

 , Johanna de Almeida Mello 1,2, Anja Declercq 1,3
, Johanna de Almeida Mello 1,2, Anja Declercq 1,31 LUCAS – Centre for Care Research & Consultancy KU Leuven, 3000 Leuven, Belgium
2 Population studies Oral health KU Leuven, 3000 Leuven, Belgium
3 CeSO - Centre for Sociological Research KU Leuven, 3000 Leuven, Belgium
Abstract
Dementia affects not only the patients, but also the caregivers. Timely targeted supporting for informal caregivers of people with dementia can improve their health and life quality, as well as contribute to sustainable healthcare. However, which interventions could efficiently support them and why still remains unclear. This systematic review aims to close this gap by critically assessing the current state of randomized controlled evidence concerning informal caregivers of older people with early dementia. We searched the electronic databases PubMed, CINAHL, Embase, Cochrane and Web of Science and assessed the methodological quality of the selected studies using the validated PEDro scale. A total of 2067 studies were identified in the initial searching, and 29 randomized controlled studies were finally selected based on the rigorous inclusion and exclusion criteria. Through completely assessing the methodological quality of studies, and the essentials and effectiveness of the 22 different types of interventions, we identified which interventions were effective and why. Timely targeted interventions for this caregiver group remains scarce. Furthermore, we highlight that there is a lack of systematic caregiver needs assessments prior to or when delivering the interventions.
Keywords
- Review
- Informal caregivers
- Aged
- Psychosocial interventions
- Early dementia
- Cognitive decline
Cognitive decline and dementia affect not only older people but also their informal caregivers [1, 2, 3]. In the face of growing numbers of people living with dementia, ensuring that those who support them can remain healthy is a policy priority [4, 5]. Worldwide, around 50 million people have dementia, and there are nearly 10 million new cases every year [6]. People with dementia are mostly cared for by their family members, friends or neighbors, who are referred to as informal caregivers. The input from informal caregivers is a complex area, but regardless of how the input is calculated, it is estimated by Alzheimer’s Disease International that the annual global number of informal care hours provided to people with dementia living at home was about 82 billion hours in 2015. This is equivalent to 2089 hours per year or 6 hours per day. This figure was equal to the input of more than 40 million full time workers in 2015, a figure that will increase to 65 million full time workers by 2030. This contribution is substantial for the health care system [7]. While the contribution is important, informal caregivers are often exposed to emotional strain, relationship deprivation, family conflicts and financial burden, which can impact their health and life quality [8]. Compared to other informal caregivers, those who care for older people with cognitive decline experience an even greater burden. This greater burden includes higher stress [9], increasing isolation and burden of care [10], higher levels of depression due to severe psychiatric and behavioral problems of the cared person [11, 12], lower quality of life [13], and poorer health [14]. A growing body of evidence points out that it is essential to develop effective interventions for this type of informal caregivers [15, 16, 17, 18, 19, 20].
Informal caregivers of older people with cognitive decline bear increasing responsibility and burden with the progress of the disease. Even a newly acquired role as a caregiver affects other roles and often results in additional burden and emotional strain. This case will become worse especially when a caregiver has no prior experience in caregiving [8]. Moreover, family members often need to transition their relationship with the parent or spouse from that of a family member to that of a proactive caregiver. Early adjustment into this transition is needed because unprepared informal caregivers experienced frustration, resentment, grief, as well as relational deprivation [21].
Offering timely interventions for informal caregivers of people with dementia can help them better adapt to the transition, feel more competent to care and experience less psychological problems [22]. Timely supporting informal caregivers at risk of adverse outcomes showed an added value to the health care system [23]. Furthermore, this timely support can contribute to the caregiver’s resilience to stress [24]. At this point, timely targeted supporting for informal caregivers of people with dementia can improve their health and life quality, as well as contribute to sustainable healthcare.
However, much remains unknown about how to best support informal caregivers of older people with early dementia. Most interventions developed focus on the persons who are affected by early dementia, but not on the informal caregivers. These interventions aim to improve the patients’ physical and cognitive functions, quality of life, and the skills to perform activities of daily living [25]. A recent meta-review recommended that interventions should be developed to meet informal caregivers’ changing needs in the course of dementia [26]. Scientific evidence shows that appropriate information and professional service for informal caregivers of people with early dementia are still lacking [27, 28]. Moreover, most systematic reviews focused on informal caregivers of people with moderate or advanced stages of dementia. These reviews assessed the effectiveness of interventions [29, 30, 31, 32, 33] concerning informal caregivers’ outcomes, such as health-related quality of life [34], care burden, depression, disruptions in health and social support [35], and cost-effectiveness of the interventions [36], and the effects of content of the interventions [37]. The current state of randomized controlled evidence, particularly concerning informal caregivers of older people with early dementia, has not yet been systematically assessed. We aim to close this gap and explore which psychosocial interventions exist for informal caregivers of older people with early dementia. We also addressed the following questions: (1) What components of psychosocial interventions are effective for informal caregivers of older people with early dementia? (2) What theories underpin these interventions? (3) What caregivers’ needs were assessed in these interventions?
A systematic review protocol was developed to identify and assess the intervention studies for informal caregivers of older people with early dementia. The review followed the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement [38]. Details of the protocol can be found in Appendix.
