




 , Mahmut Selçuk 1,*
, Mahmut Selçuk 1,* , Ercan Saruhan 2
, Ercan Saruhan 21 Department of Psychiatry, Muğla Sıtkı Koçman University Faculty of Medicine Kötekli, 48000 Menteşe/Muğla, Türkiye
2 Department of Medical Biochemistry, Muğla Sıtkı Koçman University Faculty of Medicine Kötekli, 48000 Menteşe/Muğla, Türkiye
Abstract
Major depressive disorder (MDD) has been increasingly associated with neuroinflammatory and neurovascular dysfunction. Claudin-5, a key tight junction protein essential for blood–brain barrier integrity, has an unclear role as a peripheral biomarker in MDD. This study examined serum Claudin-5 alongside systemic inflammatory indices—including the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), monocyte-to-lymphocyte ratio (MLR), the inflammation score (INFLA), and suicidal ideation in antidepressant-naive or medication-free (for at least three months) adult MDD patients.
73 antidepressant-naive or drug-free MDD patients and 74 age- and sex-matched healthy controls were enrolled. Depression severity and suicidality were assessed using the Hamilton Depression Rating Scale (HAM-D) and Beck Scale for Suicide Ideation (BSSI). Serum Claudin-5, C-reactive protein (CRP), and complete blood counts were measured, and inflammatory indices (NLR, PLR, MLR, INFLA) were calculated. Between-group comparisons, correlation analyses, and receiver operating characteristic (ROC) analyses were performed.
MDD patients showed significantly reduced Claudin-5 and elevated NLR, PLR, CRP, and INFLA scores compared with controls (all p < 0.05). Claudin-5 was not associated with symptom severity, suicidality, or inflammatory indices. ROC analysis for serum Claudin-5 indicated fair accuracy in distinguishing MDD from controls (AUC = 0.737) but limited value for predicting suicidal ideation (AUC = 0.628).
Reduced serum Claudin-5 in untreated MDD may indicate relatively stable endothelial alterations rather than acute, state-dependent changes. Although Claudin-5 alone had limited prognostic value for suicidality, inflammatory indices—particularly NLR and INFLA—showed stronger associations. Integrating vascular and immune biomarkers may enhance biological stratification and suicide risk assessment in depression and guide future multimodal studies.
Keywords
- blood–brain barrier
- Claudin-5
- inflammation
- major depressive disorder
- suicidal ideation
Major depressive disorder (MDD) is a complex psychiatric condition influenced by biological and environmental factors [1]. Among biological mechanisms, inflammation has gained particular attention for linking peripheral immune activation with central neurobiological alterations—including disrupted neuroimmune signaling, neurotransmission, and neurovascular integrity—that contribute to depressive symptoms [2, 3]. Dysregulated immune responses and elevated peripheral inflammation have been widely reported in depression and have been linked to poorer prognosis and reduced antidepressant response [1, 2]. Dysfunction of the blood–brain barrier (BBB) and neurovascular unit may mediate the effects of systemic inflammation on the central nervous system (CNS) [3, 4].
The BBB is a selective interface that maintains neural homeostasis by separating the CNS from systemic circulation. It consists of endothelial cells, pericytes, astrocytes, neurons, and microglia [5]. Tight junctions between endothelial cells regulate paracellular permeability. Claudin-5, the main transmembrane protein in endothelial tight junctions, is expressed throughout the vascular system but shows particularly high expression in brain microvascular endothelial cells, where it maintains BBB integrity [6, 7].
Disruption of Claudin-5 compromises BBB integrity, allowing peripheral cytokines
such as interleukin-6 (IL-6), tumor necrosis factor-alpha
(TNF-
The mechanisms underlying altered peripheral Claudin-5 levels remain debated. One hypothesis proposes a spillover mechanism in which BBB leakage releases tight-junction proteins into circulation [10, 11], while another suggests transcriptional downregulation, where inflammatory or epigenetic factors suppress Claudin-5 expression in CNS endothelial cells [12, 13]. Claudin-5 expression is modulated by pro-inflammatory cytokines, vascular endothelial growth factor, and glutamate (downregulation) and by estrogen, glucocorticoids, and glial cell line-derived neurotrophic factor (upregulation) [14, 15]. Because cerebrospinal fluid sampling is invasive, serum Claudin-5 provides a more accessible but indirect marker of BBB integrity. However, peripheral levels may only partially mirror central tight-junction status. Experimental and clinical evidence support this interpretation, showing that Claudin-5 dysregulation alters BBB permeability and contributes to neuroinflammatory changes in depression and related disorders [10, 11, 12, 13, 16, 17]. Such studies collectively support the use of serum Claudin-5 as an accessible, albeit indirect, indicator of BBB integrity.
