



 , Lei Liu 1, Xi Liu 1, Shuhong Li 1, Simiao Liu 1, Rui Wang 1
, Lei Liu 1, Xi Liu 1, Shuhong Li 1, Simiao Liu 1, Rui Wang 11 Department of Gastroenterology, Tianjin Nankai Hospital, 300100 Tianjin, China
Academic Editor: Pietro Gentile
Abstract
Objective: Reflux esophagitis animal models represent an important component in the preclinical study of digestive system drugs, and the aim of this study was to determine the best modeling method. Methods: Female Wistar rats were used to establish reflux esophagitis models by employing the following methods: improved chemical burn, external pyloric clamp plus anterior gastric ligation, cardiomyotomy plus semipyloric ligation, cardiomyotomy plus internal pyloric ligation, cardiomyotomy plus external pyloric ligation, and cardioplasty plus pyloric ligation plus gastrojejunal Roux-en-Y anastomosis. The body weight, lower esophageal pH and esophageal mucosal injury of the rats were observed. Results: The model formation rate was 83% based on cardiomyotomy plus external pyloric ligation. On the 3rd day after the operation, lower esophageal mucosa congestion occurred, and the model was successfully established. On the 7th day, mucosal hyperemia and erosion were observed in the most serious lesions, indicating optimal model conditions. On the 14th day, the lower esophageal mucosa remained congested, suggesting that the model was useful from the 3rd to the 14th day. The method caused less trauma to the animals. The ligation diameter was uniform, and the model was more stable. Conclusion: Cardiomyotomy plus external pyloric ligation is the best method.
Keywords
- Reflux esophagitis
- Animal model
- Cardiomyotomy plus external pyloric ligation
Reflux esophagitis (RE) is a common upper gastrointestinal disease caused by lower esophageal sphincter dysfunction, gastric juice or mixed intestinal juice reflux stimulation [1, 2]. Gastric juice or mixed intestinal juice reflux stimulation promotes proliferation and reduces apoptosis of esophageal mucosal cells. Therefore, gastroesophageal reflux has been identified as a major risk factor for esophageal adenocarcinoma and Barrett’s esophagus. Acidostatic therapy is the main method for treating RE at present. Gastric acid inhibitors effectively heal and alleviate symptoms of esophagitis. However, in certain patients, symptoms cannot be significantly improved, and their conditions continue to worsen [3]. In recent years, the incidence of RE has increased due to the increasing pressure of daily life and numerous other unfavorable factors, such as poor living habits [4].
Reflux esophagitis is mainly caused by excessive exposure to gastric contents due to impairments of various protective mechanisms that prevent reflux into the esophagus. Studies have shown that reflux gastric juice does not directly damage the esophagus but stimulates esophageal epithelial cells to secrete chemokines, which mediate damage to esophageal tissue [5]. The pathogenesis of RE has always been the focus of medical theory and practical research. The RE animal model is an important component in the preclinical study of digestive system drugs. At present, an external pyloric clamp plus anterior gastric ligation and cardiomyotomy plus semipyloric ligation are common modeling methods. However, the low survival rate of model animals and poor molding effects affect research progress. Thus, a better RE model method is urgently needed. Based on previous research, we explored a new modeling method, namely, cardiomyotomy plus external pyloric ligation, to effectively generate an acid reflux model. In this study, we compared the commonly used methods for establishing reflux esophagitis models and identified the best method for model establishment.
The present study was approved by the Ethics Committee of Tianjin Nankai
Hospital (Tianjin, China). In total, 55 female Wistar rats weighing approximately
280 g were used in the study. The animals were maintained at a constant room
temperature of 22
The rats were maintained under isoflurane inhalation anesthesia. Rats were induced with 1.5% isoflurane and the isoflurane concentration was gradually reduced and maintained at 0.5% after the loss of righting reflex. To prevent bleeding during cardiotomy, the branch of the left gastric artery that passes across the gastroesophageal junction was sutured with a fine needle. A pyloric clamp was placed at the junction of the duodenum and pyloric ring. The ring was fixed with a 3/0 line after closure, and the 2/3 fundus of the stomach was ligated with the other end of this line to prevent the pyloric clamp from shifting to the distal end [6]. After closing the abdominal cavity, gentamicin sulfate was dripped into the abdominal cavity. The abdominal cavity was closed, and the wound was subsequently disinfected with iodophor. After awakening, the rats were fed a 5% glucose and sodium chloride solution.
