



 , Sha Nie 1,2,†, Rong Zeng 1,2,†, Jian-Xin Mai 1,2, Xiong Huang 1,2, Shi-Chao Xu 1,2, Xin-Hu Yang 1,2, Qing-Bin Zeng 3, Xing-Bing Huang 1,2,*
, Sha Nie 1,2,†, Rong Zeng 1,2,†, Jian-Xin Mai 1,2, Xiong Huang 1,2, Shi-Chao Xu 1,2, Xin-Hu Yang 1,2, Qing-Bin Zeng 3, Xing-Bing Huang 1,2,* , Wei Zheng 1,2,*
, Wei Zheng 1,2,*1 Department of Psychiatry, The Affiliated Brain Hospital, Guangzhou Medical University, 510370 Guangzhou, Guangdong, China
2 Key Laboratory of Neurogenetics and Channelopathies of Guangdong Province and the Ministry of Education of China, Guangzhou Medical University, 510370 Guangzhou, Guangdong, China
3 Department of Psychiatry, The Third People’s Hospital of Foshan, 528041 Foshan, Guangdong, China
†These authors contributed equally.
Abstract
Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE) technique prolongs apnea duration. However, there is limited knowledge regarding the effectiveness and safety of THRIVE technique compared to conventional facemask ventilation during electroconvulsive therapy (ECT) in Chinese patients with major mental disorders.
Seventy adult individuals with major mental disorders (schizophrenia, n = 17; bipolar disorder, n = 25; major depressive disorder, n = 28) undergoing their first ECT session were assigned to either the THRIVE group (n = 35) or the facemask group (n = 35) based on the random sequence. The primary outcome was the lowest peripheral oxygen saturation (SpO2) levels. Secondary outcomes included the incidence of oxygen desaturation, electroencephalogram seizure duration, stimulation dosage, mean arterial pressure (MAP), average SpO2 levels, and heart rate (HR). Airway-related complications were documented within 24 hours following ECT.
In the THRIVE group, the lowest SpO2 levels were notably higher than those in the facemask group (p < 0.05). Patients receiving THRIVE technique had consistently higher average SpO2 levels than those receiving conventional facemask ventilation (p < 0.05). The incidence of oxygen desaturation in THRIVE group was lower than that in facemask group (p > 0.05). Moreover, significant differences between two study groups were not observed in terms of electroencephalogram seizure duration, stimulation dosage, MAP, and HR (all ps > 0.05). No airway-related complications were reported in either group.
In this preliminary open-label randomized controlled trial, the THRIVE technique appeared to be more effective than conventional facemask ventilation in preserving SpO2 levels during ECT in major mental disorders, establishing itself as a safe and effective oxygenation alternative.
No: ChiCTR2400084318, https://www.chictr.org.cn/showproj.html?proj=229304.
Keywords
- electroconvulsive therapy
- anesthesia
- transnasal humidified rapid-insufflation ventilatory exchange
- major mental disorders
(1) The Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE) technique is a novel intraoperative ventilatory technique.
(2) This is the first study to examine the efficacy and safety of the THRIVE technique compared to conventional facemask ventilation in Chinese patients with major mental disorders during electroconvulsive therapy (ECT) procedure.
(3) The THRIVE technique demonstrates superiority over conventional facemask ventilation in preserving peripheral oxygen saturation levels during the ECT procedure.
Electroconvulsive therapy (ECT) is a noninvasive brain stimulation (NIBS) technique. It has been considered an effective physical treatment for a broad spectrum of severe mental disorders [1, 2, 3]. To prevent injuries resulting from widespread epileptic seizures during the ECT procedure, patients must undergo general anesthesia [4, 5]. Conventional facemask ventilation has conventionally been the primary technique for airway management during ECT procedures; however, it may not be the optimal choice [6, 7]. When conventional facemask ventilation is used in ECT procedures, the incidence of oxygen desaturation could range from 2.5% to 29.0% [8, 9, 10, 11, 12]. Oxygen desaturation during ECT could shorten the seizure duration and even result in arrhythmias or myocardial infarction [13, 14]. Moreover, conventional facemask ventilation increases the risk of aspiration of gastric contents [15, 16]; it might be challenging for patients with facial tumors, large jaws, thick beards, or edentulous conditions [17, 18, 19]. Therefore, there is a need for the development of advanced airway devices and technologies.
Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE), a novel ventilation technique, involves supplying patients with warm, humidified, high-flow oxygen to prolong apneic oxygenation under general anesthesia [20, 21]. The THRIVE technique removes carbon dioxide (CO2) more efficiently than conventional apneic oxygenation, extending the safe apnea time [22, 23]. Previous studies have reported that safe apnea time maintained with the THRIVE technique ranges from 20 minutes to 65 minutes under general anesthesia [22, 24, 25]. When the THRIVE technique is used during the induction of anesthesia, it does not further increase the risk of gastric insufflation [26, 27]. The THRIVE technique is hands-free, allowing anesthesiologists to devote more attention to patient care. The method has found applications in various settings, such as laryngotracheal surgery [22, 28], rapid sequence intubation (RSI) [21, 29], and endoscopy [30, 31].
The safety and effectiveness of using the THRIVE technique during ECT procedures
have been demonstrated by several studies [27, 32, 33, 34], although with inconsistent
findings. For example, a non-randomized cross-over study involving 201 adult
participants with a body mass index (BMI) under 40 kg/m2 found a 0.5%
incidence of oxygen desaturation during ECT with the THRIVE technique [32].
However, Zhu et al. [27] reported a 5.3% incidence of desaturation
during ECT with the THRIVE technique in 150 adult patients with a BMI lower than
24 kg/m2. In most studies, the peripheral oxygen saturation (SpO2)
levels of all patients undergoing the THRIVE technique during ECT procedure
remained
In this preliminary open-label randomized controlled trial (RCT), participants
with major mental disorders (i.e., major depressive disorder (MDD), bipolar
disorder (BD), and schizophrenia) were divided into the THRIVE and facemask
groups during ECT procedures. This study primarily aimed to compare the efficacy
(i.e., SpO2 level
This study was a preliminary open-label RCT, which was carried out at the Affiliated Brain Hospital, Guangzhou Medical University, from 01 June 2024 until 01 August 2024. The Institutional Review Board (IRB) of the Affiliated Brain Hospital, Guangzhou Medical University, approved this trial (approval number: 2024034). The protocol was registered in the Clinical Trials Registry, China (registered number: ChiCTR2400084318) on May 14, 2024. The reporting of this study complied with the Consolidated Standards of Reporting Trials (CONSORT) guidelines [35]. All participants provided informed written consent. This study was conducted in compliance with the Declaration of Helsinki and national ethical regulations.
Participants were recruited from the inpatient unit of the Affiliated Brain Hospital, Guangzhou Medical University, a 1800-bed psychiatric treatment center located in Guangzhou, China. The eligibility criteria for this study included: (1) adult patients (aged 18–65 years) who had been diagnosed with schizophrenia, BD, or MDD according to the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-V); (2) patients with a BMI ranging from 18.5 to 23.9 kg/m2 [27]; (3) patients with American Society of Anesthesiologists (ASA) physical status I-II [36]; and (4) patients who were able to receive THRIVE technique following instructions properly.
The criteria for exclusion in this study included: (1) the presence of other psychiatric disorders as defined by DSM-V, such as alcohol or substance use disorder; (2) those suffering from obstructive sleep apnea syndrome (OSAS) along with nasopharyngeal abnormalities, epistaxis, or a history of nasal surgery; (3) known or anticipated airway obstruction requiring intubation; (4) patients suffering from severe or unstable somatic conditions (e.g., emphysema and chronic obstructive pulmonary disease); (5) pregnant or lactating individuals; and (6) contraindications to ECT or anesthesia.
Participants were recruited only for their first ECT session, during which ECT was administered using either the THRIVE technique or conventional facemask ventilation.
The sample size of 70 in this study was established according to a prior RCT (n = 70) that applied THRIVE for painless endoscopic mucosal resection of colorectal polyps [37]. The Statistical Package for the Social Sciences (SPSS) software (version 23.0, IBM SPSS Statistics for Windows, Armonk, NY, USA) was employed to generate the random sequence with a 1:1 ratio. A researcher, independent of the assessment and treatment processes, assigned patients to either the THRIVE group or the facemask group based on the random sequence. Due to the different appearance of the masks and high-flow nasal cannulas, it is not feasible for patients and assessors to be blinded.
