characterized by heterogeneous clinical manifestations, including ventricular arrhythmias, asymptomatic cases, and sudden death, that result from gene–environmental influences and the failure of protective processes [2, 3]. Despite the unclear pathological mechanisms, there is a correlation between multiple factors that contribute to the HCM condition, including heterozygous mutations in genes that encode structural and/or regulatory proteins in the sarcomere of cardiac cells, particularly MYBPC3 and MYH7 [3, 4], and other mechanisms, including mitochondrial dysfunction and oxidative stress, which contribute significantly to cardiac remodeling and hypercontraction to generate a feedback loop driven by increased energy demand [5]. Significant correlations exist between microRNAs (miRNAs) and several pathobiological processes, including alterations in sarcomeric proteins [4]. miRNAs mediate several pathophysiological processes in the post-transcriptional regulation of cardiac protein production [4, 6] and play important regulatory roles; thus, aberrant miRNA production contributes to the pathogenesis of myocardial diseases [4, 7].
Current therapeutic strategies for hypertrophic cardiomyopathy focus primarily on symptom control and hemodynamic improvement, including beta-blockers, calcium-channel blockers, septal reduction therapies, and, more recently, cardiac myosin inhibitors [5]. However, these approaches do not directly address the molecular mechanisms underlying disease progression. In this context, circulating microRNAs have emerged as promising molecular regulators of myocardial hypertrophy and fibrosis. Although miRNA-based therapies are not yet clinically available, accumulating experimental evidence suggests that miRNAs may represent future therapeutic targets, in addition to their role as noninvasive biomarkers. Understanding their relationship with structural remodeling may therefore help develop more personalized therapeutic strategies in HCM [3, 4, 5, 6, 7, 8].
Precise correlations between genotypes and phenotypes in HCM are lacking. Family members with the same genetic mutation may exhibit distinct HCM symptoms, conferring phenotypic heterogeneity [8]. Non-coding RNAs, such as circRNAs and miRNAs, have emerged as potential diagnostic and prognostic biomarkers and therapeutic targets [4, 6, 9]. This review aimed to quantify the correlation between circulating miRNAs and structural and functional cardiac parameters in patients with HCM.
This systematic review and meta-analysis were performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline [10]. The study was registered with PROSPERO (https://www.crd.york.ac.uk/PROSPERO/; registration number CRD420251058653).
On May 6, 2025, the PubMed, Scopus, Embase, and Web of Science databases were searched for randomized controlled trials and observational studies published between 2007 and May 2025, using the search terms and keywords (“Mirna”) and (“hypertrophic cardiomyopathy”), without restrictions on the language of the studies. The Cochrane Library was not included in the primary search strategy because it primarily includes randomized controlled trials and interventional studies. As the present review focused on observational studies evaluating correlations between circulating microRNAs and clinical parameters, databases more suited for observational and translational research were prioritized. To minimize the risk of missing relevant studies, the reference lists of all included articles were manually screened. Each study was carefully referenced to ensure that no relevant research was ignored (Supplementary Methods).
The reference lists of the studies identified in the databases were exported to Rayyan software (version 5:210, University of Oxford, UK, 2016) to remove duplicates. The study selection was conducted in two phases: first, two independent reviewers assessed the titles and abstracts according to the eligibility criteria; second, the same reviewers reapplied the inclusion criteria after reading the full text. A third reviewer resolved discrepancies.
Studies were included if: (I) a clear Pearson correlation coefficient assessed the correlation between miRNA levels and the variable of interest; (II) there was sufficient data for statistical analysis of the sample; and (III) identification and quantification of miRNAs. Studies using overlapping patient cohorts were excluded. In cases of multiple publications on the same patient group, preference was given to publications with the most extensive dataset. Studies lacking sufficient data for visualization analysis, such as Pearson’s coefficient or primary information for their design, were excluded. The prespecified data points extracted from each study included study design, sample size, patient characteristics, microRNA-specific details, and measures of detail (e.g., Pearson’s coefficient and p-value).
To assess the potential for bias, each study included in the analysis was independently evaluated by two reviewers using the Risk of Bias in Non-randomized Studies - of Interventions (ROBINS-1) and classified into one of four risk profiles, from negligible to concerning [11]. Confounding factors, selection, and categorization of intervention measurements, deviations from planned interventions, missing data, outcome measurements, and reporting biases were included.
Publication bias was assessed using funnel plot analysis and Egger’s test, with the primary outcomes of the review considered.
The clinical outcomes included structural and functional parameters, with a
focus on the main phenotypic features of HCM, including hypertrophy, fibrosis,
and ventricular dysfunction. Myocardial fibrosis, identified primarily by late
gadolinium enhancement (LGE) on cardiac magnetic resonance imaging (MRI),
reflects the degree of tissue remodeling and chronic structural damage.