Due to its tight-junction specificity, Claudin-5 has emerged as a key biomarker of neurovascular dysfunction in depression. Unlike general inflammatory markers, it directly reflects endothelial integrity. Preclinical studies show that Claudin-5 dysregulation increases BBB permeability and induces stress-related depressive phenotypes [13, 16]. Postmortem research has revealed reduced Claudin-5 mRNA expression in the nucleus accumbens of unmedicated individuals with MDD, as demonstrated by Menard et al. [13], and summarized in subsequent reviews [16]. Nonetheless, there are few clinical studies assessing peripheral Claudin-5 levels in untreated adult MDD populations.
Animal models show that chronic social defeat stress downregulates Claudin-5 in brain regions such as the prefrontal cortex and nucleus accumbens, leading to increased BBB permeability and depressive-like behaviors [10, 12, 13]. Recent evidence also identifies Claudin-5 as a potential therapeutic target in depression and schizophrenia [5, 16, 17].
Moreover, BBB dysfunction and Claudin-5 downregulation have been linked to
suicidal ideation, a major concern in MDD. Elevated IL-6 and
TNF-
Postmortem and experimental studies further confirm Claudin-5 reduction in the brains of suicide victims and stress-exposed animals showing depressive behaviors [12, 13].
Beyond molecular BBB markers, systemic inflammatory indices—such as the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), monocyte-to-lymphocyte ratio (MLR), and the inflammation score (INFLA)—have emerged as simple and inexpensive indicators of low-grade inflammation. Meta-analytic and clinical studies show that NLR, PLR, and MLR are elevated in depressive disorders and associated with symptom severity [21, 22]. These indices are also linked to suicidal ideation and behavior, suggesting systemic immune activation that compromises BBB integrity and interacts with Claudin-5 dysregulation in depression and suicidality [18, 19, 23].
Despite these findings, many previous studies included heterogeneous samples with ongoing treatment or medical comorbidities, limiting interpretability [23, 24, 25]. To date, no clinical study has simultaneously examined Claudin-5 with peripheral inflammatory markers—NLR, PLR, MLR, and the INFLA score—in relation to suicidal ideation in an untreated adult MDD population. This present study addresses that gap by evaluating Claudin-5 as a peripheral marker of neurovascular integrity alongside systemic inflammation and suicidality, compared with age- and sex-matched healthy controls.
By integrating molecular and immunological biomarkers in an untreated clinical cohort, this study aims to clarify how neurovascular and inflammatory mechanisms contribute to MDD. Such an approach may inform the development of multidimensional biomarkers and novel therapeutic targets beyond symptom-based frameworks. Here, it is hypothesized that serum Claudin-5 levels should be lower in MDD patients than in controls and correlate with both suicidal ideation and inflammatory indices (NLR, PLR, MLR, INFLA score).
A total of 147 participants were included: 73 patients diagnosed with MDD and 74 age- and sex-matched healthy controls. All patients were recruited from the Psychiatry Outpatient Clinic of Muğla Training and Research Hospital and were evaluated during an acute depressive episode. None were hospitalized at the time of assessment. All patients were medication-free for at least three months, and both illness duration and episode history were recorded during the Structured Clinical Interview for DSM-5 Disorders (SCID-5) clinical interview and review of medical history. Based on this information, patients were classified as either first-episode (antidepressant-naive) or recurrent (with previous episodes but currently drug-free). Controls were recruited from hospital staff and community volunteers, matched for age and sex, and were free from any current or past psychiatric disorders or systemic illnesses (confirmed by SCID-5).
Participants were excluded if they had used any psychotropic or anti-inflammatory medications (e.g., antidepressants, antipsychotics, mood stabilizers, non-steroidal anti-inflammatory drugs (NSAIDs), or corticosteroids) or had experienced major physical trauma or surgery in the preceding three months. This restriction was implemented as both pharmacologic and physical factors significantly alter systemic inflammation and endothelial biomarkers.
Antidepressants and other psychotropic medications modulate cytokine production
(e.g., IL-6, TNF-
Additionally, tissue injury or surgical intervention activates immune responses and increases vascular permeability, with effects that may persist for months [28]. Therefore, a three-month washout period was applied to minimize residual influences of medications or recent systemic stressors and ensure that the measured biomarkers more accurately reflect the underlying pathophysiology of MDD.
Clinical raters administering the Hamilton Depression Rating Scale (HAM-D) and Beck Scale for Suicide Ideation (BSSI) were independent psychiatrists blinded to the diagnostic status of participants, laboratory data, and study hypotheses. Group assignments (MDD vs. control) were coded by a research assistant not involved in assessment or analysis, and all rating sessions were conducted using standardized instructions without access to demographic or biochemical information. Laboratory personnel analyzing serum Claudin-5, CRP, and hematologic parameters were likewise blinded to all clinical information and received only anonymized sample codes. Data coding and blinding were maintained until completion of statistical analysis, after which group labels were re-linked by an independent investigator for final reporting.
All participants were evaluated using the SCID-5, a semi-structured diagnostic tool widely used in psychiatric research to ensure standardized assessment and diagnostic reliability. The Turkish validity and reliability study was conducted by Elbir et al. [29].
