






 , Sefayi Merve Özdemir 1, Tekincan Çağrı Aktaş 1,2, Özde Elif Gökbayrak 1, Aylin Erol 1, Deniz Kızmazoğlu 3, Safiye Aktaş 1,*
, Sefayi Merve Özdemir 1, Tekincan Çağrı Aktaş 1,2, Özde Elif Gökbayrak 1, Aylin Erol 1, Deniz Kızmazoğlu 3, Safiye Aktaş 1,*
1 Department of Basic Oncology, Oncology Institute, Dokuz Eylül University, 35330 İzmir, Turkey
2 Department of Pharmacology, Ege Üniversity, 35000 İzmir, Turkey
3 Department of Pediatric Oncology, Oncology Institute, Dokuz Eylül University, 35330 İzmir, Turkey
Abstract
Neuroblastoma (NB) is the most common extracranial solid tumor among pediatric cancers and accounts for approximately 15% of childhood cancer-related deaths. Neurotrophic receptor tyrosine kinases (NTRKs) are genes that play critical roles in the development and function of the nervous system. Therefore, elucidating the role of NTRKs in NB is important for both understanding basic biological mechanisms and developing novel therapeutic approaches. Specifically, NTRK fusions are being investigated as potential biomarkers and therapeutic targets for targeted therapy strategies. The tumor-agnostic TRK inhibitors larotrectinib and entrectinib are used to treat advanced or metastatic solid tumors with NTRK gene fusions. Accordingly, this study aimed to investigate the clinical significance of NTRK1, NTRK2, and NTRK3 point mutations, gene fusions, and protein expression, and to assess the effectiveness of these in guiding targeted therapy decisions in NB.
This study investigated pan-TRK expression, point mutations, and fusions in the NTRK1, NTRK2, and NTRK3 genes using next-generation sequencing (NGS) on paraffin-embedded blocks from 173 patients diagnosed with NB. Findings were analyzed in SPSS 29.0 using clinical data, MYCN amplification, and 11q deletion status, with Pearson correlation analysis applied at the p < 0.05 significance level.
Immunohistochemistry (IHC) for NTRK revealed that 67.9% of cases were NTRK-positive. NGS analysis identified NTRK1 missense point mutations in 20 cases, NTRK2 in 9 cases, and NTRK3 in 9 cases. In addition, 5 fusions were detected in 4 of the 103 patients who underwent fusion analysis.
Owing to the presence of neural tissue, NTRKs are highly positive in IHC, making these genes unsuitable as biomarkers for assessing NTRK inhibitor sensitivity and resistance, which are tissue-agnostic drugs. The observed low fusion rate is consistent with the literature, and the significance of the numerous point mutations identified as agnostic markers warrants further investigation. NTRK expression, fusion, and point mutations were not associated with clinical parameters or survival.
Graphical Abstract
Keywords
- neuroblastoma
- neurotrophic receptor tyrosine kinase
- gene fusion
- point mutation
Neuroblastoma (NB) is the most common extracranial solid tumor among pediatric cancers and is responsible for 15% of childhood cancer deaths [1, 2, 3]. The process typically begins with primary tumors arising in the adrenal medulla or along the sympathetic nervous system. NB is notable for its biological heterogeneity, and the course of the disease can exhibit diverse clinical courses, including spontaneous regression, differentiation, or metastasis [4, 5].
TRK proteins contain three main domains: an extracellular domain, a
transmembrane domain, and an intracellular domain. The tyrosine kinase domain is
the most important part of the receptor. The active kinase domain initiates
biological responses by triggering various signaling pathways within the cell,
including RAS/MAPK, PI3K/AKT, and PLC-
Neurotrophic receptor tyrosine kinases (NTRKs) are genes that play critical roles in the development and function of the nervous system. NTRK genes (NTRK1, NTRK2, and NTRK3) encode transmembrane receptors with tyrosine kinase activity [7, 8]. These receptors activate signaling pathways through interaction with neurotrophic factors, regulating biological processes such as cell proliferation, differentiation, and survival. However, abnormalities in these genes such as fusions, mutations, or overexpression, can affect tumor growth and metastasis, altering sensitivity to treatment [5, 7].
The role of NTRK genes in NB is important both for elucidating the underlying biological mechanisms and for developing therapeutic approaches. NTRK fusions or aberrant expression are being evaluated as potential biomarkers and therapeutic targets for targeted therapy strategies [8, 9]. In recent years, studies on the role of NTRK genes in NB have been an important step in understanding genetic heterogeneity.
Neurotrophic tyrosine receptor kinase (NTRK) inhibitors target abnormal tropomyosin receptor kinase (TRK) fusion proteins resulting from NTRK gene fusions, blocking their tyrosine kinase activity and thereby inhibiting the growth of cancer cells [10, 11]. Drugs such as larotrectinib and entrectinib bind with high affinity to TrkA, TrkB, and TrkC receptors, inhibiting their phosphorylation and thus downstream signaling pathways. This inhibition inhibits tumor growth by stopping cell proliferation and promoting apoptosis [12, 13].
Accordingly, examining NTRK gene expression and genetic alterations in NB not only provides a better understanding of the disease’s biology but also allows for the development of more effective treatment approaches. The potential of NTRK genes in targeted therapies, particularly the clinical success of tumor-agnostic TRK inhibitors, highlights the importance of NTRK fusions and other abnormalities as therapeutic targets. However, the rarity of NTRK fusions and factors such as genetic heterogeneity necessitate more comprehensive investigation of other alterations in these genes, particularly mutations and aberrant expression, to understand their clinical significance.
