




 , Qiuhong Chen 1, Ting Leng 1, Mengling Gu 1, Lin Luo 1, Furong Jiang 1, Xiahong Huang 1,*
, Qiuhong Chen 1, Ting Leng 1, Mengling Gu 1, Lin Luo 1, Furong Jiang 1, Xiahong Huang 1,*
1 Division of Critical Care Medicine, Deyang People’s Hospital, 618000 Deyang, Sichuan, China
Abstract
Cardiac rehabilitation (CR) serves as a critical component in ongoing care for cardiovascular disease patients, improving postoperative anxiety and depression in cardiac surgery patients while reducing readmission rates and mortality. However, patient completion rates for CR programs remain low due to insufficient awareness and lack of social support. This study aimed to investigate the impact of family support levels on self-management behaviors in postoperative cardiac surgery patients, providing a basis for family-based cardiac rehabilitation interventions.
This cross-sectional survey involved 76 patients who had undergone major vascular surgeries one month prior and were subsequently discharged from the hospital’s cardiology department. Participants completed questionnaires assessing demographic details, family support, psychological status, and self-management practices. Logistic regression analysis identified factors influencing perceived social support from family (PSS-Fa), while correlation analyses examined relationships between family support and self-management behaviors.
The mean PSS-Fa score was 10.82 ± 1.50, and the average self-management behavior score was 140.80 ± 20.46. Female gender, marital status, and educational attainment significantly influenced higher family support scores (p < 0.05). For the univariate analysis, key determinants of better self-management included age, educational level, marital status, household income, type of medical insurance, presence of comorbidities, cardiac function classification, and psychological states indicative of anxiety or depression (all p < 0.05). Multiple linear regression analysis showed that PSS-Fa, age, and education level significantly influenced self-management behaviors in postoperative cardiac patients. Family support and education level had a positive effect, while age had a negative impact. The model’s overall fit statistics are R2 = 0.821 and F = 33.722 (p < 0.05). Pearson’s correlation analysis revealed a positive association between family support and overall self-management behaviors (r = 0.303, p < 0.05), particularly in nutrition management, exercise adherence, self-monitoring, and timely medical consultations.
This suggests that the role of family support should be fully considered in developing CR programs in the future, and targeted interventions should be implemented to enhance this support, thereby potentially improving patient outcomes and adherence to CR programs.
Keywords
- patients after cardiac surgery
- cardiac rehabilitation
- family support
- self-management
- correlation analysis
Cardiac rehabilitation (CR) is a comprehensive outpatient program that combines exercise training and educational interventions to promote lifestyle changes, control risk factors, and implement secondary prevention strategies. Studies have shown that CR is not only effective in alleviating anxiety and depressive symptoms but also significantly improves patients’ quality of life and reduces readmission and mortality rates in patients after cardiac surgery [1, 2]. However, despite these substantial benefits, many eligible individuals fail to fully engage in CR programs as intended. Indeed, participation rates for CR are notably low in China, ranging from 19% to 45% [3, 4]. Several factors contribute to this underutilization, including personal characteristics such as age, gender, and level of education, as well as socioeconomic factors such as income and social support networks [5, 6]. Furthermore, post-surgical patients frequently experience heightened emotional distress, which complicates self-management efforts and adherence to prescribed CR protocols [7, 8].
Family support is a key component in the social support system that provides patients with financial, material, and psychological assistance and significantly enhances their self-management skills [9]. Given the limited accessibility of traditional CR programs, Chinese CR experts advocate for home-based cardiac rehabilitation (HBCR) as an alternative for stable patients [10]. A study conducted by McDonagh et al. [11] demonstrated that HBCR was comparable to facility-based CR programs regarding clinical outcomes and health-related quality of life while validating its safety and efficacy. However, the success of HBCR hinges on patient engagement and optimal self-management practices.
Although some studies have demonstrated the positive impact of family support on the self-management behaviors of patients after cardiac surgery, most existing studies have focused on qualitative analyses, meaning the quantitative assessment of the relationship between family support and self-management remains underexplored [12, 13]. Additionally, there is insufficient exploration into how cultural differences impact the efficacy of family support, especially within the Chinese context [14, 15].