We searched electronic databases PubMed, CINAHL, Embase, Cochrane and Web of Science using search terms in accordance with the following concepts: psychosocial interventions, evaluation, informal caregivers, older persons, dementia and cognitive problems. We did not impose data limits, and this review reflects the latest search through July 2021. Two independent reviewers constructed a comprehensive list of Medical Subject Headings (MeSH), which was designed for 5 explicit categories: (1) interventions; (2) evaluation; (3) informal caregivers; (4) older persons; and (5) dementia (Table 1). Terms were coupled with relevant MeSH terms and were truncated as appropriate. We hand-searched references in reviews and published literature to include more potential studies that could have been missed in the database searching.
| Search category | MeSH terms |
| Interventions | Counseling, education, support, problem solving, cognitive behavioral therapy, coping skills, art, singing, museums, music |
| Evaluation | Program evaluation, treatment outcome, evaluation study, health impact assessment |
| Informal caregivers | Family caregivers, spouse caregivers |
| Older persons | Aged |
| Dementia | Dementia, cognitive decline, mild cognitive impairment, memory disorders |
| * For a detailed table with MeSH terms, keywords and explosions of the search strategy, please contact the authors. | |
After removing duplicates, abstracts were identified upon the initial search, and two independent raters selected abstracts for full review based on inclusion/exclusion criteria. After each rater independently reviewed the abstracts, findings were reviewed to find a consensus producing a final list of studies for full-text examination. Full-text examination was also performed by the two raters independently.
All papers selected for final inclusion met the following criteria.
• Only peer-reviewed journal articles written in English were included.
• Only randomized controlled trial designs were included.
• Interventions had to specifically focus on informal caregivers of people with early dementia delivered in the community setting. Studies were also included when people with early dementia were part of their care population, even when they also included more severe cases.
• Informal caregivers were viewed as those who are primarily responsible for the care and wellbeing of care recipients. They may be spouses, children or other family members, either or not living with the care recipient.
• Studies included efficacy evaluation of the interventions for informal caregivers intended to enhance their health and life quality (possibly also of the care recipient).
• The intervention must primarily focus on informal caregivers. Interventions intended primarily for care recipients where the caregivers assisted with implementation were excluded.
•Studies were also excluded if the caregivers were professionals, and the care recipients were institutionalized.
• Descriptive studies such as protocol trials were excluded.
• Studies only focusing on older people with moderate or advanced stages of dementia were not the target of our review and were also excluded.
Two independent raters read the full text of each study included in the review, and extracted key content of the studies using an ad-hoc data collection form to record the following information: (1) author, year and country, (2) theoretical underpinnings, (3) caregiver needs assessment, (4) sample, (5) people delivering the intervention, (6) intervention duration, (7) intervention elements, (8) main outcomes of care recipients, (9) main outcomes of caregivers, (10) main findings, (11) study limitations. Studies were categorized based on the composing elements of an intervention (e.g., training, counseling) to facilitate synthesis of the studies.
Two independent raters selected the studies and rated them independently for
their quality using a modified 11-item version of the PEDro scale [39, 40].
Differences in scoring were discussed and resolved collaboratively. According to
the rating rule of PEDro scale, criteria 1 (i.e., Specification of eligibility
criteria) is not included in the final score. Hence the PEDro scale consists of
10 quality ratings, each receiving either a yes (value 1) or no (value 0) score,
which is based on the Delphi list developed by Verhagen et al. [41]
PEDro score 9–10 is categorized as of excellent quality, PEDro score 6–8 is
categorized as good quality, PEDro score 4–5 is categorized as of fair quality,
and PEDro score
As illustrated in Fig. 1, a total of 2067 studies were finally identified through online databases and hand-searching. A total of 343 duplicates were removed. After full-text eligibility screening for 156 records, 29 randomized controlled studies were included based on rigorous inclusion and exclusion criteria. Raters then performed data extraction and quality of assessment on the included studies.
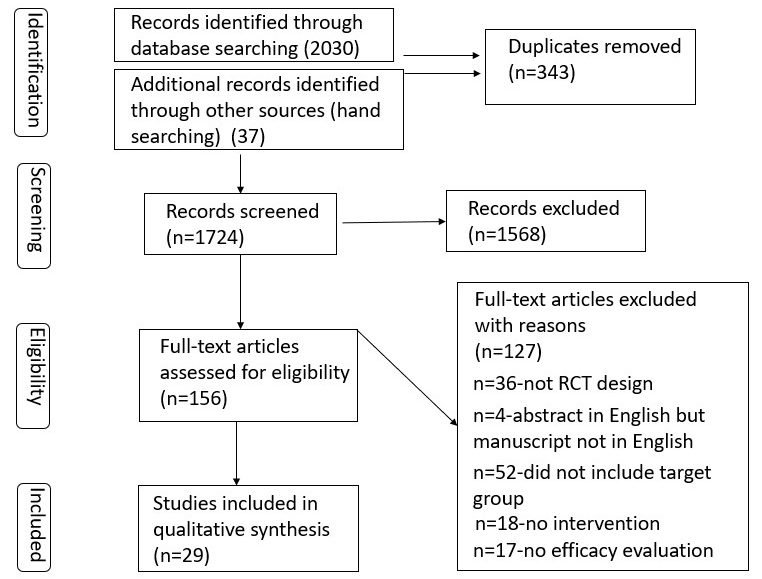 Fig. 1.
Fig. 1.Prisma flow diagram.