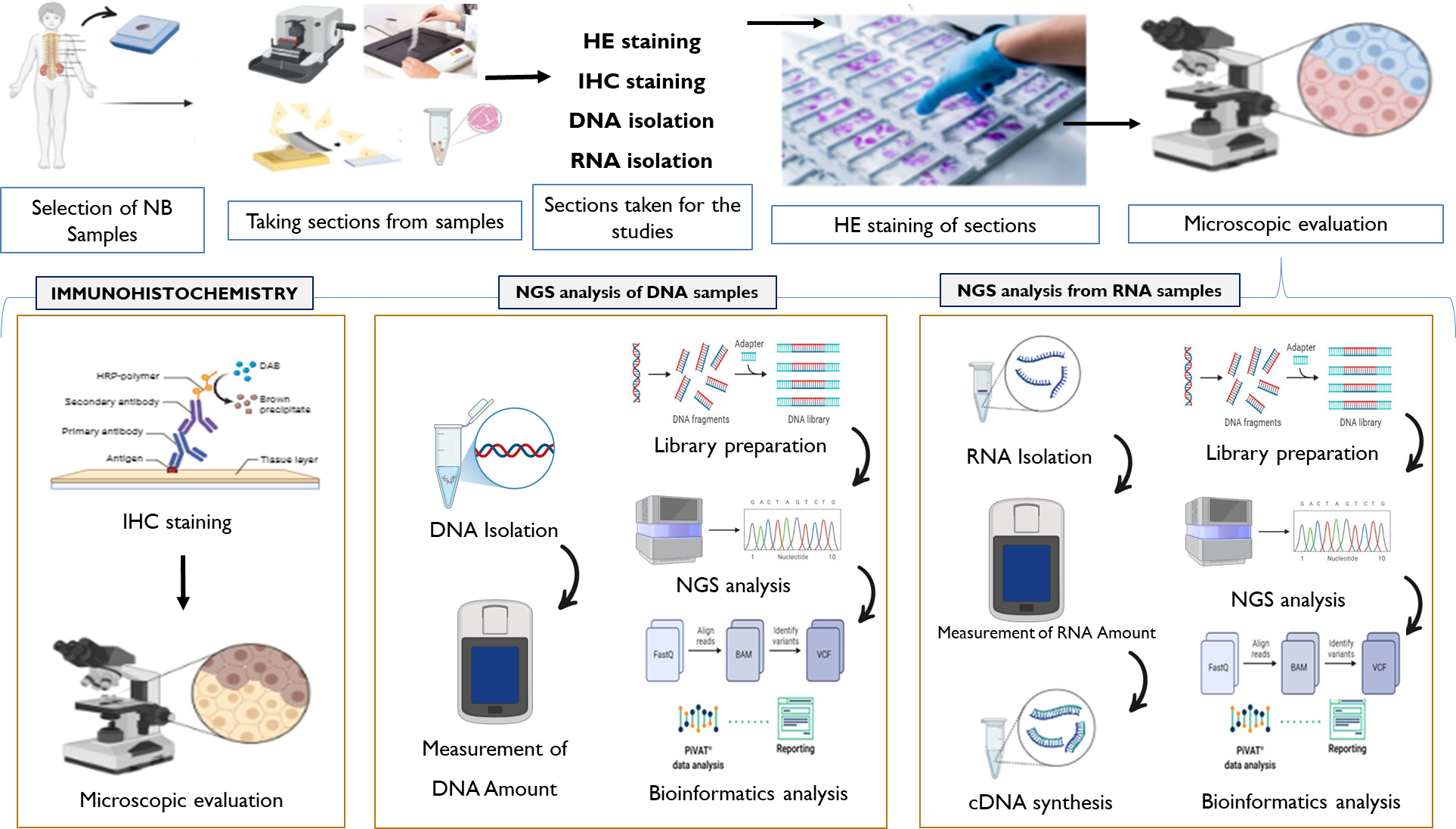
This study aimed to investigate neurotrophic tyrosine kinases at the genomic and protein levels in 173 patients diagnosed with NB, obtained from the Turkish Pediatric Oncology Group (TPOG) Association’s completed TPOG Neuroblastoma 2009 Protocol and the ongoing TPOG Neuroblastoma 2020 Protocol. For this purpose, paraffin block samples from patients diagnosed with NB were used to investigate pan-tyrosine kinase protein expression by immunohistochemistry (IHC); NTRK1, NTRK2, and NTRK3 gene fusions by RNA next generation sequencing (NGS) analysis; and single nucleotide variants (SNVs) in the NTRK1, NTRK2, and NTRK3 genes by DNA NGS analysis.
Demographic characteristics and prognoses of 173 patients diagnosed with neuroblastoma, diagnosed, treated, and followed at our institution, were obtained from patient records. These cases were evaluated according to international neuroblastoma staging, risk classification, and treatment strategies and were evaluated within the scope of the Turkish Pediatric Oncology Group Association neuroblastoma protocol. Slide sections were taken from tumor samples obtained from archived paraffin tissues for immunohistochemistry. For Next generation sequencing (NGS), 100-micrometer sections were taken from paraffin blocks for DNA extraction, placed in two microtubes for point mutation and fusion determination from each case.
Sections were prepared on lysine-coated slides and stained with primary TrkA+B+C (5T6) monoclonal Antibody (BIOSS BSM-52715R) at 1/100 dilution. Pan NTRK was visualized by UltraView Universal DAB Detection Kit (REF 760-500, Ventana Medical Systems, Roche Group, Tucson, AZ, USA) and hematoxylin counterstaining. Samples were analyzed with a positive control and scored nuclear and cytoplasmic expression in percentage [14].
The study was performed in accordance with the ONCO/Reveal™ Solid Tumor Panel guidelines. (REF: HDA-HS-1002-24, LOT: 23PB0318, Pillar Biosciences, Natick, MA, USA) NTRK 1, NTRK2, NTRK3 genes are present in the panel. DNA isolation was performed by the spin column method (Roche® High Pure PCR Template Preparation Kit, version 23, LOT: 37696800, Roche Diagnostics, Indianapolis, IN, USA). DNA amount was measured in the Qubit device using Qubit-HS reagent (Qubit® fluorometer, Invitrogen, Thermo Fisher Scientific, MA, USA). After amplification by PCR, digestion was performed with exonucleases. Magnetic bead-based purification was performed. Indexing was performed by PCR and purified again. Quantification was performed again with Qubit. After library creation and normalization, the cartridge was loaded into the Illumina MiniSeq (Illumina©, Inc., San Diego, CA, USA) device. The data obtained from the device was evaluated with appropriate bioinformatics programs by taking “FASTQ” and the detection of variants was done according to the reference genome [15].