A semi-structured form developed by the researchers was used to record participants’ demographic and clinical characteristics, including age, gender, education, marital status, comorbidities, substance use, treatment history, and suicidal ideation or attempts.
The HAM-D, developed by Hamilton (1960), is a clinician-rated scale assessing
depression severity across 21 items, including mood, guilt, suicidality, sleep,
somatic symptoms, and insight. Total scores (0–51) indicate severity: 0–7 =
none, 8–15 = mild, 16–28 = moderate,
Suicidal ideation was evaluated using both a clinical interview and the BSSI, a 21-item clinician-rated scale assessing passive and active suicidal thoughts, intent and planning. Items are scored 0–2 (total = 0–38), with higher scores indicating greater severity. Developed by Beck et al. [31], its Turkish version was validated by Ozcelik et al. [32].
The psychometric instruments (SCID-5, HAM-D, and BSSI) were administered face-to-face by board-certified psychiatrists experienced in the use of standardized rating scales and trained in the SCID-5. The same psychiatrists conducted all assessments in a consistent, blinded manner to ensure inter-rater reliability and procedural standardization across participants.
After a 12-hour overnight fast, venous blood samples were collected between
08:00 and 10:00 AM for complete blood count (CBC), CRP, and Claudin-5 analysis.
CBC samples were drawn into ethylenediaminetetraacetic acid (EDTA) tubes and
CRP/Claudin-5 samples into gel-separator tubes, then centrifuged at 1300
CBC was analyzed using an automated hematology analyzer (SP-50, Sysmex Corporation, Kobe, Japan). From CBC data, NLR, MLR, and PLR ratios were calculated. CRP levels were measured via immunoturbidimetry (Cobas c-701, Roche Diagnostics, Basel, Switzerland).
Serum Claudin-5 concentrations were determined by enzyme-linked immunosorbent assay using a commercial kit (BT LAB, Shanghai, China; Cat. No. E2303Hu; detection range 20–4500 ng/L, sensitivity 9.51 ng/L), following the manufacturer’s protocol.
The INFLA-score, originally proposed by Bonaccio et al. [33], combines CRP, white blood cell (WBC) count, platelet count, and granulocyte-to-lymphocyte ratio into a composite index of low-grade inflammation (range –16 to +16, higher values indicating greater inflammation). It has been validated in large population-based cohorts and shown to correlate with depressive symptoms, supporting its use as an integrated marker of systemic inflammation in depression [33, 34].
Sample size estimation with G*Power 3.1 (Heinrich Heine University,
Düsseldorf, Germany) indicated that 71 participants per group were required
to detect a medium effect size (Cohen’s d = 0.5) with 80% power at
Analyses were conducted in IBM SPSS Statistics 26.0 (IBM Corp., Armonk, NY,
USA). Descriptive data were summarized as mean
Multivariate logistic regression identified independent predictors of suicidal ideation within the MDD group. Analyses for depression severity (HAM-D) and diagnostic status (MDD vs. control) were not performed, as the former showed limited within-group variance and the latter was already examined in group comparisons. Receiver operating characteristic (ROC) analyses assessed the diagnostic accuracy of Claudin-5 and inflammatory indices for differentiating patients from controls and exploring their predictive value for suicidal ideation. Although group-level differences were nonsignificant, these exploratory analyses aimed to assess potential individual-level discriminative ability.
Variables included Claudin-5, NLR, INFLA score, and family history of
psychiatric illness, selected a priori based on theoretical and
empirical relevance and univariate associations (p
Effect sizes were interpreted according to Cohen’s criteria: small (d
A total of 160 individuals were screened for eligibility; 13 were excluded (eight not meeting inclusion criteria and five declining participation). Consequently, 147 participants were included in the final analysis, comprising 73 patients with MDD and 74 healthy controls. Among the 73 patients with MDD, 28 (38.4%) were first-episode, antidepressant-naive cases, and 45 (61.6%) were recurrent patients with a history of previous antidepressant treatment but medication-free for at least three months. Thirteen patients (17.8%) had a history of suicide attempt, and 22 patients (30.1%) exhibited current active suicidal ideation at the time of assessment (Fig. 1). The patient and control groups were comparable in age, sex, marital status, residence, and living status, while patients had lower educational attainment, higher unemployment, and greater smoking prevalence (Table 1, Ref. [35]).
