










 , Teruo Sekimoto 1, Aloke V. Finn 1,2, Renu Virmani 1,*
, Teruo Sekimoto 1, Aloke V. Finn 1,2, Renu Virmani 1,*
1 CVPath Institute, Inc, Gaithersburg, MD 20878, USA
2 School of Medicine, University of Maryland, Baltimore, MD 21201, USA
Abstract
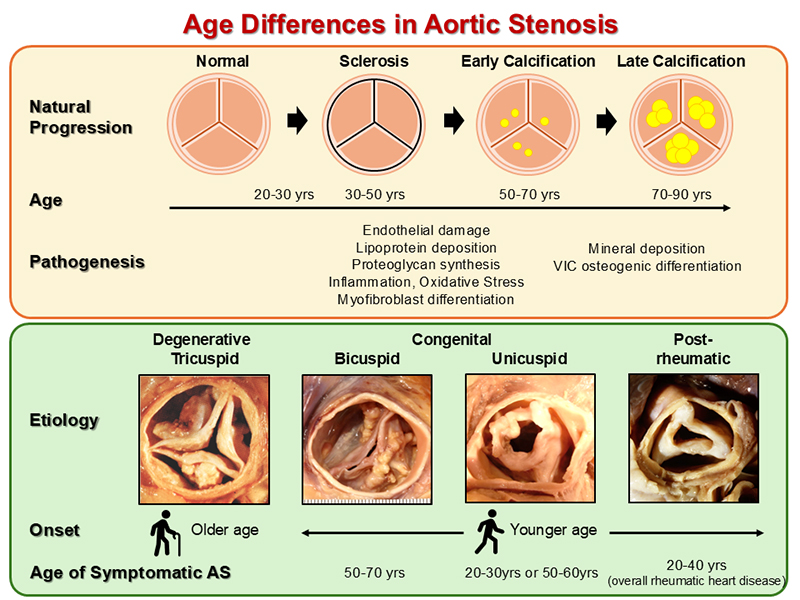
Aortic stenosis (AS) is a significant and growing concern, with a prevalence of 2–3% in individuals aged over 65 years. Moreover, with an aging global population, the prevalence is anticipated to double by 2050. Indeed, AS can arise from various etiologies, including calcific trileaflets, congenital valve abnormalities (e.g., bicuspid and unicuspid valves), and post-rheumatic, whereby each has a distinct influence that shapes the onset and progression of the disease. The normal aortic valve has a trilaminar structure comprising the fibrosa, spongiosa, and ventricularis, which work together to maintain its function. In calcific AS, the disease begins with early calcification starting in high mechanical stress areas of the valve and progresses slowly over decades, eventually leading to extensive calcification resulting in impaired valve function. This process involves mechanisms similar to atherosclerosis, including lipid deposition, chronic inflammation, and mineralization. The progression of calcific AS is strongly associated with aging, with additional risk factors including male gender, smoking, dyslipidemia, and metabolic syndrome exacerbating the condition. Conversely, congenital forms of AS, such as bicuspid and unicuspid aortic valves, result in an earlier disease onset, typically 10–20 years earlier than that observed in patients with a normal tricuspid aortic valve. Rheumatic AS, although less common in developed countries due to effective antibiotic treatments, also exhibits age-related characteristics, with an earlier onset in individuals who experienced rheumatic fever in their youth. The only curative therapies currently available are surgical and transcatheter aortic valve replacement (TAVR). However, these options are sometimes too invasive for older patients; thus, management of AS, particularly in older patients, requires a comprehensive approach that considers age, disease severity, comorbidities, frailty, and each patient’s individual needs. Although the valves used in TAVR demonstrate promising midterm durability, long-term data are still required, especially when used in younger individuals, usually with low surgical risk. Moreover, understanding the causes and mechanisms of structural valve deterioration is crucial for appropriate treatment selections, including valve selection and pharmacological therapy, since this knowledge is essential for optimizing the lifelong management of AS.
Graphical Abstract
Keywords
- aortic stenosis
- calcific aortic valve disease
- bioprosthetic valve failure
The prevalence of clinical aortic stenosis (AS) increases with age, affecting
approximately 2–3% of individuals
The etiology of AS is diverse, with varying epidemiological and histopathological features, molecular mechanisms, and optimal treatment strategies. Therefore, a deeper understanding based on its different etiologies is essential for addressing this increasingly prevalent disease, which poses a significant global health burden.
In this review, we summarize the current understanding of the mechanisms underlying the natural progression of calcific aortic valve disease. We then provide a detailed description of the epidemiological, histopathological, and molecular mechanisms of calcific, congenital, and rheumatic AS individually. Lastly, we discuss the lifetime management of AS, incorporating our histopathological insights into bioprosthetic valve dysfunction.
A normal aortic valve apparatus is located in the aortic root, which is
anatomically defined as the section of the thoracic aorta extending from the
sinotubular junction to the basal ring (aortic annulus). The aortic root,
approximately 2 to 3 cm in length, comprises three main components: the three
aortic valve leaflets, the sinus of Valsalva (the expanded portion of the aortic
root), and the three interleaflet triangles (Fig. 1A,B) [8, 9]. The coronary
ostia are typically located in the left and right coronary sinuses. The aortic
valve has three semicircular cusps and leaflets (left, right, and non-coronary),
which are attached to the aortic sinus in a ring-like structure (semi-lunar
attachment) and are cornet-shaped, called the annulus fibrosus (surgical aortic
annulus). For the interventionist, the annulus, which means “ring”, is the
ventriculoaortic junction. The geometric height of the leaflet is different from
the effective height of the leaflet [10]. The three leaflets are uneven; the free
margin length varies (right 35.2
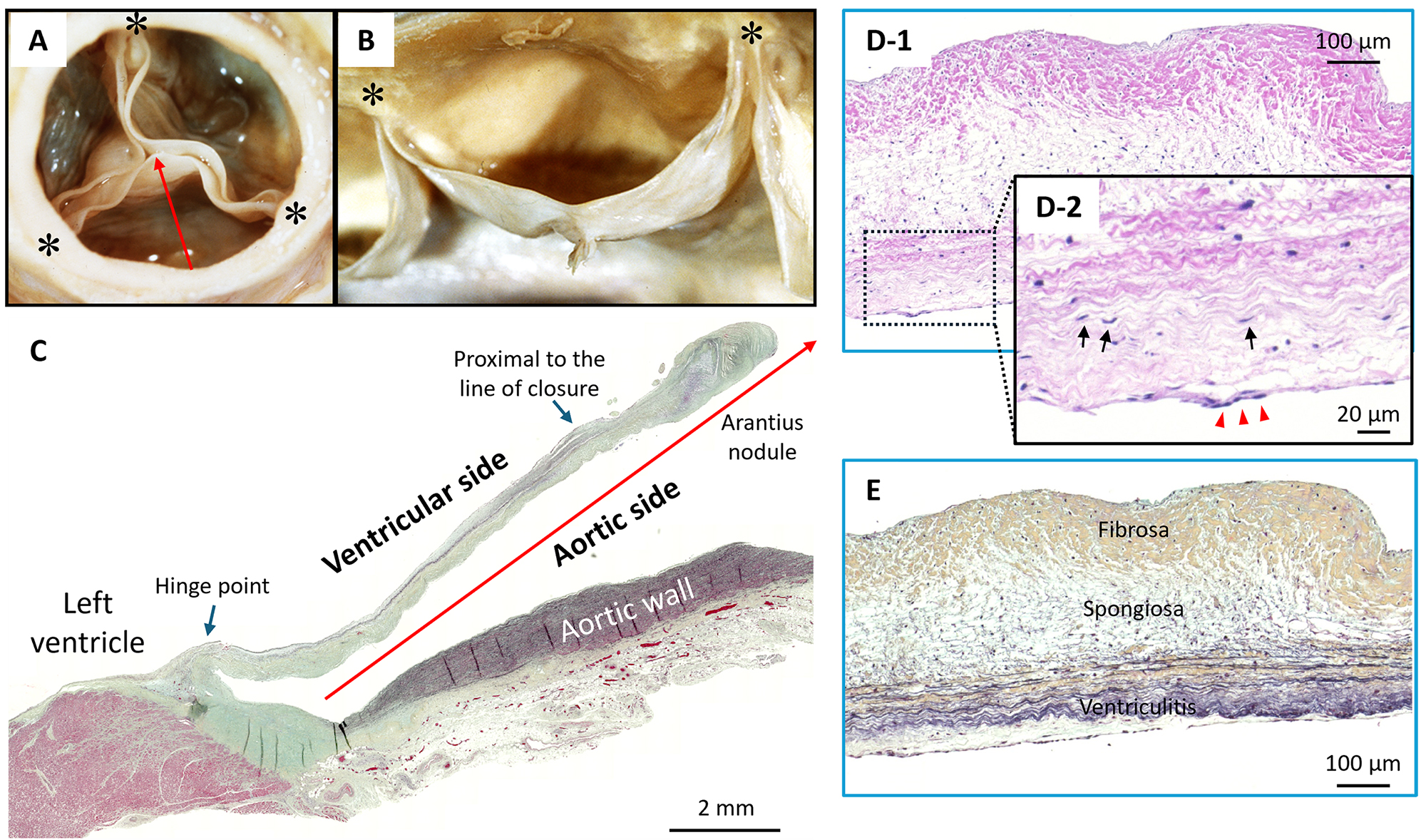 Fig. 1.