Ventricular hypertrophy was assessed in the left ventricular wall by
echocardiography, the gold standard for diagnosis; an interventricular septal
thickness
| Study | Study design | Country | Sample, N | HCM or HOCM diagnosed by Echocardiography% | Setting | Application | Gold standard | Female sex, N (%) | Age, yearsa | Age, yearsb |
| Roncarati et al. 2014 [12] | Observational study | Italy | 82 | 50.0 | HCM patients with wall thickness |
Peripheral plasma levels of miRNAs were assessed by quantitative real-time polymerase chain reaction | Echocardiography | 0 (0) | 50 |
50 |
| Fang et al. 2015 [19] | Observational study | Australia | 8 | 66.6 | HCM patients with interventricular septum thickness |
Peripheral plasma levels of miRNAs PCR array | Echocardiography | 3 (37.5) | 42.0 |
51.3 |
| Huang et al. 2020 [18] | Observational study | China | 72 | 58.3 | HOCM patients with myocardial wall |
Peripheral plasma levels of miRNAs were assessed by quantitative real-time polymerase chain reaction | Echocardiography | 23 (31.9) | 45.57 |
46.24 |
| Derda et al. 2015 [13] | Observational study | Germany | 73 | 68.4 | HCM patients with a hypertrophic cardiac septum ( |
Peripheral plasma levels of miRNAs were assessed by quantitative real-time polymerase chain reaction | Echocardiography | 45 (61.64) | 42.45 (NR) | 56.17 (NR) |
| Gudkova et al. 2020 [17] | Observational study | Russia | 93 | 52.7 | HCM patients with echocardiographic evidence of maximum left ventricular wall thickness |
Peripheral plasma levels of miRNAs were assessed by quantitative real-time polymerase chain reaction | Echocardiography | 55.1 | NR | 50 (32–65) |
| Li et al. 2018 [14] | Observational study | China | 20 | 50.0 | HCM patients with echocardiographic evidence of maximum left ventricular wall thickness |
Peripheral plasma levels of miRNAs were assessed by quantitative real-time polymerase chain reaction | Echocardiography | 4 (20) | NR | 39 |
| Ntelios et al. 2017 [21] | Observational study | Netherlands | 80 | 60.0 | Patients were subjected to standard echocardiographic evaluation | Peripheral plasma levels of miRNAs were assessed by quantitative real-time polymerase chain reaction | Echocardiography | NR | NR | NR |
| Sonsöz et al. 2022 [2] | Observational study | Turkey | 40 | 50.0 | The diagnosis of HCM was based on echocardiographic demonstration of a hypertrophic but non-dilated left ventricle (wall thickness |
Peripheral plasma levels of miRNAs were assessed by quantitative real-time polymerase chain reaction | Echocardiography | 17 (42.5) | 42 |
47 |
| Thottakara et al. 2021 [15] | Observational study | Germany | 35 | 68.6 | HCM patients with echocardiographic evidence of maximum left ventricular wall thickness |
Peripheral plasma levels of miRNAs were assessed by quantitative real-time polymerase chain reaction | Echocardiography | 18 (51.4) | 49 |
54 |
| Zhang et al. 2022 [16] | Observational study | China | 25 | 84.0 | The diagnosis of HCM was based on echocardiographic or CMR demonstration of a hypertrophied but nondilated LV (with maximal wall thickness |
Peripheral plasma levels of miRNAs were assessed by quantitative real-time polymerase chain reaction | Echocardiography | 15 (60) | 51 (32–59) | 55 (41–60) |
| Davydova et al. 2020 [20] | Observational study | Russia | 105 | 57.1 | HCM patients with echocardiographic evidence of maximum left ventricular wall thickness |
Peripheral plasma levels of miRNAs were assessed by semiquantitative real-time polymerase chain reaction | Echocardiography | NR | 51.5 (36.2–65.7) | NR |
a Mean
b Mean
HCM, hypertrophic cardiomyopathy; HOCM, hypertrophic obstructive cardiomyopathy; miRNAs, microRNAs; PCR, polymerase chain reaction; ECG, electrocardiogram; CMR, cardiac magnetic resonance; LV, left ventricle; NR, Not Reported.
Other relevant outcomes included the left ventricular mass index adjusted for body surface area, which provides a more accurate estimate of myocardial mass overload; maximum ventricular wall thickness, which is considered a marker of the severity of hypertrophy; and left ventricular outflow-tract obstruction, which is seen in a significant proportion of patients and confers more severe clinical symptoms and a higher risk of events (Table 2). In addition to representing the primary pathophysiological targets in HCM, these outcomes were selected for their clinical and prognostic relevance. The analysis of their correlation with circulating miRNA levels could elucidate their potential as noninvasive biomarkers of underlying cardiac alterations, enabling risk stratification and personalized clinical decision-making.
| microRNA | Outcome | Correlation coefficient (r) | 95% CI | p-value | I2 (%) | Significance |
| miR-29a/29a-3p | Fibrosis & hypertrophy | 0.52 | 0.47–0.72 | 0% | Significant | |
| miR-21 | Fibrosis & remodeling | 0.53 | 0.35–0.67 | 67.7% | Significant | |
| miR-199a-5p | Hypertrophy | 0.32 | 0.03–0.56 | 0.030 | 19.5% | Significant |
| miR-27a | Hypertrophy | 0.42 | 0.13–0.65 | 0.006 | - | Significant |
| miR-1/1-3p | LV function | 0.25 | 0.04–0.44 | 0.163 | 71.3% | Significant |
| miR-10b/10b-5p | LV function | −0.46 | −0.87 to 0.22 | 0.161 | 0% | Not Significant |
| miR-155 | Protective association | Negative | Not stated | Not stated | - | Significant |
| miR-19b | Protective association | Negative | Not stated | Not stated | - | Significant |
Pearson’s correlation coefficients (r) and the corresponding 95% confidence
intervals (CI) for circulating miRNA levels and clinical and structural
parameters of HCM were combined using the inverse-variance method. To stabilize
the variance of the coefficients, Pearson’s correlations were transformed into
Fisher’s Z-scores (ZCOR) as described by Zhang et al. (2022) [16].
Heterogeneity among the included studies was assessed using Cochran’s Q statistic
(chi-square) and I2 index. Heterogeneity was considered statistically
significant at p
Subgroup analyses were conducted to explore potential sources of variation, considering study characteristics, including the specific miRNA type analyzed, the clinical outcome (e.g., myocardial fibrosis, interventricular septal thickness, LVMI, and LVEF), and the grouping of outcomes (structural versus functional). Differences between subgroups were analyzed using the Q-statistic for heterogeneity. Meta-regression analyses were performed using continuous variables (mean participant age, proportion of women in the sample, and sample size) to investigate the influence of these factors on the correlation coefficients.