The study was conducted in accordance with the ONCO/Reveal™ Multi-Cancer RNA Fusion v2 Panel (Part No.: HRA-HS-1002-24, İllumina, San Diego, CA, USA) Reference Guide. For the NTRK1 gene: TPM3, TFG, LMNA, SQSTM1, CHTOP, ARHGEF2, NFASC, IRF2BP2, PPL, BCAN, SCYL3, TP53, CD74, MPRIP, and TPR fusions. For the NTRK2 gene: AFAP1, NACC2, BCR, TRIM24, QKI, PAN3, and SQSTM1 fusions. For the NTRK3 gene: ETV6, BTBD1, EML4, SQSTM1, TFG, and RBPMS fusions. RNA isolation was performed using the spin column method (High Pure FFPET RNA Isolation Kit, Roche Diagnostics, Lot No. 89176700, Mannheim, Germany). cDNA Synthesis was performed using cDNA Master Mix and reverse transcription under thermal cycling. RNA concentration was determined using the Qubit RNA BR Assay kit (Life Sciences, Cat. Q10211 and Q10210; Quantitation range: 20–1000 ng). The lid was opened and the reaction was applied to a thermal cycler. After cDNA synthesis was completed, the reaction was diluted with nuclease-free water or low TE. Gene-Specific PCR Transcript Target Amplification, Gene-Specific Primer Annealing, and Purification were performed with AMPure XP beads. PCR indexing and re-purification were performed, and PCR products were quantified with Nanodrop. After indexing and library construction, sequencing was set up and initiated with the Illumina MiniSeq Instrument combined with the PhiX library control according to the “MiniSeq System User Guide” instructions. Fast Q data was acquired [15].
Fast Q data was converted to BAM data. Data were obtained using the Pillar-Biosciences PiVAT (Pillar Variant Analysis Toolkit).
SPSS 29.0 version (IBM Corp., Armonk, NY, USA) statistical analysis program was
used to analyze the data. After performing descriptive statistics and normal
distribution analysis, the relationship between the independent variable of the
NTRK fusion in NB and MYCN, 11Q deletion, age, gender, EFS, and OS was
examined using the Pearson correlation test. Parametric tests were used to
examine the relationship between the groups. The Kaplan–Meier test was used for
survival analyses, and the Log-Rank test was used to correlate survival analyses.
p
This study included 173 patients diagnosed with neuroblastoma (NB). Of these
patients, 54.3% were male and 45.7% were female. The patient ages ranged from 1
to 204 months. The mean patient age was 39.33
| Category | Patient number (N) = 173 | |||
| Min | Max | Mean | ||
| Age (month) | 1.00 | 204.00 | 39.33 | |
| Event free survival | 1 | 131 | 27.97 | |
| Overall survival | 1 | 131 | 19.41 | |
| Sex | 94 (54.3%) Male | 79 (45.7%) Female | ||
| MYCN amplification status | 36.4% Amplified | 63.6% Non-amplified | ||
| 11q deletion status | 33.5% Positive | 62.4% Negative | 4.1% No data | |
| DNA index | 74.0% DI = 1 (Diploid) | 9.8% DI |
16.2% No data | |
| Risk stratification (2020) | (4.6%) Too-low risk | (13.9%) Low risk | (11%) Medium risk | (70.5%) High risk |
| INRG stage | 15.6% L1 stage | 13.9% L2 stage | 64.7% M stage | 5.8% MS stage |
| Pathology | 34.7% good | 65.3% worse | ||
After paraffin block sections of NB samples were taken, the suitability of tumors was determined using hematoxylin & eosin (H&E) staining. Immunohistochemical analysis was performed on 134 tissues identified by HE staining, as shown in Fig. 1. 67.9% were evaluated as NTRK positive and 32.08% as NTRK negative. Nuclear staining was observed in 16 (17.6%) of the positive patients. 75 (82.4%) of Pan-TRK positive NB samples demonstrated cytoplasmic staining.
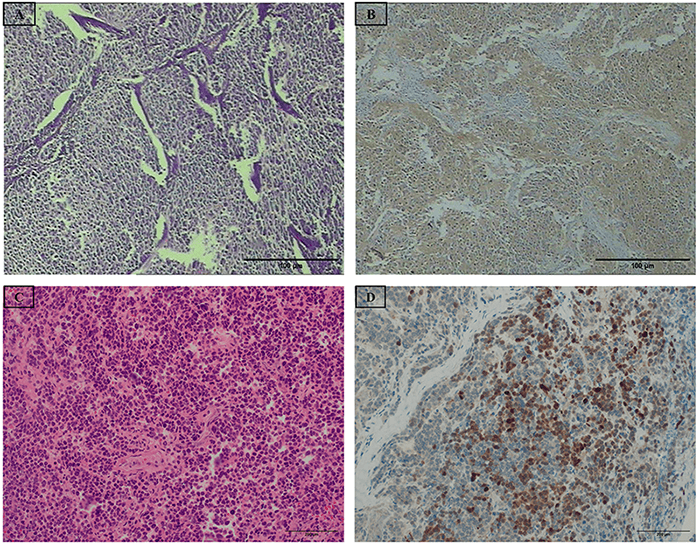 Fig. 1.
Fig. 1.
The microscope images of hematoxylin & eosin (H&E) staining
and immunohistochemical Pan-TRK expression. (A) 4 µm thick NB tumor
slices stained with H&E at 40
The H&E staining of well-differentiated NB tumor tissue is seen in Fig. 1A. Pan-TRK is cytoplasmically expressed in 90% of NB tumor tissues in Fig. 1B. Poorly differentiated NB tumor tissue is stained with H&E (Fig. 1C). Pan-TRK is expressed in 70% of tumor tissues. NTRK expression is mainly nuclear or cytoplasmic (Fig. 1D).