Adult patients undergoing ECT received bilateral electrode placement using the Thymatron System IV device (Somatics LLC, Lake Bluff, IL, USA). The seizure threshold determination was based on the half-age dosing method, with the energy percentage calculated as the age multiplied by 0.5 [38]. After pre-oxygenation, all patients underwent general anesthesia following a standardized anesthesia protocol. Premedication anesthesia was induced by intravenous injection of atropine (0.5 mg) and propofol (1.5–2.0 mg/kg) before ECT administration. Once the patient became unconscious, intravenous succinylcholine (0.8–1.0 mg/kg) was administered to relax the muscles.
The Optiflow® THRIVE (Fisher & Paykel Healthcare, Auckland, New Zealand) is a humidifier with an integrated flow generator that delivers humidified, warmed, and high-flow oxygen at up to 70 L/min. Before using the THRIVE device, the humidifier must be heated for five minutes to reach a temperature of 37 °C [39]. Patients were fitted with appropriate high-flow nasal cannulas. During the 3-minute preoxygenation phase, 100% oxygen was administered at a flow rate of 30 L/min [36]. Exhalation was performed through the mouth, while inhalation was through the nose [33]. A flow rate of 70 L/min was maintained during apnea, even after administering muscle relaxants [33]. After sufficient spontaneous breathing, the flow rate was gradually reduced to 30 L/min and sustained at that level until the patient fully regained consciousness.
In the facemask group, preoxygenation with 100% oxygen was carried out for 3 minutes at a flow rate of 10 L/min, with no positive airway pressure applied, using an appropriately sized mask [21]. Immediately following the muscle relaxant injection, patients were ventilated using conventional facemasks and 100% oxygen until they fully regained consciousness. Until patients resumed spontaneous breathing, they received 100% oxygen using a mask, with a flow rate of 10 L/min.
All data were collected during the patients’ first ECT session. During the ECT procedure, specific time points were defined, including the baseline (T0), induction of anesthesia (T1), delivery of ECT stimulus (T2), recovery of spontaneous breathing (T3), and regaining consciousness (T4). At these designated time points (T0–T4), mean arterial pressure (MAP), heart rate (HR), and SpO2 levels were recorded.
The lowest SpO2 levels were continuously measured throughout the ECT
procedure using a pulse oximeter as the primary outcome [27, 33]. Secondary
outcomes encompassed the incidence of oxygen desaturation (defined as a SpO2
level
Airway-related complications, such as nose bleeds, nasal dryness, pain, and itching, were recorded for up to 24 hours following the ECT procedure.
All statistical analyses were conducted using the SPSS software (version 23.0,
IBM Corp., Armonk, NY, USA). The normal distribution of quantitative data was
assessed via the Shapiro–Wilk test. Quantitative data were properly presented as
either means and standard deviations (SD) or medians and interquartile ranges
(IQR), while qualitative data were described using frequency (N) and percentage
(%). Categorical variables were compared using either Pearson’s chi-square test
or Fisher’s exact test, while continuous variables were assessed through either
the Mann–Whitney U test or the independent samples t-test, as
appropriate. Linear mixed models with a Bonferroni correction were utilized to
compare HR, MAP, and SpO2 levels across multiple time points between the
THRIVE and the facemask groups. Statistical significance was set at p
The CONSORT flowchart detailing the recruitment process is presented in Fig. 1.