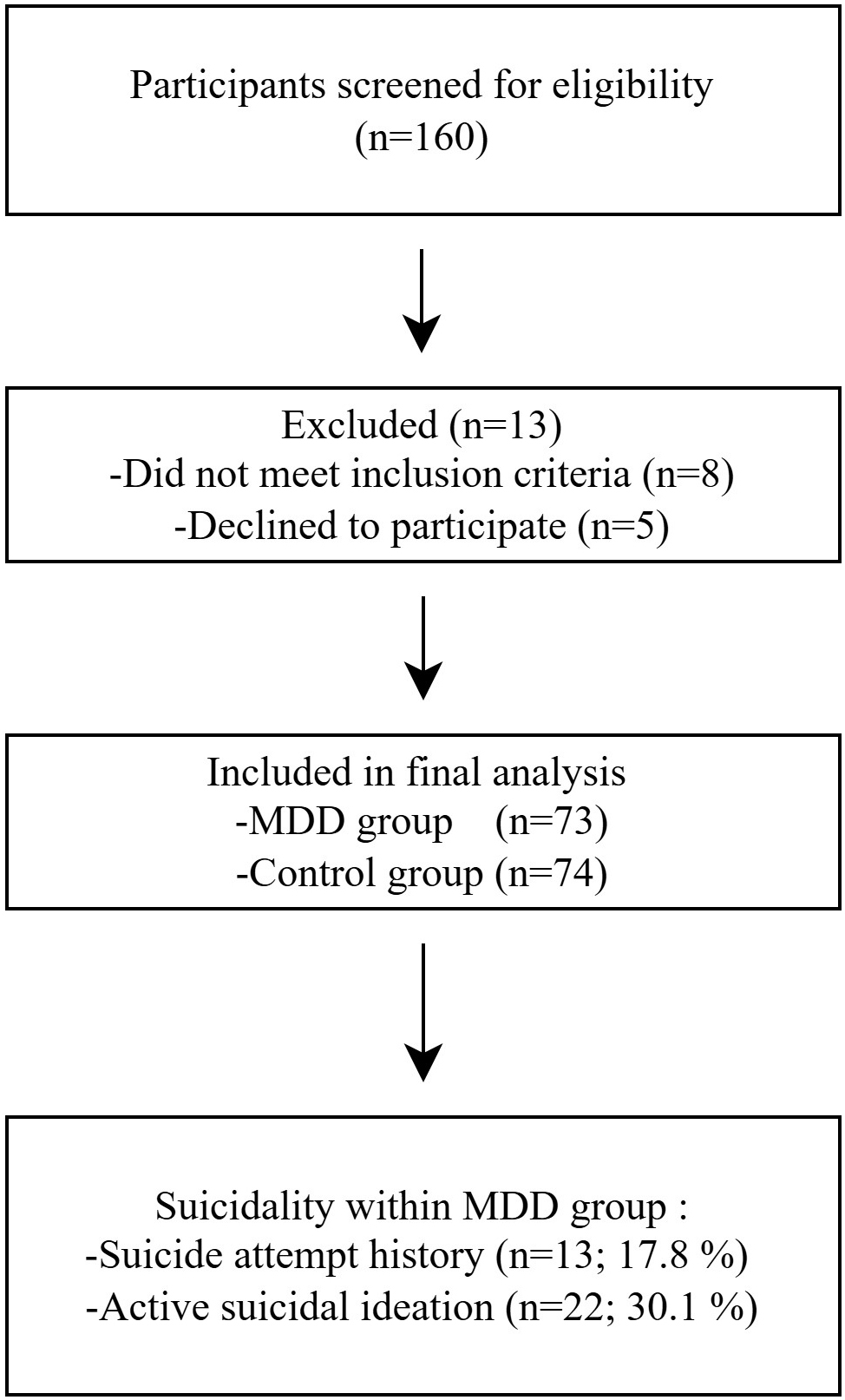 Fig. 1.
Fig. 1.
Flow Diagram of Participant in the Case–Control Study. MDD, Major depressive disorder.
| Variables | Patient (n = 73) | % | Control (n = 74) | % | p-value | Effect size | |
| n | n | ||||||
| Sex | 0.307 | 0.093 | |||||
| Female | 49 | 67.1 | 43 | 58.1 | |||
| Male | 24 | 32.9 | 31 | 41.9 | |||
| Marital Status | 0.181 | 0.182 | |||||
| Single | 33 | 45.2 | 30 | 40.5 | |||
| Married | 33 | 45.2 | 42 | 56.8 | |||
| Divorced/Widowed | 7 | 9.6 | 2 | 2.7 | |||
| Education Level | 0.287 | ||||||
| Primary | 24 | 32.9 | 7 | 9.5 | |||
| Secondary and Higher | 49 | 67.1 | 67 | 90.5 | |||
| Living Status | 0.393 | 0.070 | |||||
| Living alone | 19 | 26.0 | 24 | 32.4 | |||
| Not living alone | 54 | 74.0 | 50 | 67.6 | |||
| Residence | 0.087 | 0.146 | |||||
| Rural | 17 | 23.3 | 9 | 12.2 | |||
| Urban | 56 | 76.7 | 65 | 87.8 | |||
| Employment Status | 0.432 | ||||||
| Employed | 32 | 43.8 | 63 | 85.1 | |||
| Unemployed | 41 | 56.2 | 11 | 14.9 | |||
| Occupation | - | - | |||||
| Civil Servant | 12 | 16.4 | 48 | 64.8 | |||
| Worker | 12 | 16.4 | 11 | 14.9 | |||
| Student | 12 | 16.4 | 9 | 12.2 | |||
| Tradesperson | 5 | 6.9 | 2 | 2.7 | |||
| Other | 22 | 30.2 | 4 | 5.4 | |||
| None | 10 | 13.7 | - | - | |||
| BMI Group (n = 145) | 0.652 | 0.067 | |||||
| Underweight | 5 | 6.8 | 3 | 4.2 | |||
| Normal weight | 33 | 45.3 | 37 | 51.4 | |||
| Overweight | 35 | 47.9 | 32 | 44.4 | |||
| Smoking Status | 0.277 | ||||||
| Smoker | 35 | 47.9 | 16 | 21.6 | |||
| Non-smoker | 38 | 52.1 | 58 | 78.4 | |||
Note: Chi-square tests were used for categorical variables unless otherwise
specified. Effect sizes (Cramér’s V) were interpreted as small
(0.10), medium (0.30), and large (0.50) according to Cohen [35]. Occupational
status was excluded from statistical analysis due to empty cells in certain
categories. Significance is assumed for p