The methodological quality of the included studies ranged from good to excellent (Table 2). Amongst the 29 studies [42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70], 9 studies [43, 53, 54, 55, 56, 57, 59, 60, 61] were categorized as of excellent quality (PEDro score = 9–10). As included studies were trials examining psychosocial interventions, subject and therapist blinding were unattainable. Moreover, because of the nature of the population studied, ‘concealed allocation’ and ‘assessor blinding’ were poorly met. The scores of ‘intention to treat analysis’ and of ‘over 85% follow-up of at least one key outcome’ were relatively poor. However, all included studies appeared to have good methodological rigor including specification of eligibility criteria, loss to follow-up information provided, point estimates and measures of variability of at least one key outcome and use of a treatment fidelity protocol.
| PEDro scale criteria | Frequency n (%) |
| 1. Specification of eligibility criteria (standard, this item is excluded in the final score) | 29 (100) |
| 2. Random allocation | 29 (100) |
| 3. Concealed allocation | 13 (45) |
| 4. Assessor blinding | 13 (45) |
| 5. Prognostic similarity at baseline | 29 (100) |
| 6. Loss to follow-up information provided | 29 (100) |
| 7. Over 85% follow-up of at least one key outcome | 16 (55) |
| 8. Between-group statistical comparison of at least one key outcome | 29 (100) |
| 9. Point estimates and measures of variability of at least one key outcome | 29 (100) |
| 10. Intention to treat analysis | 18 (62) |
| 11. Intervention fidelity protocol available | 29 (100) |
The intervention components, intervention delivery and duration, as well as sample characteristics varied in a total of 22 different types of interventions described in 29 studies (see Tables 3,4, Ref. [42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70]). Most studies were performed in the USA (14 studies), and others were performed in the UK (5 studies), China (2 studies), Japan (1 study), India (1 study), Germany (1 study), Netherlands (3 studies), Norway (1 study), Denmark, Poland and Spain (1 study). In addition, the years of these published studies varied from 2003 to 2021. In most studies, informal caregivers of relatives with early and later stages of dementia are the sample participants, except for 5 studies [49, 50, 58, 62, 66] where the participants are solely informal caregivers of older people with early dementia. Four studies evaluated a single-element intervention (i.e., education, training) [42, 43, 44, 45], and the remaining 25 studies evaluated a multi-component intervention (i.e., support group + training) [46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70]. The interventions are delivered by a wide array of individuals (e.g., nurse, counselor, etc.), and two internet-based interventions are carried out by participants themselves [42, 47]. In two studies [51, 52], the intervention was carried out by an interdisciplinary team, including a home care advisor, lay counselor, nurse, psychiatrist and coordinator. Most interventions were delivered by therapists or nurses [44, 45, 46, 48, 53, 54, 55, 56, 57, 58, 63, 64, 69], and only interventionists of the NYU Caregiver intervention (NYUCI) and Resources for Enhancing Alzheimer’s Caregiver Health (REACH) were officially certified [53, 54, 55, 56, 57]. Of the 29 studies, only 5 studies specifically targeted informal caregivers of people with early dementia [49, 50, 58, 62, 66]. The remaining 25 studies evaluated the interventions for informal caregivers of people with early and later stages of dementia.
| Author, year, country | Sample | Theory basis | Needs assessment | People delivering intervention | Duration |
| Kajiyama, Bruno, et al. 2013 USA [42] | Caregivers of relatives with early and later stages of dementia | Not reported | No | No | 3 months |
| Charlesworth, Georgina, et al. 2008 UK [43] | Caregivers of relatives with early and later stages of dementia | Not reported | No | Befriending volunteers | 6-, 15-, 24-month follow-up |
| Gonyea, Judith G. et al. 2006 USA [44] | Caregivers of relatives with early or moderate dementia | Cognitive behavioral group intervention | No | Therapists | 5 weeks |
| Gonyea, Judith G. et al. 2016 USA [45] | Caregivers of relatives with early or moderate dementia | Cognitive behavioral group intervention | No | Therapists | 5 weeks and 3-, 6-, 9-, 12-week follow-up |
| Huang, Huei‐Ling, et al. 2003 China [46] | Caregivers of relatives with early and later stages of dementia | Progressively Lowered Stress Threshold | No | Gerontological nurses | 3 weeks and 3-month follow-up |
| Núñez-Naveira, Laura, et al. 2016 Denmark, Poland, Spain [47] | Caregivers of relatives with early and later stages of dementia | Not reported | No | No | 3 months |
| Gitlin, Laura N., et al. 2010 USA [48] | Care dyads (relatives with diagnosis of probable dementia or MMSE |
Competence-Environmental Press theory | Interview of caregivers to identify patient routines, interests, caregiver concerns | Occupational therapists and advance practice nurses | 4-, 9-month follow-up |
| Garand, Linda, et al. 2014, 2019 USA [49, 50] | Caregivers of relatives with mild cognitive impairment or early dementia | Problem Solving Therapy (PST) | No | Social workers | 4 weeks, and 3-, 6-, 12-month follow-up |
| Dias, Amit, et al. 2008 India [51] | Care dyads (relatives with mild or moderate dementia) | Not reported | No | Community team (home care advisors, lay counselors, psychiatrists) | Flexible, at least once a fortnight for six months |
| Tanner, Jeremy A., et al. 2015 USA [52] | Care dyads (older people with memory disorders) | Not reported | Checklist for identification of care recipient and caregiver needs | Intervention team (coordinators, nurses, geriatric psychiatrist) | 9-, 18-month follow-up |
| Mittelman, Mary S, et al. 2004, 2007, 2004 USA [53, 54, 55] | Caregivers of relatives with early and later stages of dementia | Pearlin’s stress process model | Systematic assessment for caregiver needs | Certified counselors | 4 months, regular follow-up intervals for as long as the caregiver participated |
| in the study | |||||