A total of 79 patients were assessed for eligibility. Of these, nine were
excluded (three refusals to participate and six non-fulfillments of inclusion
criteria). Finally, 70 patients with major mental disorders (schizophrenia, n =
17; BD, n = 25; MDD, n = 28) met the enrollment criteria for this study. Table 1
summarizes the clinical characteristics and demographics of the 70 patients who
underwent ECT, with 35 receiving conventional facemask ventilation and 35
receiving the THRIVE technique. In terms of sex, weight, hemoglobin levels, age,
baseline SpO2 levels, BMI, diagnosis, ASA grade, and education levels, there
were no significant differences between the THRIVE and facemask groups (all
ps
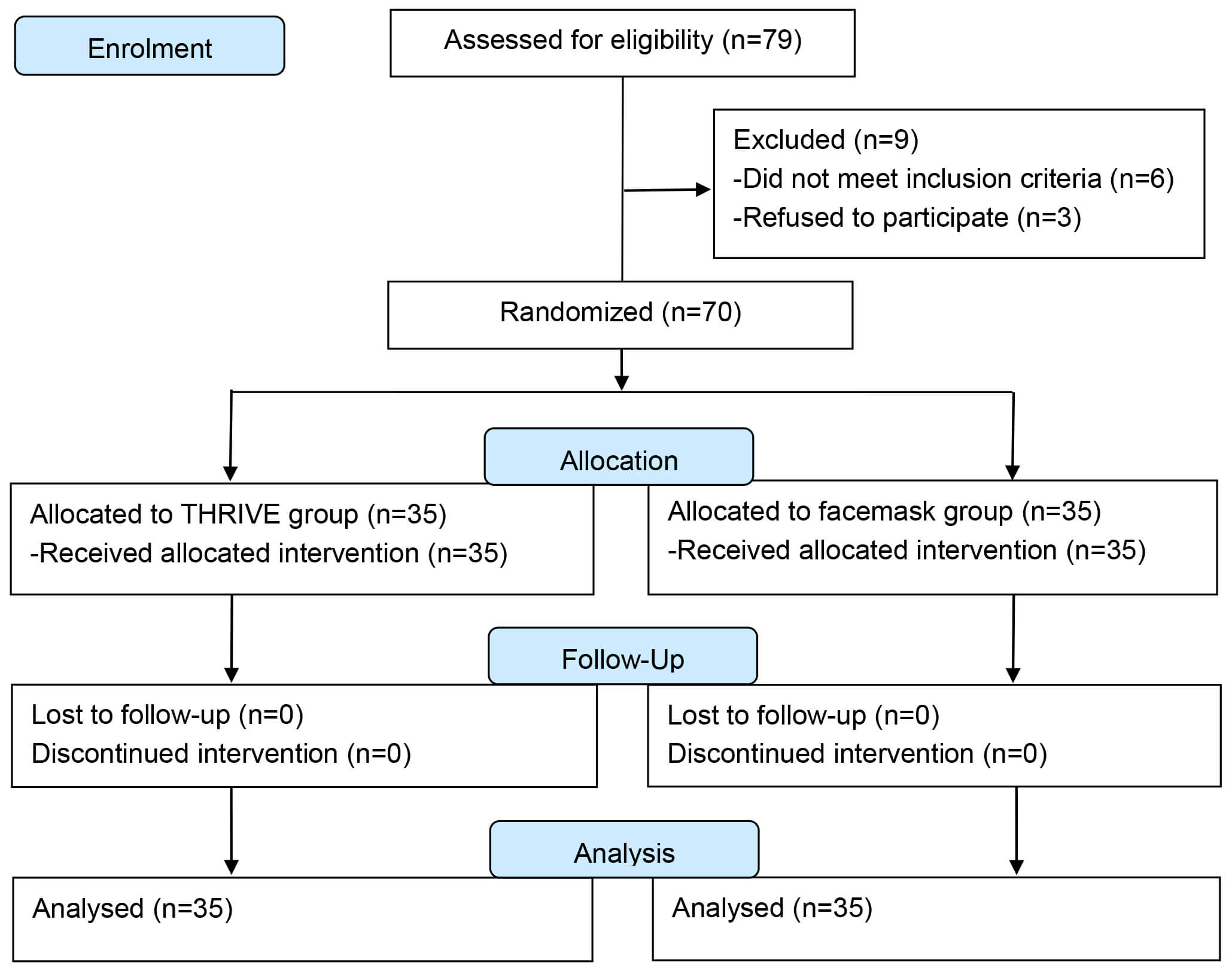 Fig. 1.
Fig. 1.
