

 , Yan Pu 1,2,*,†
, Yan Pu 1,2,*,†
1 Department of Reproductive Medicine Nursing, West China Second University Hospital, Sichuan University, 610041 Chengdu, Sichuan, China
2 Key Laboratory of Birth Defects and Related Diseases of Women and Children (Sichuan University), Ministry of Education, 610041 Chengdu, Sichuan, China
†These authors contributed equally.
Abstract
Psychological stress in infertile individuals undergoing artificial insemination with their husband’s sperm (AIH) remains understudied, despite its potential impact on reproductive outcomes. The current study aimed to evaluate the prevalence, influencing factors, and effects of psychological stress on conception success in a population undergoing AIH.
This retrospective cohort study analyzed data from 976 patients treated between June 2020 and January 2024. Standardized psychological assessments were used to evaluate anxiety, depression, somatic symptoms, and sleep quality. These included generalized anxiety disorder 7-item (GAD-7), patient health questionnaire 9-item (PHQ-9), patient health questionnaire 15-item (PHQ-15), and the Pittsburgh Sleep Quality Index. Logistic regression analysis was performed to identify predictors of stress and their association with clinical pregnancy rates.
Younger age (<30 years) was significantly correlated with higher anxiety (odds ratio (OR) = 1.801, p = 0.012). Whilst, unemployment (OR adjusted = 2.183, p = 0.002) and prolonged duration (3–5 years) of infertility (OR adjusted = 1.445, p = 0.014) were significantly correlated with somatic symptoms. Moreover, unemployment (OR adjusted = 2.020, p = 0.008) and prolonged duration (≥5 years) of infertility (OR adjusted = 1.780, p = 0.008) were also significantly correlated with sleep disorders. However, no direct links were found between anxiety, depression, somatic symptoms or sleep quality and conception outcomes.
Our findings highlight the need to target psychological interventions for specific populations, including younger individuals, unemployed persons, and patients experiencing prolonged infertility.
Keywords
- psychological stress
- artificial insemination
- conception success
- cohort study
Artificial insemination with the husband’s sperm (AIH) is a fundamental assisted
reproductive technology (ART) involving transuterine deposition of processed
spermatozoa during the ovulatory window [1, 2]. This technique preserves genetic
parenthood, distinguishing it from donor insemination, and circumvents cervical
factors to achieve clinical pregnancy rates (CPR) of 8%–15% per cycle in
unexplained infertility [1]. Population-specific data from China demonstrate an
overall CPR of 13.0% across 3015 AIH cycles [3], consistent with global
estimates. Published evidence has established that ovarian stimulation combined
with intrauterine insemination (IUI-OS) significantly increases live birth rates
(LBR) and CPR up to 3-fold compared to expectant management, thus supporting its
role as a first-line therapeutic strategy for unexplained infertility [4].
Current evidence-based guidelines recommend age-stratified treatment algorithms,
with IUI-OS being indicated for women aged
Accumulating evidence confirms that psychological stress adversely impacts AIH
outcomes [5]. Elevated depressive symptoms (center for epidemiological studies
depression scale (CES-D)
The psychosocial burden associated with AIH stems from multifactorial stressors
encompassing socioeconomic constraints, interpersonal discord, and cultural
expectations. A cross-sectional analysis of 175 AIH patients revealed an inverse
correlation between the severity of anxiety and the magnitude of perceived social
support (
A prospective study combined psychological stress assessments with the analysis
of salivary biomarkers (
The present study aimed to address these gaps by evaluating the prevalence and severity of psychological stress in AIH patients, identifying modifiable psychosocial and biological predictors of stress, and measuring how stress affects pregnancy outcomes.
This single-center cohort study evaluated psychological stress levels in patients undergoing IUI with their husband’s sperm. In addition, we identified associated factors and assessed the impact of stress on clinical pregnancy outcomes. This retrospective cohort study utilized data that were collected prospectively within the electronic medical records database of the Center of Reproductive Medicine, West China Second University Hospital, Sichuan University.