| Drentea, Patricia, et al. 2006 USA [56] | Caregivers of relatives with early and later stages of dementia | Pearlin’s stress process model | Systematic assessment for caregiver needs | Certified counselors | 4 months, regular follow-up intervals for as long as the caregiver participated |
| in the study | |||||
| Berwig, Martin, et al. 2017 Germany [57] | Caregivers of relatives with early and later stages of dementia | Schulz’s stress–health process | Risk assessment of 5 caregiver domains | Certified interventionists | 6-, 9-month follow-up |
| Jansen, Aaltje PD, et al. 2011 Netherlands [58] | Care dyads (older adults with early dementia) | Not reported | Caregiver Capacity and burden questionnaires | District nurses | 6-, 12-month follow-up |
| Livingston G, et al. 2013,2014 UK [59, 60, 61] | Caregivers of relatives with early and later stages of dementia | Based on Coping with Caregiving program | A self-completed measure of coping strategies | Supervised psychology graduates | 4-, 8-, 24-month follow-up |
| Whitlatch CJ, et al. 2019 USA [62] | Care dyads (persons with early-stage dementia) | Not reported | No | Counselors | 6 sessions |
| Bruvik FK, et al. 2013 Norway [63] | Care dyads (persons with early and later stages of dementia) | Not reported | No | Registered nurses, occupational therapists | 12 months |
| Seike A, et al. 2021 Japan [64] | Caregivers of relatives with early and later stages of dementia | Adult learning theory, Stress, appraisal and coping theory, Cognitive behavior therapy | No | Physicians, geriatric and dementia care nurses, clinical psychologists, and medical social workers | 12 weeks |
| van Wezel N, et al. 2021 Netherlands [65] | Caregivers of relatives with early and later stages of dementia | Not reported | No | Trained educators | 1–2 weeks, 3-month follow-up |
| Brown KW, et al. 2016 USA [66] | Caregivers of relatives with early-stage dementia | Not reported | No | Trained facilitators | 8 weeks, 3-month follow-up |
| Kor PP, et al. 2020 China [67] | Caregivers of relatives with early and later stages of dementia | Mindful coping model | No | Qualified interventionist | 10 weeks, 6-month follow-up |
| Judge KS, et al. 2013 USA [68] | Care dyads (persons with early and later stages of dementia) | Stress Process Model | A strength-based inventory assessing care dyad’s strengths across domains | Intervention specialists | 6 sessions, around 18.5 weeks |
| Wenborn J, et al. 2021 UK [69] | Care dyads (persons with early and later stages of dementia) | Not reported | No | Occupational therapists | 12 weeks, and 26-week follow-up |
| Boots LM, et al. 2018 Netherlands [70] | Caregivers of relatives with early and later stages of dementia | Not reported | No | Personal coach | 8 weeks |
| Author, year, country | Intervention components | Main outcomes of care-recipients | Main outcomes of informal caregivers | Main findings | Study limitations |
| Kajiyama, Bruno, et al. 2013 USA [42] | Training in stress management | No | Depressive symptoms, perceived stress, level of bother due to disruptive behaviors, quality of life | Greater improvement in perceived stress | Sample primarily on Caucasian women with some college education, low rate of participation, high dropout rate |
| Charlesworth, Georgina, et al. 2008 UK [43] | Befriending support | No | Caregiver wellbeing, perceived social support, positive affectivity, health related quality of life | No significant differences between groups | Narrow difference between intervention and control conditions, low rate of participation |
| Gonyea, Judith G. et al. 2006 USA [44] | Training in behavior management, pleasant events and relaxation | Neuropsychiatric symptom severity | Distress about the neuropsychiatric symptoms of care-recipients, caregiver burden | Less distress about the neuropsychiatric symptoms of care-recipients | Low rate of participation, small sample and no follow-up |
| Gonyea, Judith G. et al. 2016 USA [45] | Training in behavior management, pleasant events and relaxation | Neuropsychiatric symptom severity | Neuropsychiatric symptom-related distress, depressive symptoms, caregiver self-efficacy, caregiver anxiety | Lower neuropsychiatric symptoms severity of care-recipients, less distress about neuropsychiatric symptoms, a greater sense of self-efficacy in providing care, less depressive symptoms | Few male participants, lack of statistical power and no-treatment control group |
| Huang, Huei‐Ling, et al. 2003 China [46] | Training in helping identify behavior problems and plan environmental modifications + Telephone consultation | Behavioral problems | Caregiver self-efficacy | Decreased care-recipients’ behavior problems and increased caregiver self-efficacy | Small sample size and the relatively short follow-up |
| Núñez-Naveira, Laura, et al. 2016 Denmark, Poland, Spain [47] | UnderstAID Application covering education on dementia, skills training + Social network forum | No | Caregiving competence and satisfaction, depressive symptoms | Significantly decreased depressive symptoms | Sample bias based on the caregivers access to the internet, previous experience with smart devices, no follow-up |
| Gitlin, Laura N., et al. 2010 USA [48] | Education in dementia management skills + Training in home safety modifications, simplifying tasks, and stress reduction | Functional dependence, activity engagement, | caregiver well-being, confidence, perceptions of patient quality of life, appraisal of study benefits | At 4 months, improved patient functioning, especially IADLs, patient engagement, caregiver well-being and confidence using activities; at 9 months, no statistically significant differences between two groups | Only 15% male and a higher proportion of male caregivers than female caregivers dropped out |
| Garand, Linda, et al. 2014, 2019 USA [49, 50] | Education (5 topics) + Training (systematic application of PST) | No | Depressive symptoms, symptoms of anxiety, problem solving orientation, objective caregiver burden, subjective caregiver burden | Lower depressive symptom levels and mean anxiety levels, improvements in negative problem-solving orientation (NPO) scores; positive impact on subjective caregiving burden | Small sample size, focus on caregivers residing with care-recipient, no information on length of caregiving, reliance on Registry for recruitment |