Fig. 1.
Representative Histology Images of a Normal Tricuspid Aortic Valve. (A) Gross image of a normal aortic valve from the aortic surface and (B) lateral surface. Asterisks (*) show commissures. The sinus of Valsalva of the non-coronary leaflet and the free margin of the leaflet are shown, along with the line of closure and the nodule of Arantius. (C) Normal aortic valve of 48-year-old male who experienced sudden death from an unknown cause, scale bar: 2 mm. Low-power image of left coronary cusp leaflet (Movat Pentachrome stain). Red arrow shows the dimension of the slice corresponding to (A). The hinge point and area proximal to the line of closure (blue arrows) are the regions prone to greater mechanical forces. (D,E) Normal aortic valve images of 23-year-old male who died with seizure. Low-power image (D-1, scale bar: 100 µm) and high-power image (D-2, scale bar: 20 µm) of H&E stains show valve interstitial cells comprising aortic valve (black arrows) and valve endothelial cells covering valve layers (red triangles). (E) Low-power image of Movat Pentachrome stain shows three layers of lamina fibrosa (upper), spongiosa (middle), and ventricularis (lower), scale bar: 100 µm. H&E, Hematoxylin and Eosin. Images (A) and (B) are reproduced with permission from Virmani R et al. Cardiovascular pathology (pp. 248). 2nd edn. W.B. Saunders Company: Philadelphia. 2001 [9].
Histologically, each leaflet consists of three layers: lamina fibrosa, spongiosa, and ventricularis (Fig. 1D,E). The aortic and ventricular surfaces are covered by valvular endothelial cells (VECs), which work as the interface between the blood and the leaflet. Valvular interstitial cells (VICs) are quiescent, fibroblast-like cells present throughout these three layers and are the major cell component of the valve leaflet. The fibrosa layer, located on the aortic side, consists largely of type I and type III fibrillar collagen with dispersed VICs, which are thought to reinforce the valvular structure [12, 13]. The middle spongiosa layer is composed primarily of proteoglycans and glycosaminoglycans, which absorb a portion of the mechanical stress generated during the cardiac cycle. The ventricularis layer, localized on the ventricular inflow side, consists of collagen and elastin fibers [14, 15].
The aortic valve is structured to allow low-impedance, unidirectional forward blood flow during opening, and to close with enough strength to endure systemic blood pressure [16]. During systole, the aortic valve experiences laminar shear stress on the ventricular side as blood flows past the leaflets, while during diastole, oscillatory shear stress acts on the aortic side as blood pools into the sinuses [17]. Diastolic coronary flow partially generates laminar shear stress on the left and right cusp, while the non-coronary cusp may be solely exposed to oscillatory shear stress. Therefore, throughout the cardiac cycle, the ventricularis layer is subjected to higher, unidirectional forces due to blood flow, while the fibrosa layer experiences lower, bidirectional wall shear stress, especially on the non-coronary leaflet [18, 19].
The earliest change occurs on the aortic surface and is the result of stress-induced cellular senescence, which includes endothelial barrier dysfunction and allows blood lipids to enter the subendothelial space. The mechanical stress pattern generated by the blood flow over time likely initiates aortic valve sclerosis, primarily affecting the aortic side of the valve, typically beginning at the base of the leaflet. This, like the atherosclerotic process, may be followed by inflammatory infiltrate, cell death, and eventual calcification.
AS is caused by three main etiologies: calcific AS (previously referred to as degenerative or senile AS), congenital abnormalities such as bicuspid or unicuspid valve, and rheumatic AS [11]. Table 1 (Ref. [11]) shows the frequency of each AS etiology among patients who underwent SAVR.
| Etiology | Mayo Clinic | University of Minnesota | London | Mayo | AFIP | Baylor University | Toronto | |
| (1965) | (1979–1983) | (1976–1979) | (1990) | (1990–1997) | Medical Center | (2008) | ||
| (1993–2004) | ||||||||
| Tricuspid degenerative (calcific aortic stenosis) | 0% | 28% | 12% | 51% | 49% | 46% | 64% | |
| Congenital | ||||||||
| Bicuspid | 49% | 49% | 56% | 36% | 30% | 49% | 32% | |
| Unicuspid | 10% | 1% | 0% | 0% | 6% | 4% | 3% | |
| Rheumatic | 33% | 23% | 24% | 9% | 13% | - | 11% | |
| Other | 7% | 0% | 8% | 2% | 2% | 1% | 1% | |
Modified with permission from Ladich E et al. Future Cardiol 2011; 7: 629–642 [11]. AFIP, armed forces institutee of pathology.
Unicuspid aortic valve (UAV), has 2 subtypes that are associated with valve
dysfunction, one found in childhood and adolescence (under the age of 25 years),
and the second in adulthood (mean age 51
Calcific AS in patients with tricuspid aortic valve (TAV) occurs in approximately 2–3% of those 65 and over, as well as 7% of those over 80 years old [1, 2, 3]. Overall, calcific AS is more prevalent in men than women (male:female = 1.6:1) [11]. The rarest form is quadricuspid valve, with an estimated incidence of 0.013–0.043% in the general population. The most common clinical manifestation is aortic regurgitation (75%), and pure AS is seen only in 0.7% of cases [28, 29]. A histopathological study from Toronto General Hospital involving over 1000 consecutive surgically excised aortic valves found that TAV, BAVs, and UAVs were present in 64.5%, 31.9%, and 3.0% of patients, respectively [30]. Rheumatic heart disease was present in 11% of all cases, which is lower than earlier studies, indicating that the prevalence of post-rheumatic AS has declined over the past half-century in developed countries.
The burden of calcific AS is expected to increase in the coming decades, due to the aging population and the lack of effective prevention strategies. Current prevalence data and demographic projections indicate that the number of patients over 70 years old with calcific AS will double to triple over the next 50 years in developed countries [7, 31].
Calcific AS is a progressive disease, characterized by pathological features that progress from minimal fibrocalcific changes in early lesions to fibrotic thickening and calcium nodules in advanced stages. Our laboratory has observed varying degrees of calcification in valves removed during both surgery and autopsy.
Early calcification can be clearly identified using von Kossa staining, appearing as finely stippled calcifications or small nodular concretions, typically located in the fibrosa, especially in areas with early atherosclerotic changes (Fig. 2A,B, Ref. [32]). The location is often specific and is seen along the “line of closure” just below the free margin of the aortic leaflets and at “hinge” points. These areas, forming a radial pattern near the attachment of the aortic root, are where early calcific deposits are found, representing regions prone to greater mechanical forces. Early calcifications gradually merge into larger, more complex nodules, extending toward the middle of the leaflet while sparing the free margin, and may eventually protrude onto the aortic surface. Calcification in each cusp has been observed in various forms, including bridges, fingers, and other patterns, such as “radiation” in radiographs (Fig. 3, Ref. [33, 34]) [33].