Of the 115 patients who underwent SNV analysis, 20/115 (17.4%) had one or more clinically significant mutations in NTRK1, while 9/115 (7.83%) had clinically significant mutations in NTRK2 and 9/115 (7.83%) in NTRK3. Among the patients with SNV mutations, NTRK1 and NTRK2 were observed together in 2 patients, NTRK1 and NTRK3 were observed in 2 patients, and NTRK3 and NTRK2 were observed in 2 patients. Only NTRK1, NTRK2, and NTRK3 mutations were observed together in 3 patients. Mutation types observed in SNV analysis of patient tissues were categorized as synonymous, missense, stop-gained, and frameshift mutations. Missense, stop-gained, and frameshift mutations that were found as clinically significant in PIVAT program were chosen. According to SNV analysis, all of the single nucleotide variants detected in the NTRK1, NTRK2 and NTRK3 genes were seen in the tyrosine kinase domain of NTRK1, NTRK2 and NTRK3, as seen in Fig. 2. The UniProt database (https://www.uniprot.org/uniprotkb?query=NTRK1) was used to determine the domain of the NTRK protein in which the detected NTRK somatic mutations were located. The data found are visualized in the Fig. 2.
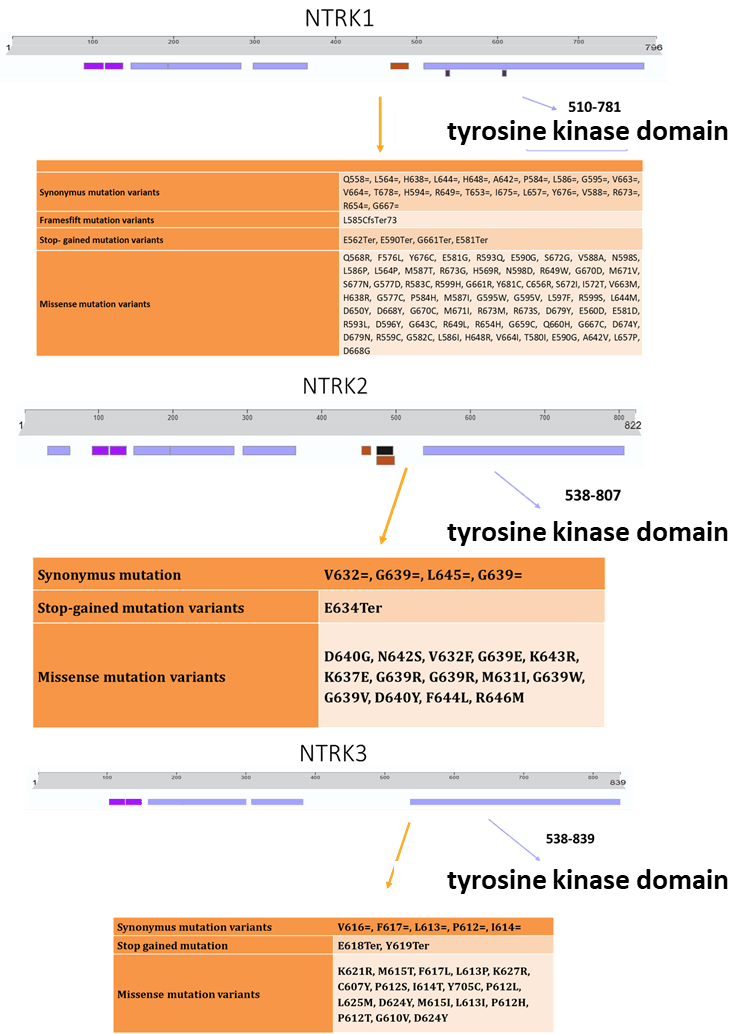 Fig. 2.
Fig. 2.
Schematic representation of NTRK 1, 2 and 3 protein structures. Synonymous, missense, frame-shift and stop-gained mutations were observed in the NTRK1, 2 and 3 tyrosine kinase domains. NTRK1, 2 and 3, Neutrophic tyrosine kinase 1, 2 and 3.
NGS RNA fusion analysis was performed on 103 of 173 patients. 4 /103 (3.9%) patients had NTRK fusions. Whereas NTRK1 fusions were detected in 2 patients, 2 patients had NTRK3 fusions. Of the four fusions observed, the first patient had TFG(e4):NTRK1(e9), the second had TPR(e6):NTRK1(e5), the third patient had EML4(e14):NTRK3(e6), and the fourth patient had both EML4(e14):NTRK3(e6) and TFG(e4):NTRK3(e6). A total of five fusions were detected in four different patients. Except for the example with a double fusion, all fusions were observed in the metastatic stage (Table 2). Immunohistochemical staining types were evaluated as diffuse positive in the case with TFG(e4):NTRK1(e9) fusion, 40% cytoplasmic positive in the case with TPR(e6):NTRK1(e5) fusion, 50% cytoplasmic positive in the case with EML4(e14):NTRK3(e6) fusion, and 10% cytoplasmic positive in the case with EML4(e14):NTRK3(e6), TFG(e4):NTRK3(e6) fusions.