The study population comprised of patients who initiated IUI cycles using their partner’s sperm between June 2020 and January 2024. Initial screening identified 1946 patients who had undergone psychological assessment during their treatment period (Fig. 1). To increase internal validity and mitigate confounding factors, stringent exclusion criteria were applied: (1) the use of donor sperm (n = 566); (2) treatment discontinuation (n = 127); and (3) started IUI treatment more than two months after psychological assessment (n = 229). Following these exclusions, 1024 participants were eligible for inclusion in the study. Subsequent analysis revealed that 48 treatment cycles were cancelled for various clinical reasons, resulting in a final analytical cohort of 976 completed IUI cycles.
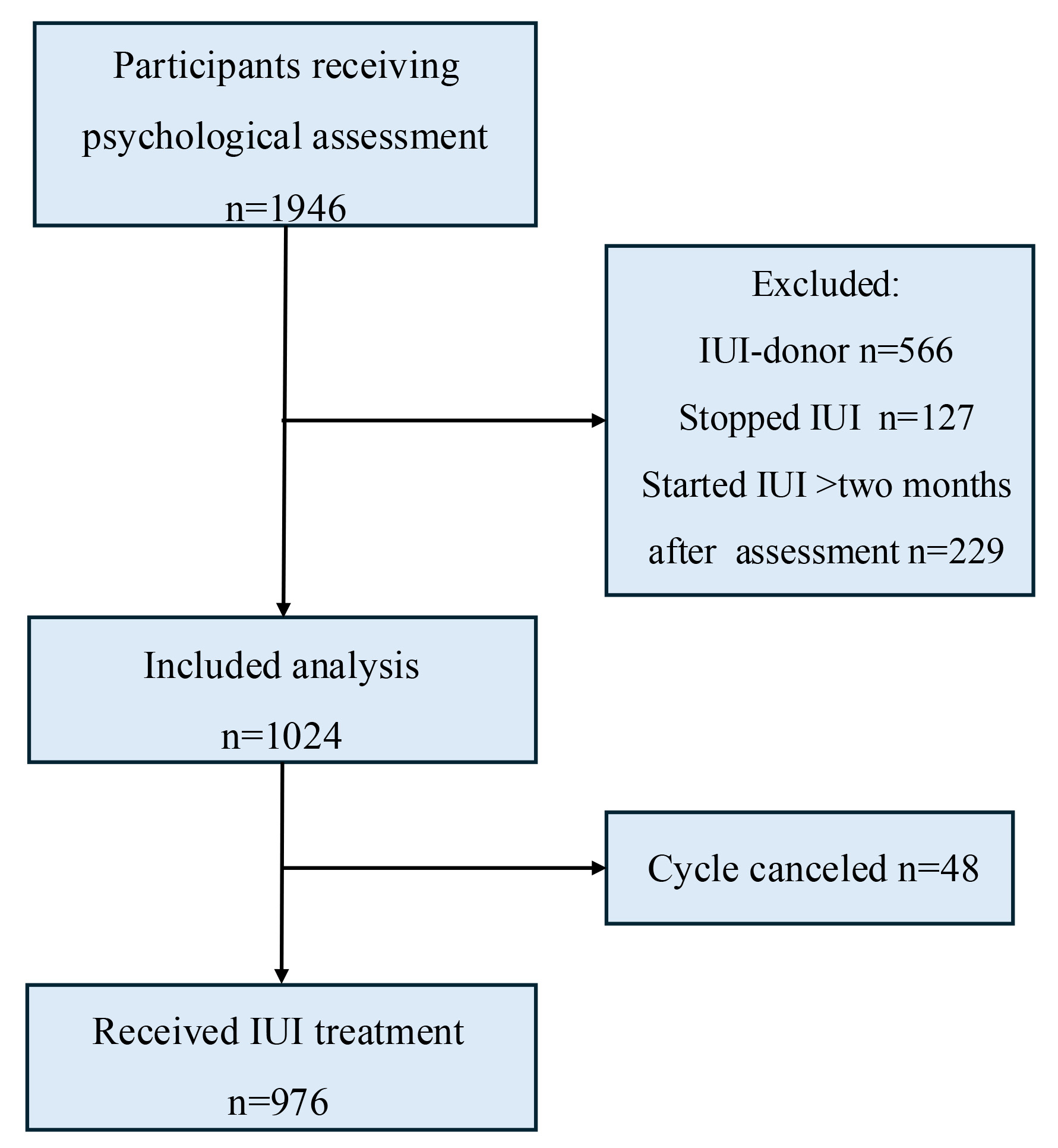 Fig. 1.