The robustness of the results was verified through a leave-one-out sensitivity analysis, in which each study was sequentially excluded to assess the impact on the pooled estimate and overall heterogeneity. Prediction intervals were calculated to estimate the expected variability in future studies with similar designs. Publication bias was assessed by visual inspection of funnel plots and Egger’s and Begg’s statistical tests. If identified, the trim-and-fill imputation method was used to correct graph asymmetry.
All statistical analyses were performed using R version 3.6.0 (R Foundation for Statistical Computing, Vienna, Austria) with the “meta” and “metafor” packages.
A leave-one-out sensitivity analysis was performed for the primary outcomes to assess the influence of individual studies on the pooled results. A Baujat plot was used to identify the potential sources of heterogeneity. Univariate meta-regression with a mixed-effects model was conducted to evaluate the following moderators: age of the control group, age of the HCM/HOCM group, percentage of females, prevalence of HCM/HOCM, and sample size.
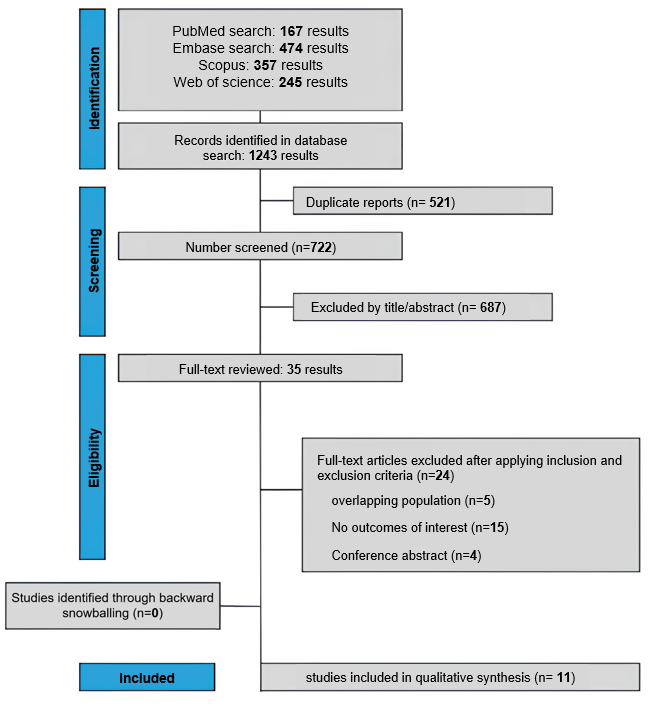
The initial search yielded 1243 articles (Fig. 1). Of these, 35 articles underwent a detailed review, and after careful evaluation, only 11 were selected for inclusion in the meta-analysis. All selected studies were observational and non-interventional, implying data analysis without direct manipulation of the variables of interest. The sample sizes of the studies included varied substantially, ranging from 8 to 105 patients, with a total of 633 patients, as shown in Supplementary Table 1.
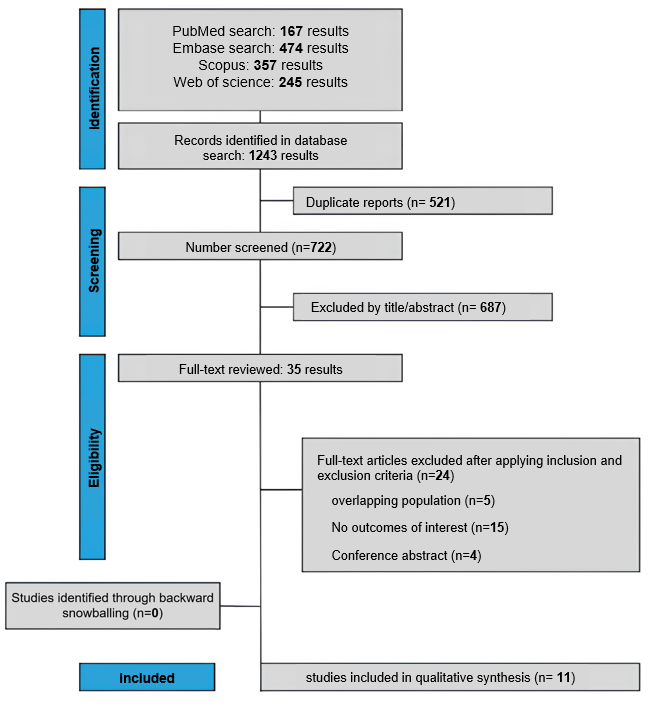 Fig. 1.
Fig. 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart.
The reference gold standard for diagnosing HCM is echocardiography, due to its high accuracy in detecting structural heart abnormalities. To evaluate the biomarkers under investigation, the studies analyzed human plasma miRNA levels using real-time PCR (qPCR). The choice of miRNAs as biomarkers is supported by increasing evidence of their role in regulating pathophysiological processes, including outcomes analyzed in the studies (Supplementary Table 2).