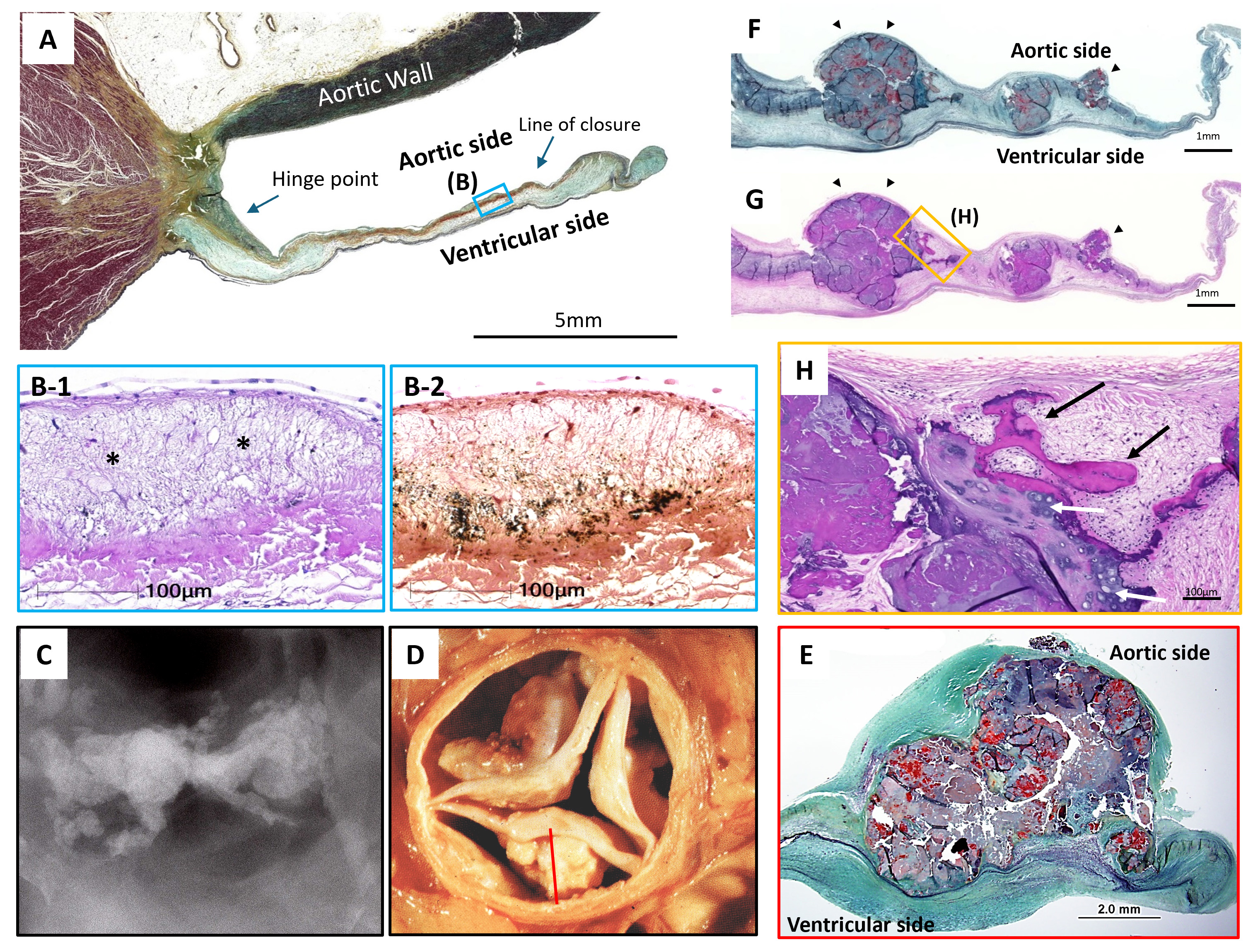 Fig. 2.
Fig. 2.
Representative Histology Images of Tricuspid Aortic Valve Calcification. (A,B) Early-stage calcification resembling atherosclerotic changes. Aortic valve leaflet from 47-year-old male who died due to accidental head trauma. scale bar: 5 mm. (A) Low-power image of the left coronary cusp leaflet stained with Movat Pentachrome (B1,B2). High-power images from the blue box in (A) at the line of closure, showing lipid insudation (*). (B1) H&E revealing calcification as black dots. (B2) von Kossa stain highlighting calcific deposits, scale bar: 100 µm. (C–E) Advanced calcification in aortic valves. Aortic valve from an 82-year-old female. (C) Radiograph showing severely calcified leaflets. (D) Gross image showing significant nodular calcification within the cusps, with large deposits filling the sinuses. (E) Histologic section of the cusp revealing calcific nodules disrupting the normal architecture of the leaflet, scale bar: 2.0 mm. Note fibrotic thickening of the ventricular surface. (F–H) Bone formation in advanced aortic stenosis. Aortic valve leaflet from a 70-year-old female who underwent surgical aortic valve replacement (SAVR) for severe aortic stenosis (AS), F: scale bar: 1 mm; G: scale bar: 1 mm; H: scale bar: 100 µm. Low-power images of Movat Pentachrome (F) and H&E (G) stain showing nodular calcification on the aortic surface (black arrow). The upper and lower surfaces indicate the aortic and ventricular side, respectively. (H) High-power H&E stain image from the boxed region in (G), revealing ossification (black arrow) and cartilaginous metaplasia (white arrow) at the edge of nodular calcification. H&E, Hematoxylin and Eosin. Modified and reproduced with permission from Sato Y et al. Mastering Structural Heart Disease (pp.12). 1st edn. Wiley: NJ. 2023 (A, B1, B2, F, G, and H) [32] and Elena L et al., Future Cardiol 2011; 7: 629–642 (C, D, and E) [11].
 Fig. 3.
Fig. 3.
Calcification Patterns Seen in Radiography and Computed Tomography. (A) Patterns of calcific deposit and regions of cusp flexion. (Upper left) Coaptation pattern: calcification predominantly occurs along the coaptation line (C) of the leaflet. (Upper right) Radial pattern: calcium accumulates in spokes radiating outward from the cusp attachment area (A) toward the center of the cusp. (Lower left) Combination pattern: calcification occurs along both the coaptation line and the cusp attachment, a frequently observed phenomenon. (Lower right) As the aortic valve opens and closes, the cusps of the valve experience significant flexion at the cusp attachment area (A). The cusps also undergo flexion along the coaptation line (C). (B) Patterns of leaflet calcification seen in radiograph. Bridge forms occur as two spokes along the line of cusp coaptation, corresponding to the coaptation pattern in (A), whereas finger forms are seen when calcium deposits incompletely along the line of cusp coaptation. (C) Among our autopsy calcific aortic stenosis cases, 31% accounted for bridge forms, 30% for finger forms, and 39% for other forms. (D) Different grades of calcification are seen in computed tomography: (1) mild, (2) moderate, (3) heavy, and (4) massive calcification, which shows a significant positive correlation with the Agatston score. CT, computed tomography. Modified and reproduced (A) with permission from Thubrikar MJ et al. Am J Cardiol 1986; 58: 304–308 [33], and modified and reproduced (D) with permission from John D et al. JACC Cardiovasc Interv 2010; 3: 233–243 [34].
Aortic valve sclerosis (fibrosis) and calcification have been described to occur
as age advances [35]. Stewart et al. [35] showed that in healthy
individuals 65 to 74 years old undergoing echocardiography, aortic valve
sclerosis was observed in 20% and calcification in 2%; in individuals 75 to 84
years old, sclerosis occurred in 35% and calcification in 2.4%; the highest was
in individuals
Previous epidemiological studies have identified several risk factors for calcific AS, many of which overlap with those for coronary atherosclerosis, including age, male sex, smoking, elevated cholesterol and lipoprotein(a) levels, hypertension, and metabolic syndrome [35, 37, 38, 39]. Furthermore, calcific AS has been linked to chronic kidney diseases and abnormalities in calcium and phosphate metabolism [40].
Since calcific AS and coronary artery disease (CAD) share common risk factors, CAD frequently coexists in patients with severe AS. The prevalence of significant CAD in severe AS patients ranges from 25–50% [41, 42]. CAD is reported in 35–65% of cases among those undergoing SAVR [43, 44] and in 40–75% of TAVR cases [41]. The impact of concomitant CAD on the prognosis of severe AS remains controversial. For SAVR, some studies have indicated higher long-term mortality in patients undergoing coronary artery bypass graft (CABG) surgery with SAVR compared to SAVR alone [45]. In contrast, a large observational study using propensity matching for comorbidities and risk factors found no significant difference in long-term mortality between these groups [44]. Regarding TAVR, while earlier studies suggested that the presence of CAD does not increase mortality rates [46, 47], recent findings indicate that the severity of CAD, rather than its presence alone, may influence outcomes of patients undergoing TAVR [48, 49]. Collectively, whether CAD directly affects the prognosis of patients with severe AS or serves as a bystander condition remains unresolved.
Calcific AS was once regarded as a degenerative disease, both passive and age-related. However, recent studies have suggested that it is a disease involving active cellular processes, with identifiable clinical and genetic risk factors, as well as specific cellular and molecular pathways (Fig. 4, Ref. [11]). Indeed, similarities in clinical risk profiles and extensive experimental research revealed that aortic valve calcification involves mechanisms akin to atherosclerosis, including lipoprotein deposition, chronic inflammation, and mineralization.