After 24 hours of fasting, half (15 g/d) of the standard pellet diet was given for 3 days, and the full (30 g/d) diet was given for 14 days. On the 3rd, 7th, 10th and 14th days after the operation, general specimens of the rat esophagus and pathology of the lower segment of the esophagus were observed under microscopy, and immunohistochemistry analysis was performed (Fig. 1A).
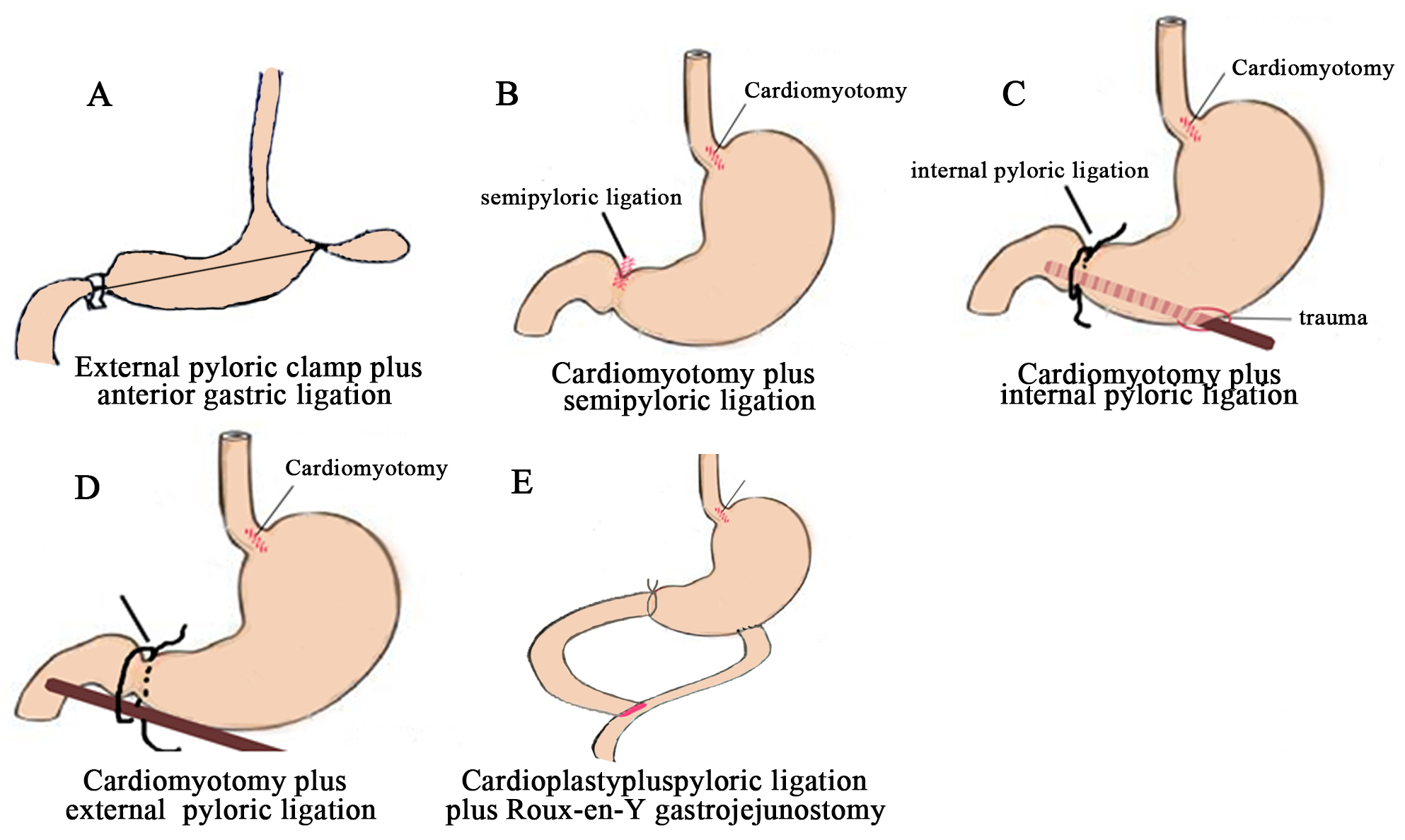 Fig. 1.