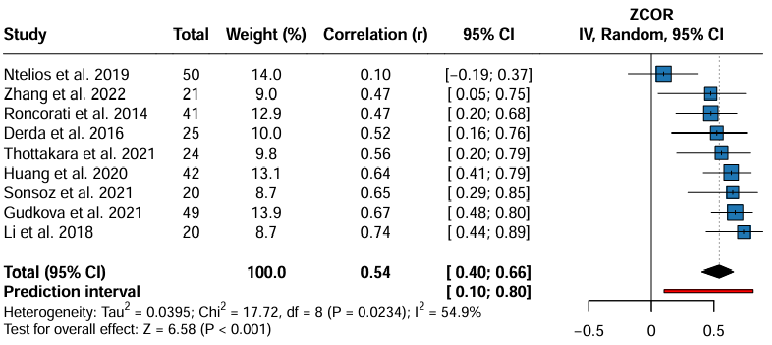
The meta-analysis of nine studies (Fig. 2) investigated the overall
association between circulating miRNAs and cardiac changes in HCM. It is
important to note that heterogeneity among studies is also due to the variety of
miRNAs examined and to the specific cardiac changes assessed, such as fibrosis
and hypertrophy. An overall positive and significant correlation was observed (r
= 0.54; 95% CI: 0.40–0.66; p
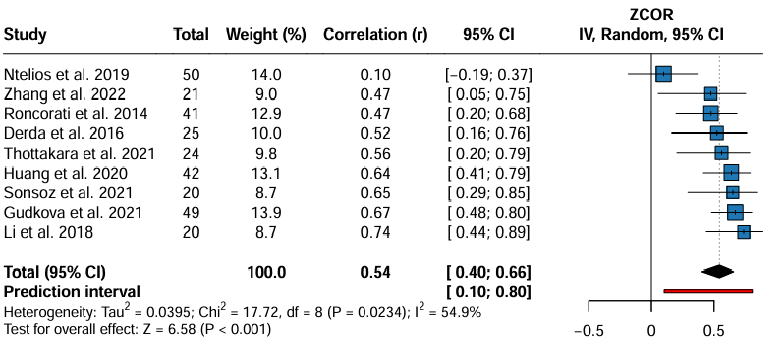 Fig. 2.
Fig. 2.
Pooled correlation between circulating miRNAs and LV structural parameters in HCM. Abbreviations: HCM, Hypertrophic Cardiomyopathy.
The leave-one-out sensitivity analysis further supported the robustness of the
meta-analysis (Supplementary Fig. 1). The pooled correlation coefficient
(r) remained stable, ranging from 0.51 to 0.59, and consistently reached
statistical significance across all individual study omissions (p
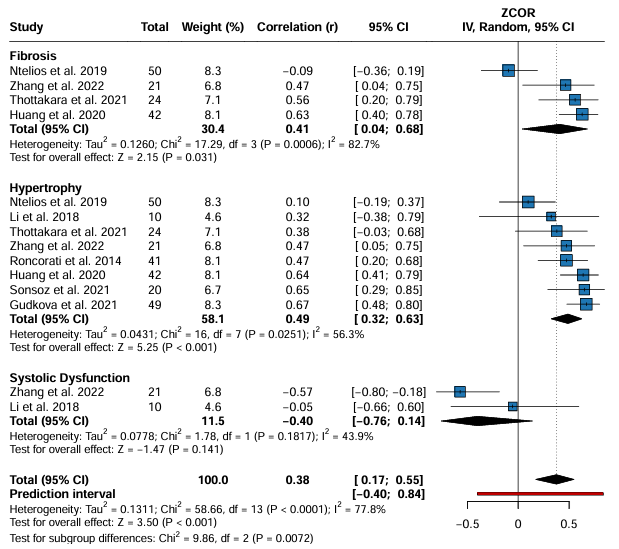
Pooled meta-analyses with 14 (Fig. 3) and 16 (Fig. 4) studies were conducted to
evaluate the correlation between molecular biomarkers and different structural
and functional parameters of the heart, respectively. Fig. 3 shows distinct
associations: significant positive correlations were observed for myocardial
fibrosis (r = 0.41; p = 0.031) and ventricular hypertrophy (r = 0.49;
p
 Fig. 3.
Fig. 3.
Subgroup meta-analysis of circulating miRNAs in HCM.
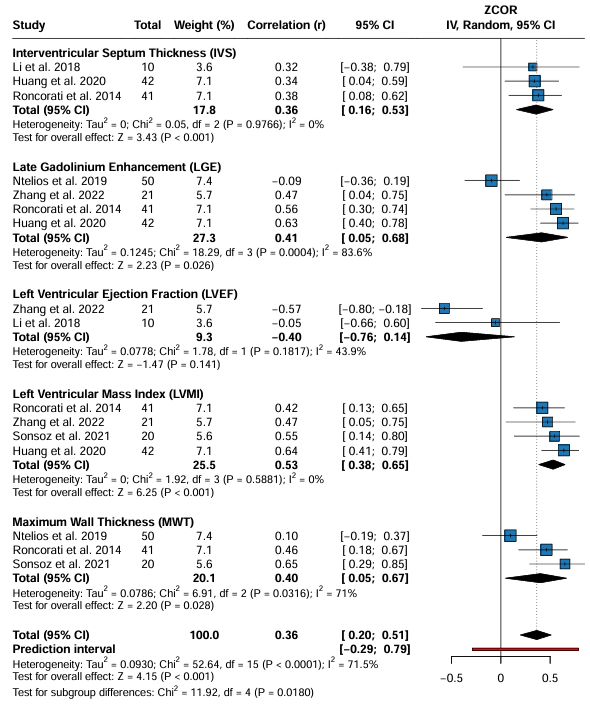
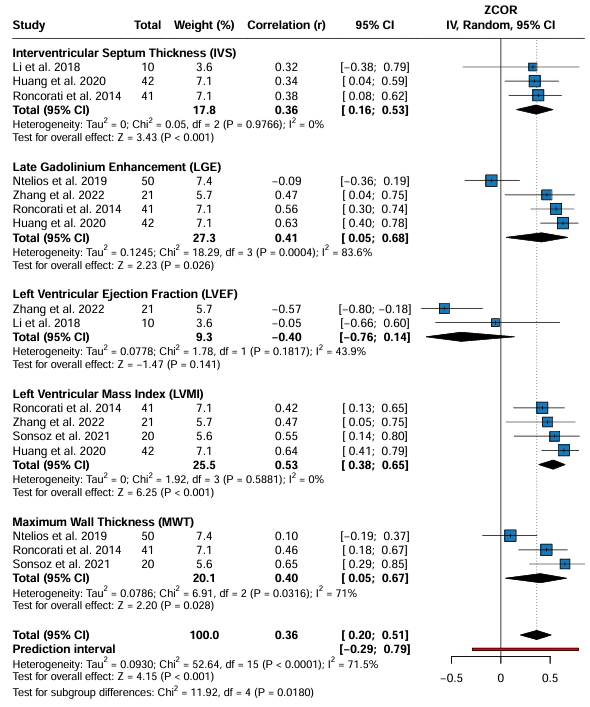 Fig. 4.