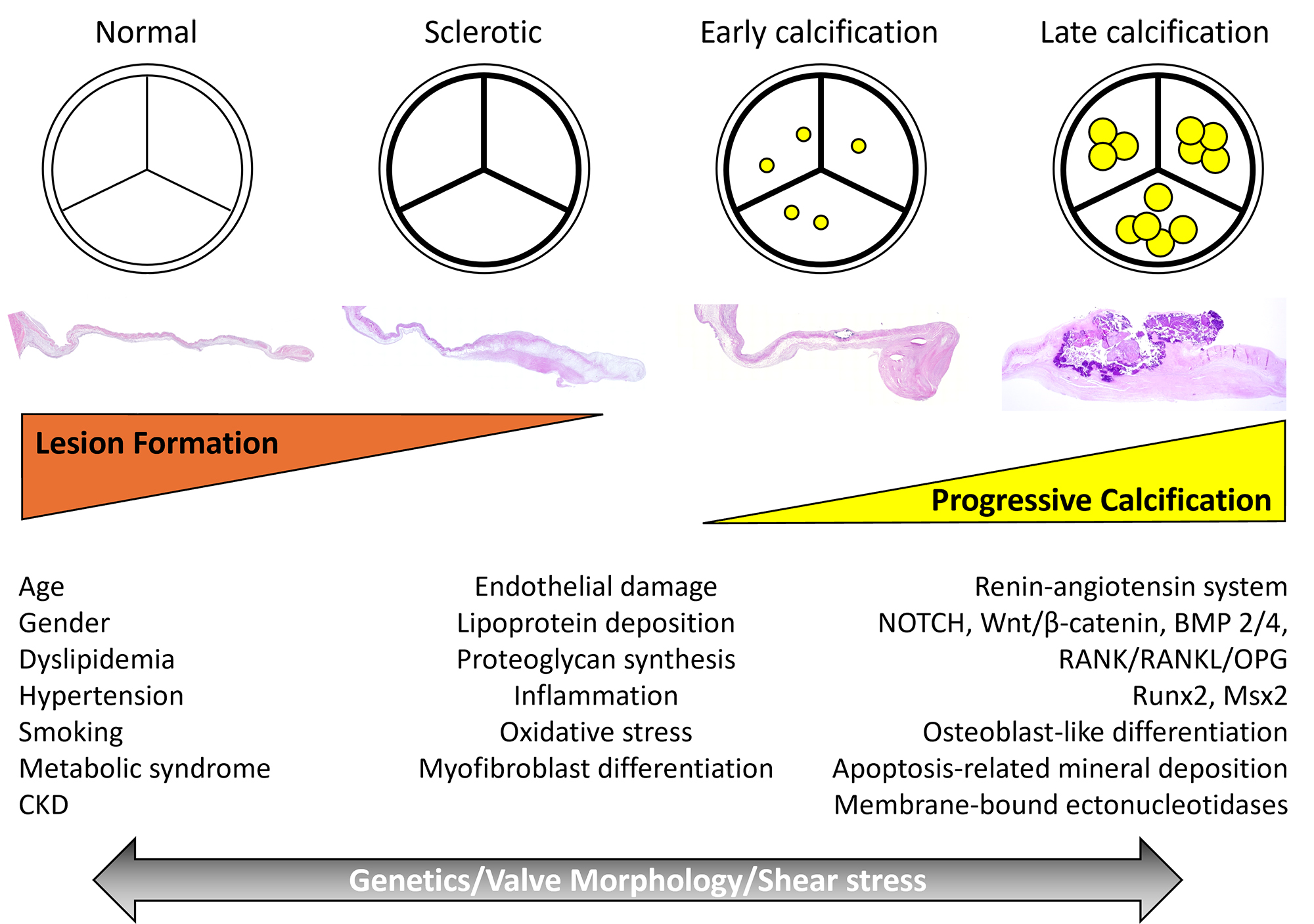 Fig. 4.
Fig. 4.
Diagram Illustrating the Potential Paradigm for the
Understanding of Calcific Aortic Stenosis. Traditional risk factors promote
valve sclerosis and calcification via similar mechanisms to atherosclerosis.
Endothelial damage and proteoglycan synthesis allow for lipoprotein deposition,
which contributes to inflammation and oxidized stress. These processes lead to
myofibroblast differentiation and activate the renin-angiotensin system, leading
to valve sclerosis. Pathways such as NOTCH, Wnt/
Endothelial damage allows for lipid infiltration, specifically low-density lipoprotein and Lp(a), which triggers the recruitment of inflammatory cells [50]. This endothelial injury can be induced by several factors including lipid-derived species, cytokines, and mechanical stress [31]. Proteoglycans such as biglycan and decorin are highly expressed in early phases of calcific aortic valve disease, potentially playing a key role in lipid retention and modification [51, 52]. Additionally, the production of reactive oxygen species (ROS), which is enhanced by the uncoupling of nitric oxide synthase, promotes the oxidization of lipids with osteogenic properties [53, 54].
Inflammation, encompassing innate and adaptive responses, follows endothelial
damage and oxidized phospholipid deposition, driving disease progression [55, 56]. Macrophages and T lymphocytes are key players in the inflammatory process;
however, the involved immune cell network is highly complex, comprising a diverse
and heterogeneous array of immune cell phenotypes [55]. Briefly, pro-inflammatory
(M1) macrophages, which are the predominant subset found in calcific AS, produce
pleiotropic cytokines, such as tumor necrosis factor (TNF)-
The phase of mineralization largely involves two mechanisms: osteogenic
differentiation of VICs and mineral deposition. Osteogenic differentiation occurs
through several distinct pathways, including osteoprotegerin/RANKL (receptor
activator of nuclear kappa B ligand) signaling, NOTCH1 signaling, BMP-2
signaling, Wnt/
BAV is one of the most common congenital heart diseases. Although it initially functions normally at birth, BAV undergoes a degenerative process similar to that of TAV. However, BAVs typically develop stenosis about 10–20 years earlier than TAVs [76]. BAV features a conjoint area of two underdeveloped leaflets that are joined together in the area of commissure. These leaflets are malformed and known as a “raphe”. Normally, the commissure of the aortic valve is the space where two adjacent leaflets attach parallelly without adhering to each other. In BAVs, one or two commissures may be obliterated, or a raphe may be absent [21].
The pathogenesis of congenital BAV formation remains unknown. Several researchers believe that abnormal blood flow during valvulogenesis leads to improper separation of the valve cusp [77], although this claim lacks sufficient evidence. BAV is widely accepted to have a genetic basis and is hereditary within families, occasionally associated with genetic syndromes such as Marfan syndrome, Turner syndrome, and Loeys-Dietz syndrome [78, 79]. However, BAV is a complex disorder with a polygenic basis, exhibiting incomplete penetrance and variable expressivity [80]. To date, variants in NOTCH1, MYH6, GATA4, GATA5, GATA6, PALMD, EXOC4, TEX41, FBN1, ROBO4, and SMAD6 have been reported to be associated with BAV [81, 82, 83, 84, 85, 86, 87, 88]. BAV is also strongly associated with congenital abnormalities of the aorta, such as coarctation and patent ductus arteriosus, as well as the proximal coronary vasculature. Additionally, after development, it could be linked to conditions like aortic dilation, aneurysm, and dissection. In this context, BAV should be recognized as a condition that impacts the entire aortic root.
BAVs are categorized into three main types based on their morphologic characteristics: types 0, 1, and 2 (Fig. 5, Ref. [32]) [89]. Sievers et al. [89] demonstrated the prevalence of BAV types from 304 patients undergoing surgery. The classification is based on: (1) the number of raphes, (2) the spatial positioning of cusps or raphes, and (3) the functional status of the valve (i.e., stenosis, regurgitation, or both). Type 0, found in 7% of cases, is considered purely bicuspid without a raphe, with commissures located either anterior/posterior or left/right. Type 1, which is the most common (88%), consists of three developmental cusps and two commissures instead of three. In this type, two of the cusps are unequal in size, with the larger conjoint cusp featuring a central raphe. The conjoint cusp is generally less than twice the size of the non-conjoint cusp. The most prevalent common type is the fusion of the left and right coronary cusps (71%), followed by fusion of the non-coronary and right coronary cusps (15%), and the least common is fusion of the left and non-coronary cusps (3%). According to Sievers’ classification, BAVs with two raphes are categorized as type 2 (5%), while several other studies categorize them as unicommissural or unicuspid valves [90, 91].