| NTRK | Fusion status | NTRK IHC result | Stage | Risk stratification |
| NTRK1 | TFG(e4):NTRK1(e9) | Positive | M | High risk |
| NTRK1 | TPR(e6):NTRK1(e5) | Positive | M | High risk |
| NTRK2 | - | - | - | - |
| NTRK3 | EML4(e14):NTRK3(e6) | Positive | M | High risk |
| NTRK3 | EML4(e14):NTRK3(e6), | Positive | L1 | Low risk |
| TFG(e4):NTRK3(e6) | Positive |
The normal distribution of patient data was determined using the
Kolmogorov-Smirnov Normality test. The data were found to be normally
distributed, and parametric tests were performed. The relationship between NTRK
IHC results and other parameters was investigated using the ordinal logistic
regression test and Pearson’s chi-square tests. Ordinal logistic regression
analysis indicates that NTRK IHC positivity was significantly associated with
predicting increasing neuroblastoma risk classes (
To further evaluate the relationship between NTRK IHC status and INRG stage, we
also performed ordinal logistic regression using INRG staging (L1–L2–M–MS) as
ordinal input. The model showed a significantly better fit compared to the
intercept-only model (
The association between NTRK immunohistochemistry and NTRK SNV status was
assessed using both Pearson’s chi-square test (
A significant relationship was observed between NTRK IHC positivity and the
presence of NTRK1 mutations (Pearson
No statistically significant association was observed between NTRK2
mutations and NTRK IHC positivity (Pearson
There was no statistically significant association observed between
NTRK3 mutations and NTRK IHC positivity (Pearson
No significant association was observed between NTRK fusion status and NTRK IHC
expression (Pearson
When we examined the effects of NTRK protein expression positivity on EFS and OS times of NB patients, we used Kaplan-Meier survival curve with Log-Rank test as shown in Fig. 3. As a result, EFS and OS were longer in NB patients with negative NTRK expression than in NTRK-positive patients. Although NTRK positivity had an effect on EFS and OS, this was not statistically significant (EFS p = 0.153, OS p = 0.368).
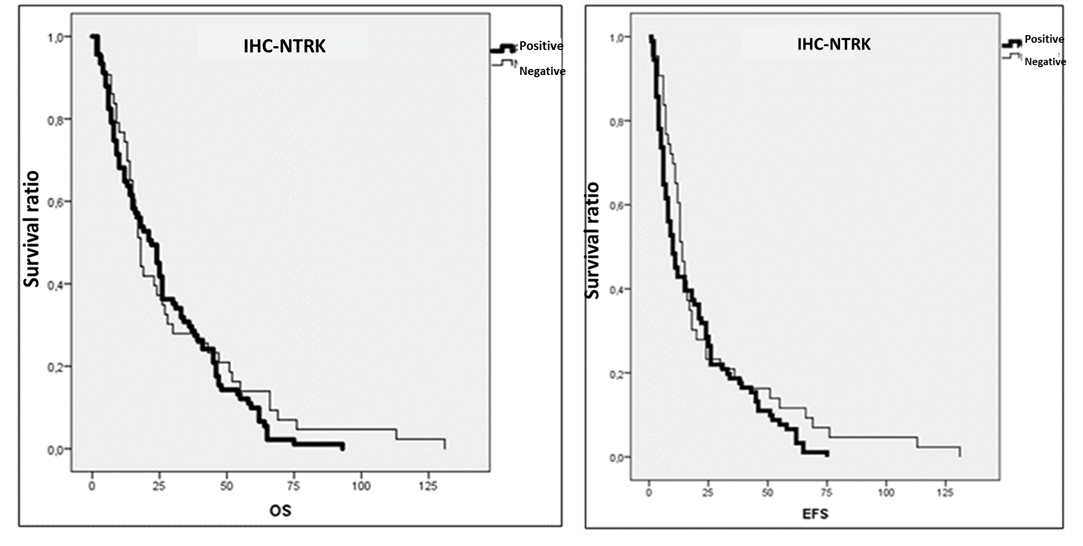 Fig. 3.
Fig. 3.
The Kaplan-Meier survival analysis of neuroblastoma patients in
respect to the presence of NTRK status. OS and EFS times (month) in Pan-TRK
positive and negative NB pateints were analyzed by Log-rank test. p
As shown in Fig. 4, NTRK SNV demonstrated clinically significant mutations. When we investigated whether the presence of NTRK SNV in the patient affected the patient’s EFS and OS duration, the EFS and OS survival times of patients with NTRK SNV were found to be shorter. However, this finding was not found to be statistically significant in the Log-rank test (OS p = 0.904, EFS p = 0.230).
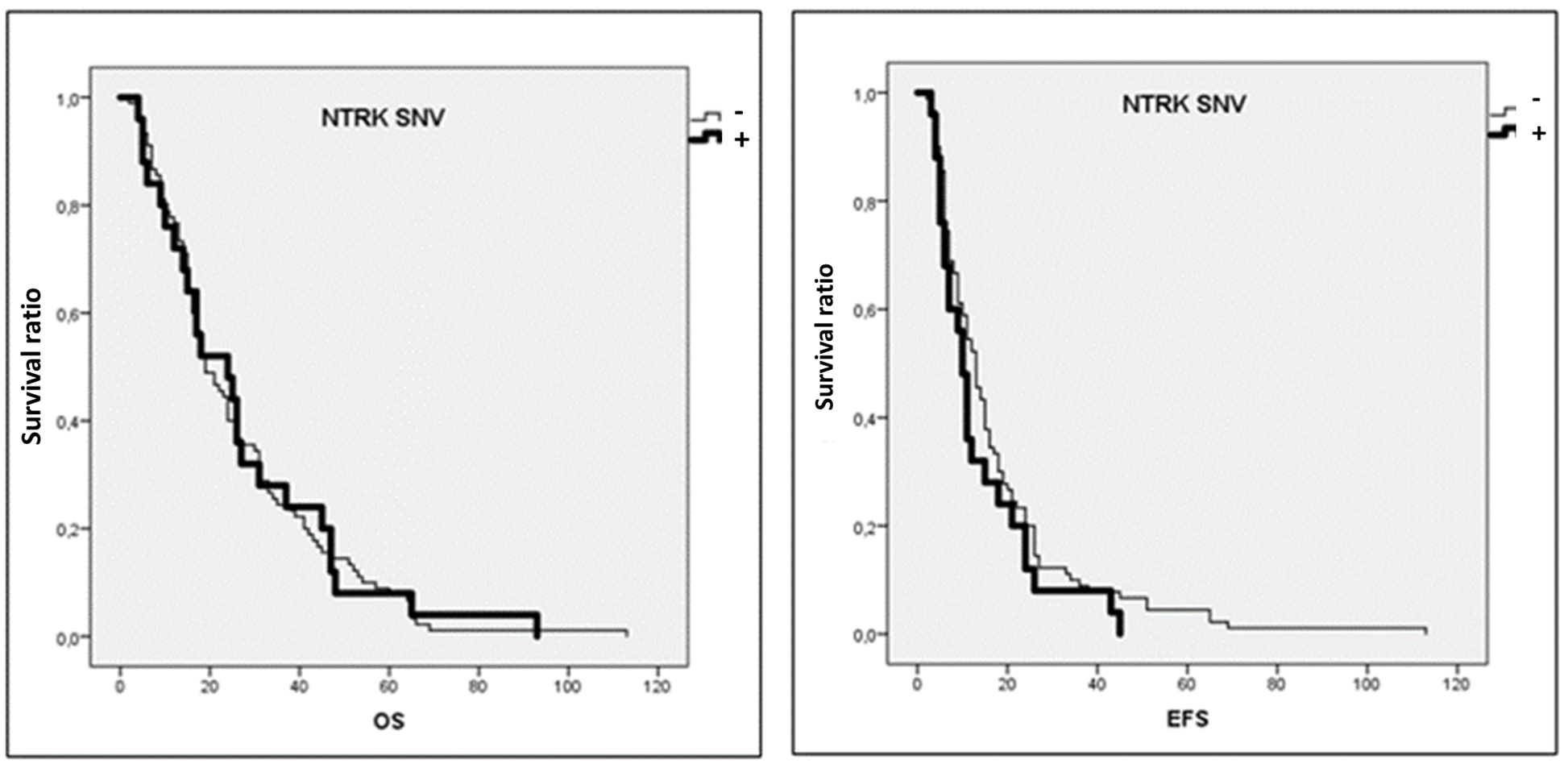 Fig. 4.