Fig. 4.
Subgroup meta-analysis of circulating miRNAs and cardiac parameters in HCM.
In the analysis of the second group (Fig. 4), the correlation between biomarkers
and interventricular septal thickness (IVS) showed a significant association (r =
0.36; 95% CI: 0.16–0.53; p
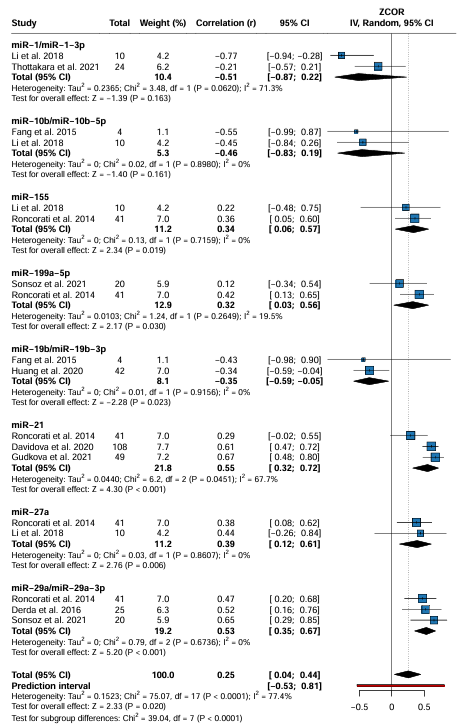
The subgroup analysis of specific correlations between different miRNAs (Fig. 5) and cardiac remodeling parameters grouped the studies into 8 subgroups based on the miRNAs analyzed. Heterogeneity between subgroups was statistically significant, which indicated important differences in the estimated effects among the miRNAs evaluated. Neither miR-1/miR-1-3p nor miR-10b/miR-10b-5p showed significant associations with cardiac outcomes. miR-10b/miR-10b-5p showed a negative correlation (r = –0.46; 95% CI: –0.83 to 0.19), but without significance (p = 0.161) or heterogeneity (I2 = 0%) [17, 19]. Thus, despite potential trends, miRNAs do not demonstrate a statistically significant correlation with structural or functional alterations in HCM [12, 14, 19].
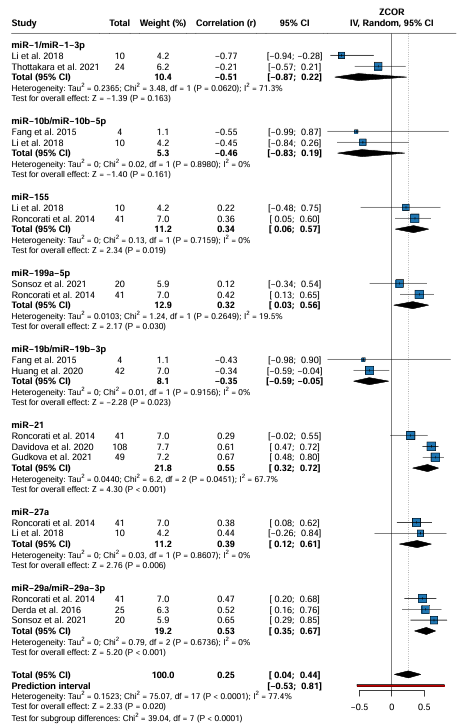 Fig. 5.
Fig. 5.
Specific correlations between circulating miRNAs and cardiac structural parameters in HCM.
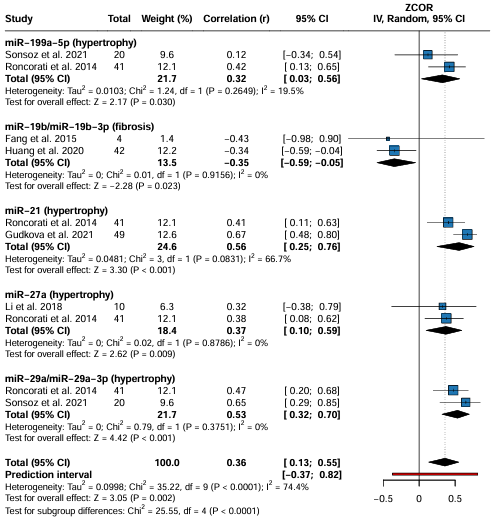
Subgroup analyses of specific miRNA types (Figs. 6,7) identified several
biomarkers that were significantly positively correlated with cardiac
alterations. Notably, miR-29a/miR-29a-3p (r = 0.53; 95% CI: 0.32–0.70;
p
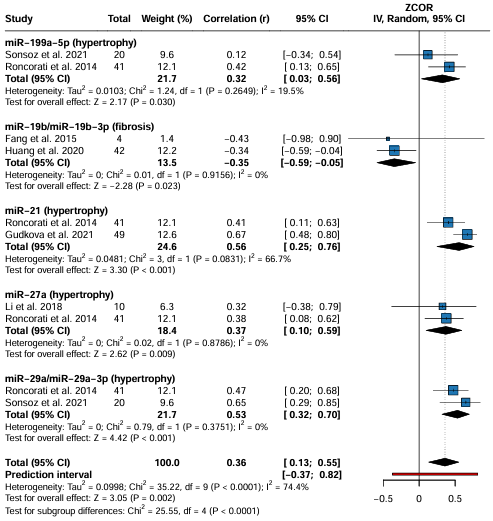 Fig. 6.