Fig. 1.
Flow chart of the study (IUI, intrauterine insemination).
The severity of anxiety symptoms was assessed using the generalized anxiety disorder 7-item scale (GAD-7),
initially developed by Spitzer et al. [13] and subsequently
translated and introduced to China by China by He XY et al. [14]. GAD-7 is a self-rating scale for
anxiety-related symptoms experienced in the 2 weeks prior. Each item is scored on
a four-point Likert scale of 0–3, with 0 indicating “not at all” and 3
indicating “almost every day”. The reliability and validity of GAD-7 were
confirmed in previous studies [14, 15]. The Cronbach’s
The patient health questionnaire 9-item (PHQ-9) initially developed by Kroenke et al.
[16] was used to assess the severity of the depression-related symptoms. PHQ-9 is
a self-rating scale for symptoms related to depression which have been
experienced in the past 2 weeks. Each item is scored on a four-point Likert scale
of 0–3, with 0 indicating “not at all” and 3 indicating “almost every day”.
PHQ-9 is widely used in both clinic and community settings, and was introduced to
China in 2007 [17]. The reliability and validity of PHQ-9 have been demonstrated
in infertile populations in mainland China [18]. The Cronbach’s
The patient health questionnaire 15-item (PHQ-15) used in this study to evaluate
the patient’s somatic symptoms was initially developed by Kroenke et al. [19]. PHQ-15 is
a self-rating scale for the severity of somatic symptoms experienced during the
past 2 weeks. Each item is scored on a four-point Likert scale of 0–2, with 0
indicating “no influence at all” and 2 indicating “significant influence”.
PHQ-15 is widely used in both clinical and community settings, and its
reliability and validity have been demonstrated in infertile populations in
mainland China [18]. The Cronbach’s
Patient sleep quality was evaluated using the Pittsburgh Sleep Quality Index
(PSQI), which is a self-rating scale for sleep quality and disturbances over a
1-month time interval. The PSQI evaluates subjective sleep quality, latency,
duration, efficiency, disturbances, use of sleep medication, and daytime
dysfunction. The score for each part is between 0–3 points, and the global score
(sum of these 7 components) ranges from 0 to 21. The reliability and validity of
PSQI have been demonstrated in mainland China [20]. The Cronbach’s
Psychological assessments were part of standard clinical data collection in our department, used to identify individuals with severe negative emotions. Before a patient entered the artificial insemination cycle, trained nurses guided them through the psychological assessment. The patient was informed of the result at the completion of the assessment. Patients with no or only mild symptoms received psychological guidance from the department’s counselors. Those evaluated as having moderate or severe symptoms were referred for psychological counseling in the outpatient department. Data collection was performed through the hospital’s electronic medical records system. All clinical data was prospectively collected. Primary data was collected for demographic characteristics such as age, body mass index (BMI), whether the patient was undergoing IUI for the first time, the health status of the partner, and the patient’s fertility history (e.g., duration of infertility, prior pregnancies). In addition to psychological assessment data, information related to treatment was also collected, including the treatment regimen (e.g., the use of ovulation-stimulating drugs), the number of treatment cycles, the number of IUI attempts, and the final treatment outcome (i.e., whether the patient became pregnant).