| Dias, Amit, et al. 2008 India [51] | Education on dementia and caregiving skills + Referral resources + Family networking | Behavioral problems and activities of daily living in patients | Caregiver mental health, caregiver burden, distress due to behavioral disturbances of care-recipients | Improvements in caregiver mental health and perceived burden, non-significant reductions in care recipients’ behavior disturbances and functional ability | Small sample size, short follow up period |
| Tanner, Jeremy A., et al. 2015 USA [52] | Dementia education + Referral resources + Skills training | No | Objective caregiver burden, subjective caregiver burden, quality of life, depression | No statistically significant group differences in caregiver outcomes | Urban sample, lack of no-treatment control group |
| Mittelman, Mary S., et al. 2004, 2007, 2004 USA [53, 54, 55] | Counseling (individual and family) + Support group + Ad hoc counseling | No | Depressive symptoms, self-rated health, number of illnesses, caregiver appraisals of behavior problems in patients | Fewer depressive symptoms sustained for 3.1 years after baseline; better self-rated health sustained for 2 years, fewer illness reported; significantly reduced caregivers’ reaction ratings | Usual care group also received support and counseling, measure of number of illnesses was not weighted by severity of illness |
| Drentea, Patricia, et al. 2006 USA [56] | Counseling (individual and family) + Support group + Ad hoc counseling | No | Support satisfaction, size of network, frequency of visit and phone contact, emotional, informational and instrumental support | Higher levels of satisfaction with their social support network over the first 5 years, higher levels of emotional support, more visits, and having more network members | Usual care group also received support and counseling |
| Berwig, Martin, et al. 2017 Germany [57] | Dementia education + Training (problem solving, stress management) + Support group | Frequency of challenging behavior of patients | Caregiver perceived burden and social support, mental health, health-related quality of life, reaction to challenging behaviors of patients | Stabilizing effects on caregiver burden, improvements in health-related quality of life and reactions to challenging behavior of patients, reduced frequency of challenging behavior of patients. Decreased follow-up period effects | Intervention change process was evaluated only basically |
| Jansen, Aaltje PD, et al. 2011 Netherlands [58] | Referral resources + Family meetings + Telephone consultation | Quality of life | Quality of life, depressive symptoms, competence, burden | No significant differences between two groups | Insufficient sample size power to detect a small effect |
| Livingston G, et al. 2013,2014 UK [59, 60, 61] | Education + Training (communication, relaxation, behavioral management etc.) + Information support + Plans of maintain skills learnt | Quality of life | Potentially abusive behavior by caregivers towards the recipient, anxiety, depression, mental health, care burden, quality of life | Significantly reduced caregiver anxiety and depression scores, improved mental health, effects persisted at 24-month follow-up | Sample bias based on caregivers with more problems, not enough time and budget to translate the whole manual for non-English speaking participants |
| Whitlatch CJ, et al. 2019. USA [62] | Education + support + referral resources | Completion of a care plan, use of services, dyadic relationship functioning, participant well-being, program satisfaction | Completion of a care plan, use of services, dyadic relationship functioning, participant well-being, and program satisfaction | Able to construct a balanced care plan, increased use of services, dyadic functioning improved for one dimension (decreased emotional disruptions), higher program satisfaction | Lack of long-term effects evaluation, control group is not as usual care, sample is not large and diverse |
| Bruvik FK, et al. 2013 Norway [63] | Education + counseling + group meeting | Depression | Depression | No statistical significance | Geriatric Depression Scale might not fit well for carers |
| Seike A, et al. 2021 Japan [64] | Dementia education + skill training + social support | Cognitive function, ADL and BPSD | Depression, caregiving time, subjective burden, caregiving appraisal, care coping skills | Improved depression, caregiving appraisals and coping skills, sustained benefits over 24-, 48-week follow-up | Small sample size, not assess which program components were most effective |
| van Wezel N, et al. 2021 Netherlands [65] | Dementia education + support options | No | Knowledge about dementia, perceived ability to talk about dementia, support received and self-perceived pressure | Improvement in knowledge about dementia, a significant increase over time in the support received from home-care staff | Lack of long-term effects evaluation |
| Brown KW, et al. 2016 USA [66] | Class discussion of caregiving + mindfulness exercises | No | Perceived stress, experiential avoidance, mental and physical functioning, caregiver burden, mood, diurnal salivary cortisol, caregiver-recipient relationship quality | Lowe levels of perceived stress, tension, anger and caregiver burden, no statistical significance in 3-month follow-up | Small ample size |
| Kor PP, et al. 2020 China [67] | Psychoeducation on stress + mindfulness activities + peer sharing | Behavioral and psychological symptoms of dementia (BPSD) | Perceived stress, caregivers’ burden, depressive symptoms, anxiety, resilience, quality of life, and mindfulness | Improvement in perceived stress, depression, anxiety, BPSD-related caregivers’ distress, and mental health-related quality of life | Self-reported questionnaires might have resulted in a social desirability bias, small sample size |
| Judge KS, et al. 2013 USA [68] | Education + training communication skills, cognitive rehabilitation | No | Caregiver mastery, emotional health strain, physical health strain, self-efficacy, role captivity, dyadic relationship strain, quality of life, self-esteem, depression, anxiety | Less emotional health strain, dyadic relationship strain, role captivity, and improved caregiving mastery, fewer symptoms of anxiety and depression | Lack long-term effect evaluation, low adherence to the intervention |