Fig. 4.
The Kaplan-Meier survival analysis of neuroblastoma patients in
respect to the presence of SNV. OS and EFS times (month) in NTRK-SNV positive
and negative NB pateints were analyzed by Log-rank test. p
When we examined the risk classification groups, we observed that EFS and OS times were shorter in the very low-risk group, while EFS and OS times were longer in the low-risk group (Fig. 5). However, the Log-rank test showed that this finding was not statistically significant (EFS p = 0.079, OS p = 0.132).
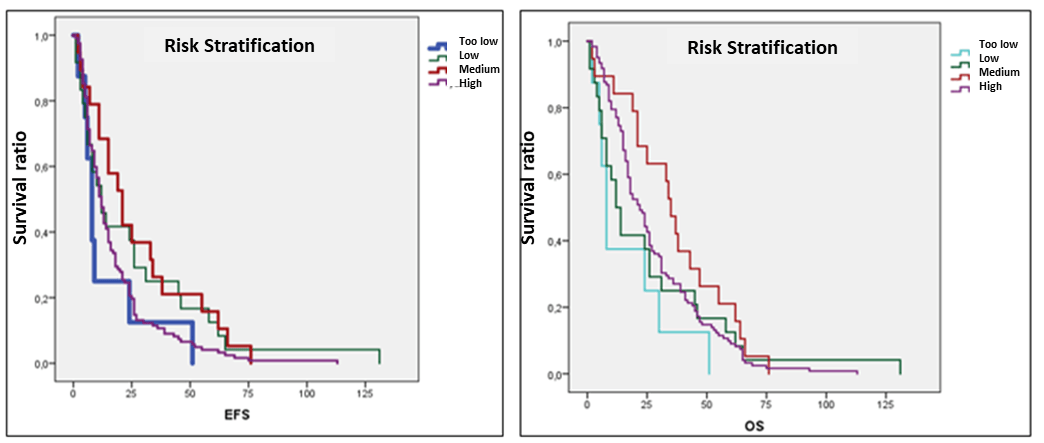 Fig. 5.
Fig. 5.
The Kaplan-Meier survival analysis in respect to risk
stratification of NB patients. OS and EFS times (months) were analyzed by
Log-rank test. p
In the INRG staging system, EFS time was shorter in the metastatic stage and OS time was shorter in the L2 stage. EFS and OS times were longer in the L1 stage than in the other stages (Fig. 6). In this case, Log-rank analysis was found to be statistically significant in EFS periods (EFS p = 0.044, OS p = 0.476).
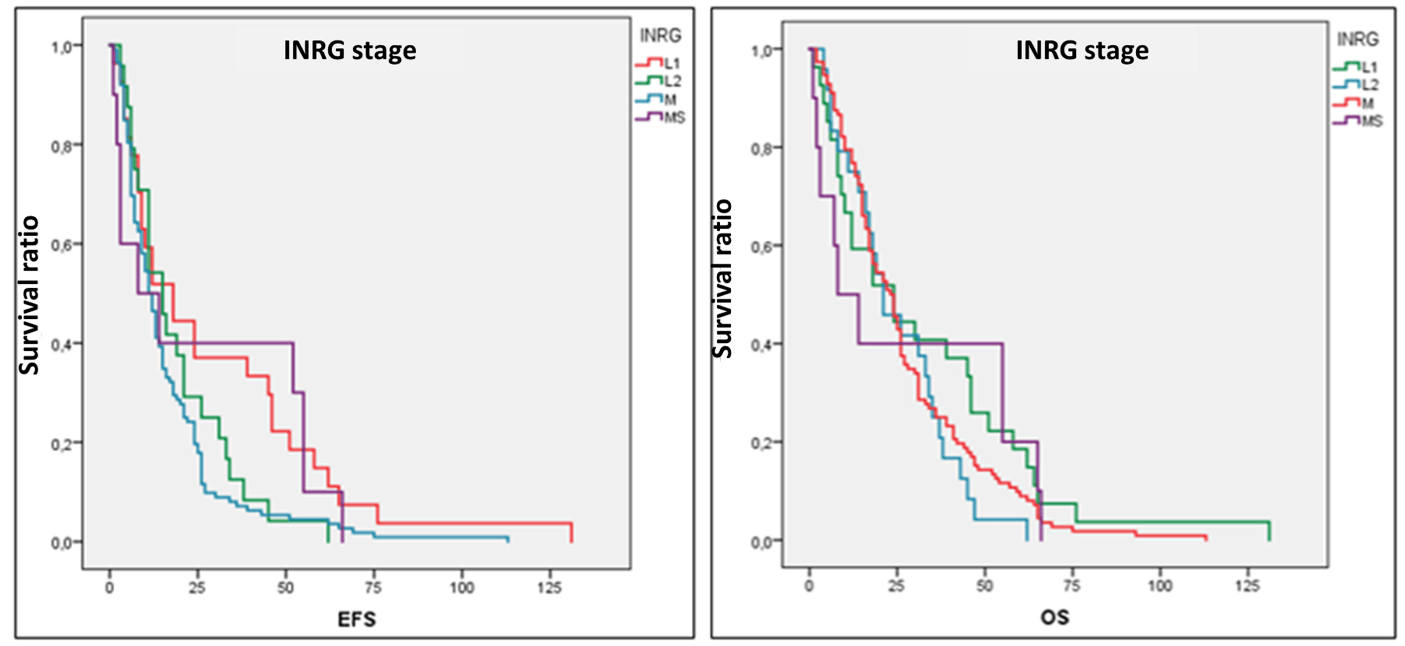 Fig. 6.