Self-management is vital to patients following cardiac surgery since it encompasses a broad spectrum of elements, including managing anticoagulation therapy, monitoring symptoms, regular follow-up assessments, preventing infection, lifestyle modification, and emotional regulation [16]. Although systematic reviews have emphasized the importance of self-management in the context of HBCR [17, 18], there remains a lack of research on the specific level of self-management and its influencing factors in these patients. Therefore, this study aimed to assess the level of family support and related self-management behaviors one month after cardiac surgery to explore the impact of family support on self-management outcomes and to provide a scientific basis for HBCR interventions.
This manuscript presents a reanalysis of data that was previously published in ‘The Effect of Family Support Level on Psychological State and Self-Management Behavior in Patients Undergoing Cardiac Surgery’ in Prevention and Treatment of Cardiovascular Diseases. It not only includes original findings but also offers deeper insights into the influence of varying levels of family support on postoperative self-management behaviors. Specifically, it provides additional perspectives on how different degrees of family support can impact patient outcomes, thereby offering more targeted guidance for interventions aimed at improving these patients’ self-management practices.
This study employed a cross-sectional correlation design to investigate patients
who underwent cardiac surgery at our hospital between January 2024 and June 2024.
Inclusion criteria: (1) age
This study employed power analysis to determine a suitable sample size. Based on
existing literature reporting the correlation between self-management behaviors
and family support in postoperative cardiac surgery patients [12], we anticipated
an effect size of 0.5 (considered a medium effect) to achieve 80% power and to
detect this effect size with a two-tailed significance level of
The hospital’s Medical Ethics Committee (2024-04-074-K01) reviewed and approved the study protocol, and all participants provided written informed consent.
Four trained researchers conducted a telephone questionnaire to investigate the patients who met the inclusion and exclusion criteria after cardiac surgery. The survey included demographic data such as gender, age, education level, marital status, etc. Clinical data and disease-related characteristics of patients were also obtained by reviewing medical records. Self-reported questionnaires were used to assess family support, anxiety, depression, and self-management behavior.
Before conducting the survey, each researcher explained to the participant the purpose, content, anonymity, free of charge, and necessary study precautions. Once participants fully understood these aspects, informed consent was provided. To ensure that patients could clearly understand the questions, complex terminology was avoided as much as possible during the survey to ensure that the questions were easy to understand and answer. After completing the study, researchers reviewed the data for completeness and reasonableness. For any missing or unclear responses, the researcher contacted the participant promptly to correct or add information as needed.
All patients completed a general information questionnaire (including gender, age, education level, marital status, per capita monthly household income, type of medical insurance, comorbidities, cardiac function grade, etc.). Additionally, the family support self-rating scale, general hospital anxiety and depression scale, and self-management behavior scale were simultaneously measured.
The perceived social support from family (PSS-Fa) [19] was used to assess the
level of family support each patient received. The scale contains 15 entries with
a total score from 0 to 15; 0 to 10 represents a low level of family support, and
The General Hospital Anxiety and Depression Scale (HADS) was used to detect psychological states. The scale contains two categories of anxiety and depression, each containing seven items, and can be scored on a scale of 0–3, with total scores ranging from 0–21 points. The higher the score, the more serious the depression or anxiety. For each subscale, a score from 0 to 7 indicates no anxiety or depression, 8 to 10 indicates mild depression or anxiety, 11 to 14 indicates moderate depression or anxiety, and 15 to 21 indicates severe depression or anxiety [20].
The self-management behavior scale for heart valve replacement surgery, designed by Wang [21], was used to assess patients’ self-management ability. This scale includes six dimensions comprising medication, nutrition, health care, exercise, self-monitoring, and medical-seeking, with 38 entries. A Likert 5-point scale with a maximum score of 190 was used. The content validity of the scale was 0.937, the content validity of each dimension was 0.93–1.00, and the Cronbach’s alpha coefficient was 0.94.
Data preprocessing: we conducted preliminary checks on all collected data to ensure quality, including cleaning outliers and consistency.