Data analysis was performed using SPSS 26.0 (IBM Corp., Armonk, NY, USA), with a
significance level set at p
The demographic and fertility characteristics of the 1024 participants included
in this study were examined in detail (Table 1). Analysis of the age distribution
showed that 29.30% of participants were
| Characteristics | n (%)/median (IQR) | ||
| Female | |||
| Age (years) | |||
| 300 (29.30) | |||
| 30–34 | 575 (56.20) | ||
| 149 (14.50) | |||
| Ethnicity | |||
| Han | 986 (96.30) | ||
| Minority | 38 (3.70) | ||
| Marital status | |||
| First marriage | 961 (93.80) | ||
| Digamy | 63 (6.20) | ||
| Occupational status | |||
| Employed | 950 (92.80) | ||
| Not working | 74 (7.20) | ||
| Educational degree | |||
| Junior college and below | 420 (41.02) | ||
| Bachelor | 462 (45.12) | ||
| Master and above | 142 (13.86) | ||
| Preconception BMI | |||
| Low ( |
126 (12.30) | ||
| Normal ( |
780 (76.20) | ||
| Overweight/obesity ( |
117 (11.40) | ||
| Missing data | 1 (0.10) | ||
| Duration of infertility | 2.61 (1.83) | ||
| Previous pregnancy | 269 (26.30) | ||
| Gravida (time), median (IQR) | 0 (1.00) | ||
| Parity (time), median (IQR) | 0 (0) | ||
| Spontaneous abortion (time), median (IQR) | 0 (0) | ||
| Induced abortion (time), median (IQR) | 0 (0) | ||
| Male | |||
| Age (years) | |||
| 206 (20.12) | |||
| 30–34 | 540 (52.73) | ||
| 278 (27.15) | |||
| Ethnicity | |||
| Han | 986 (96.30) | ||
| Minority | 36 (3.50) | ||
| Other | 1 (0.10) | ||
| Missing data | 1 (0.10) | ||
| Marital status | |||
| First marriage | 942 (92.00) | ||
| Digamy | 82 (8.00) | ||
| Occupational status | |||
| Employed | 1010 (98.60) | ||
| Not working | 14 (1.40) | ||
| Educational degree | |||
| Junior college and below | 385 (37.60) | ||
| Bachelor | 480 (46.90) | ||
| Master and above | 159 (15.50) | ||
IQR, interquartile range; BMI, body mass index.
Descriptive data on psychological symptoms, including anxiety, depression, somatic symptoms, and sleep disorders, were collected using the standardized scales GAD-7, PHQ-9, PHQ-15, and PSQI (Table 2). Abnormal anxiety levels were seen in 29.10% of participants and abnormal depression levels in 34.20%, while 57.30% of participants reported no somatic symptoms and 79.60% had good sleep quality.
| Classification | n (%) | |
| GAD-7 | ||
| Normal (0–4) | 726 (70.90) | |
| Abnormal (5–21) | 298 (29.10) | |
| PHQ-9 | ||
| Normal (0–4) | 674 (65.80) | |
| Abnormal (5–27) | 350 (34.20) | |
| PHQ-15 | ||
| Normal (0–4) | 587 (57.30) | |
| Abnormal (5–30) | 437 (42.70) | |
| PSQI | ||
| Good (0–6) | 815 (79.60) | |
| Poor (7–21) | 209 (20.40) | |
Note: GAD-7, generalized anxiety disorder 7-item; PHQ-9, patient health questionnaire 9-item; PHQ-15, patient health questionnaire 15-item; PSQI, pittsburgh sleep quality index.