Fig. 1.Sketch of the operative method in these groups. (A) External pyloric clamp plus anterior gastric ligation. (B) Cardiomyotomy plus semipyloric ligation. (C) Cardiomyotomy plus internal pyloric ligation. (D) Cardiomyotomy plus external pyloric ligation. (E) Cardioplasty plus pyloric ligation plus Roux-en-Y gastrojejunostomy.
Anesthesia, vascular ligation and cardiomyotomy were performed as described in group A. The median abdominal incision was approximately 25 mm. The cardiac muscle was cut longitudinally at the junction of the esophagus and stomach for approximately 1 cm, and the mucosa was completely exposed. Half of the pylorus was sutured with a 3/0 suture needle, and blood vessels were avoided. The feeding method was the same as that described for group A (Fig. 1B).
Anesthesia, vascular ligation and cardiomyotomy were the same as that described in group C. The median abdominal incision was approximately 25 mm. The cardiac muscle was cut longitudinally at the junction of the esophagus and stomach for approximately 1 cm, and the mucosa was completely exposed. A metal needle was punctured into the stomach from the stomach body and passed through the pylorus to the duodenal end. The outer diameter of the metal needle was 1.55 mm. The remaining pylorus outside the metal needle was sutured and ligated. The metal needle was removed after the suture was completed. The feeding method was the same as that noted for group A (Fig. 1C).
Anesthesia, vascular ligation and cardiomyotomy were performed as described in group C. The median abdominal incision was approximately 25 mm. The cardiac muscle was cut longitudinally at the junction of the esophagus and stomach for approximately 1 cm, and the mucosa was completely exposed. The metal rod was placed longitudinally outside the pylorus of the stomach. The metal rod was ligated with the pylorus, and the metal rod was subsequently pulled out. The diameter of the metal rod was 4 mm. The feeding method was the same as that described in group A (Fig. 1D).
Anesthesia, vascular ligation and cardiomyotomy were the same as that described in group A. The median incision in the upper abdomen was approximately 25 mm, and the incision of the cardia was approximately 0.5 cm. The two ends reached the esophagus and stomach. The blood vessels of the pylorus were sutured transversely and intermittently with noninvasive sutures, and the pylorus was ligated with noninvasive sutures. The jejunum was cut off approximately 8–10 cm away from the pylorus. The distal end was anastomosed end to side with the greater curvature of the glandular stomach, and the proximal end was anastomosed to the sidewall of the small intestine (end-to-side anastomosis) approximately 12–15 cm from the cut edge (Fig. 1E).
After anesthesia, the rats were laparotomized (the specific steps are the same as above), a small hole was pierced in the great curvature of the stomach, the pH electrode of the automatic pH recorder (digraphertmmk III, Synaptics) was inserted into the stomach from the perforation, and entered the esophagus through the cardia. The electrode was placed at the esophageal mucous membrane 1 cm above the gastroesophageal junction, and the pH value was read and recorded 1 min later.
The animals were sacrificed by chloral hydrate anesthesia, and the abdomen was opened thereafter. The lower esophagus was excised and observed, and the specimen was scored based on the evaluation method.
The excised specimen was washed with 10% formalin and fixed with 10% formalin
solution for at least 24 h. The esophagus was cut into 3-mm intervals and
embedded in paraffin. Then, 5-
The rats were sacrificed on the 3rd, 7th, 10th and 14th days after the operation. Approximately 3 cm of the esophagus was removed from the upper edge of the cardia. The esophagus was longitudinally dissected and rinsed with 0.9% sodium chloride solution. The general manifestations of the lower esophageal mucosa were observed and graded with the naked eye. Classification criteria: 0 (normal) = could have histological changes, score 0; I (mild) = points or strips of redness, erosion, no fusion, score 1; II (moderate) = strips of redness, erosion, and fusion but not full-cycle, score 2; and III (severe) = extensive lesions, redness, erosion, fusion, or ulcers, score 3.