Handling of missing values: for cases with missing data, we employed multiple imputation techniques to fill in the gaps, preserving the integrity and completeness of our sample.
To summarize the sociodemographic and clinical characteristics of the sample, we
conducted descriptive statistical analyses. Categorical variables are presented
as frequencies and percentages (%), and the chi-square test or Fisher’s exact
test was employed to compare proportions between groups. Continuous variables
that met the assumptions of normality were described using the mean and standard
deviation (
Given the aim of our study—to explore a simple linear relationship between levels of family support and self-management behaviors—we primarily chose to use Pearson’s correlation coefficient. Scatter plots were visually inspected to confirm the linearity assumption before applying Pearson’s correlation. This bivariate approach was deemed suitable for exploring direct associations without modeling complex interactions between multiple predictors.
Multiple linear regression analyses were conducted to identify key factors influencing self-management behaviors. Variables included in the regression model were selected based on their theoretical relevance and preliminary univariate analyses.
Statistical significance was set at a two-tailed p-value
This study included 76 patients, 48 (63.15%) of whom were female and 28 (36.85%) were male, with a mean age of 52.81 years (SD = 11.96). Of the participants, 39 (51.31%) reported high levels of family support, as indicated by a mean PSS-Fa score of 10.82 (SD = 1.50), whereas 37 (48.68%) reported lower levels of family support. Table 1 shows the distribution of sociodemographic and clinical characteristics of the participants.
| Characteristics | N (%) | PSS-Fa | Expected N | t/F | p-value | |
| Gender | –3.041 | 0.003* | ||||
| Male | 28 (36.8) | 10.2 |
27.5 | |||
| Female | 48 (63.2) | 11.2 |
48.5 | |||
| Age | 0.597 | 0.553 | ||||
| 15 (19.7) | 11.2 |
15.2 | ||||
| 45–60 | 36 (47.4) | 10.8 |
35.6 | |||
| 25 (32.9) | 10.7 |
29.2 | ||||
| Education level | 2.805 | 0.046* | ||||
| Primary education | 19 (25.0) | 10.1 |
18.8 | |||
| Junior high school | 35 (46.1) | 10.9 |
35.5 | |||
| High school | 16 (21.1) | 11.1 |
16.4 | |||
| University and above | 6 (7.8) | 11.8 |
7.3 | |||
| Marital status | 15.600 | 0.000* | ||||
| Married | 53 (69.7) | 11.2 |
52.4 | |||
| Unmarried | 7 (9.2) | 11.3 |
7.1 | |||
| Divorced/widowed | 16 (21.1) | 9.2 |
16.5 | |||
| Monthly income, USD | 2.992 | 0.056 | ||||
| 9 (11.8) | 9.8 |
9.6 | ||||
| 280–700 | 47 (61.8) | 10.9 |
46.5 | |||
| 20 (26.4) | 11.2 |
20.9 | ||||
| Medical insurance type | 3.308 | 0.042* | ||||
| Self-financing | 5 (6.6) | 10.4 |
5.1 | |||
| Resident medical insurance | 48 (63.1) | 10.6 |
47.5 | |||
| Employee medical insurance | 23 (30.3) | 11.5 |
22.4 | |||
| Diagnosis | 1.123 | 0.346 | ||||
| AD | 6 (7.8) | 11.0 |
6.0 | |||
| CT | 8 (10.5) | 11.5 |
8.2 | |||
| VHD | 60 (78.9) | 10.8 |
60.1 | |||
| ASD | 2 (2.6) | 9.5 |
2.7 | |||
| Comorbidities | 0.586 | 0.626 | ||||
| Hypertension | 20 (26.3) | 10.7 |
20.0 | |||
| Diabetes | 13 (17.1) | 10.5 |
13.3 | |||
| Others | 7 (9.2) | 11.0 |
7.2 | |||
| None | 36 (47.4) | 11.0 |
36.5 | |||
| Cardiac function | 0.950 | 0.392 | ||||
| NYHA class I | 12 (15.8) | 11.3 |
12.3 | |||
| NYHA class II | 31 (40.8) | 10.8 |
30.7 | |||
| NYHA class III | 33 (43.4) | 10.6 |
32.0 | |||
| Anxiety/depression | 2.066 | 0.134 | ||||
| Low | 18 (23.7) | 11.0 |
18.1 | |||
| Medium | 43 (56.6) | 11.0 |
42.6 | |||
| Moderate to severe | 15 (19.7) | 10.1 |
15.3 | |||
Note: PSS-Fa, perceived social support from family; AD, aortic dissection; CT, cardiac tumor; VHD, valvular heart disease; ASD, atrial septal defect; NYHA, New York Heart Association.