CONSORT flowchart of recruitment. CONSORT, Consolidated Standards of Reporting Trials; THRIVE, Transnasal Humidified Rapid-Insufflation Ventilatory Exchange.
| Variables | THRIVE group (n = 35) | Facemask group (n = 35) | Statistics | |||||
| Medians | IQR | Medians | IQR | z | df | p | ||
| Age (years) | 27.0 | 23.0, 39.0 | 28.0 | 22.0, 35.0 | 0.11 | —a | 0.916 | |
| Education (years) | 13.0 | 9.0, 15.0 | 15.0 | 9.0, 16.0 | –0.98 | —a | 0.329 | |
| Weight (kg) | 60.0 | 55.0, 67.0 | 54.0 | 51.0, 64.0 | 1.64 | —a | 0.101 | |
| Baseline SpO2 (%) | 98.0 | 97.0, 99.0 | 98.0 | 97.0, 98.0 | 0.98 | —a | 0.328 | |
| Variables | THRIVE group (n = 35) | Facemask group (n = 35) | Statistics | |||||
| Mean | SD | Mean | SD | t | df | p | ||
| BMI (kg/m2) | 21.2 | 1.7 | 20.9 | 1.7 | –0.79 | 68 | 0.433 | |
| Hemoglobin (g/L) | 135.4 | 15.9 | 129.7 | 13.9 | –1.59 | 68 | 0.116 | |
| Variables | THRIVE group (n = 35) | Facemask group (n = 35) | Statistics | |||||
| N | % | N | % | df | p | |||
| Male | 22 | 62.9 | 15 | 42.9 | 2.81 | 1 | 0.094 | |
| Diagnosis | 1.63 | 2 | 0.443 | |||||
| Schizophrenia | 8 | 22.9 | 9 | 25.7 | ||||
| BD | 15 | 42.9 | 10 | 28.6 | ||||
| MDD | 12 | 34.3 | 16 | 45.7 | ||||
| ASA grade | 0.08 | 1 | 0.780 | |||||
| I | 26 | 74.3 | 27 | 77.1 | ||||
| II | 9 | 25.7 | 8 | 22.9 | ||||
aMann–Whitney U test.
ASA, American Society of Anesthesiologists; BMI, body mass index; BD, bipolar
disorder; df, degree of freedom; IQR, interquartile range; MDD, major depressive
disorder; SpO2, peripheral oxygen saturation; SD, standard deviation;
The median lowest SpO2 levels in the THRIVE group were 98.0%