| Wenborn J, et al. 2021. UK [69] | Training problem-solving skills and coping strategies + goal setting and achievement +plan future | Cognition, quality of life, assistance needed with ADL, mood, number of social contacts and leisure activities | Mood, sense of competence, number of social contacts and leisure activities | No significant differences in the validated outcome measures | Sample is not diverse, only English-speaking participants, and no consideration of sample ethnicity |
| Boots LM, et al. 2018 Netherlands [70] | Education + social support+ training coping stress, positive thoughts, communication etc. | No | Self-efficacy, mastery, depression, anxiety, and perceived stress, quality of life | Improvement in self-efficacy, mastery and quality of life | Only computer-literate caregivers included, low adherence to the intervention, lack of long-term effect evaluation |
Table 3 shows the theory basis of interventions and caregiver needs assessment matched with the interventions. Not all studies reported the theory basis of the interventions, except for the following studies: (1) A home-based caregiver training program was based on the Progressively Lowered Stress Threshold Model (PLST), which is tailored to individual needs of caregivers to improve their self-efficacy [46]. (2) A behavioral home-based Care of Persons with Dementia in their Environments (COPE) intervention was based on the Competence-Environmental Press theory, which targeted modifiable environmental stressors to maximize physical function in people with dementia and build dementia management skills in caregivers [48]. (3) A PST intervention was based on the Problem-Solving Therapy (PST) which focuses on training caregivers in adaptive problem-solving attitudes and skills [49, 50]. (4) An evidence-based multi-component intervention (NYUCI) and the Acquiring New Skills While Enhancing Remaining Strengths (ANSWERS) intervention are conceptually grounded in the Stress Process Model, which aims to build and improve the resources of caregivers in adapting to and managing care demands [53, 54, 55, 56, 68]. and (5) A multi-component individualized intervention (REACH) was based on the Schulz’s Stress–health Process Model, which aims at reducing risks in five caregiver domains (see below caregiver needs assessment) [57]. (6) A 5-week behavioral intervention reported in 2 studies [44, 45] and an individual therapy program (START, STrAtegies for RelaTives) reported in 3 studies [59, 60, 61] were based on the Coping with Caregiving (CWC), which was based on principles of cognitive behavioral therapy to reduce caregiver distress related to neuropsychiatric symptoms of people with dementia and general caregiver burden. (7) A group-based multicomponent psychoeducation intervention was grounded in the Adult learning theory, Stress, appraisal and coping theory and Cognitive behavior therapy, which aims to reduce caregiver depression, and improve caregiving appraisals and coping skills, and improve the conditions of people with dementia [64]. In addition, the mechanism of a modified mindfulness-based cognitive therapy is the mindful coping model [67].
Of all the 29 studies, only 12 studies mentioned the use of a caregivers’ needs assessment, including: (1) An individualized, comprehensive assessment battery for caregivers in the NYUCI systematically assessed the caregiving role, physical health and emotional health of caregivers, social support, caregiver understanding and response to the illness and social support [53, 54, 55, 56]. (2) An initial interview consisted of a core battery of caregiver assessment used by all REACH sites [48]. (3) The COPE used the Johns Hopkins Dementia Care Needs Assessment (JHDCNA) consisting of 4 major caregiver domains (i.e., caregiver education, resource referral, mental healthcare, medical healthcare) [52]. (4) Individual treatment strategies in the REACH intervention were selected based on an individualized risk assessment of five caregiver domains (i.e., knowledge of dementia, ability to care, perceived social support, emotional and physical well-being and challenging behavior) [57]. (5) The caregiver’s situation was explored by a nurse with a capacity and burden questionnaire to formulate a care plan [58]. (6) The START intervention used a brief COPE, a validated self-completed measure of coping strategies by the caregiver, with subscales measuring problem focused, emotion focused, and dysfunctional coping [59, 60, 61]. (7) The ANSWERS intervention applied a strength-based inventory assessing care dyad’s strengths across different domains, including cognitive, physical health, social activities, personality, life roles, leisure activities, and history and culture [68].
All interventions were categorized into a single-element or a multi-component group based on the intervention components and most interventions reported effective outcomes on informal caregivers. These studies reported a variety of health outcomes in informal caregivers, including depression, stress, anxiety, caregiver self-efficacy, caregiver burden and quality of life. Some studies also collected other outcomes including social support, role captivity, positive affectivity, self-rated health, wellbeing, appraisal of study benefits, completion of a care plan, use of services, dyadic relationship functioning, potentially abusive behavior by caregivers towards the care recipients and caregiver’s appraisals of behavior problems in care recipients [43, 48, 53, 54, 55, 56, 57, 59, 60, 61, 62, 68]. In 14 studies, outcomes about the care recipients were also evaluated, such as quality of life, functional dependence, depression, completion of a care plan, use of services, dyadic relationship functioning, wellbeing, program satisfaction, activity engagement, assistance needed with ADL, mood, number of social contacts and leisure activities, behavioral problems, frequency of challenging behavior, and neuropsychiatric symptom severity [44, 45, 46, 48, 51, 57, 58, 59, 60, 62, 63, 64, 67, 69]. Detailed information of the interventions is shown on Table 4.