NYHA classes are defined as follows:
The t-test was used for gender comparisons; ANOVA was used for age,
educational level, marital status, per capita monthly income, medical insurance
type, diagnosis, complication, cardiac function, and anxiety/depression
comparisons; * indicates significance: p
Statistical analysis revealed no significant differences in PSS-Fa scores across
various demographic characteristics such as age, monthly family income,
diagnosis, presence of comorbidities, cardiac function, and levels of anxiety or
depression (all p
Given that the PSS-Fa scores of unmarried patients were slightly higher than
those of married patients, we conducted a Kruskal–Wallis test. The results
showed a chi-square value (H) of 25.025 with 2 degrees of freedom, and both the
asymptotic and exact significance levels were 0.000 (p
These findings suggest that while marital status does influence perceived family support, the distinction is most pronounced when comparing those who are married or unmarried with those who are divorced or widowed. Therefore, the lack of significant difference between married and unmarried individuals underscores the complexity of this relationship and highlights the need for further investigation into the factors contributing to perceived family support within these subgroups. Future research with a larger sample size may provide more definitive insights into the nuanced relationship between marital status and perceived family support.
Table 2 presents the self-management behaviors of patients with different levels
of family support. The overall mean score of self-management behaviors for the 76
patients was 140.80
| Group | n | Medication | Nutrition | Exercise | Health caring | Self-monitoring | Medical-seeking | Total points |
| High level | 39 | 16.3 |
16.2 |
14.2 |
43.3 |
23.9 |
32.7 |
146.5 |
| Low level | 37 | 15.8 |
15.0 |
13.3 |
40.8 |
20.2 |
29.7 |
134.8 |
| t | 1.084 | 2.643 | 1.268 | 1.574 | 2.373 | 2.132 | 2.579 | |
| p-value | 0.282 | 0.010 | 0.209 | 0.120 | 0.020 | 0.036 | 0.012 |
Note: Family support levels definitions:
Independent samples t-tests were used to compare the means of self-management behavior scores between the high and low family support groups.
Figs. 1,2,3,4 present scatter plots comparing PSS-Fa scores with self-management behavior scores to confirm the linearity assumption for Pearson’s correlation analysis. These figures show the relationship between family support and specific self-management behaviors, along with fitted lines for both linear and cubic polynomial models. These findings indicate that higher levels of family support are associated with better self-management behaviors in these specific areas.
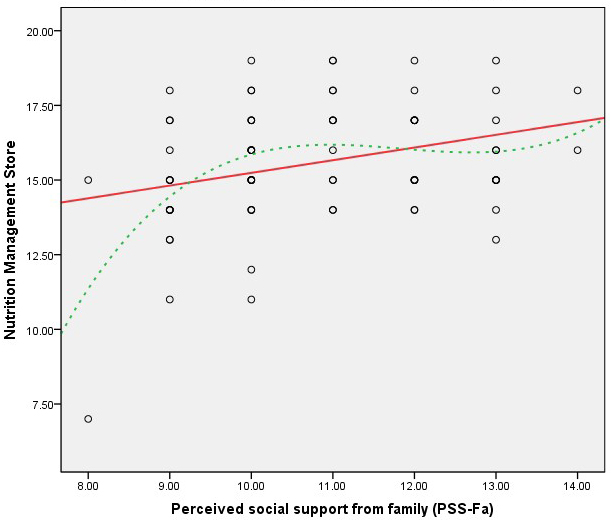 Fig. 1.
Fig. 1.
Scatter plot of PSS-Fa vs. nutrition management (linear model RL2 = 0.095; cubic polynomial model R2 = 0.205). Note: the red solid line represents the linear fit, and the green dashed line depicts the cubic polynomial fit.