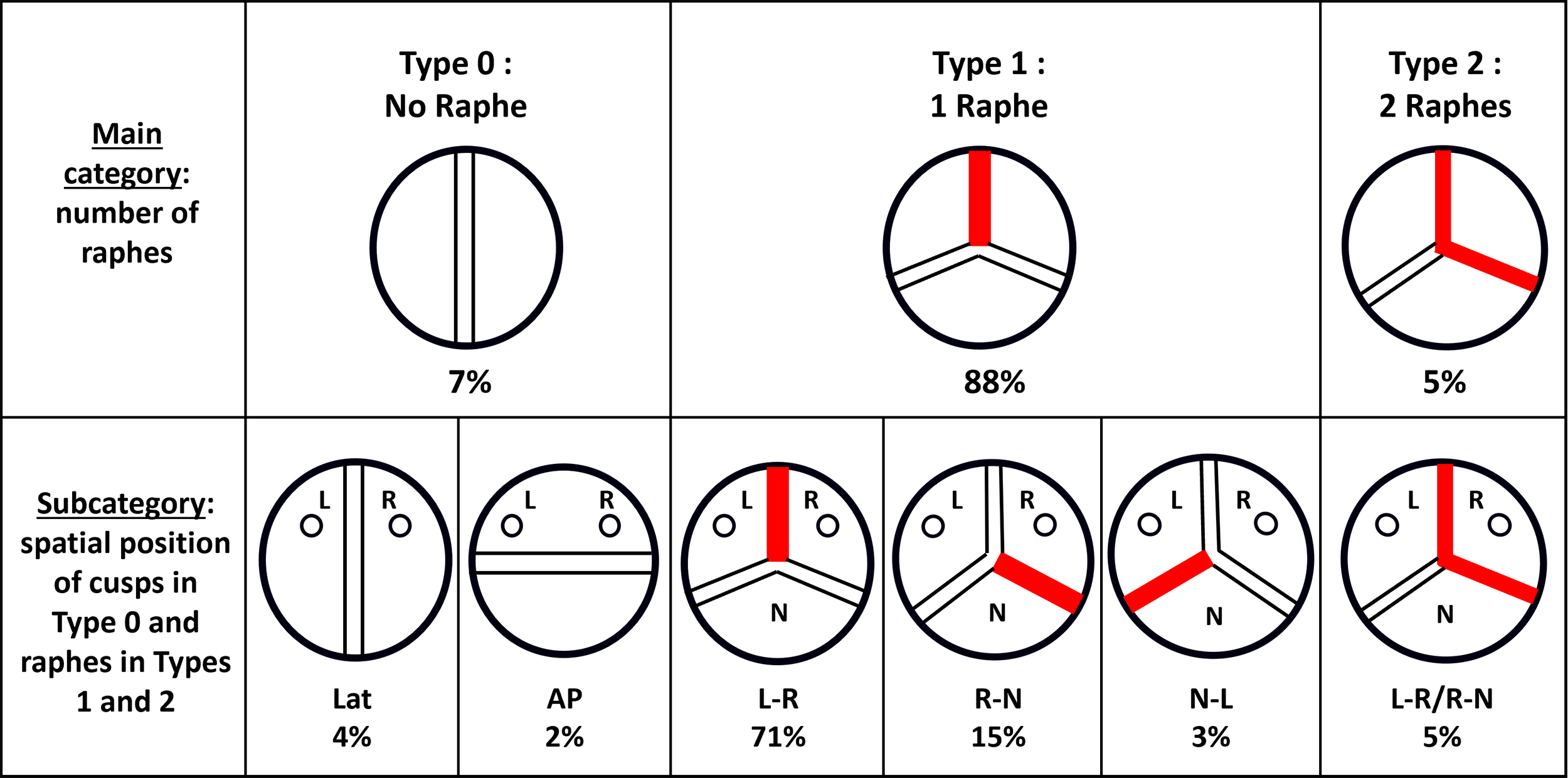 Fig. 5.
Fig. 5.
Schematic Overviews of Bicuspid Aortic Valve (BAV). Red lines in the schematic illustrations represent a raphe. BAV is classified into three main types based on the number of raphes: Type 0, with no raphe (7%); Type 1, the most common type of configuration, with one raphe (88%); and Type 2, with two raphes (5%). Each type is further categorized as AP, Lat, L-R, R-N, N-L, and L-R/R-N. AP, anterior-posterior; Lat, lateral; L, left coronary sinus; R, right coronary sinus; N, non-coronary sinus. Modified and reproduced with permission from Sato Y et al. Mastering Structural Heart Disease (pp.12). 1st edn. Wiley: NJ. 2023 [32].
BAVs often exhibit signs of calcification by the time individuals reach their thirties [92]. Calcification typically initiates in the raphe, appearing as a linear opacity on radiographs, and gradually extends toward the free margin of the leaflet, generally sparing the true commissures (Fig. 6). In severe AS cases related to BAVs, calcification spreads diffusely through the conjoint and non-conjoint cusps, involving the body of the leaflets. Calcific nodules potentially ulcerate the aortic surface (Fig. 6). The variability of the raphe in BAVs sometimes complicates the distinction between congenital and acquired BAV (e.g., rheumatic AS). In congenital BAVs, the raphe typically contains abundant elastic fibers, whereas acquired BAVs show collagen-rich fibrous tissue at fused commissures due to inflammatory scaring [93].
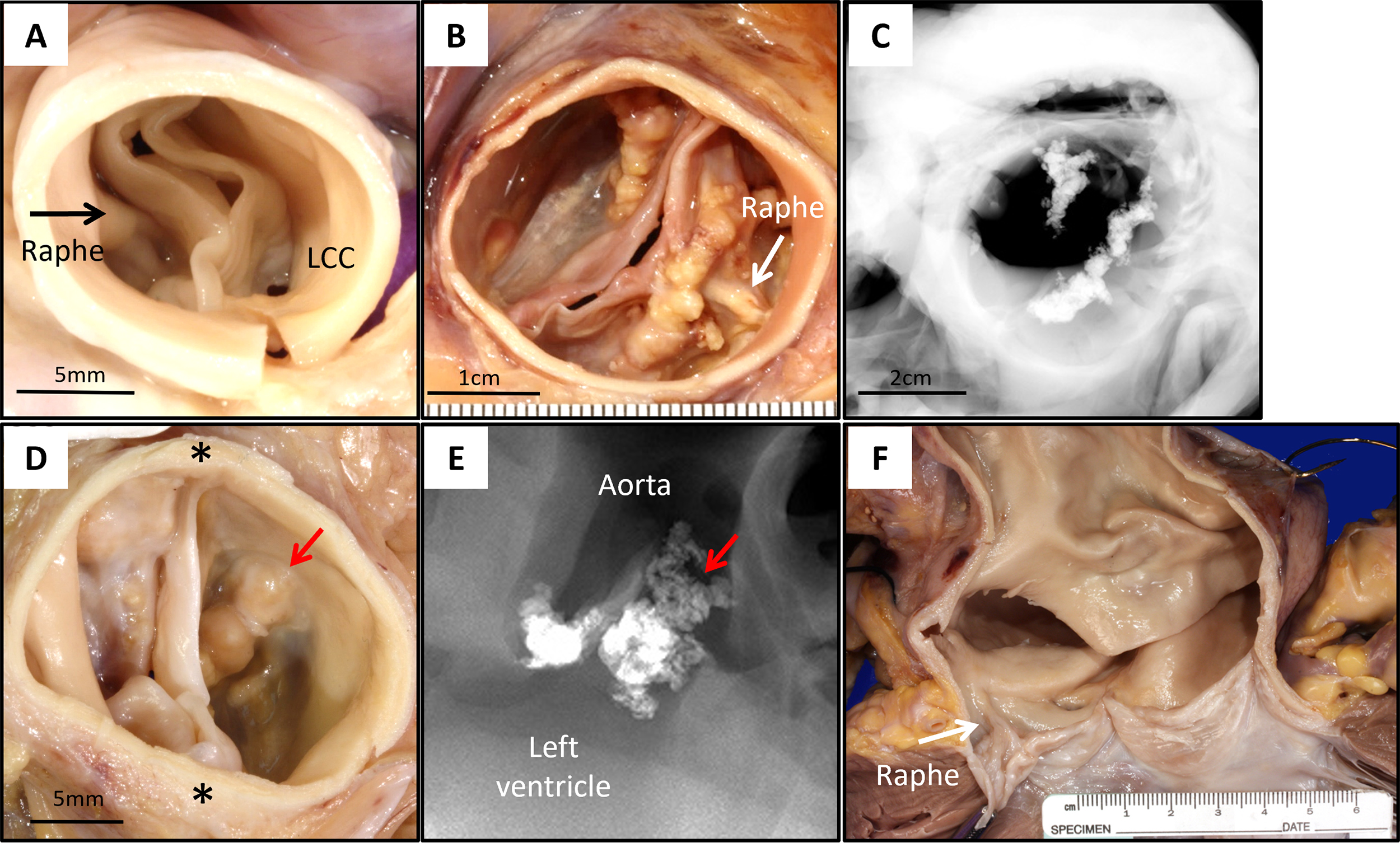 Fig. 6.
Fig. 6.
Representative Images of BAV. (A) Aortic valve from a 5-year-old male who experienced sudden death from unknown causes. Gross image from the aortic surface (A) shows BAV with a midline raphe between conjoint right and non-coronary cusps (black arrow). The conjoint cups are thickened and stiff with prominent raphe, without any calcification, scale bar: 5 mm. (B,C) Aortic valve from a 47-year-old male who experienced sudden death during motocross. (B) Gross image from aortic surface shows conjoint left and right coronary cusps, anterior calcified raphe (white arrow), and calcification of the aortic side of the non-coronary cusp near the left commissure, scale bar: 1 cm. (C) Radiography shows calcification corresponding to the gross image, scale bar: 2 cm. (D,E) Aortic valve from a 53-year-old male who experienced sudden death from unknown cause. (D) Gross image from the aortic surface shows calcific aortic stenosis arising in type 0 BAV: left and right coronary valve cusps with anterior-posterior commissures (*), no well-defined raphe, scale bar: 5 mm. (E) Radiography shows severe calcification corresponding to gross images (red arrows). (F) Gross image of the aortic valve and ascending aorta from a 38-year-old male who experienced sudden death from ruptured ascending aortic aneurysm. Note BAV with raphe (white arrow) between conjoint right and left coronary cusps is seen in (F). LCC, left coronary cusp.