Table 3 shows the relationships between anxiety, depression, somatic symptoms,
and sleep quality with various demographic and fertility characteristics. A
linear relationship was found between age and anxiety (
| Variables | Total, n (%) | Anxiety symptom | Depressive symptom | Somatic symptom | Sleep quality | ||||||||||
| yes | no | yes | no | yes | no | poor | good | ||||||||
| Female | |||||||||||||||
| Age (years) a | 6.03*b | 1.87 | 2.03 | 0.21 | |||||||||||
| 300 (29.30) | 99 (33.00) | 201 (67.00) | 112 (37.30) | 188 (62.70) | 137 (45.70) | 163 (54.30) | 57 (19.00) | 243 (29.80) | |||||||
| 30–34 | 575 (56.20) | 167 (29.00) | 408 (71.00) | 191 (33.20) | 384 (66.80) | 242 (42.10) | 333 (57.90) | 122 (21.20) | 453 (78.80) | ||||||
| 149 (14.50) | 32 (21.50) | 117 (78.50) | 47 (31.50) | 674 (65.80) | 58 (38.90) | 91 (61.10) | 30 (20.10) | 119 (79.90) | |||||||
| Ethnicity | 0.04 | 0.77 | 0.06 | 0.09 | |||||||||||
| Han | 986 (96.30) | 288 (29.20) | 698 (70.80) | 334 (33.90) | 652 (66.10) | 422 (42.80) | 564 (57.20) | 200 (20.30) | 786 (79.70) | ||||||
| Minority | 38 (3.70) | 10 (26.30) | 28 (73.70) | 16 (42.10) | 22 (57.90) | 15 (39.50) | 23 (60.50) | 9 (23.70) | 29 (76.30) | ||||||
| Marital status | 0.66 | 2.74 | 0.19 | ||||||||||||
| First marriage | 961 (93.80) | 283 (29.40) | 678 (70.60) | 335 (34.90) | 626 (65.10) | 410 (42.70) | 551 (57.30) | 198 (20.60) | 763 (79.40) | ||||||
| Digamy | 63 (6.20) | 15 (23.80) | 48 (76.20) | 15 (23.80) | 48 (76.20) | 27 (42.90) | 36 (57.10) | 11 (17.50) | 52 (82.50) | ||||||
| Occupational status | 1.76 | 11.54** | 7.92* | ||||||||||||
| Employed | 950 (92.80) | 276 (29.10) | 674 (70.90) | 319 (33.60) | 631 (66.40) | 391 (41.20) | 559 (58.80) | 184 (19.40) | 766 (80.60) | ||||||
| Not working | 74 (7.20) | 22 (29.70) | 52 (70.30) | 31 (41.90) | 43 (58.10) | 46 (62.20) | 28 (37.80) | 25 (33.80) | 49 (66.20) | ||||||
| Educational degree a | 0.65 | 0.04 | 1.08 | 1.60 | |||||||||||
| Junior college and below | 420 (41.00) | 126 (30.00) | 294 (70.00) | 149 (35.50) | 271 (64.50) | 191 (45.50) | 229 (54.50) | 94 (22.40) | 326 (77.60) | ||||||
| Bachelor | 462 (45.10) | 135 (29.20) | 327 (70.80) | 145 (31.40) | 317 (68.60) | 185 (40.00) | 277 (60.00) | 89 (19.30) | 373 (80.70) | ||||||
| Master and above | 142 (13.90) | 37 (26.10) | 105 (73.90) | 56 (39.40) | 86 (60.60) | 61 (43.00) | 81 (57.00) | 26 (18.30) | 116 (81.70) | ||||||
| Duration of infertility (years) a | 1.00 | 3.80 | 5.27*c | 6.53*d | |||||||||||
| 607 (59.30) | 173 (28.50) | 434 (71.50) | 193 (31.80) | 414 (68.20) | 237 (39.00) | 370 (61.00) | 112 (18.50) | 495 (81.50) | |||||||
| 3–5 | 27 (27.20) | 78 (28.00) | 201 (72.00) | 103 (36.90) | 176 (63.10) | 137 (49.10) | 142 (50.90) | 57 (20.40) | 222 (79.60) | ||||||
| 138 (13.50) | 47 (34.10) | 91 (65.90) | 54 (39.10) | 84 (60.90) | 63 (45.70) | 75 (54.30) | 40 (29.00) | 98 (71.00) | |||||||
| Previous pregnancy | 0.31 | 0.20 | 2.99 | ||||||||||||
| Yes | 754 (73.60) | 219 (29.00) | 535 (71.00) | 253 (33.60) | 501 (66.40) | 325 (43.10) | 429 (56.90) | 143 (19.00) | 611 (81.00) | ||||||
| No | 269 (26.30) | 78 (29.00) | 535 (71.00) | 96 (35.70) | 173 (64.30) | 111 (41.30) | 158 (58.70) | 65 (24.20) | 204 (75.80) | ||||||
| Male | |||||||||||||||