Fig. 6.
Pooled correlations between specific circulating microRNAs and cardiac remodeling parameters in HCM, including left ventricular wall thickness, mass index, and fibrosis. Abbreviations: CI, confidence interval; r, correlation coefficient.
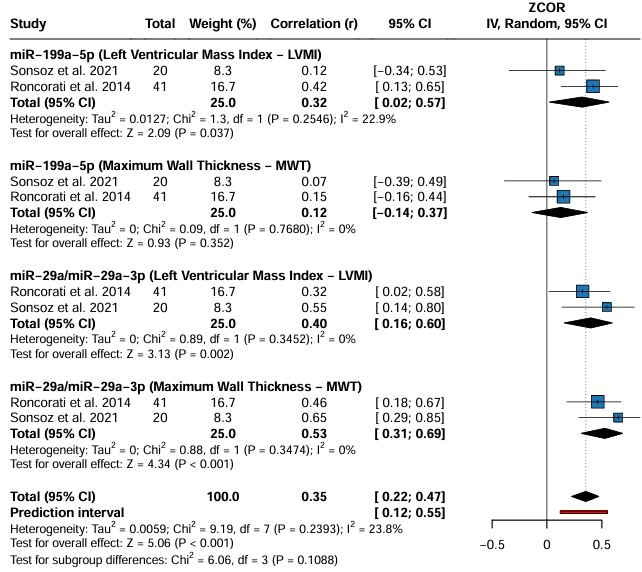
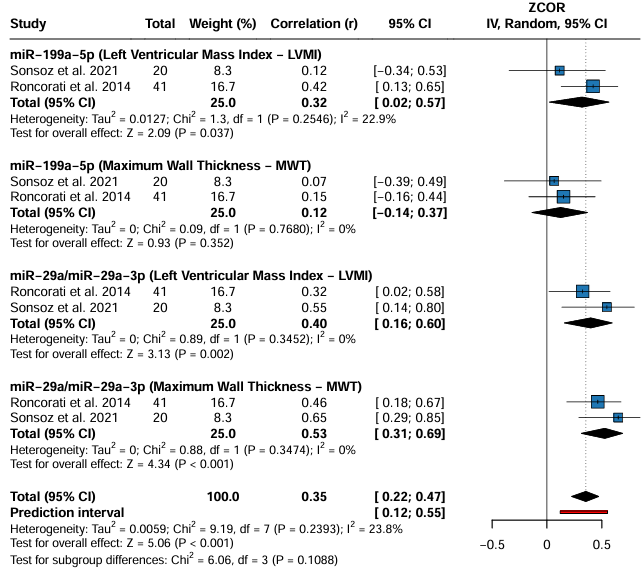 Fig. 7.
Fig. 7.
Significant positive correlations between specific circulating miRNAs and cardiac structural parameters in HCM.
These findings reinforce the relevance of specific miRNAs, particularly miR-21, miR-29a, miR-199a-5p, and miR-27a, as potential biomarkers of cardiac structural alterations. However, the negative results observed for miR-10b and the lack of significance for miR-1 suggest that not all miRNAs have the same discriminative value, which highlights the importance of careful marker selection for future studies (Fig. 7).
Meta-regression analysis investigated whether the age of the control group, age of the HCM/HOCM group, percentage of female sex, prevalence of HCM/HOCM, and sample size moderated the correlation coefficient (r). Despite the visual trends observed in the bubble plots (Supplementary Fig. 3), none of these factors demonstrated a statistically significant influence on “r”. The p-values for the moderator coefficients were as follows: age of the control, p = 0.3853; age, HCM/HOCM, p = 0.1440; percentage of female sex, p = 0.5401; prevalence of HCM/HOCM, p = 0.4471; and sample size, p = 0.4797.
Considerable significant residual heterogeneity was identified in the models for
evaluating the prevalence of HCM/HOCM (I2 = 55.45%, QE test, p =
0.0224) and sample size (I2 = 55.99%, QE test, p = 0.0187). Thus,
variables not included in the analysis may have contributed to the variation
observed in the correlation coefficients across studies. The intercepts of the
models were statistically significant for age in HCM/HOCM (p = 0.0177),
the percentage of females (p
The methodological quality of the studies was heterogeneous; the Patient Selection (D1) and Index Test (D2) domains concentrated on the risk of bias, whereas the Reference Standard (D3) and Flow and Time (D4) domains were of high quality. This resulted in a moderate overall risk of bias in more than half of the studies (Supplementary Fig. 4).
Based on the funnel plot, the distribution of the studies used to assess publication bias appeared to be asymmetrical. However, Egger’s test did not indicate a significant publication bias (p = 0.353; Supplementary Fig. 3).
