

 , Hiroaki Fukuda 1, Junya Tanaka 1, Arisa Minamino 1, Shiko Hayashi 1
, Hiroaki Fukuda 1, Junya Tanaka 1, Arisa Minamino 1, Shiko Hayashi 11 Department of Obstetrics and Gynecology, Kinan Hospital, 646-8588 Wakayama, Japan
2 Department of Obstetrics and Gynecology, Wakayama Medical University, 641-0012 Wakayama, Japan
Abstract
The number of nulliparous pregnant women of advanced maternal age, defined as 35 years or older, has increased in Japan, but there has not been a study comparing labour progression between pregnant women of advanced maternal age and young pregnant women. Therefore, we aimed to evaluate roughly whether labour progression times differed according to maternal age, with cervical dilation and foetal station used as the endpoints.
We retrospectively reviewed the medical records of 1573 nulliparous women who had spontaneous vaginal delivery (929 patients), were administered an intravenous uterotonic agent (372 patients) or underwent emergency caesarean section (272 patients) at Kinan Hospital. We collected data on the patient characteristics and reviewed vaginal examination data for comparisons of labour progression. The endpoints were cervical dilation of 10 cm (full dilation) and foetal station of 2 cm, as these metrics are sufficient for vacuum-assisted vaginal delivery (sufficient descent). Data on the elapsed time between the recorded time of each stage of labour and the endpoint were obtained from two groups, namely, pregnant women of advanced maternal age and young pregnant women, and compared.
The percentages of women of advanced maternal age were higher among those who underwent emergency caesarean section and intravenous uterotonic agent administration. When the characteristics of the pregnant women of advanced maternal age were compared to those of the young pregnant women among the 929 patients with spontaneous vaginal delivery, differences in “blood loss amount” and “vacuum delivery status” were detected. However, regarding labour progression, there was almost no difference in any of the stages when the elapsed times between each stage and full dilation or sufficient descent were compared.
We did not detect a clear impact of maternal age on labour progression in the groups of nulliparous women who had spontaneous vaginal delivery after women who underwent emergency caesarean section or intravenous uterotonic agent administration were excluded; however, further studies with larger sample sizes of women of advanced maternal age may be needed.
Keywords
- nulliparous women of advanced maternal age
- labour progression
- spontaneous vaginal delivery
- cervical dilation
- foetal head station
Owing to lifestyle changes and the increased use of infertility treatment, delayed childbearing has recently become a global phenomenon [1, 2, 3]. In Japan, the number of pregnancies and deliveries at an advanced maternal age, defined as 35 years or older at the time of delivery [4, 5], has increased [6]. Because advanced maternal age is a risk factor for adverse outcomes related to labour and pregnancy-related complications in nulliparous women [1, 5, 6, 7, 8, 9], the need for careful observation has increased, that is, we must prepare for the high possibility of emergency caesarean section among nulliparous women of advanced maternal age. Additionally, one can hypothesize that advanced maternal age would have an adverse effect on labour progression in women with spontaneous onset of labour. Therefore, since a relative increase in human resources may be needed, even when no medical intervention is needed, the comparison of labour progression between pregnant women of advanced maternal age and young pregnant women may provide valuable information.
Since the first report of the labour curve by Friedman [10], several researchers have attempted to visualize labour progression [11, 12, 13, 14, 15]. Some studies have reported the impact of maternal age on the duration of labour in the first stage [16] or the total labour duration [17]. However, there is no report of a detailed analysis of labour progression, such as an analysis of the use of Friedman’s labour curves for these women, in nulliparous women of advanced maternal age. Such an analysis might provide insights that can help reduce the decision-making time regarding whether to perform emergency caesarean section. Therefore, in this study, we aimed to perform a detailed comparison of each stage of labour progression between nulliparous women of advanced maternal age and young nulliparous women by focusing on cervical dilation and foetal station, as described in one previous study [12]. Since the ultimate aim of this study was to reduce the decision-making time for deciding whether to perform an emergency caesarean section, the endpoint for labour progression was set to a cervical dilation of 10 cm, namely, “full dilation”, and a foetal station of 2 cm, namely, “sufficient descent”. Under these conditions, vacuum-assisted vaginal delivery is generally considered applicable [18], and emergency caesarean section can likely be avoided. In this study, the duration between each stage and meeting this goal was considered the main index for detecting the impact of advanced maternal age on labour progression.