| Age (years) a | 1.97 | 0.12 | 0.28 | 0.01 | |||||||||||
| 206 (20.12) | 67 (32.50) | 139 (67.50) | 71 (34.50) | 135 (65.50) | 89 (43.20) | 117 (56.80) | 38 (18.40) | 168 (81.60) | |||||||
| 30–34 | 540 (52.73) | 157 (29.10) | 383 (70.90) | 187 (34.60) | 353 (65.40) | 234 (43.30) | 306 (56.70) | 119 (22.00) | 421 (78.00) | ||||||
| 278 (27.15) | 74 (26.60) | 204 (73.40) | 92 (33.10) | 186 (66.90) | 114 (41.00) | 164 (59.00) | 52 (18.70) | 226 (81.30) | |||||||
| Marital status | 0.17 | 0.02 | |||||||||||||
| First marriage | 942 (92.00) | 272 (28.90) | 670 (71.10) | 323 (34.30) | 619 (65.70) | 402 (42.70) | 540 (57.30) | 192 (20.40) | 750 (79.60) | ||||||
| Digamy | 82 (8.00) | 26 (31.70) | 56 (68.30) | 27 (32.90) | 55 (67.10) | 35 (42.70) | 47 (57.30) | 17 (20.70) | 65 (79.30) | ||||||
| Educational degree (male) a | 3.62 | 0.13 | 3.84 | 2.40 | |||||||||||
| Junior college and below | 385 (37.60) | 123 (31.90) | 262 (68.10) | 138 (35.80) | 247 (64.20) | 186 (48.30) | 199 (51.70) | 89 (23.10) | 296 (76.90) | ||||||
| Bachelor | 480 (46.90) | 137 (28.50) | 343 (71.50) | 155 (32.30) | 325 (67.70) | 183 (38.10) | 297 (61.90) | 91 (19.00) | 389 (81.00) | ||||||
| Master and above | 159 (15.50) | 38 (23.90) | 121 (76.10) | 57 (35.80) | 102 (64.20) | 68 (42.80) | 91 (57.20) | 29 (18.20) | 130 (81.80) | ||||||
Note: aThe Cochran-Armitage trend method was used to test the linear
relationship between ordered categorical variables (female age, female
educational degree, infertility duration, male age, male educational degree) and
binary categorical outcomes. bPearson test: r = –0.077, p
= 0.014, suggesting a weak negative correlation between female age and anxiety.
cPearson test: r = –0.072, p = 0.022, suggesting a weak
positive correlation between duration of infertility and somatic symptoms.
dPearson test: r = –0.080, p = 0.011, suggesting a weak
positive correlation between duration of infertility and sleep quality. The
remaining associations were all non-significant (p
Logistic regression analysis identified the key factors influencing anxiety,
depression, somatic symptoms, and sleep quality (Table 4). Age was found to be
significantly associated with anxiety, with participants aged
| Variables | Crude | Model 1 | |||||
| Beta | OR (95% CI) | p value | Beta | OR (95% CI) | p value | ||
| Anxiety | |||||||
| Age (years) | |||||||
| 0.588 | 1.801 (1.138–2.850) | 0.012 | - | - | - | ||
| 30–34 | 0.403 | 1.497 (0.973–2.302) | 0.066 | - | - | - | |
| Ref. | Ref. | Ref. | - | - | - | ||
| Somatic symptom | |||||||
| Occupational status (not working) | 0.701 | 2.015 (1.222–3.324) | 0.006 | 0.781 | 2.183 (1.323–3.603) | 0.002 | |
| Duration of infertility (years) | |||||||
| Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | ||
| 3–5 | 0.336 | 1.399 (1.045–1.873) | 0.024 | 0.368 | 1.445 (1.078–1.937) | 0.014 | |
| 0.260 | 1.297 (0.881–1.910) | 0.188 | 0.311 | 1.365 (0.926–2.013) | 0.116 | ||
| Educational degree (male) | |||||||
| Junior college and below | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | |
| Bachelor | –0.246 | 0.782 (0.586–1.044) | 0.782 | –0.034 | 0.967 (0.726–1.287) | 0.817 | |
| Master and above | –0.020 | 0.980 (0.660–1.457) | 0.922 | 0.184 | 1.202 (0.796–1.815) | 0.382 | |
| Sleep quality | |||||||