Fig. 6.
The Kaplan-Meier survival analysis in respect to INRG stage of
NB patients. OS and EFS times (months) were analyzed by Log-rank test.
p
To examine whether IHC-based NTRK expression is an independent prognostic
factor, multivariable Cox proportional hazards regression analyses were applied
for both event-free survival (EFS) and overall survival (OS), adjusting for
clinical and biological risk factors, including MYCN amplification, 11q
deletion, DNA ploidy, risk stratification and INRG stage. In a multivariable Cox
model for EFS, including IHC-based NTRK expression demonstrated a trend toward
improved EFS (HR = 0.574), although this was not statistically significant
(p = 0.074). Risk stratification remained an independent prognostic
factor for EFS. In the multivariate Cox analysis for OS, IHC-based NTRK
expression was independent of OS status (death/alive), whereas 11q deletion was
found to be an independent negative prognostic factor (HR = 3.704, p =
0.038). Cox multivariate analysis with NTRK SNV and clinical factors
showed that NTRK SNVs have a non-significant trend toward poorer
event-free survival (HR = 1.77, p = 0.059), whereas there was no
association between NTRK SNVs and overall survival (HR
This study investigated the distribution and clinical significance of NTRKs in
173 NB cases using point mutations in the NTRK1, NTRK2, and
NTRK3 genes from DNA samples, fusion analyses from RNA samples, and IHC
expression rates. The study results revealed a high percentage of
immunohistochemical expression of NTRKs (67.9%) and NTRK point mutations
(78.26%) in NB, while the percentage of NTRK fusions (3.88%) was low.
NTRK missense mutations were commonly seen in tyrosine kinase domains of
NTRKs. A study has determined whether the c.1810C
In our study, NTRK mutations were found at a high frequency in neuroblastoma patients. According to the literature, NTRK mutations are rare and, while most are polymorphisms, are rarely seen in cancers. Furthermore, studies have reported that NTRK point mutations (especially found in tyrosine kinase domain) have oncogenic potential and can cause TRK inhibitor resistance [17, 18]. NTRK1 L564H, V573M and G667C mutations or NTRK3 F617L, G623E, G623R and G696A were detected by NGS and resistant to Cabozantinib, Larotrectinib and Entrectinib that are TRK inhibitors [17, 18, 19]. Joshi et al. [20] identified somatic NTRK2 and NTRK3 mutations in hematological neoplasms and functionally demonstrated to be transforming/oncogenic that NTRK2 and NTRK3 point mutations. NTRK1 p.G595R and p.G667C mutations have been associated with entrectinib/larotrectinib resistance in tumors with NTRK fusions (e.g., colorectal cancer). These mutations were generally identified as resistance mutations located within the ATP-binding pocket of the TRK fusion protein [21]. In our study, we found NTRK1 p.G667C and NTRK3 F617L mutations.
NTRK gene fusions were first identified in a colorectal adenocarcinoma cell line in 1982 [22]. The concept of tumor-agnostic markers refers to markers used as therapeutic targets in tumors with specific genetic or molecular characteristics (e.g., a specific biomarker or mutation), regardless of cancer type. This concept represents modern oncological approaches, where cancer treatment is based on the molecular profile of the tumor rather than its location [23]. The approval of larotrectinib as a tumor-agnostic treatment by the FDA in 2018 and by the European Medicines Agency (EMA) in 2019 has provided access to treatment for patients with NTRK gene fusion regardless of age and tumor type [9, 24, 25].
In our cohort, NTRK fusions were identified in 4 of 103 tested patients (3.9%), comprising 2 patients having NTRK1 and 2 patients having NTRK3 fusions. This detection ratio is concordant with the low prevalence of NTRK alterations reported across solid tumors, yet it is notably higher than the 8.7% fusion prevalence observed by Mohamed et al. [26] in CNS tumors when performing a combined NGS and Pan-TRK IHC workflow. Importantly, while Mohamed et al. [26] demonstrated that Pan-TRK expression lacked specificity—detecting fusion–negative tumors in 82% of Pan-TRK–positive CNS cases—our study relied exclusively on RNA-based NGS for fusion detection, thereby avoiding false-positive immunoreactivity and ensuring high analytical accuracy. The absence of NTRK2 fusions in our cohort also contrasts with their study, where both confirmed fusions were NTRK2-driven, underscoring potential biological differences between tumor types and patient populations [26]. Collectively, these findings highlight the substantial variability of NTRK fusion across tumor groups and strengthen RNA-based NGS as a more trusted diagnostic method compared with IHC, particularly in settings where physiologic TRK expression or tumor heterogeneity may confound IHC interpretation.