Serum biomarker analyses revealed significantly lower Claudin-5 levels and elevated NLR, PLR, CRP, and INFLA scores in patients compared to controls, whereas MLR did not differ (Table 2, Ref. [35]). When patients were further divided into first-episode (antidepressant-naive) and recurrent subgroups, no significant differences were found in Claudin-5 or inflammatory indices, indicating that these alterations were consistent across both subgroups. Claudin-5 levels were not significantly associated with sociodemographic or clinical characteristics, although a nonsignificant trend toward higher values in mild depression was noted.
| Variable | Group | Mean |
Median | Min | Max | p-value | Effect size |
| Claudin-5 (ng/L) | Patients | 1137.11 |
797.30 | 401.30 | 3324.00 | 0.891 | |
| Controls | 1888.66 |
1895.50 | 218.90 | 3363.00 | |||
| MLR | Patients | 0.06 |
0.02 | 0.00 | 0.40 | 0.144 | 0.106 |
| Controls | 0.07 |
0.02 | 0.00 | 0.50 | |||
| NLR | Patients | 2.23 |
2.00 | 0.90 | 8.90 | 0.829 | |
| Controls | 1.55 |
1.50 | 0.80 | 3.60 | |||
| PLR | Patients | 133.95 |
123.40 | 64.00 | 277.00 | 0.032* | 0.368 |
| Controls | 118.25 |
111.30 | 65.00 | 261.00 | |||
| CRP (mg/L) | Patients | 3.10 |
1.40 | 1.00 | 18.00 | 0.003* | 0.571 |
| Controls | 1.56 |
0.70 | 0.00 | 9.00 | |||
| INFLA score | Patients | 2.14 |
2.00 | –12.00 | 15.00 | 1.055 | |
| Controls | –3.03 |
–4.00 | –7.00 | 4.00 |
Note: Values are presented as (mean
PLR and INFLA scores correlated positively with HAM-D scores (r =
0.289, p = 0.013; r = 0.296, p = 0.011), but these
associations did not remain significant after Bonferroni correction (adjusted
| Variables | HAM-D score | BSSI score |
| Pearson r (p) | Pearson r (p) | |
| Claudin-5 level | −0.084 (0.479) | −0.069 (0.560) |
| MLR | 0.001 (0.996) | −0.003 (0.977) |
| NLR | 0.207 (0.078) | 0.079 (0.507) |
| PLR | 0.289 (0.013)* | 0.190 (0.107) |
| CRP | 0.001 (0.992) | −0.085 (0.475) |
| INFLA score | 0.296 (0.011)* | 0.038 (0.752) |
Note: Pearson correlation coefficient (r) and p-value (p) are given. Statistically significant correlations are indicated by an asterisk (*). HAM-D, Hamilton Depression Rating Scale; BSSI, Beck Scale for Suicide Ideation.
In additional analyses, none of the inflammatory indices showed significant correlations with BSSI Score, including MLR (r = –0.003, p = 0.977), NLR (r = 0.079, p = 0.507), PLR (r = 0.190, p = 0.107), CRP (r = –0.085, p = 0.475), and the INFLA score (r = 0.038, p = 0.752) (Table 3).