| Occupational status (not working) | 0.700 | 2.014 (1.200–3.379) | 0.008 | 0.703 | 2.020 (1.202–3.396) | 0.008 | |
| Duration of infertility (years) | |||||||
| Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | ||
| 3–5 | 0.101 | 1.106 (0.770–1.587) | 0.586 | 0.102 | 1.108 (0.771–1.591) | 0.580 | |
| 0.580 | 1.787 (1.169–2.731) | 0.007 | 0.576 | 1.780 (1.161–2.728) | 0.008 | ||
| Previous pregnancy (yes) | 0.265 | 1.303 (0.929–1.829) | 0.125 | 0.260 | 1.297 (0.920–1.830) | 0.138 | |
Model 1: adjusted for age; OR, odds ratio; CI, confidence interval; Ref, reference.
We next examined the relationship between successful conception and psychological symptoms. Following adjustment for age, employment status, duration of infertility and other characteristics, no significant associations were observed between successful conception and the factors of anxiety, depressive symptoms, somatic symptoms, or poor sleep quality (Table 5).
| Variables | Successful conception, n (%) | Crude | Model 1 | Model 2 | ||||
| OR (95% CI) | p value | OR (95% CI) | p value | OR (95% CI) | p value | |||
| Anxiety symptoms | ||||||||
| Yes | 74 (10.8) | 0.936 (0.639–1.370) | 0.733 | 0.933 (0.636–1.367) | 0.721 | 0.706 (0.430–1.159) | 0.169 | |
| No | 23 (7.9) | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | |
| Depressive symptoms | ||||||||
| Yes | 65 (10.2) | 0.927 (0.593–1.446) | 0.737 | 0.925 (0.592–1.444) | 0.732 | 0.955 (0.607–1.504) | 0.843 | |
| No | 32 (9.5) | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | |
| Somatic symptom | ||||||||
| Yes | 55 (9.9) | 1.022 (0.669–1.560) | 0.921 | 1.019 (0.666–1.557) | 0.932 | 1.029 (0.668–1.584) | 0.897 | |
| No | 42 (10.0) | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | |
| Sleep disorder | ||||||||
| Yes | 76 (9.8) | 1.066 (0.640–1.775) | 0.807 | 1.067 (0.640–1.776) | 0.805 | 1.087 (0.645–1.831) | 0.753 | |
| No | 21 (10.4) | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | |
Crude: unadjusted; Model 1: adjusted for age; Model 2: adjusted for ethnicity, marital status, BMI, occupational status, educational level, infertility duration, previous pregnancy, follicle-stimulation hormone (basic), progesterone (basic), testosterone (basic), prolactin (basic), estrogen (basic) and anti-mullerian hormone.
This study provides insights into the psychological stress experienced by women undergoing AIH, as well as the impact of this stress on the rate of pregnancy success. The findings highlight the significant role of demographic factors such as age, occupational status, and duration of infertility in predicting psychological issues like anxiety, somatic symptoms, and sleep disorders. These factors can influence the overall wellbeing of patients, and hence may indirectly affect the success of fertility treatments.
The prevalence of mental health disorders, including anxiety, depression,
somatic symptoms and sleep disorder, was found to be high among women undergoing
AIH. This finding concurs with the results of a systematic review of 32 studies
conducted by Bagade and coworkers [21]. These authors found the prevalence of
mental health disorders, including anxiety, depression, psychological distress,
and stress, was higher among women with infertility compared to fertile women.