The lower portion of the esophagus was fixed in 10% formalin solution, and paraffin sections were prepared. After hematoxylin and eosin (HE) staining, each section was observed under light microscopy, and the pathological grading score was calculated. The integral standard refers to Table 1.
| Pathological characteristics | Classification | ||
| Mild | moderate | severe | |
| Squamous epithelial hyperplasia | + | + | + |
| Papillary extension of lamina propria mucosa | + | + | + |
| Inflammatory cell infiltration in epithelial cell layer | + | + | + |
| Mucosal erosion | – | + | – |
| Ulceration | – | – | + |
| Barrett’s esophageal changes | – | – | + |
The data in the study are presented as the mean
At 14 days after operation, the pH value of lower esophagus was 3.73
| Modeling method | |||||
| External pyloric clamp plus anterior gastric ligation | Cardiomyotomy plus semipyloric ligation | Cardiomyotomy plus internal pyloric ligation | Cardiomyotomy plus external pyloric ligation | Cardioplasty plus pyloric ligation plus Roux-en-Y gastrojejunostomy | |
| Model rate | 0.286 | 1 | 0.55 | 1 |
0 |
| Mortality | 0.714 | 0 | 0.45 | 0 |
1 |
| PH value of lower esophagus on the 14th day | 3.73 |
5.5 |
5.55 |
3.53 |
/ |
| Duration of esophagitis in rats | 7rd day to the 14th day after operation | 3rd day to the 14th day after operation | 3rd day to the 14th day after operation | 3rd day to the 14th day after operation | / |
| Note: The success ratio of modeling in different groups. The model formation rate of goup D was higher than that in group A, B and E ( | |||||
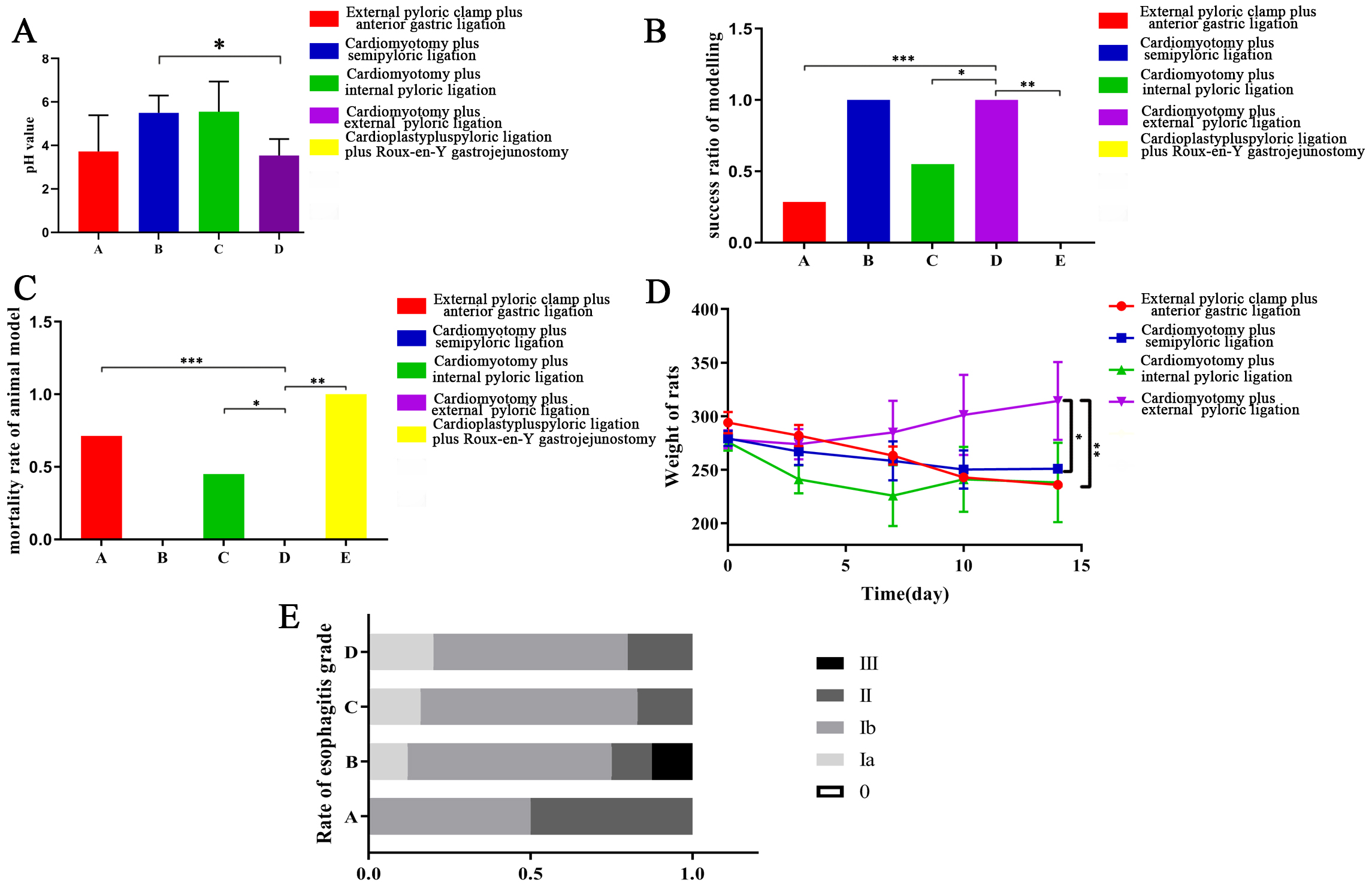 Fig. 2.