Four studies that evaluated a single-element intervention were identified [42, 43, 44, 45]. Three of them had good methodological quality [42, 44, 45]. One of the four studies (25%), whose intervention is to provide informal caregivers with befriending support, did not report significant effects [43]. Three studies whose single intervention element is training reported statistically significant effects, including lower levels of neuropsychiatric symptoms severity in care recipients, reduced caregiver stress, a greater sense of self-efficacy in providing care, less depressive symptoms and less distress about the neuropsychiatric symptoms [42, 44, 45]. Among the three training programs, one’s [42] intervention emphasis is to provide stress management training for informal caregivers, and it was carried out via internet by a video tape. The other two interventions [44, 45] mainly focused on the training on behavior management of care recipients, planning of pleasant events and relaxation techniques, and these interventions were delivered by therapists.
The other 25 studies evaluated multi-component interventions. 17 studies were categorized as of good methodological quality [46, 47, 48, 49, 50, 51, 52, 58, 62, 63, 64, 65, 66, 67, 68, 69, 70], and 8 studies even had excellent methodological quality [53, 54, 55, 56, 57, 59, 60, 61]. 4 of the 25 studies (16%) did not show statistically significant benefits [52, 58, 63, 69]. 11 of 12 studies which had a common intervention component (i.e., social support) reported benefits for caregivers, such as improvements in mental health, emotional support, caregiving appraisals and coping skills, mastery, increased use of services [46, 47, 51, 53, 54, 55, 56, 57, 62, 64, 70], except for 1 study [58]. 10 of 12 studies which shared a common intervention component (i.e., training) all reported significant effectiveness for caregivers, such as improved quality of life and caregiver self-efficacy, reduced caregiver burden, less emotional health strain, less dyadic relationship strain, less role captivity, less distress and depressive symptoms [46, 48, 49, 50, 57, 59, 60, 64, 68, 70], except for 2 studies [52, 69]. 14 out of 16 studies which had a common intervention component (i.e., education) reported benefits for caregivers, such as increased caregiver self-efficacy, mastery, coping skills, improved wellbeing and quality of life, reduced caregiver burden and depressive symptoms, less role captivity [47, 48, 49, 50, 51, 57, 59, 60, 62, 64, 65, 67, 68, 70], except for 2 studies [52, 63].
Six interventions that had common intervention components (i.e., education and social support) demonstrated beneficial effects on caregiver’s depressive symptoms, caregiver’s mental health and perceived burden, caregiving appraisals, coping skills, and quality of life [47, 51, 57, 62, 64, 70]. 9 of 10 studies which shared common intervention component (i.e., education, training) reported such benefits for caregivers as improved quality of life, reduced caregiver burden, improved caregiving mastery [48, 49, 50, 57, 59, 60, 64, 68, 70], except for one study [52]. Among them, the COPE intervention consisting of education and training components improved patient functioning and activity engagement as well as caregiver wellbeing at 4 months, yet no significant effect was found in outcomes during the 9 months follow-up period [48]. Similarly, one study reported that the REACH intervention composed of education, training and support group based on individualized assessment of caregivers’ needs, had a reduced stabilization effect on the burden caused by care in the follow-up period [57]. Of all the effective interventions, only the NYUCI and the START intervention presented sustained benefits after years of follow-up due to its unique intervention elements, not found in other interventions (i.e., on-going support group participation, ad hoc counseling, plans of maintaining skills learnt) [53, 54, 55, 56, 59, 60]. Sustained effective outcomes include fewer depressive symptoms for 3.1 years, better self-rated health for 2 years, higher levels of satisfaction with social support network in caregivers for 5 years [53, 54, 55, 56], improved mental health and reduced anxiety and depression for 2 years [59, 60].
This systematic review identified 29 studies describing 22 different types of interventions for informal caregivers of older people with early dementia. Most studies reported effective outcomes on informal caregivers, and 19 of the 22 different types of interventions comprised two or more components (i.e., education, training, support group). Only 10 different types of interventions mentioned the theoretical underpinnings. This paper represents the very first to systematically assess randomized controlled trials (RCTs) for informal caregivers of older people with early dementia.
Well-established evidence emphasized the great benefits of timely support for informal caregivers of older people with early dementia [71]. One recent systematic review also reported that informal caregivers of people with dementia felt it was the right time to receive information and support directly after or at the time of diagnosis [72]. However, 15 different types of interventions identified in our systematic review are effective for informal caregivers of older people with early and later stages of dementia [42, 44, 45, 46, 47, 48, 51, 52, 53, 54, 55, 56, 57, 59, 60, 61, 63, 64, 65, 67, 68, 70]. Furthermore, 3 different types of effective interventions solely focused on informal caregivers of older people with early dementia [49, 50, 62, 66]. To provide timely target support for this type of caregivers, future research should consider more clinical trials to develop and implement effective interventions for them.
Psychosocial interventions for informal caregivers need to be person-centered through structured needs assessment, as interventions for the persons with dementia [73, 74]. A needs-matched intervention for informal caregivers of people with cognitive decline should be developed further [75]. Yet our review showed that only five studies applied a structured needs assessment for informal caregivers prior to or when delivering the intervention [53, 54, 55, 56, 57]. Namely, only 2 different types of psychosocial interventions (i.e., NYUCI, REACH) were person-centered and tailored to informal caregivers’ comprehensive needs. Moreover, just one study developed and validated a screener based on interRAI assessments to assess informal caregivers’ wellbeing [76]. A validation study of a systematic assessment for informal caregivers is still lacking.