Patients with and without active suicidal ideation did not differ in Claudin-5 or inflammatory markers (Table 4, Ref. [35]).
| Variables | Active suicidal ideation present (n = 22) | Active suicidal ideation absent (n = 51) | p-value | Effect size (r) |
| Median (min–max) | Median (min–max) | |||
| Claudin-5 level | 834.900 (401.300–3324.000) | 774.900 (511.100–3183.000) | 0.697 | 0.040 |
| MLR | 0.027 (0.000–0.310) | 0.026 (0.000–0.460) | 0.197 | 0.130 |
| NLR | 2.120 (1.200–8.900) | 2.010 (0.900–4.200) | 0.446 | 0.320 |
| PLR | 126.840 (94.000–277.000) | 123.190 (64.000–260.000) | 0.228 | 0.370 |
| CRP | 1.410 (1.000–10.000) | 1.410 (1.000–18.000) | 0.651 | 0.010 |
| INFLA score | 4.000 (−6.000–15.000) | 2.000 (−12.000–12.000) | 0.264 | 0.290 |
Note: Values are presented as median (min–max). Mann–Whitney U test
was used to compare groups with and without suicidal ideation. Effect sizes (r)
were interpreted according to Cohen [35], as small (0.10), medium (0.30), and
large (0.50). p
ROC analysis demonstrated that Claudin-5 had fair diagnostic accuracy for
distinguishing patients from controls (AUC = 0.737) (Table 5A, Ref. [36]) (Fig. 2), but limited value for predicting suicidal ideation (AUC = 0.628) (Table 5A,
Fig. 3). When Claudin-5, NLR, and INFLA scores were entered together into a
composite ROC model, the model retained fair diagnostic accuracy (AUC = 0.720,
p
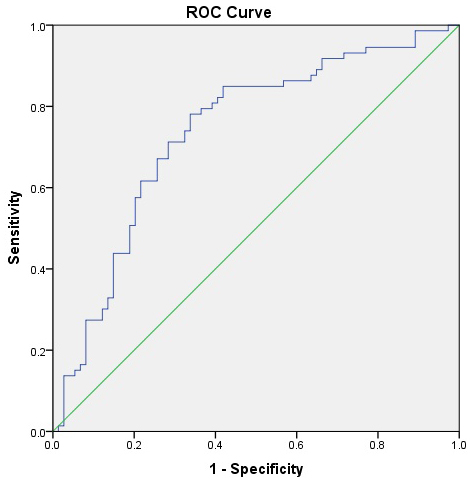 Fig. 2.
Fig. 2.
ROC curve for Claudin-5 distinguishing patients with
major depressive disorder (MDD) from healthy controls. The AUC was 0.737 (95%
CI: 0.655–0.819, p
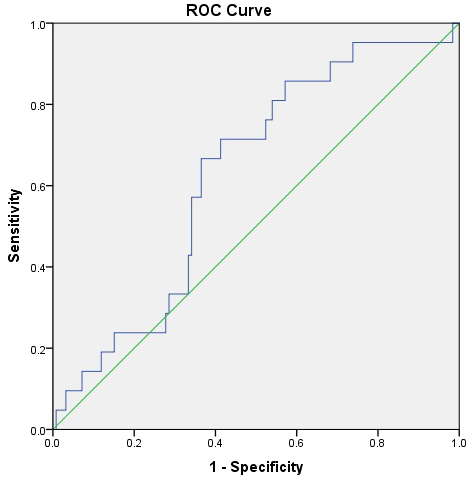 Fig. 3.
Fig. 3.
ROC curve for Claudin-5 predicting the presence of suicidal ideation among patients with major depressive disorder (MDD). The AUC was 0.628 (95% CI: 0.512–0.744, p = 0.061), suggesting limited discriminative power for suicidal ideation.
| Risk factor | Outcome | AUC (95% CI) | Cut-off | p-value | Sensitivity/Specificity |
| Claudin-5 | Depression Presence | 0.737 (0.655–0.819) | 1134.0 | 71.2%/71.6% | |
| Claudin-5 | Suicidal Ideation | 0.628 (0.512–0.744) | 910.25 | 0.061 | 61.9%/63.5% |
Note. Claudin-5 levels were tested for discriminating major depressive disorder
vs. control status and the presence of suicidal ideation. Optimal cut-off values
were determined using Youden’s index. Significance is accepted for p
| Model | AUC (95% CI) | p-value | Sensitivity/Specificity |
| Claudin-5 + NLR + INFLA | 0.720 (0.637–0.803) | 72.5%/70.3% |
Note. Composite model derived from binary logistic regression using predicted probabilities.
| Variable | 95% CI | p-value | |
| Claudin-5 (ng/L) | –0.145 | −0.312–0.025 | 0.091 |
| NLR | 0.232 | 0.045–0.382 | 0.011* |
| INFLA Score | 0.198 | 0.014–0.332 | 0.037* |
| Family History (Yes/No) | 0.102 | −0.034–0.229 | 0.131 |
Note. Standardized beta coefficients (
This study demonstrated that serum Claudin-5 levels were significantly lower in patients with MDD who had either never used antidepressants or had been medication-free for at least three months, while no significant associations were found between Claudin-5 and symptom severity, suicidal ideation, or inflammatory markers. Beyond statistical significance, several group differences—particularly the reductions in Claudin-5 and elevations in NLR—showed medium-to-large effect sizes, suggesting that these alterations may hold clinical as well as statistical significance. To the author’s knowledge, this is the first study to assess serum Claudin-5 alongside inflammatory indices and suicidal ideation in untreated adults with MDD, providing new insights into its neurovascular pathophysiology.