This systematic meta-analysis comprehensively explored the correlation between
circulating miRNAs and clinical and structural parameters of HCM. It reinforced
the role of miRNAs as potential molecular biomarkers for both diagnosis and
monitoring of disease progression [2, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21]. Aggregated data from 11
observational studies, including 633 patients with HCM, showed a moderate overall
positive correlation (p
Pooled analyses stratified by clinical outcomes showed significant positive correlations between miRNA levels and indicators of myocardial fibrosis and ventricular hypertrophy. In contrast, the association with left ventricular systolic dysfunction, as assessed by ejection fraction, did not reach statistical significance, suggesting that the miRNAs studied may be more strongly related to structural remodeling than to contractile function. This dissociation may be explained by the relative preservation of systolic function in most patients with HCM, particularly in early-stage disease.
Garmany et al. [22] demonstrated a relationship between circulating miRNA levels and the activation of inflammatory, acute-phase signaling, IL-6, and hypertrophy pathways, which lead to clinical outcomes such as inflammation, hypertrophy, and fibrosis. Osmak et al. [23] reinforced these pathways by highlighting that the clinical outcomes of fibrosis and sudden cardiac death overlap with elevated miRNA levels in HCM. These studies contribute to our understanding of the regulatory pathways of miRNAs in the pathophysiology and complications of HCM.
Besides clusters, more specific anatomical parameters, such as IVS thickness,
LVMI, and MWT, correlated positively with circulating miRNA levels. For example,
the LVMI (r = 0.53; 95% CI: 0.38–0.65; p
Subgroup analyses allowed the identification of specific miRNAs with greater
discriminative power. Among the biomarkers with significant positive correlation,
the following stand out: miR-29a/miR-29a-3p, miR-21, miR-199a-5p, and miR-27a
[2, 12, 13, 17]. MiR-29a/miR-29a-3p (r = 0.53, 95% CI: 0.35–0.67; p
In contrast, miRNAs such as miR-155 and miR-19b showed a significant negative correlation with cardiac outcomes with high consistency, indicating a potential protective or associative role in less severe disease states. However, miR-10b/miR-10b-5p and miR-1/miR-1-3p did not demonstrate statistically significant correlations. This suggests that not all miRNAs studied have equivalent clinical applicability, reinforcing the need for individualized functional validation of these biomarkers. Other studies found correlations between miR-1-3p and miR-1 and hypertrophy [14, 15, 27, 28].
The heterogeneity observed in several analyses, especially among miRNAs grouped by type, highlights the biological differences in the regulatory and expression pathways of these small noncoding RNAs. This reinforces the need for specific approaches for each miRNA of interest and discourages the use of generic panels without prior validation owing to the high genetic and clinical heterogeneity of HCM [29, 30, 31].
In the clinical context of HCM, our findings reinforce the association between circulating miRNA expression profiles and relevant phenotypic disease manifestations, such as myocardial hypertrophy, fibrosis, and sudden cardiac death. Ventricular hypertrophy, a key feature of HCM, significantly correlated positively with miRNAs, such as miR-21, miR-199a-5p, and miR-27a, particularly with respect to structural parameters, including left ventricular mass index and maximum wall thickness. Myocardial fibrosis, which contributes to diastolic dysfunction and arrhythmic risk, is robustly associated with miR-29a, which is regulates the extracellular matrix. Regarding sudden cardiac death, although this outcome was not directly quantified in the pooled statistical analysis, individual studies indicated elevated levels of proinflammatory and pro-fibrotic miRNAs in patients with severe arrhythmic events, suggesting a possible future applicability of these markers in arrhythmic risk stratification [22, 23]. The results indicate a direct relationship between the levels of specific miRNAs and the most relevant clinical components of HCM, indicating their potential as complementary tools in prognostic assessment and, eventually, in personalized therapeutic decision-making.
Early detection of HCM is clinically challenging, especially in asymptomatic patients or those with milder disease, for whom imaging tests may not be conclusive in the early stages [30, 32]. Findings regarding circulating miRNAs, particularly miR-29a, miR-21, and miR-199a-5p, which robustly correlate with hypertrophy and fibrosis, have encouraged the development of noninvasive and low-cost screening tests. Blood collection and analysis by real-time PCR (qPCR) can complement current clinical and genetic assessments to identify individuals at risk who may require more complex cardiac examinations, such as echocardiography or MRI. This represents a significant advancement, enabling cardiologists and general practitioners to perform more effective screening, utilize diagnostic imaging resources more efficiently, and optimize patient management from the earliest stages.
Although most studies in our review focused on correlation analysis, only three assessed diagnostic performance and reported area under the curve (AUC) values ranging from 0.71 to 0.92; these preliminary data suggest that miRNAs, either alone or in combination, may differentiate patients with HCM from healthy individuals or between disease subtypes. However, these studies were limited by small sample sizes, a lack of standardization in miRNA quantification, and heterogeneous reference standards. Further prospective studies incorporating predefined diagnostic thresholds and multivariate models are needed to validate these findings and establish clinical cutoff values.
The translational potential of circulating miRNAs depends on their mechanistic relevance. For example, miR-21 and miR-29a are known modulators of fibrosis-related pathways, whereas miR-199a-5p is associated with cardiomyocyte hypertrophy. These associations suggest that, beyond serving as biomarkers, miRNAs could eventually be therapeutic targets or part of gene expression panels to inform personalized treatment strategies. As miRNA profiling technologies advance, integrating molecular signatures into HCM phenotyping may enhance precision medicine in cardiomyopathy care.