UAVs are classified into two morphologic types: (1) an acommissural valve shaped like a dome with three aborted commissures (or raphes) and (2) a unicommissural valve, characterized by a slit-like opening extending through the aortic wall, with a single intact commissure (Fig. 7) [27]. The acommissural form is typically accompanied by left heart failure symptoms that develop early in life, whereas the unicommissural form has a less-aggressive course, as the presence of a commissure results in a relatively larger valvular orifice area compared to the acommissural form. Unicommissural unicuspid aortic valve accounts for 60% of AS cases in patients under 15 years of age [23]. Leaflet dysplasia is frequently observed, with varying degrees of leaflet calcification; however, dysplasia in UAVs is generally more severe compared to BAVs, and its severity is influenced by the patient’s age [30].
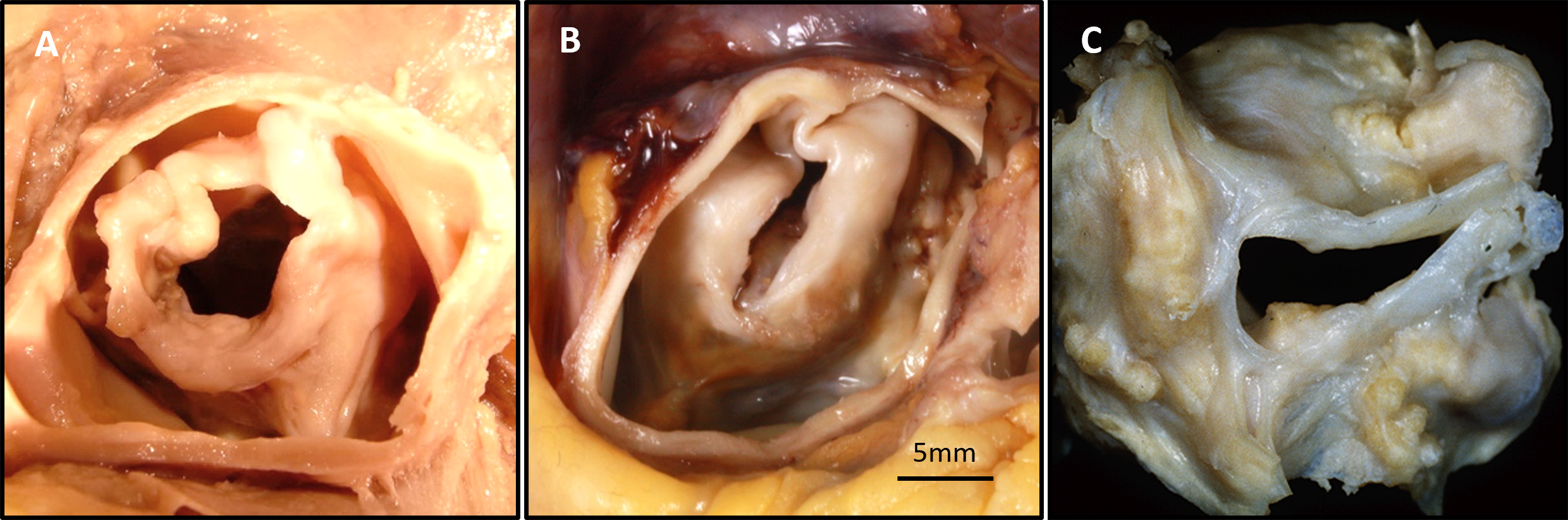 Fig. 7.
Fig. 7.
Representative Images of Unicuspid Aortic Valve (UAV). (A) UAV from a 47-year-old male who experienced sudden death from unknown causes. Gross images from the aortic surface shows dome-shaped UAV with three raphes, diffuse nodular calcification, an aortic orifice 1 cm in diameter, and concentric left ventricular hypertrophy. (B) UAV from a 28-year-old male who experienced sudden death from unknown causes. Gross image from the aortic surface shows calcific UAV with single left lateral commissure, right lateral, and anterior raphes, scale bar: 5 mm. (C) Surgically removed unicommissural aortic valve (AV).
Rheumatic heart disease occurs due to valvular damage triggered by an abnormal autoimmune response to a group A streptococcal infection, typically during childhood [94]. The use of penicillin as a preventive measure is highly effective and, in developed countries, has nearly eliminated rheumatic heart disease [95]. Nevertheless, this disease remains the leading cause of heart failure in children and young adults, resulting in at least 200,000–250,000 premature deaths every year in emerging nations [96]. A global cohort including 14 developing countries reported that rheumatic heart disease was twice as common among females, with a median age of 28 years [97].
The precise pathophysiology of the disease is not fully understood, but previous reviews have indicated that the main mechanism involves antigenic mimicry combined with an abnormal immune response from the host [98]. This process is based on three key factors: the presence of rheumatogenic group A streptococcal strains, a genetically susceptible host, and an abnormal immune response from the host. Genetically, human leukocyte antigen (HLA) class II molecules have been linked to an increased risk of the disease, although no single HLA haplotype or combination has consistently been tied to disease susceptibility [99]. CD4+ T cells are key players responding to cross-reactive antigens from streptococcal strains, which produce Th1 and potentially Th17 cytokines, leading to further inflammatory response in the heart valves [100, 101].
Typically, rheumatic heart disease affects multiple valves. The most common pattern is a combination of aortic and mitral valve disease, followed by mixed mitral valve disease. Isolated aortic valve disease is rare (2–10%) [97, 102, 103]. In contrast to bicuspid AS and senile AS, rheumatic AS has relatively little calcification [21]. Cuspid thickening and commissural fusion of at least one and generally two or three commissures are the hallmark of this disease (Fig. 8, Ref. [9]) [104, 105].
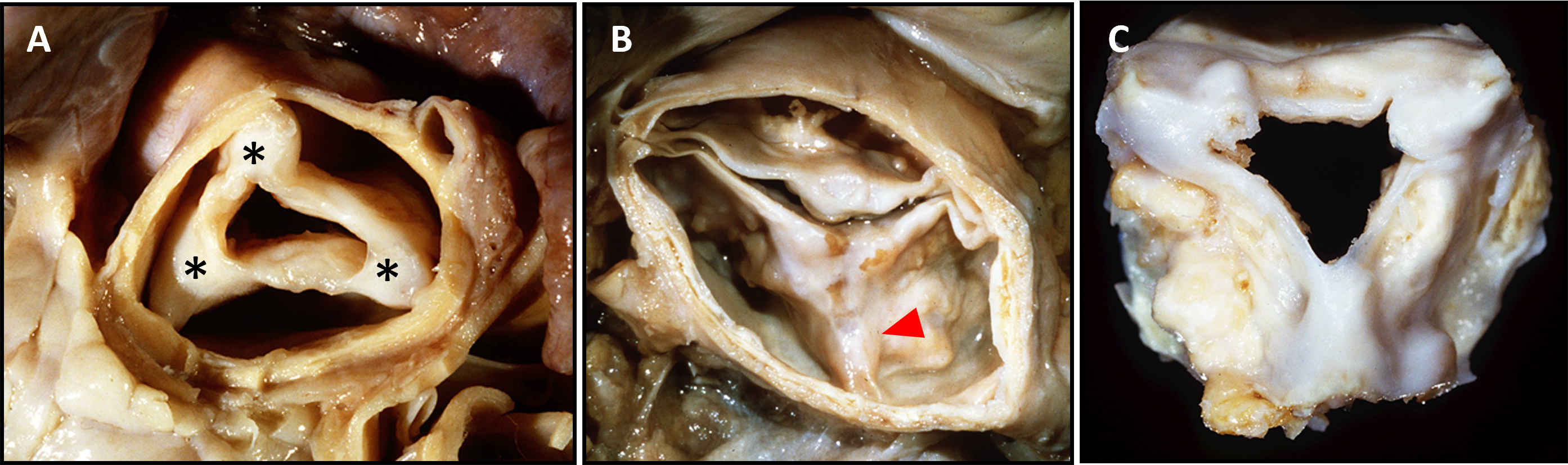 Fig. 8.
Fig. 8.
Representative Images of Post-Rheumatic Aortic Valve Diseases. (A) A 44-year-old male with known heart disease was found dead. At autopsy, he had an enlarged heart with severe mitral stenosis and aortic stenosis. Note fusion of all three aortic valve commissures (*), thickening and fibrosis of all three aortic leaflets, and no calcification. (B) An acquired bicuspid stenotic aortic valve was found in this 65-year-old man who died while awaiting valve replacement. The anterior commissure is fused (red arrowhead), and this commissure is at the same level as and equidistant from the other two non-fused commissures. (C) A surgically excised aortic valve in a 50-year-old female with mitral and aortic stenosis. All three commissures are fused, and cusp fibrosis and calcification are evident with calcification present both in the commissures and leaflets. Reproduced with permission from Virmani R et al. Cardiovascular pathology (pp. 254). 2nd edn. W.B. Saunders Company: Philadelphia, 2001 [9].