Fig. 2.Comparison of RE in rats. (A) The pH value of lower esophagus. At 14 days after operation, the pH value of lower esophagus was 3.73 ± 1.35 in group A, 5.5 ± 0.65 in group B, 5.55 ± 1.14 in group C and 3.53 ± 0.62 in group D. The pH value in group D was significantly lower than that in group B (p = 0.0365). (B) The success ratio of modeling in different groups. The model formation rate was 28.6% in group A, 100% in group B, 55% in group C and 100% in group D. The model formation rate of group D was higher than that in group A, B and E (p
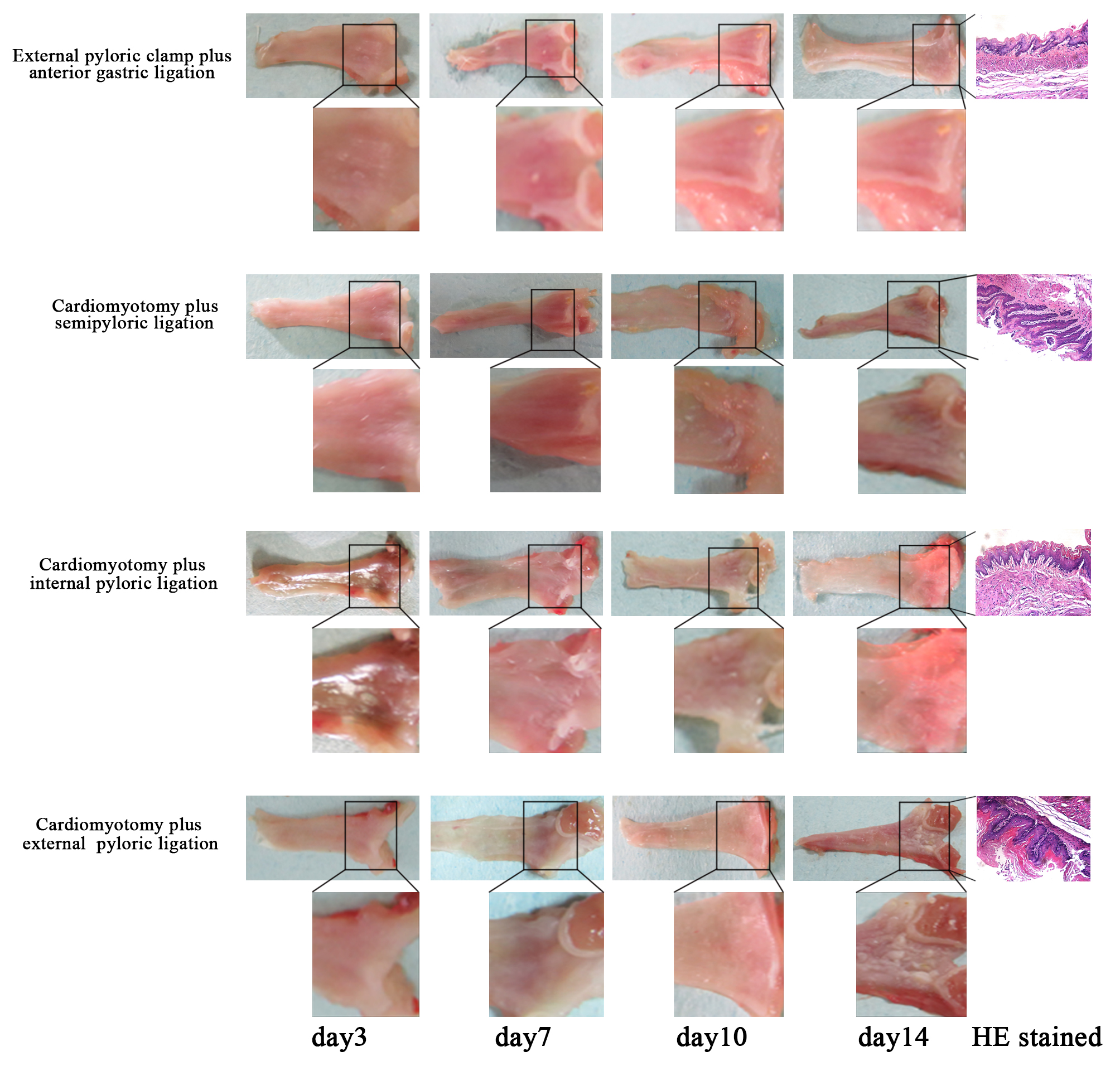 Fig. 3.