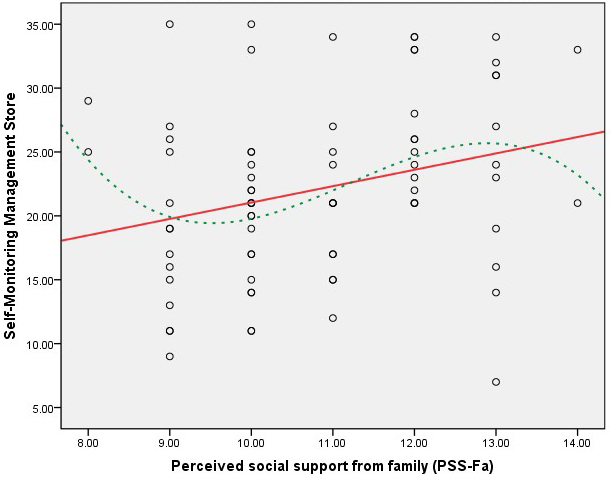 Fig. 2.
Fig. 2.
Scatter plot of PSS-Fa vs. self-monitoring management (linear model RL2 = 0.076; cubic polynomial model R2 = 0.116). Note: the red solid line represents the linear fit, and the green dashed line depicts the cubic polynomial fit.
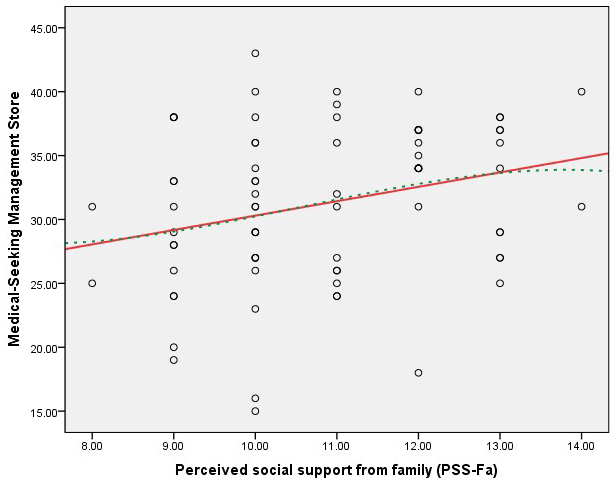 Fig. 3.
Fig. 3.
Scatter plot of PSS-Fa vs. medical-seeking management (linear model RL2 = 0.076; cubic polynomial model R2 = 0.077). Note: the red solid line represents the linear fit, and the green dashed line depicts the cubic polynomial fit.
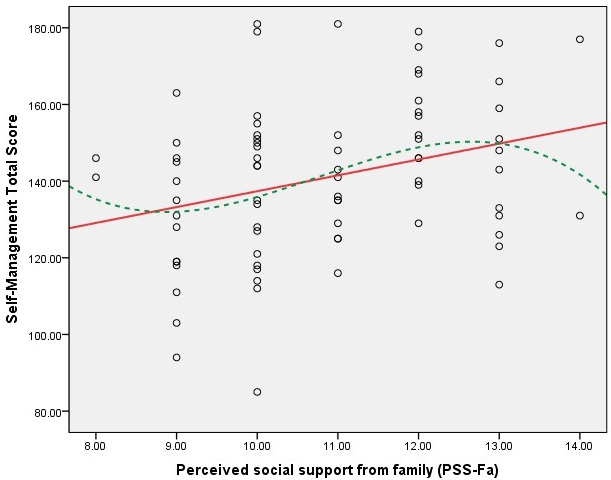 Fig. 4.
Fig. 4.
Scatter plot of PSS-Fa vs. self-management total score (linear model RL2 = 0.092; cubic polynomial model R2 = 0.111). Note: the red solid line represents the linear fit, and the green dashed line depicts the cubic polynomial fit.