(IQR 97.0%–99.0%), which was notably higher than those
in the facemask group (97.0%; IQR 97.0%–98.0%) (p
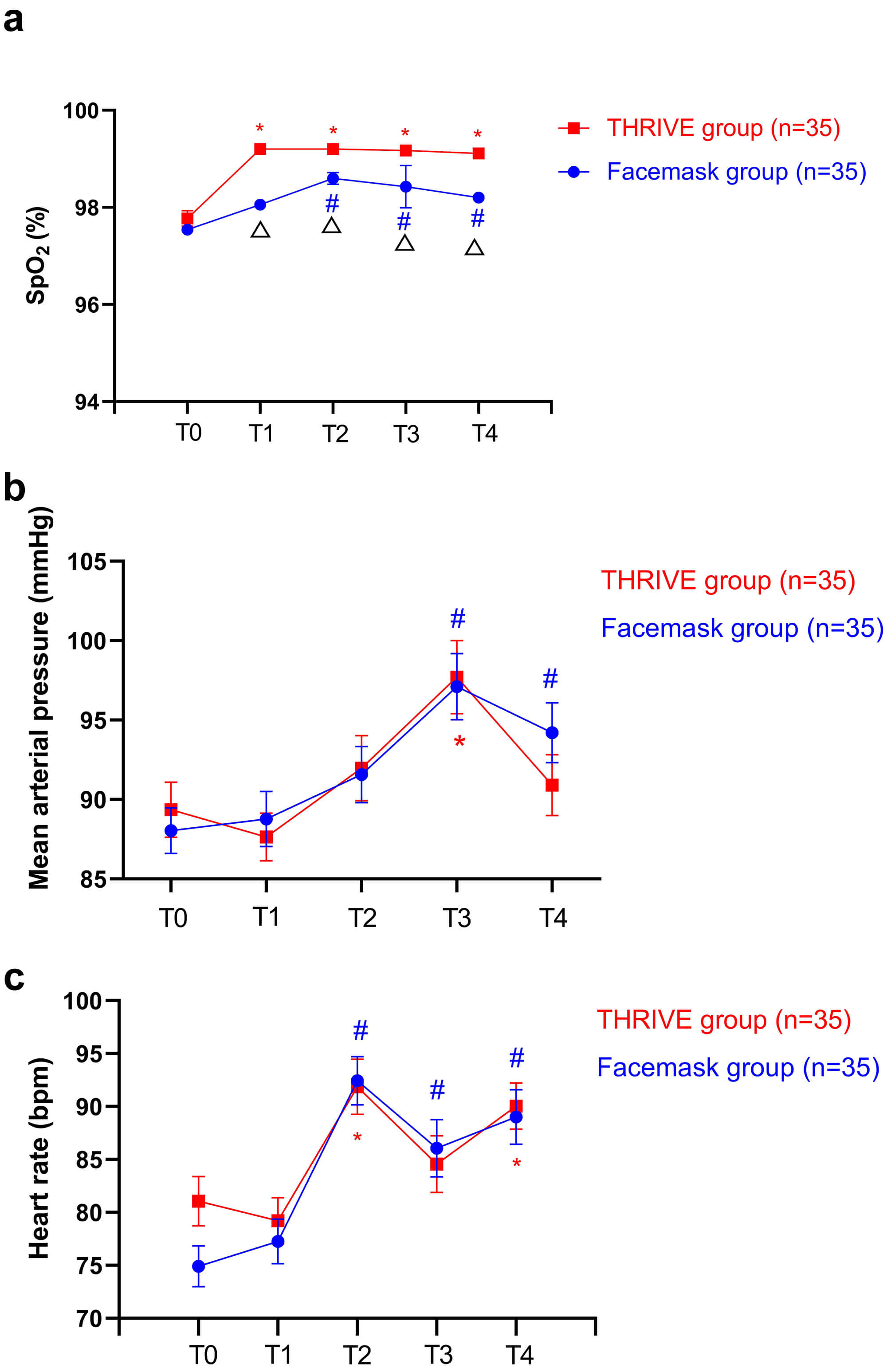 Fig. 2.
Fig. 2.
Changes in SpO2 (a), mean arterial pressure (b), and heart
rate (c) between the baseline and other timepoint in the THRIVE and facemask
groups.*Significantly different from the baseline in the THRIVE group (p
| Variables | THRIVE group (n = 35) | Facemask group (n = 35) | Statistics | |||||
| Medians | IQR | Medians | IQR | z | df | p | ||
| Lowest SpO2 levels during ECT procedure (%) | 98.0 | 97.0, 99.0 | 97.0 | 97.0, 98.0 | 3.54 | —a | ||
| Apnea duration (minutes) | 4.0 | 4.0, 6.0 | 5.0 | 4.0, 6.0 | –1.84 | —a | 0.066 | |
| Consciousness recovery time (minutes) | 10.0 | 9.0, 12.0 | 12.0 | 9.0, 13.0 | –1.35 | —a | 0.177 | |
| Propofol dosage (mg) | 110.0 | 100.0, 120.0 | 100.0 | 90.0, 110.0 | 1.48 | —a | 0.138 | |
| Succinylcholine dosage (mg) | 55.0 | 50.0, 60.0 | 50.0 | 45.0, 55.0 | 1.62 | —a | 0.106 | |
| ECT parameters | ||||||||
| Stimulation dosage (mC) | 120.0 | 96.0, 168.0 | 120.0 | 96.0, 168.0 | –0.13 | —a | 0.896 | |
| Pulse frequency (Hz) | 30.0 | 30.0, 30.0 | 30.0 | 30.0, 30.0 | –0.02 | —a | 0.982 | |
| Stimulus duration (seconds) | 2.5 | 2.3, 3.5 | 2.8 | 2.0, 3.3 | 0.15 | —a | 0.881 | |
| EEG seizure duration (seconds) | 25.0 | 22.0, 32.0 | 25.0 | 20.0, 40.0 | –0.24 | —a | 0.813 | |
| Variables | THRIVE group (n = 35) | Facemask group (n = 35) | Statistics | |||||
| N | % | N | % | df | p | |||
| SpO2 levels |
0 | 0 | 1 | 2.9 | —b | —b | 1.000 | |
The bolded values are p
aMann–Whitney U test.