Fig. 3.The macroscopic appearance of reflux esophagitis in a rat model of reflux esophagitis established in the rats.
At 14 days after operation, the pH value of lower esophagus was 5.5
At 14 days after operation, the pH value of lower esophagus was 5.55
At 14 days after operation, the pH value in group D of lower esophagus was 3.53
The model rate of group E was 0.
The lower esophageal mucosa of group A was normal on the 3rd day after the operation without congestion and erosion. On the 7th day after the operation, mucosal hyperemia occurred, and the model was successfully established. On the 14th day, mucosal lesions were aggravated with congestion and erosion, suggesting that the model was optimal from the 7th to 14th day.
Lower esophageal mucosal hyperemia occurred on the 3rd day after the operation in group B, and the model was successfully established. On the 7th day, mucosal erosion and ulceration occurred, and severe lesions were noted. Thus, this model was considered an ideal model. On the 14th day, the lower esophageal mucosa still displayed congestion and erosion, suggesting that the model was useful from the 3rd day to the 14th day.
Lower esophageal mucosal hyperemia occurred on the 3rd day after the operation in group C, and the model was successfully established. On the 7th day, mucosal hyperemia and erosion occurred, and severe lesions were noted. Thus, this model was considered an ideal model. On the 14th day, the lower esophageal mucosa remained congested, suggesting that the model was useful from the 3rd to the 14th day.
Lower esophageal mucosal hyperemia occurred on the 3rd day after the operation in group D, and the model was successfully established. On the 7th day, mucosal congestion, erosion and ulceration occurred, and severe lesions were noted Thus, this model was considered an ideal model. On the 14th day, the lower esophageal mucosa remained congested, suggesting that the model was useful from the 3rd to the 14th day.
The lower esophageal mucosa of group E exhibited no congestion or erosion on the 3rd day after the operation, and all of the animal models died.
In group A, the external pyloric clamp plus anterior gastric ligation had a significant influence on gastric emptying. Esophageal acid reflux was effective, and alkali reflux could be controlled. However, the survival rate of the animals was 28.6%, and the modeling time was long. In addition, animal trauma was noted. Moreover, the duration was short, and the effect of the model was poor, which is not conducive to follow-up experimental studies. The method of cardiomyotomy plus semipyloric ligation employed in group B was simple and minimally invasive, and the rate of model formation was 100%. There was no unified reference, and the diameter of the ligation tube was not uniform. The degree of esophageal mucosal injury was mild, which was not conducive to follow-up in basic research. The method applied in group C (cardiomyotomy plus pyloric ligation) ensures uniformity of the ligation tube diameter. However, the model formation rate is only 55%, which is not conducive to follow-up in basic research. In group D, cardiotomy plus external pyloric ligation yielded a model formation rate of 83%. This procedure was less traumatic, and a uniform ligation tube diameter was obtained. The model lasted longer and had a better effect. Alkali reflux was completely eliminated in group E, but the operation was traumatic, time-consuming, and complicated by unsustainable feeding and high mortality, which are not conducive to follow-up experiments.