Furthermore, we found that social determinants influenced the severity of
anxiety, depression, somatic symptoms and sleep disorder. Women undergoing AIH
experienced worse mental health and sleep quality if they were young (
Age is a critical factor in the success of ART, including AIH. Age-specific
disparities are quite pronounced, with women aged
Our study found no significant associations between psychological factors
(anxiety, depression, somatic symptoms, sleep disorders) and conception success,
even after adjustment for covariates such as age, occupational status, and sex
hormones. However, some studies have demonstrated an association between
psychological stress and pregnancy rate. A systematic review conducted by
Matthiesen et al. [32] found that stress, trait anxiety, and state
anxiety were negatively associated with clinical pregnancy rates. This
inconsistency may be due to dynamic changes in the psychological stress of
infertile women across treatment cycles, as well as differences between study
populations (AIH vs. in vitro fertilization-embryo transfer). Psychological
stress can impact reproductive outcomes through various mechanisms, including
neuroendocrine changes and immune system dysfunction. For example, chronic stress
can suppress LH pulsatility and reduce tubal motility, both of which can hinder
the reproductive process. While cumulative clinical pregnancy rates reach 37.4%
over three IUI-OS cycles, the live birth success rate declines by 25% per
additional cycle (OR adjusted = 0.75, 95% CI: 0.62–0.93), potentially
exacerbating the psychological distress of couples as they undergo repeated
unsuccessful attempts. Symptom Checklist-90 assessments revealed that recurrent
AIH failures exhibited higher anxiety, hostility, phobic anxiety, and total
scores compared to first-time patients (p
Our study had several limitations. First, data analysis was not controlled for biological factors such as sperm DNA fragmentation and the psychological assessment of men, which could confound the results. Secondly, psychological assessments only measure baseline stress levels, and assessments were not conducted throughout the treatment cycle. The 2024–2028 National Institutes of Health Strategic Plan advocates interdisciplinary approaches, including artificial intelligence, to disentangle cyclical stress fluctuations and confounders [37]. Such methodologies could address limitations due to static psychological assessments, as highlighted by NIH studies linking AIH failure to unmeasured biological variables. Future research should focus on longitudinal studies that track psychological stress levels throughout the treatment cycle, as well as controlling for biological factors, socioeconomic status and lifestyle to provide a more comprehensive understanding of the relationship between psychological stress and fertility outcomes.
This study examined associations between demographic characteristics and mental health disorders. Notwithstanding the methodological limitations, the findings of our study underscore the need for targeted psychological interventions among specific populations, including younger individuals, unemployed persons, and patients experiencing prolonged infertility. Although no statistically significant direct relationship was observed between mental health disorders and conception success, the amelioration of psychological wellbeing may enhance quality of life and overall health outcomes. Future research should further deconstruct the complex interplay between mental health and reproductive health to develop evidence-based interventions for vulnerable groups.
Our results support integration of the biopsychosocial model into treatment protocols for AIH, wherein psychological wellbeing constitutes an essential component of holistic patient care. By addressing psychological comorbidities—particularly anxiety, somatic symptom disorders, and sleep disturbances—this could not only optimize patient quality of life, but potentially improve the success rates of ART. Evidence-based multidisciplinary frameworks should engage both partners throughout therapeutic consultations and procedures, thereby enhancing coping mechanisms and treatment adherence while mitigating perceptions of isolation or unilateral responsibility [38]. Future investigations should aim to further delineate psycho-reproductive interactions, thereby developing more effective interventions to support dyadic wellbeing during fertility treatment.
The datasets used and analyzed during the current study available from the corresponding author on reasonable request.
MJR: design of the work, write the main manuscript; YYW: acquisition, analysis of data for the work, write the main manuscript; YP: study conception, design, data analysis. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study was approved by Ethics Committee of West China Second University Hospital, Sichuan University (No.2024248). We abided research process by the ethical principle of informed consent, voluntary, harmless. All study procedures were strictly followed the Declaration of Helsinki.
Not applicable.
This project was supported by Sichuan Nursing Association (H23008).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.