bFisher’s exact test.
df, degree of freedom; ECT, electroconvulsive therapy; EEG, electroencephalogram.
| Variables | Group-by-time interaction | Time main effect | Group main effect | |||
| F | p | F | p | F | p | |
| SpO2 (%) | 2.2 | 0.065 | 18.9 | 29.1 | ||
| Mean arterial pressure (mm/Hg) | 1.0 | 0.407 | 16.2 | 0 | 0.838 | |
| Heart rate (beats per minute) | 1.4 | 0.246 | 25.8 | 1.1 | 0.303 | |
The bolded values are p
Significant differences were not observed between the THRIVE group and facemask
group regarding anesthetic outcomes, including apnea duration, consciousness
recovery time, propofol dosage, and succinylcholine dosage (all ps
Fig. 2 compares MAP and HR changes between the groups during the ECT procedure.
At T3, both groups exhibited the most significant increase in MAP (THRIVE
group versus facemask group: 97.7
Within 24 hours following the ECT procedure, none of the patients in the THRIVE or facemask groups reported airway-related complications, such as nose bleeds, nasal dryness, pain, or itching.
To the best of our knowledge, this study represents the first examination of the safety and efficacy of the THRIVE technique compared to conventional facemask ventilation in Chinese patients diagnosed with MDD, BD, and schizophrenia during the ECT procedure. The main findings of this study include: (1) patients in the THRIVE group exhibited notably higher levels of the lowest SpO2 and average SpO2 throughout the ECT procedure when compared to the facemask group; (2) the incidence of oxygen desaturation in the THRIVE group was lower than that in the facemask group, while this difference did not reach significance; (3) there were no significant differences between the two groups regarding EEG seizure duration, stimulation dosage, MAP, and HR; and (4) no airway-related complications were recorded in either the THRIVE or facemask groups within 24 hours following the ECT procedure.
In this study, using the THRIVE technique under general anesthesia yielded
significantly higher lowest and average SpO2 levels when compared to
conventional facemask ventilation. However, Zhu et al. [27] reported
that the THRIVE technique was not inferior to conventional facemask ventilation
regarding the lowest and average SpO2 levels among ASA I-II adult patients
during the ECT procedure. Similarly, Vaithialingam et al. [32] found no
significant difference in average SpO2 levels between the THRIVE and
facemask groups in adult patients. Several studies have identified predictors of
the lowest and average SpO2 levels following THRIVE technique [41, 42, 43, 44, 45], and
they have suggested that a lower BMI [43, 45], higher flow rates or oxygen
concentrations [41, 42, 44] are associated with higher levels of the lowest
SpO2 and average SpO2. Therefore, the variations of these findings
could be partially attributed to the differences in BMI (patients with mean BMI
ranging from 21.8 to 23.4 kg/m2 in previous studies [27, 32] versus 21.2
kg/m2 in this study), flow rate (50 L/min used in previous studies [27, 32]
versus 70 L/min used in this study), and oxygen concentrations (50% oxygen
applied in Zhu et al.’s study [27] versus 100% oxygen used in this
study) across the above studies [27, 32]. It was also evident that THRIVE
technology could effectively be employed in obese patients (BMI
Oxygen desaturation represents a potential safety concern for patients
undergoing ECT procedures, leading to prolonged stays in the treatment area and
incurring considerable human and material costs [12, 33]. In this study, only one
patient in the facemask group experienced oxygen desaturation, while none did in
the THRIVE group, aligning with the findings of prior studies [33, 34]. Jonker
et al.’s study [33] recruited 13 patients who underwent ECT using the
THRIVE technique, and none of them developed oxygen desaturation (SpO2
levels
Following the induction of general anesthesia during apneic oxygenation, previous studies on the THRIVE technique during ECT procedures have observed a gradual rise in transcutaneous CO2 of 0.53 kPa/min [33]. The accumulation of CO2 has been linked to a shortened seizure duration and an increased seizure threshold in patients receiving ECT [48, 49]. In line with the findings of two previous studies [27, 32], this study did not identify significant differences between the THRIVE and facemask groups regarding seizure duration and stimulation dosage. Similarly, this study had no significant group differences regarding MAP and HR, consistent with earlier research [39, 47]. For example, two separate RCTs focusing on elderly patients [47] and edentulous elderly patients [39] under general anesthesia found no significant differences in HR or MAP between the THRIVE and facemask groups. Notably, Vaithialingam et al.’s study [32] reported a few differences in MAP and HR at selected time points; however, these differences were too minimal to have any clinical significance. The association between CO2 levels and several factors (e.g., flow rate, BMI, and apnea time) warrants further examination to avoid complications from elevated CO2 when the THRIVE technique is used as a ventilation method during the ECT procedure.