In addition, one systematic review summarizing systematic reviews of psychosocial interventions for caregivers of people with dementia showed that the most effective interventions should include both the education and therapeutic component [77]. Compared to previous systematic reviews, this systematic review firstly identified which interventions could better support informal caregivers of older people with early dementia on one hand, determining which elements are essential for this caregiver group and why on the other hand. Our systematic review revealed that intervention components, including caregiving skills training, dementia education, counseling and social support have beneficial effects on different caregiver outcomes. In addition, ongoing intervention support (e.g., ad-hoc counseling, plans of maintaining skills learnt) is of great significance for the sustainable effects of the interventions [53, 54, 55, 56, 59, 60]. This can also be supported in another two studies identified in our review, which reported the intervention effects decreased or disappeared during the follow-up period [48, 57]. We also pointed out the theoretical underpinnings of effective interventions directly, including Progressively Lowered Stress Threshold, Competence-Environmental Press Theory, Stress process model and Schulz’s stress-health process, and Adult learning theory, Stress, appraisal and coping theory, Cognitive behavior therapy. These findings could improve our understanding of the effects of interventions and facilitate future successful translation studies in this area. Furthermore, it will be possible to provide timely targeted interventions specifically for informal caregivers of people with early dementia. Beyond the implications for dementia care, the essentials of effective interventions identified in this review will inform the future development, adaptation and implementation of evidence-based interventions in similar caregiving practices (e.g., chronic diseases). Finally, future research could also consider the cost effectiveness potential in different combinations of intervention essentials, given that the dementia care is considerably expensive.
A strength of this systematic review is the fact that we used the PEDro scale to assess the methodological quality of the studies. This rigorous scale made it possible to evaluate the studies and find which ones were more robust and met the quality criteria. A limitation is the fact that we only included peer-reviewed journal articles written in English in our systematic review. Maybe we have missed some interventions reported in ‘grey literature’ or written in another language than English, which might have had a significant effect on caregiver outcomes. Another limitation is that we only included RCT studies, as this was a choice we have made to make sure studies had some standardization in the measurements, as well as a control group to evaluate the effectiveness of the interventions.
Through rigorous searching and screening, we finally identified 29 RCT-studies and a total of 22 different types of interventions. The methodological quality of studies and the intervention essentials combined with corresponding effectiveness of these interventions were critically assessed. The findings of this systematic review can provide knowledge on which and why psychosocial interventions are effective for informal caregivers of older people with early dementia.
The review findings revealed that there is a paucity of effective interventions on supporting informal caregivers of older people with early dementia. Future research should consider more evaluation trials to develop and implement compact interventions for them, given that timely support for this caregiver group has considerable benefits to the health care systems. The development or adaptation of this compact interventions should consider carefully the following essentials: a validated theoretical underpinning (e.g., stress process model, health-stress theory, PLST), tailored support matched with a systematic assessment of caregiver needs, ongoing support provision (e.g., ad-hoc counseling, plans of maintaining skills learnt) and the inclusion of multi-components in an intervention (e.g., education, social support, training). Furthermore, we highlight there is a lack of systematic caregiver needs assessment prior to or when delivering an intervention and further studies needed. The findings from our systematic review could serve as a comprehensive summary of the current state of effective psychosocial interventions for informal caregivers of older people with early dementia. This is informative for policymakers and researchers from several disciplines to further develop and implement effective interventions for caregivers in similar caregiving contexts.
Study concept and design: SW, JM, AD; Drafting of the manuscript: SW; Critical revision of the manuscript for important intellectual content: SW, JM, AD; all authors agreed with the final manuscript.
Not applicable.
We thank all the peer reviewers for their comments. We also thank the China Scholarship Council (CSC).
Shanshan Wang is supported by the China Scholarship Council (CSC) (File No. 201806330119).
The authors declare no conflict of interest.
Review question
Assessing psychosocial interventions for informal caregivers of people with early dementia: A systematic review of randomized controlled evidence.
We aim to answer the following questions:
(1) What components of psychosocial interventions are effective for informal caregivers of older people with early dementia?
(2) What theories underpin these interventions?
(3) What caregivers’ needs are assessed in these interventions?
Searches
PubMed, CINAHL, Embase, Cochrane and Web of Science.
Types of study design to be included
Randomized controlled trials (RCTs).
Condition or domain studies to be included
Early dementia or early cognitive decline or memory loss.
Participants
Informal caregivers of older people with early dementia.
Interventions
Psychosocial interventions, including counselling, education, training, support, problem solving, coping strategy, cognitive behavior therapy, art, music, singing and museums.
Context
Home setting.
Outcomes
All outcomes related to health and life quality in informal caregivers (and care recipients).
Study selection
Two reviewers will select studies for inclusion and exclusion against the criteria through screening the titles and abstracts. Uncertainties will be resolved through discussion with a third reviewer.
Study quality assessment
Two reviewers will assess the quality of each study using a modified 11-item version of the PEDro scale. Differences in scoring will be discussed and resolved collaboratively with a third reviewer.
Data extraction
Two reviewers will read the full text of each study included in the review and extract key content of the studies. According to our research aim and questions, the following characteristics will be extracted with a standardized electronic form: (1) author, year and country, (2) theoretical underpinning, (3) caregiver needs assessment, (4) sample, (5) people delivering the intervention, (6) intervention duration, (7) intervention elements, (8) main outcomes of care recipients, (9) main outcomes of caregivers, (10) main findings, (11) study limitations.