Genetics plays a central role in HCM, with the disease primarily caused by
heterozygous mutations in genes that encode sarcomeric proteins, such as
Beyond diagnosis, miRNA-based therapeutic approaches for HCM are emerging areas of research with transformative clinical potential [33]. As miRNAs play crucial roles in the post-transcriptional gene regulation of cardiac proteins and are implicated in fibrogenesis and hypertrophy pathways, they are not only biomarkers but also potential targets for novel therapies [32, 33]. Pharmacological modulation of specific miRNA expression (e.g., inhibition of pro-hypertrophic miRNAs or activation of antifibrotic miRNAs) may offer an innovative strategy to slow or reverse pathological cardiac remodeling. This suggests the need for treatments that directly target molecular pathomechanisms, complementing or even surpassing current therapies that primarily target symptoms. Although still in the research phase, a deeper understanding of the correlations between miRNAs and clinical outcomes is the first fundamental step toward translating this knowledge into interventions that can effectively modify the course of HCM and improve patient quality of life [32, 34, 35].
Future research should build on the strong evidence presented here, which links circulating microRNAs to structural changes in hypertrophic cardiomyopathy. It’s important to use prospective, long-term studies to track how miRNA levels change over time and how these changes relate to disease progression, patient outcomes, and treatment efficacy. Also, to make the results more reliable and comparable across different studies, we need to standardize how we detect and measure miRNAs.
Currently, different studies use different methods and analysis techniques. Therefore, creating standardized procedures for collecting samples, extracting RNA, and measuring it is crucial for applying these findings in personalized clinical approaches.
Future investigations should, crucially, incorporate genetic predisposition and molecular characterization, specifically sarcomeric mutations such as MYH7 and MYBPC3, alongside circulating miRNA profiles. This integrated methodology could elucidate the significant phenotypic variability seen in HCM, thereby facilitating more precise risk assessment.
Furthermore, given the growing recognition of miRNAs as modulators of fibrosis and hypertrophy, additional mechanistic and translational research is essential to investigate their potential utility not only as diagnostic indicators but also as therapeutic targets, thereby advancing precision medicine in hypertrophic cardiomyopathy.
This systematic review and meta-analysis have some limitations that must be considered for a critical, contextualized interpretation of the results. First, the observational nature of the included studies is a significant limitation; the inclusion of these non-interventional studies cannot establish causal relationships between circulating miRNA levels and clinical parameters of HCM. The lack of longitudinal follow-up limits the ability to assess the temporal dynamics of miRNA expression throughout disease progression or even in response to therapeutic interventions. Second, concerns exist regarding methodological heterogeneity among the included studies. Substantial variations were observed in the inclusion criteria, miRNA quantification methods, populations evaluated, definitions of clinical outcomes, and controls used. This heterogeneity, as reflected in the high I2 indices across several analyses, hinders direct comparability between studies and may have influenced the observed effect sizes. Third, the wide variation in sample sizes across individual studies, ranging from 8 to 105 patients, is noteworthy. This may have compromised the statistical power of some analyses and increased the risk of sampling bias. Studies with small sample sizes are more susceptible to random errors and unstable results, which can compromise the robustness of the inferences drawn from their data. Fourth, publication bias is an inherent consideration in any meta-analysis. Although studies with negative or non-significant results may be published less frequently, in this review, the funnel plot did not suggest prominent asymmetry, and Egger’s test revealed no statistically significant evidence of publication bias. Fifth, few studies have provided detailed information on confounding factors, such as medication use, cardiovascular comorbidities, age, sex, and other variables, that can influence both miRNA expression and clinical parameters of HCM. The lack of control or adjustment for these factors limits the internal validity of our findings. Despite the significant correlation between specific miRNAs and structural alterations, functional evaluation was not conducted in vitro or in vivo to confirm the biological roles of the identified miRNAs. This limitation hinders the extrapolation of molecular data for a deeper mechanistic understanding, thereby hindering the identification of effective therapeutic targets. Finally, despite the initial proposal to explore the diagnostic potential of miRNAs and the statistical robustness of these correlations, this analysis remains limited to the associative field and does not incorporate formal measures of diagnostic accuracy. The lack of studies with designs specifically focused on evaluating diagnostic performance, such as sensitivity, specificity, likelihood ratios, and AUC, limits the ability to translate these findings into clinical practice as screening or diagnostic confirmation tools. Therefore, there is a critical need for new studies with prospective designs, larger sample sizes, well-defined control groups, and a focus on quantifying the accuracy of miRNAs as clinical biomarkers. These studies should aim to enable early detection, risk stratification, and progression monitoring of patients with HCM, thereby transforming promising molecular findings into established diagnostic tools.
We provide consistent evidence of the association between circulating miRNA levels and the clinical and structural parameters of HCM. miRNAs, such as miR-29a, miR-21, and miR-199a-5p, exhibited statistically significant correlations with markers of cardiac remodeling, particularly hypertrophy and fibrosis, suggesting their potential as noninvasive biomarkers in the diagnosis and prognosis of the disease. Future studies should focus on prospective, longitudinal cohorts to validate the prognostic value of circulating microRNAs in hypertrophic cardiomyopathy. Standardization of miRNA detection methods and integration with genetic background, imaging findings, and clinical outcomes will be essential to improve reproducibility and clinical applicability. These advances may allow circulating miRNAs to serve not only as biomarkers of disease severity, but also as tools for personalized risk stratification and therapeutic decision-making in HCM.
The data that support the findings of this meta-analysis are available from the corresponding author upon reasonable request.
Conceptualization: ASMJ, HLO, KBAL, Data curation: ASMJ, HLO, KBAL. Formal analysis: HLO, KBAL. Methodology: HLO and KBAL. Project administration: ASMJ. Resources: ASMJ. Supervision: ASMJ. Validation: ASMJ, HLO, and KBAL. Writing - original draft: HLO, KBAL, ASMJ. Writing - review and editing: HLO, KBAL, ASMJ. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
The authors would like to express their gratitude to all individuals who contributed to the development of this manuscript. We also thank the peer reviewers for their valuable comments and suggestions.
This research received no external funding.
The authors declare no conflicts of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/FBS47633.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.