Table 3 presents the results of the correlation analysis between PSS-Fa scores
and self-management behavior scores one month after cardiac surgery. The study
revealed a positive correlation between the PSS-Fa score and the total
self-management behavior score (r = 0.303, p
| Item | PSS-Fa | Medication | Nutrition | Exercise | Health caring | Self-monitoring | Medical-seeking | Self-management |
| PSS-Fa | 1.000 | 0.085 | 0.308** | 0.231* | 0.157 | 0.276* | 0.275* | 0.303** |
| Medication | 0.085 | 1.000 | 0.364** | 0.500** | 0.397** | 0.597** | 0.279* | 0.630** |
| Nutrition | 0.308** | 0.364** | 1.000 | 0.248* | 0.143 | 0.368* | 0.267* | 0.428** |
| Exercise | 0.231* | 0.500** | 0.248* | 1.000 | 0.569** | 0.706** | 0.638** | 0.847** |
| Health caring | 0.157 | 0.397** | 0.143 | 0.569** | 1.000 | 0.567** | 0.234* | 0.739** |
| Self-monitoring | 0.276* | 0.597** | 0.368* | 0.706** | 0.567** | 1.000 | 0.547** | 0.897** |
| Medical-seeking | 0.275* | 0.279* | 0.267* | 0.638** | 0.234* | 0.547** | 1.000 | 0.715** |
| Self-management | 0.303** | 0.630** | 0.428** | 0.847** | 0.739** | 0.897** | 0.715** | 1.000 |
Note: * indicates
significance p
Specifically, the correlation analysis showed statistically significant positive correlations for the following self-management behavior subdomains:
However, no significant correlations were found between PSS-Fa scores and the following subdomains:
The lack of significant correlations between medication and healthcare management may be attributed to the nature of cardiac surgery. Patients undergoing cardiac surgery often have large surgical wounds and require prolonged treatment, which may enhance their self-management abilities in these specific areas. As a result, the influence of family support on these aspects of self-management may be less pronounced.
To further identify the key factors influencing self-management behaviors in
postoperative cardiac patients, we performed a one-way analysis of variance and
multiple linear regression analyses. Univariate analysis revealed that patients’
total self-management behavior scores differed significantly with respect to age
(F = 105.845), education level (F = 52.765), marital status
(F = 24.367), monthly household income (F = 18.610), type of
health insurance (F = 22.165), presence of comorbidities (F =
3.748), cardiac function (F = 5.648), and anxiety or depression status
(F = 22.937), all p
Multiple linear regression analysis: Multiple linear regression analysis was conducted to determine the significant factors influencing self-management behaviors. The results indicated that PSS-Fa score, age, and education level significantly predict self-management behaviors in postoperative cardiac patients. Specifically:
The model’s overall fit statistics are as follows:
Table 4 presents the results of multiple linear stepwise regression analyses of factors influencing self-management behavior in patients with different levels of family support.
| Predictors | B | SE | t | p-value | 95% CI | |
| PSS-Fa | 2.284 | 0.797 | 0.167 | 2.866 | 0.000 | [0.693, 3.874] |
| Age | –18.918 | 2.948 | –0.661 | –6.417 | 0.000 | [–24.805, –13.032] |
| Education level | 9.396 | 3.423 | 0.845 | 5.992 | 0.000 | [3.439, 10.231] |
| Marital status | –2.880 | 0.478 | –0.034 | –0.602 | 0.550 | [–1.243, 0.667] |
| Monthly income | 3.166 | 2.920 | 0.093 | 1.084 | 0.282 | [–2.664, 8.996] |
| Cardiac function | 1.482 | 1.666 | 0.052 | 0.889 | 0.377 | [–1.845, 4.809] |
| Complication | –1.811 | 1.229 | –0.089 | –1.473 | 0.145 | [–4.264, 0.643] |
| Medical insurance type | –3.350 | 3.181 | –0.092 | –1.053 | 0.296 | [–9.702, 3.001] |
| Anxiety/depression | –3.491 | 2.386 | –0.113 | –1.463 | 0.148 | [–8.255, 1.272] |
The primary objective of CR is to induce long-term health behavioral changes and
integrate regular physical activity and exercise training into daily life [22].