In a study by Cocco et al. [7], TRKA and TRKC expression in NB patients was generally a good prognostic indicator, while TRKB was primarily expressed in high-grade tumors that also harbor MYCN amplification and was associated with a poor prognosis. This study used a pan-TRK antibody containing all three proteins. In the study by Vingiani et al. [14], they detected NTRK fusion in only 11 of 30 (37%) cases with positive pan-TRK IHC and in 1 of 87 (1.1%) cases with negative pan-TRK IHC. This study included a cohort of 124 cancer patients (carcinomas, 93 cases; soft tissue sarcomas, 19; primary central nervous system tumors, 10; and neuroblastomas, only 2 cases and negative for fusion). Based on this information, IHC sensitivity was calculated as 91.7% and specificity as 81.9% [14]. However, when we examined the positive predictive value, it was low at 36.7%, while the negative predictive value was high at 98.8%. This indicates that there are many false-positive results. When we considered IHC results according to histological types, higher concordance was seen in carcinomas (94.2%), while the concordance rate was low in nervous system tumors and neuroblastomas (18.2%). It has been reported that IHC expression patterns of the detected TPR-NTRK1 fusion showed cytoplasmic and membranous staining patterns [14]. Compared to these data, in our study, of all cases showing positive IHC, only 44 had fusion studies and 46 had point mutation studies. Percentage-wise, fusions were observed in 6.81% of cases with immunohistochemical expression. When point mutations were evaluated, clinically significant mutations were detected in 34.78% of positive cases, while no mutations were detected in 65.21%. The high NTRK rate in our study was associated with the fact that a large proportion of the patients included were advanced-stage, relapsed-refractory patients.
In another study, Zhao et al. [27] investigated the frequency of NTRK fusions in pediatric tumors. In a cohort of 1347 pediatric patients, NTRK fusions were detected in 2.22% of all tumors and 3.08% of solid tumors. NTRK1 and NTRK3 fusions were commonly observed in papillary thyroid carcinomas, while NTRK2 fusions were more common in central nervous system tumors, and these tumors were mostly low-grade gliomas. In soft tissue tumors, fusions such as ETV6-NTRK3 were found in rare tumors such as spindle cell tumors and infantile fibrosarcoma. TRK inhibitors have emerged as an effective method to support surgery in these types of tumors. No NTRK fusion was detected in any of the 79 NB cases examined in the study [27].
In Cox model analysis, NTRK positivity was not independently associated with overall survival, but it showed a non-significant trend toward improved event-free survival. NTRK single-nucleotide variants were not independently associated with either event-free or overall survival, although a trend toward poorer event-free survival that was not significant. The lack of statistical significance may result from the low frequency of NTRK expression and the limited number of events.
Light et al.’s study [28] evaluated the impact of NTRK gene family
expression levels on the clinical features and outcomes of NB patients. 814 NB
patient samples were analyzed using Quantitative Real-Time Reverse Transcriptase
PCR (qRT-PCR). NTRK1 expression was associated with all established risk
factors; Statistically significant differences were found in patients younger
than 18 months, with low stage, MYCN amplification negative, hyperploidy, and
good histology. In patients with high NTRK1 expression, 5-year EFS and
OS rates were significantly higher than in patients with low expression levels
(p
As suggested by Märkl et al. [29], in cases with a high NTRK splicing rate, such as congenital fibrosarcoma, FISH, RT-PCR, and NGS are recommended for direct or positive results after NTRK IHC. In cases with low frequency, direct or panTRK-IHC tests were recommended if they included multiple gene assessments, and FISH and NGS were recommended for positive results. For negative results, no other analyses were required [29].
Tyrosine kinases are tumor-agnostic markers, and targeted therapies are available for them. Detecting the presence of NTRK fusions in cancers is crucial for initiating treatment. However, the importance of point mutations, gain-of-function mutations, and missense mutations for the application of NTRK-targeted therapy in NB has not been fully elucidated. In this study, IHC staining of NTRK showed NTRK expression in the majority of NB patients. Therefore, it was concluded that it cannot be a leading biomarker for fusion.
In this study, some samples were not suitable for IHC or NGS analyses due to lack of tissue in the paraffin block, inadequate tissue follow-up, or limited sample size. Furthermore, budget constraints precluded the application of NGS to all samples. However, the relatively large sample size increased statistical power. Tumor mutational burden assessment or broad copy-number analysis are the limitations of our study in terms of NGS panel that we used in this study. One of the limitations of this study is that the detected SNVs were previously interpreted and classified in clinical databases and did not include functional validation. The significant heterogeneity of neuroblastomas is another limitation that must be considered in the interpretation of the findings.
In conclusion, evaluation for TRK inhibition is needed in all cases of NB, a tumor of neural origin. NTRK fusions and NTRK point mutations or other SNVs should be both evaluated to determine possible resistance to NTRK inhibitors. Our data supported that Pan-NTRK immunohistochemistry is not a good biomarker for the selection of further NGS studies. In this study, no concordance was found with nuclear immunohistochemical NTRK expression in the four cases in which fusions were detected.
NTRK fusions are rare in NB, as confirmed in our study and the literature. As an agnostic therapeutic target, RNA fusion and multigene DNA panels containing NTRK genes should be evaluated using NGS in relapsed, refractory, high-risk, poor clinical conditions, and chemotherapy-resistant NB cases.
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
SA and TÇA designed the study. DK, NI, SMÖ, AE, and ÖEG collected the patient samples and data. NI, SMÖ, AE, and ÖEG conducted the research and laboratory experiments. SA, TÇA, and SMÖ performed the statistical analysis of the data. All authors participated in the writing and editing of the manuscript. All authors read and approved the final version of the manuscript. All authors participate in the study, taking responsibility for the adequacy of the content and contributing to the accurate and complete completion of the work.
Ethical Approval was taken from Dokuz Eylul University Non-Interventional Research Ethics Committee on 07.05.2023 with decision number 2023/22-14. Approval was obtained by having the patients’ parents sign Informed Consent forms. The study was carried out in accordance with the guidelines of the Declaration of Helsinki.
We gratefully acknowledge the Turkish Pediatric Oncology Group – Neuroblastoma team.
This research was supported by the Turkish Pediatric Oncology Group Association 2024 Research Projects Support Program for the immunohistochemical step. This study was also partially supported by Dokuz Eylül University Scientific Research Council for the NGS analysis step (Project no: TSA-2023-3007).
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/FBS46963.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.