Reflux esophagitis is a gastrointestinal motility disorder, and the pathophysiological mechanism is primarily due to a decrease in the antireflux defense mechanism and enhancement of the total effect of reflux food on the esophageal mucosa [1, 7]. It is generally believed that acid reflux is the main cause of esophageal mucosal injury. The severity of mucosal injury depends on the ability of the esophageal mucosa to reflux substances. Clear food mucosa depends on the coordination of contraction and relaxation of esophageal smooth muscle [8, 9, 10]. In recent years, based on in-depth studies of cytokines and signaling pathways related to reflux esophagitis, researchers have identified specific cytokines and signaling pathways related to reflux esophagitis [11]. Gastrin and motilin contract the lower esophageal sphincter, whereas vasoactive intestinal peptide and somatostatin relax the lower esophageal sphincter and reduce the pressure of the lower esophageal sphincter [12]. The Wnt/beta-catenin signaling pathway is not activated in nonmetaplastic Barret esophageal tissue but is found in dysplastic Barret esophageal and esophageal cancer, suggesting that the Wnt/beta-catenin signaling pathway plays an important role in the development of esophagitis in Barret esophageal tissue [13]. Key proteins of the PI3K/Akt pathway Akt and the ERK1/2 pathway ERK1/2 were also abnormally activated during normal esophageal development, reflux esophagitis, Barret esophagus, dysplasia and esophageal adenocarcinoma [14].
The establishment of animal models for reflux esophagitis is the basis for the study of cytokines and signaling pathways related to the pathogenesis of reflux esophagitis. Currently, many methods are available to establish animal models of reflux esophagitis both domestically and abroad [15, 16]. Factors, such as surgical trauma and susceptibility to infection, necessitate increased demands for experimental implementation and the research team. The basic requirements for establishing a reflux esophagitis model include a high rate of model formation, model stability, reduced trauma and simple operation procedures. At present, the most commonly used modeling method of reflux esophagitis is chemical burn method. Hydrochloric acid solution with 0.1 mol/L collocation concentration and pepsin were added to collocate digestive juice at a ratio of 1:1000. The hydrochloric acid solutionwas slowly pushed into the esophagus. The modeling method had a high model success rate and a high animal survival rate, but the modeling method could not simulate the natural course of RE. Some researchers used cardiomyotomy plus internal pyloric ligation method. The method ensures uniformity in the ligation tube diameter, but with a wound on the stomach wall. Some researchers used external pyloric clamp plus anterior gastric ligation method. As this method was with high mortality rate, it was not an ideal method. Cardiomyotomy plus semipyloric ligation was a limited method as the pyloric caliber cannot be unified. In a word, the cardiomyotomy plus external pyloric ligation was the best RE model.
Human lower esophageal mucosal cells are nonkeratinized stratified squamous epithelial cells with submucosal glands that secrete mucus to protect the epithelium from erosion. The structure and physiology of dogs and pigs are similar to those of humans, and their genomes are highly homologous to that of humans. These models are feasible for endoscopy and follow-up but are expensive. Gene modification technology is relatively complex, and it is not ideal technique for the generation of animal models. The lower esophageal mucosal cells of rats were completely keratinized and had strong resistance to gastric reflux and duodenal reflux [17]. The esophagus of mice is too thin, the operation is difficult, the success rate is low, and the reaction to reflux is obviously different. Rats with moderate size and high susceptibility to Barrett’s esophagus make for ideal animal models. In addition, the procedures should be easy to perform.
The animal survival rate is a highly important factor in the process of modeling. We use high-quality rats. Weight was strictly controlled at 250–280 g, and preoperative fasting was sufficient. Environmental temperature, humidity and hygiene are well controlled. The operation avoids blood vessels as much as possible under strict aseptic operation conditions (abdominal antibiotics). Postoperative feeding should be gradually introduced to avoid postoperative intestinal obstruction and gastric dilatation. Attention should be focused on the time limit of rat models to avoid missing out on the best time to use the models.
In this study, we used rats as experimental subjects and compared 5 different modeling methods. The results showed that cardiotomy plus external pyloric ligation was the best method. In this study, detection of the lower esophageal pH value in rats was transient and had selected limitations, which can be further improved in future studies.
YT designed the study and supervised the data collection. LL analyzed the data and interpreted the data. XL, SL (Shuhong Li), SL (Simiao Liu) and RW prepared the manuscript for publication and reviewed the draft of the manuscript. All authors have read and approved the manuscript.
Ethical approval was obtained from the Ethics Committee of Tianjin Nankai Hospital. The ethics code is “IRM-DWLL-2015223”.
Not applicable.
This study was supported by the Chinese National Natural Science Foundation (Grant Nos. 81573737 and 82074213).
The authors declare no conflict of interest.