In this study, all participants undergoing ECT were followed up for 24 hours, and none of them in either THRIVE or facemask groups reported airway-related complications, such as nose bleeding, nasal dryness, pain, or itch. Similarly, numerous previous studies have also reported the safety of the THRIVE technique during ECT procedures [32, 39]. For example, Vaithialingam et al. [32] found that none of the patients receiving the THRIVE technique reported airway-related complications (e.g., pneumothorax, hoarseness, or nasal injury) within 24 hours following the ECT procedure. Shen et al. [39] reported that the THRIVE technique was utilized as safely in edentulous elderly patients as conventional facemask ventilation. The safety of the THRIVE technique might be attributed to its provision of heated and humidified oxygen [50, 51].
Several limitations should be considered in the context of this study. First, it is essential to recognize that this research was conducted at a single center and included a specific study population, limiting the generalizability of our findings. Second, blood gas analysis was not included in this study. This was not ethically justifiable for research purposes alone. Third, the sample size of this study was relatively small, which decreased the statistical power and also limited the generalizability of these findings. Furthermore, the sample size was not determined by power analysis, nor was it based on the THRIVE study in ECT. Fourth, as the participants in this study were of a healthy weight (BMI 18.5–23.9 kg/m2) according to the BMI classification criteria for Chinese adults [52], these findings may not apply to all patients undergoing ECT procedures. Further studies focusing on patients with overweight or obesity should be conducted. Finally, subgroup analysis based on different diagnoses was not performed in this study.
The THRIVE technique appeared to be more effective than conventional facemask ventilation in preserving SpO2 levels during ECT in patients with major mental disorders, presenting itself as a safe and effective hands-free alternative for oxygenation. However, caution is advised when applying the THRIVE technique to patients with a high BMI. Moreover, patients receiving the THRIVE technique should be given appropriate oxygenation, including an adequate flow rate and oxygen concentration.
The data used and analyzed during the current study are available from the corresponding author upon reasonable request.
Data curation - C-JD, SN, RZ, X-HY, Q-BZ; Investigation - C-JD, SN, RZ, J-XM, S-CX; Validation - C-JD, SN, RZ, J-XM; Writing—Original Draft - C-JD, SN, RZ, J-XM, XH, S-CX, X-HY, Q-BZ; Formal analysis - XH, S-CX, Q-BZ; Funding acquisition - SN, X-HY, X-BH, WZ; Conceptualization - X-BH, WZ; Supervision - X-BH, WZ; Methodology - X-BH, WZ; Project administration - X-BH, WZ; Writing—Review & Editing - X-BH, WZ. All authors approved the final version to be submitted. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The Institutional Review Board (IRB) of the Affiliated Brain Hospital, Guangzhou Medical University, approved this trial (approval number: 2024034; date: April 26, 2024). Informed written consent was obtained from patients or their families/legal guardians. The study was carried out in accordance with the guidelines of the Declaration of Helsinki.
Not applicable.
This study was funded by the Science and Technology Program of Guangzhou (20251A011047, 20252A011018, 20241A010043), Science and Technology Planning Project of Liwan District of Guangzhou (202201012), National Clinical Key specialty construction project [(2023) 33], The Natural Science Foundation Program of Guangdong (2023A1515011383, 2024A1515012578), Guangzhou Municipal Key Discipline in Medicine (2025-2027), Guangzhou High-level Clinical Key Specialty, Department of Emergency Medicine of National clinical key specialty and Guangzhou Research-oriented Hospital. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
The authors declare no conflict of interest. Wei Zheng is serving as Editor-in-Chief and Guest editor of this journal. We declare that Wei Zheng had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Francesco Bartoli.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/AP39942.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.