Our study provided important insights into the level of family support and
self-management behaviors of patients after cardiac surgery one month
postoperatively and identified relevant influencing factors. The results showed
that the PSS-Fa score of patients after cardiac surgery one month postoperatively
was 10.82
The potential factors influencing the level of family support of patients include that the PSS-Fa scores of women were higher than those of male patients, and the family support scores of married or unmarried patients were significantly higher than those of divorced or widowed patients, suggesting that spouses can provide more psychological support than other family members. Higher education was also associated with higher family support, which aligns with the results of patients with chronic heart failure [24]. Regarding the mechanism of gender differences in family support, we believe that women usually have better communication skills and can express their needs and obtain support more effectively. In the Chinese cultural context, women, as the central bond of the family, tend to take on the role of caregiver and thus are more likely to receive family support [25]. Furthermore, higher education was associated with higher family support, possibly because highly educated patients have better tolerance for major setbacks, are more willing to learn about the disease and prognosis, and actively communicate with their families for support [26]. In addition, the findings showed that married patients had significantly higher PSS-Fa scores than divorced or widowed patients, which may be because spouses can provide more psychological support to patients than children, parents, or other family members. Spouses provide more emotional comfort and help in real life, which is especially important for patients who lack channels of expression and emotional comfort [27]. However, it is noteworthy that unmarried patients showed a slightly higher mean PSS-Fa score compared to married patients. This suggests that other factors beyond marital status may contribute to perceptions of family support among unmarried individuals. Indeed, strong social networks outside of marriage, such as close friendships or extended family relationships, could play a significant role in this context. Unmarried individuals might rely on these alternative support systems to compensate for the absence of spousal support, leading to comparable or even higher levels of perceived family support [28]. Moreover, future research should explore the underlying mechanisms through which these factors influence family support perceptions.
Cardiac surgery patients require long-term CR to restore cardiac function, and
better self-management ability is essential for ensuring that patients adhere to
medical advice during the rehabilitation process. The results of this study
showed that the total score of self-management behavior in postoperative cardiac
surgery patients ranged from 85 to 181, with a mean of 140.80
As individuals within a social network, patients’ behavior is closely linked to
their psychological state and social environment [32]. The results of this study
identified several factors influencing the self-management behavior of
postoperative cardiac patients, including age, education level, marital status,
monthly family income, self-payment for medical care, comorbidity with other
illnesses (such as hypertension), cardiac function class, and the presence of
anxiety or depression. Multiple linear regression analysis showed that PSS-Fa,
age, and education level were significant factors influencing self-management
behaviors of postoperative cardiac patients, with PSS-Fa and education level
showing a significant positive effect. In contrast, age showed a significant
negative impact (R2 = 0.821, F = 33.722, p
Our results highlight the significant correlation between family support and self-management behaviors in cardiac surgery patients. Moreover, this study emphasizes the necessity of enhancing family support as an integral component of CR for patients. Furthermore, we underscore the importance of incorporating international comparisons in future studies to improve the identification of unique characteristics of Chinese patients and provide more practical clinical recommendations tailored to the local context. The health ecology model [37] posits that numerous factors, including health services, the social environment, physical life conditions, and individual attributes, are interdependent and mutually influential, collectively impacting individual health. Consequently, when formulating health promotion strategies for postoperative cardiac patients, it is imperative to consider the varying levels of family support and tailor HBCR programs.
Despite the valuable insights provided by this study, several limitations should be acknowledged. First, this study chose patients discharged from our hospital after cardiac surgery treatment between January 2024 and June 2024. This specific time frame and single-center approach may introduce selection bias, limiting the generalizability of the findings to a broader population. Future studies should consider a multi-center design and a longer recruitment period to ensure a more diverse and representative sample. At the same time, the research team assessed the level of family support and self-management behavioral ability one month after discharge. This cross-sectional design does not capture the process or trend of changes in family support and self-management ability over time, limiting the study’s understanding of dynamic changes. A longitudinal study could track these variables over a longer period, providing a more in-depth understanding of their dynamics and potential causal relationships. In addition, this study analyzed the factors affecting self-management behavioral competence based on patients’ sociodemographic and clinical characteristics; however, it did not explore other potential factors such as socioeconomic status, access to healthcare resources, or cultural influences. Future research could incorporate a broader range of variables to provide a more comprehensive understanding of the factors influencing self-management behaviors. Lastly, with a sample size of 76 patients, the study may have limited statistical power to detect small to moderate effects. This limitation might result in type II errors (failing to detect true effects). Future studies should perform a priori power analysis to determine the minimum sample size required to achieve adequate statistical power for detecting meaningful effects. The failure of this study to directly measure CR participation in all patients is an important limitation. Although we highlighted significant correlations between family support and self-management behaviors, the lack of specific data on CR participation limits a comprehensive understanding of the overall recovery pathway. Future studies should include data collection on CR participation to more fully assess the relationship between family support, self-management behaviors, and CR participation.