Groups were matched for age, sex, and body mass index (BMI), reducing demographic confounding. Although unemployment and smoking were slightly higher in MDD, these factors are unlikely to explain the biochemical differences observed.
Claudin-5, which is crucial for BBB integrity, has been implicated in several neuropsychiatric disorders, including MDD [12, 13, 16]. These findings align with recent evidence on tight-junction proteins in psychiatry: A 2025 systematic review reported altered Claudin-5 and occludin levels across major psychiatric disorders, supporting BBB involvement beyond single-study findings and diagnostic categories [24].
The findings reported here of reduced serum Claudin-5 levels are consistent with previous postmortem and preclinical studies showing downregulation in the hippocampus and nucleus accumbens of depressed individuals [12, 13]. A drug-free cohort minimized medication effects; elevated Claudin-5 in medicated or adolescent samples, and likely reflects treatment or developmental influences [37, 38, 39]. Additionally, genetic and molecular vulnerabilities involving Claudin-5 and other blood–brain barrier–related pathways have been associated with cognitive and affective disturbances, suggesting a broader etiological role for tight-junction dysregulation in mood disorders [16, 39, 40].
No significant associations were found between serum Claudin-5 levels and depression severity, suicidal ideation, or duration of untreated symptoms. This suggests that Claudin-5 reflects relatively stable cerebrovascular alterations rather than acute, state-dependent changes. While imaging and experimental studies have reported BBB permeability changes correlating with symptom severity, peripheral markers such as Claudin-5 may only partially reflect such central neurovascular dynamics [11, 40, 41]. The BBB is a complex multicellular structure involving pericytes, astrocytes, and immune modulators; thus, single protein measures may not capture its full functional integrity.
The absence of correlation between Claudin-5 or inflammatory indices and depression severity may reflect their different temporal and biological characteristics. Claudin-5 may represent a relatively stable marker of endothelial integrity, indicating a persistent neurovascular vulnerability, whereas systemic indices such as NLR, PLR, and MLR are state-dependent and fluctuate with short-term physiological or psychosocial stress. Their lack of association with depression severity in this cross-sectional sample may reflect temporal immune variability and depressive heterogeneity rather than a lack of pathophysiological relevance. Overall, these findings suggest that Claudin-5 and inflammatory markers capture distinct yet complementary dimensions of neurovascular and immune dysregulation in MDD [3, 40, 42].
The current findings are in line with several previous studies reporting reduced Claudin-5 expression in both clinical and preclinical models of depression. For instance, Menard et al. [13] and Dion-Albert et al. [12] demonstrated stress-induced downregulation of Claudin-5 in animal models and in unmedicated depressed individuals. Similarly, lower circulating levels of other tight-junction proteins such as occludin and zonulin have been observed in mood and psychotic disorders [17, 24]. Conversely, studies involving medicated or adolescent samples have sometimes found elevated Claudin-5, likely reflecting treatment or developmental effects [24, 37, 38]. Together, these findings reinforce the hypothesis that endothelial dysfunction and altered BBB integrity are common biological features across major psychiatric conditions.
Mechanistically, chronic inflammation may contribute to BBB disruption through
cytokine-mediated pathways. Experimental studies have shown that pro-inflammatory
cytokines such as IL-6 and TNF-
Although PLR and INFLA scores showed positive correlations with depression severity, these associations did not remain significant after Bonferroni correction, suggesting that they should be interpreted as trend-level findings. Future studies with larger samples are needed to confirm these relationships.
To further contextualize Claudin-5 within neuroimmune mechanisms and its
relationship with inflammatory markers, it was found that MDD patients exhibited
significantly elevated NLR, PLR, CRP, and INFLA scores compared to healthy
controls (p
Hematologic indices such as the NLR and PLR are non-specific and may be influenced by lifestyle or metabolic factors (e.g., smoking, obesity, stress). Although smoking and unemployment were more frequent in the MDD group, these factors did not significantly affect inflammatory marker or Claudin-5 levels, and the group difference in Claudin-5 remained significant after accounting for them. Still, residual confounding cannot be excluded, and future studies should control for such variables.
Experimental studies indicate that inflammatory cytokines such as
TNF-
Overall, Claudin-5 appears to be a promising but complex biomarker of neurovascular dysfunction in MDD. Its peripheral concentrations may reflect more stable endothelial traits rather than fluctuating clinical states, and its role should be explored further through multimodal and longitudinal research integrating central and peripheral assessments.
Subgroup analysis comparing first-episode and recurrent MDD patients showed no significant differences in Claudin-5 or inflammatory indices (MLR, NLR, PLR, CRP, INFLA score). These results suggest that neurovascular and inflammatory alterations in MDD are not strongly affected by illness chronicity or recent treatment, supporting Claudin-5 as a relatively stable endothelial marker in untreated MDD.