When conducting valve replacement surgery, the selection of prosthesis (whether bioprosthetic or mechanical) requires careful consideration, taking into account the patient’s age, potential for pregnancy, and the likelihood of adherence to anticoagulant therapy, particularly in remote or socioeconomically disadvantaged areas [106].
The only curative treatment available for patients with symptomatic severe AS is the implantation of a prosthetic heart valve, either surgically or percutaneously. Traditionally, the choice between TAVR and SAVR was often straightforward, based on age, anatomy, and surgical risk. However, current recommendations emphasize a more comprehensive approach, considering multiple factors when choosing a prosthetic valve, including the severity, symptoms, left ventricular function, comorbidities, frailty, cognitive function, and patients’ preferences [107, 108].
Specifically, in current American College of Cardiology (ACC)/American Heart Association (AHA) guidelines, SAVR is recommended for patients
who are
Moreover, both the ACC/AHA and the ESC/EACTS guidelines suggest that SAVR is
more appropriate for BAV cases [107, 108]. However, a recent randomized trial
showed that among low-risk patients aged
Although no medical therapies are currently approved, several novel treatment
strategies have been explored based on an advanced understanding of the
underlying pathophysiological mechanisms [110]. These include therapies targeting
lipoprotein(a), such as niacin, antisense oligonucleotide therapy, and proprotein
convertase subtilisin/kexin type 9 (PCSK9) inhibitors; bisphosphonates targeting
the receptor activator of nuclear factor kappa-B (NF-
Previous analyses of randomized control trials or propensity score-matched analyses from registries comparing TVAR vs. SAVR revealed assuring results on the midterm durability of TAVR, which are favorable when compared to SAVR [111]. The incidence of all-cause TAVR bioprosthetic valve failure was as follows: (i) PARTNER 2A and SAPIEN 3 intermediate-risk registry: 4.7% in TAVR with SAPIEN XT, 2.6% in TAVR with SAPIEN 3 vs. 1.3% in SAVR at 5 years [112]; (ii) PARTNER 3: 3.3% in TAVR with SAPIEN 3 vs. 3.8% in SAVR at 5 years [113]; and (iii) NOTION RCT: 9.7% in TVAR with CoreValve vs. 13.8% in SAVR at 10 years [114]. Therefore, with the exception of the first generation of SAPIEN valves, the midterm (up to 7–8 years) durability of TAVR valves is at least comparable to that of SAVR valves. The NOTION RCT is the only trial that has reached 10-year follow-up. Although the results of this trial are quite promising, no definitive conclusion can be made on the long-term durability of TAVR based on these findings, because this trial had several limitations: one was that only 25% of the patients remained alive after 10 years; the other was that the TAVR arm only included first-generation valves, and the SAVR arm included 35% of the Trifecta (Abbott) or Mitroflow (Sorin) valves, which have both been shown to have durability concerns. The long-term durability of TVAR valves will need to be confirmed by analyses of the low-risk TAVR vs. SAVR trials at 10 years [113, 115].
We have recently reported our findings on bioprosthetic valve dysfunction in SAVR and TAVR valves that were removed surgically or at autopsy. Bioprosthetic valve dysfunction means impaired functional performance of the bioprosthetic valve, encompassing four types: structural valve deterioration (SVD), non-SVD, thrombosis, and endocarditis [108, 116, 117]. Among these, SVD is the most prevalent cause of failure, and is characterized by irreversible changes in the bioprostheses due to leaflet thickening, fibrosis, pannus formation, calcification, and leaflet tear [111]. We previously published on 43 TAVR cases [118, 119] from the PARTNER trial [120] as well as the CoreValve U.S. Pivotal High-Risk Trial [121]. In two cases of Edwards SAPIEN valves with bovine pericardial leaflets, valve calcification was observed (Fig. 9, Ref. [118]). In addition, valve leaflet thrombosis is one of the most important causes of bioprosthetic valve dysfunction, which can be observed as “hypo-attenuated leaflet thickening (HALT)” by computed tomography. Subclinical leaflet thrombosis may occur in as much as 5 to 25% of patients during the first year following TAVR or SAVR [122, 123]. Valve thrombi observed histologically within 30 days are primarily platelet-rich, whereas those seen after 30 days are predominantly fibrin-rich, with or without signs of organization. These later-stage thrombi show the presence of smooth muscle cells within a proteoglycan- and type III collagen-rich matrix (neointima formation) (Fig. 10, Ref. [124]) [118, 119].
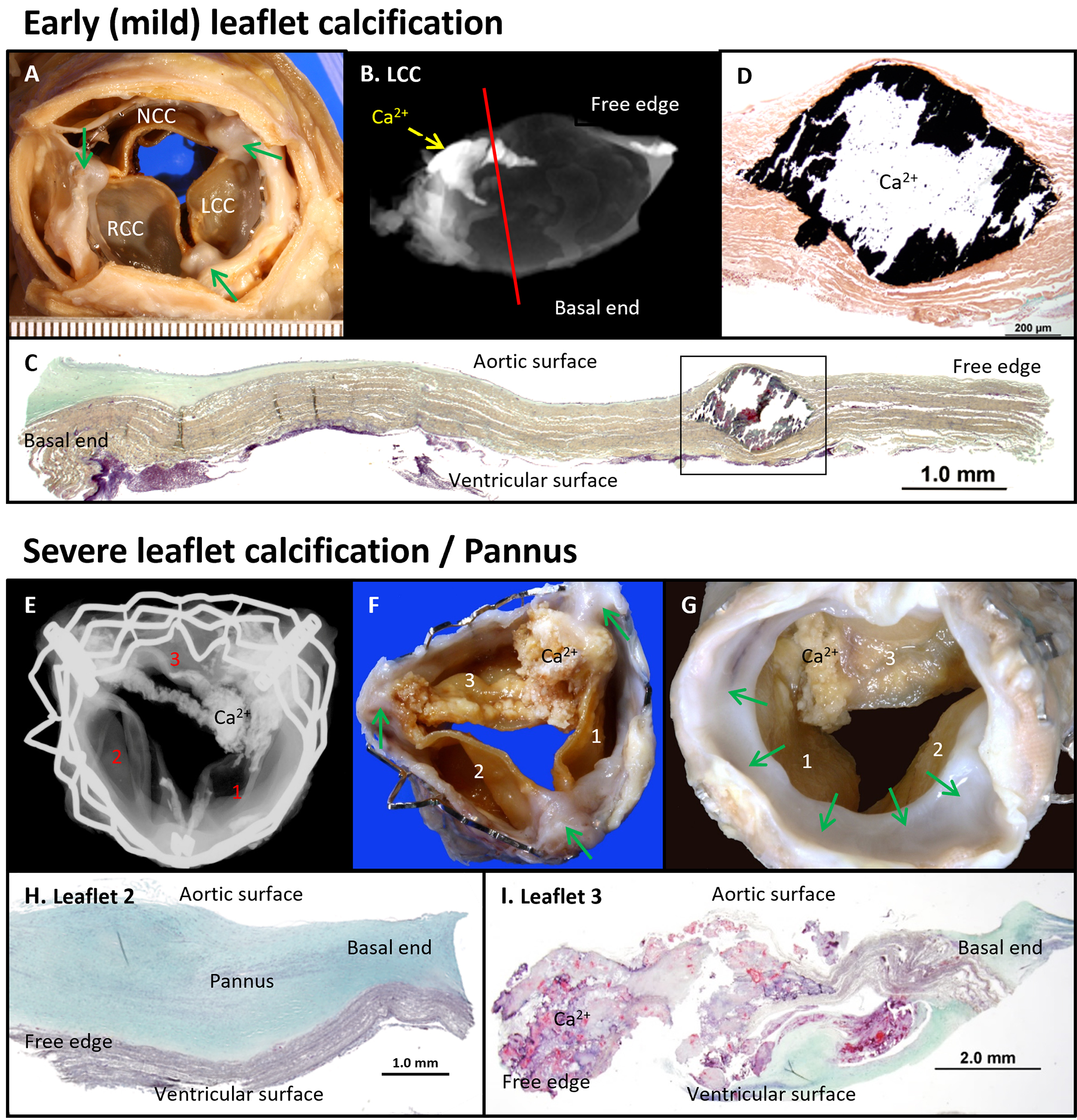 Fig. 9.
Fig. 9.