This study has several strengths: The present study focused on HBCR to investigate the level of family support and self-management ability of patients and analyzed the factors influencing them, providing valuable insights for developing targeted interventions in the future. For example, patients with low levels of family support could be targeted with additional family support or psychological interventions.
CR is a critical component of care for patients with cardiovascular disease, yet its implementation remains nascent in China. Many hospitals currently lack the infrastructure and resources to provide comprehensive CR services. As an alternative strategy, HBCR holds promise for increasing patient participation rates. Our study demonstrated that higher levels of family support are positively associated with improved self-management abilities post-cardiac surgery, which in turn enhances the effectiveness of postoperative CR. Specifically:
The future management of patients following cardiac surgery should apply targeted intervention measures to address the diverse needs of different patient categories. These interventions could include:
(1) The development of tailored programs that empower both male and female patients to communicate their needs effectively and access appropriate support.
(2) The implementation of initiatives to enhance health literacy and coping skills among patients with varying educational backgrounds, promoting better family support and self-management.
(3) The provision of counseling services to strengthen spousal relationships and improve emotional support for married patients. For unmarried individuals, alternative support systems such as community groups, online forums, and peer support networks should be established to compensate for the absence of spousal support.
(4) We recommend targeted interventions to address the apparent deficiencies in patient self-monitoring and exercise management.
A detailed exercise program tailored to each post-cardiac surgery patient should be implemented based on existing exercise prescribing principles and practice guidelines; for example, it is recommended to perform moderate-intensity aerobic exercises, such as brisk walking or bicycling, at least three times a week; to continue for more than 30 minutes at a time, incorporating a 5–10-minute warm-up and cool-down period. To ensure the safety and effectiveness of exercise, the patient’s progress should be assessed regularly, and the exercise program should be adjusted accordingly. At the same time, patients are encouraged to record their daily activities so that their physicians can understand and evaluate their physical responses and instruct them accordingly [38].
Regarding self-monitoring, patients are taught how to correctly measure key indicators such as blood pressure and heart rate and explain the significance of these data. Smart devices or apps can also assist with monitoring, enabling patients to complete self-checks easily at home. Thus, by addressing these factors, healthcare providers can significantly improve family support and encourage patients to adopt healthier behaviors, ultimately leading to better clinical outcomes and enhanced quality of life.
CR, cardiac rehabilitation; HBCR, home-based cardiac rehabilitation; PSS-Fa, perceived social support from family; AD, aortic dissection; CT, cardiac tumor; VHD, valvular heart disease; ASD, atrial septal defect; SD, standard deviation.
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
TS conducted the research, data collection, and analysis, drafted and revised the manuscript. QHC and TL participated in data acquisition and interpretation and drafted the manuscript. MLG and LL designed part of the experiments and collected patients who had undergone cardiac surgery. FRJ contributed to the concept and design and revised the manuscript. XHH designed the research, supervised the project implementation, applied for funding, and completed the paper review and editing. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study was approved by the Research Ethics Committee of Deyang People’s Hospital (2024-04-074-K01). Participants had written informed consent to participate in the study before participating. The study was carried out in accordance with the guidelines of the Declaration of Helsinki.
We want to give our heartfelt thanks to all the people who have ever helped us with this paper. We are really grateful to all those who devoted much time to reading this paper and gave us much advice, which will benefit us in our later studies.
This research was funded by the 2024 project of the Sichuan Key Research Base on Mental Health Education (XLJKJY2421B).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.