Although this is the first study to assess Claudin-5 in drug-free adult MDD patients alongside inflammatory markers and suicidal ideation, the findings reported here suggest that Claudin-5 alone has limited predictive value as a biomarker of suicide risk. In ROC analysis, serum Claudin-5 demonstrated moderate accuracy in differentiating MDD patients from healthy controls (AUC = 0.737, p = 0.001), aligning with earlier findings in adolescent populations [38]. However, its ability to predict suicidal ideation was weak (AUC = 0.628), suggesting that Claudin-5 alone may not significantly serve as a reliable standalone marker for suicide risk assessment.
Multivariate logistic regression revealed that NLR and INFLA score were significant independent predictors of suicidal ideation, consistent with prior research highlighting systemic inflammation as a key contributor to suicide vulnerability [18, 25]. Consistent with these multivariable results, a recent meta-analysis has shown that immune-related biomarkers differ between individuals with and without suicidal behaviors, reinforcing the clinical relevance of systemic inflammation in suicide vulnerability [25, 46]. Interestingly, although NLR and INFLA score did not show significant differences between patients with and without suicidal ideation in univariate comparisons, both emerged as independent predictors in multivariate regression. This discrepancy likely reflects the fact that regression analysis accounts for potential confounders and reveals underlying associations that simple group comparisons may obscure. In this context, systemic inflammation may exert a subtle but clinically meaningful influence on suicidal vulnerability, which becomes more evident when considered alongside other biological and clinical variables. These findings emphasize the importance of using multivariable approaches to capture the complex interplay between inflammation and suicidality in MDD.
Importantly, when Claudin-5 was combined with NLR and INFLA score in a composite
biomarker model (Table 5B), the model retained fair diagnostic accuracy (AUC =
0.720, p
Given their low cost and accessibility, NLR and INFLA score could be readily integrated into clinical risk assessment protocols for suicide in psychiatric settings. Moreover, the inclusion of Claudin-5 alongside inflammatory markers may enhance the biological specificity of such models. Emerging research on gut–brain–microbiome interactions suggests that peripheral barrier dysfunction (“leaky gut”) may interact with BBB disruption and inflammatory pathways, further linking systemic and neurovascular processes in depression and suicidality [8, 40, 49]. Future prospective and neuroimaging studies are needed to further explore the combined role of Claudin-5 and inflammatory indices in MDD. If validated in future studies, Claudin-5 and inflammatory indices such as NLR and INFLA score could potentially serve as peripheral biomarkers for refining biological subtypes of depression and identifying patients at heightened suicide risk.
This study has several strengths, including drug-naive or medication-free MDD patients, which allowed an unconfounded assessment of peripheral Claudin-5 levels. The use of age- and sex-matched controls improved internal validity, while simultaneous evaluation of depressive severity, suicidality, and inflammatory indices provided a multidimensional view of Claudin-5’s clinical relevance. Together, these findings support its role in neurovascular dysregulation and its potential as a peripheral marker of BBB dysfunction in depression.
However, several limitations warrant consideration. The cross-sectional design
precludes causal inference, and serum Claudin-5 may not fully represent central
levels. Neuroimaging methods such as dynamic contrast-enhanced MRI were not used
to confirm BBB permeability. Although the total sample size was adequate for
medium effects, subgroup analyses (e.g., suicidality) were likely underpowered;
detecting small-to-moderate effects (d = 0.3, 80% power,
This study provides preliminary but important evidence that serum Claudin-5 levels are significantly reduced in untreated patients with MDD, possibly indicating relatively stable endothelial alterations rather than acute, state-dependent changes. While Claudin-5 alone showed limited utility for predicting symptom severity or suicide risk, peripheral inflammatory markers such as NLR and INFLA scores were independently associated with suicidal ideation. Although the composite biomarker model combining Claudin-5 with inflammatory indices did not improve predictive performance compared with Claudin-5 alone, these markers may offer complementary biological information reflecting distinct neurovascular and inflammatory mechanisms. Future longitudinal and multimodal studies are warranted to confirm these findings and to develop integrated biomarker approaches for depression and suicidality.
This article is based on the medical specialty thesis titled “Comparison of Serum Claudin-5 Levels in Patients with Major Depressive Disorder and Healthy Controls: Evaluation of the Relationship Between Serum Claudin-5 Levels, Suicidal Ideation, Anxiety Severity, and Systemic Inflammatory Parameters”, conducted by Nurbanu Keskin at Muğla Sıtkı Koçman University Training and Research Hospital under the supervision of primary advisor Mahmut Selçuk and secondary advisor Ercan Saruhan.
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
NK: Conceptualization, Methodology, Data Collection, Formal Analysis, Writing–Original Draft. MS: Conceptualization, Methodology, Supervision, Writing–Original Draft, Review & Editing, Validation. ES: Formal Analysis, Supervision, Methodological Guidance, Review & Editing. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study protocol was approved by the Non-Invasive Clinical Research Ethics Committee of İzmir Bakırçay University (Decision No: 1786, Date: 02/10/2024). All procedures were conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.