Calcification and Pannus Formation in Edwards SAPIEN TAVR Leaflets. Early leaflet calcifications observed four years after implantation (A–D). (A) Gross image from the aortic surface showing commissural fusion (green arrows). (B) Radiographic image highlighting focal calcification (Ca2+) at the commissure site. (C) Histologic section showing focal intrinsic calcification in the valve leaflet (Movat Pentachrome stain), scale bar: 1.0 mm. (D) High-power image of the black boxed area in D (von Kossa stain), scale bar: 200 µm. Severe leaflet calcification with pannus formation observed in a surgically removed TAVR valve five years following the implantation (E–I). (E) Radiograph showing severe leaflet calcification (Ca2+), predominantly at the commissure sites between leaflet 1 and 3. (F,G) Gross images from the aortic and ventricular surfaces, respectively, with green arrows showing pannus formation, mainly on the ventricular surface. (H) Histologic section revealing a thick pannus composed of smooth muscle cells in a proteoglycan (green) collagenous matrix on leaflet 2, scale bar: 1.0 mm. (I) Severe calcification with neointimal growth in leaflet 3, scale bar: 2.0 mm. Modified and reproduced with permission from Yahagi K et al. Catheter Cardiovasc Interv 2017; 90: 1048–1057 [118]. NCC, non-coronary cusp; RCC, right coronary cusp.
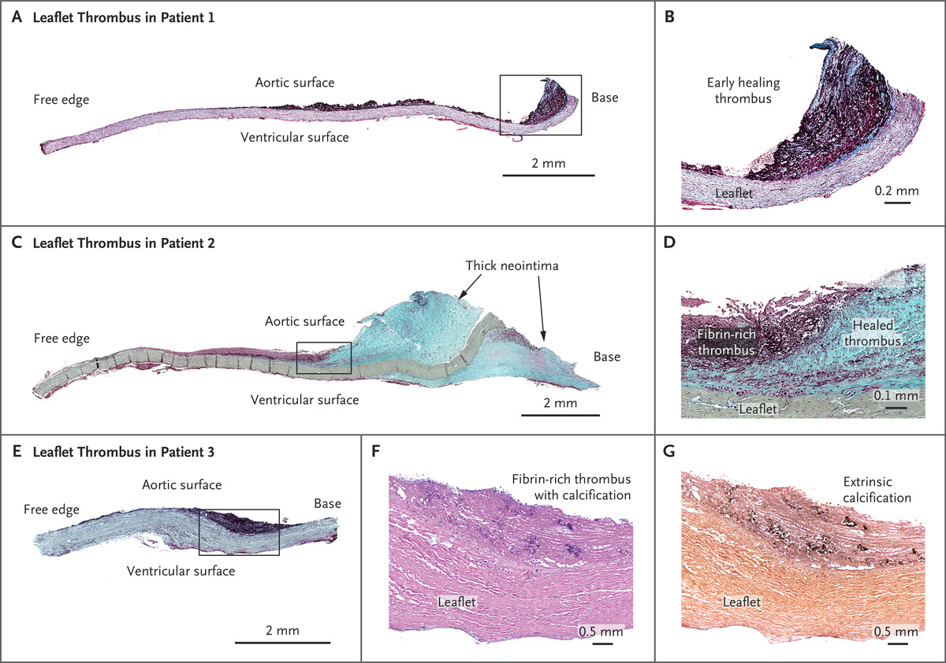 Fig. 10.
Fig. 10.
Histological Images of Leaflet Thrombus from Patients Who Underwent TAVR. (A) Low-power image of a leaflet with fibrin-rich thrombus on the aortic surface, 38 days after implantation, scale bar: 2 mm. (B) High-power image of the boxed area in (A) showing the thrombus attached to the base of the leaflet, with early thrombus organization indicated by visible proteoglycan (green areas within the magenta-colored thrombus), scale bar: 0.2 mm. (C) Low-power image of a leaflet at 105 days after implantation, showing fibrin-rich thrombus in the midportion and a thickened neointima from healed thrombus at the base, on both the aortic and ventricular surfaces, scale bar: 2 mm. (D) High-power image of the boxed area in (C), showing organizing thrombus, with fibrin-rich thrombus transitioning to smooth muscle cells in a proteoglycan matrix (green), scale bar: 0.1 mm. (E) Low-power image of a leaflet at 517 days after implantation showing fibrin-rich thrombus on the aortic surface, scale bar: 2 mm. (F) High-power image of the leaflet thrombus, with purple areas indicating calcification (H&E stain), scale bar: 0.5 mm. (G) Early spotty extrinsic calcification in the thrombus (von Kossa stain), scale bar: 0.5 mm. All specimens in panels (A–E) are stained with Movat Pentachrome. TAVR, transcatheter aortic valve replacement. Reproduced with permission from Yahagi K et al. N Engl J Med 2020; 383(2): e8 [124].
AS is an age-related disease and previous clinical trials have identified age as the most significant risk factor associated with aortic stenosis or sclerosis [35]. However, recent studies have revealed that calcific AS is not merely a “degenerative” disease caused by time-dependent wear and tear of the leaflets Instead, it is now considered to involve active cellular mechanisms including lipoprotein deposition, chronic inflammation, and mineralization, similar to that of atherosclerotic disease progression. These processes could potentially be targeted by medical treatments; however, to date, no pharmacological treatments are able to successfully halt the progression of AS or improve long-term outcomes. As a result, treatment is currently limited to SAVR or TAVR, which can be too invasive for elderly patients.
The onset and progression of AS varies significantly depending on the types of AS. Congenital AS (e.g., bicuspid and unicuspid AS) and rheumatic AS tend to develop at a younger age. In contrast, degenerative AS in tricuspid valve typically occurs at an older age. Given the aging population and increased life expectancy, the need for treatment of symptomatic AS in elderly patients is growing and is expected to continue increasing without effective medical treatment. TAVR has become an important, minimally invasive option for elderly AS patients; however, its long-term outcome remains to be fully elucidated. A key concern is the durability of TAVR valves over time, as bioprosthetic valve dysfunction can occur due to various mechanisms. Understanding the underlying causes and mechanisms is crucial for making appropriate treatment choices (i.e., valve selection and pharmacological therapy) and essential for effective lifetime management of AS.
TH conceived and designed the review, performed most of the literature analysis, and wrote the manuscript. TS contributed to the literature analysis. AVF was involved in the conception and design of the review, and in critically reviewing the draft for important intellectual content. RV was involved in the conception and design of the review, the development of the framework, and key themes, as well as offering supervision and overall guidance throughout the project. All authors contributed to editorial changes in the manuscript. All authors read and approved of the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
Not applicable.
This research received no external funding.
CVPath Institute has received institutional research support from NIH-HL141425, Leducq Foundation Grant, 4C Medical, 4Tech, Abbott Vascular, Ablative Solutions, Absorption Systems, Advanced NanoTherapies, Aerwave Medical, Alivas, Amgen, Asahi Medical, Aurios Medical, Avantec Vascular, BD, Biosensors, Biotronik, Biotyx Medical, Bolt Medical, Boston Scientific, Canon, Cardiac Implants, Cardiawave, CardioMech, Cardionomic, Celonova, Cerus, EndoVascular, Chansu Vascular Technologies, Children’s National, Concept Medical, Cook Medical, Cooper Health, Cormaze, CRL, Croivalve, CSI, Dexcom, Edwards Lifesciences, Elucid Bioimaging, eLum Technologies, Emboline, Endotronix, Envision, Filterlex, Imperative Care, Innovalve, Innovative Cardiovascular Solutions, Intact Vascular, Interface Biolgics, Intershunt Technologies, Invatin, Lahav, Limflow, L&J Bio, Lutonix, Lyra Therapeutics, Mayo Clinic, Maywell, MDS, MedAlliance, Medanex, Medtronic, Mercator, Microport, Microvention, Neovasc, Nephronyx, Nova Vascular, Nyra Medical, Occultech, Olympus, Ohio Health, OrbusNeich, Ossio, Phenox, Pi-Cardia, Polares Medical, Polyvascular, Profusa, ProKidney, LLC, Protembis, Pulse Biosciences, Qool Therapeutics, Recombinetics, Recor Medical, Regencor, Renata Medical, Restore Medical, Ripple Therapeutics, Rush University, Sanofi, Shockwave, SMT, SoundPipe, Spartan Micro, Spectrawave, Surmodics, Terumo Corporation, The Jacobs Institute, Transmural Systems, Transverse Medical, TruLeaf, UCSF, UPMC, Vascudyne, Vesper, Vetex Medical, Whiteswell, WL Gore, Xeltis. AVF. has received honoraria from Abbott Vascular; Biosensors; Boston Scientific; Celonova; Cook Medical; CSI; Lutonix Bard; Sinomed; Terumo Corporation; and is a consultant to Amgen; Abbott Vascular; Boston Scientific; Celonova; Cook Medical; Lutonix Bard; and Sinomed. RV is a consultant/scientific advisory board member of Abbott Vascular; Bosten Scientific; Celonova; Cook Medical; CSI; Edwards Lifesciences; Bard BD; Medtronic; OrbusNeich Medical; ReCor Medical; SinoMedical Sciences Technology; Surmodics; Terumo Corporation; W. L. Gore; and Xeltis. The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.