This study was approved by the Human Ethical Committee of Kinan Hospital
(approval number: 288). After the exclusion of nulliparous women who were
directly transported from another hospital (14 patients) or who underwent
elective caesarean section (14 patients), the deidentified medical records of
1573 nulliparous women who delivered at term from 37–42 gestational weeks
between April 1, 2017, and March 31, 2024, were retrospectively reviewed. Among
these women, to extract nulliparous women with naturally progressing labor, we
retrospectively excluded women who underwent emergency cesarean section (272
patients) and those who received an intravenous uterotonic agent, such as
oxytocin and prostaglandin F2
To compare labour progression between women of advanced maternal age, defined as those aged 35 years or older, and young women, defined as those aged 34 years or younger, we collected vaginal examination data, which are usually collected 3–5 times during labour. First, we defined cervical dilation of 10 cm (full dilation) and a foetal station of 2 cm (sufficient descent) as the goals of labour progression and because at these points, emergency caesarean section can be avoided by performing vacuum-assisted vaginal delivery. The times at which the cervical dilation and foetal station reached 10 cm and 2 cm, respectively, were recorded. Data on the number of vaginal examinations performed before the patients reached these goals were also extracted from the medical records to calculate the elapsed time. In total, 2599 data points on cervical dilation and 3088 data points on foetal station were extracted.
We extracted data on pregnant women’s characteristics, including basic personal characteristics, maternal complications, and delivery outcomes, although the indices were limited due to the retrospective approach. These indices included the following: (1) “gestational week”; (2) “maternal age”; (3) “maternal height”; (4) “maternal body mass index (BMI)”; (5) “infertility treatment status”, defined as pregnancy after infertility treatment; (6) “uterine leiomyoma”, defined as uterine leiomyoma; (7) “threatened preterm delivery”, defined as a medical history of threatened preterm delivery; (8) “PROM”, defined as cases of premature rupture of membranes (PROM) noted at the time of hospitalization; (9) “GBS-positive”, defined as Group B Streptococcus (GBS) positivity detected from vaginal discharge; (10) “GDM”, defined as gestational diabetes mellitus (GDM); (11) “blood loss amount”; (12) new-born birth weight; (13) “Apgar score (1 minute)”, defined as the Apgar score recorded at 1 minute after delivery; (14) “Apgar score (5 minutes)”, defined as the Apgar score recorded at 5 minutes after delivery; and (15) “vacuum delivery”, defined as vacuum-assisted vaginal delivery. The 929 nulliparous women were divided into 2 groups; women aged 35 years or older were included in the advanced age group, and women aged 34 years or younger were included in the young age group, and the patient characteristics of the groups were compared.
Next, the elapsed time from each vaginal examination to full dilation of the cervix or sufficient descent of the foetal head was calculated by subtracting the time of each vaginal examination from the time of full dilation or sufficient descent. Then, subgroups were generated to compare the elapsed time between the 2 groups as follows: (1) cervical dilation subgroups, 1 cm, 2 cm, 3 cm, 4 cm, 5 cm, 6 cm, 7 cm, 8 cm, and 9 cm and (2) foetal station subgroups, –3 cm, –2 cm, –1 cm, 0 cm and 1 cm.
Statistical analyses were performed with Microsoft Excel 365 (Microsoft Corporation,
Redmond, WA, USA) and JMP version 18 for Windows (SAS Institute, Inc., Tokyo, Japan).
Comparisons of the aforementioned patient characteristics and
elapsed times were analysed by means of Student’s t-test, Pearson’s
Chi-square test and Wilcoxon rank-sum test. Odds ratios (ORs) and 95% confidence intervals (95% CIs) were
estimated to determine the strengths of the correlations. p
To visualize labour progression, the relationships between cervical dilation and foetal station (X-axis) and the calculated elapsed time (Y-axis) in each subgroup were plotted. Then, by considering the labour goal, that is, cervical dilation of 10 cm or a foetal station of 2 cm, as the origin (0, 0), regression lines were established for visual comparison.
To analyse the data of nulliparous women who underwent spontaneous vaginal delivery with almost no medical intervention, we classified patients into the following 3 groups: (1) intravenous uterotonic agent administration; (2) emergency caesarean section; and (3) spontaneous vaginal delivery. As expected, when maternal age in the 3 groups were compared, we noted significant differences for all patterns, namely, 1 vs. 2, 1 vs. 3, and 2 vs. 3 (Table 1).
| Age (Avg. | |
| Intravenous uterotonic agent administration | 29.9 |
| Emergency caesarean section | 31.6 |
| Spontaneous vaginal delivery | 28.3 |
| All deliveries | 29.3 |
Comparisons of maternal age were performed among the 3 groups classified according labour-related interventions. For each subgroup, we calculated averages, standard deviations and minimum and maximum values and obtained count data from medical records. In this table, for all patterns of comparison indicated by *, **, and ***, significant differences were detected via Student’s t-test. *: comparison between the groups of “Intravenous uterotonic agent administration” and “Emergency caesarean section”. **: comparison between the groups of “Intravenous uterotonic agent administration” and “Spontaneous vaginal delivery”. ***: comparison between the groups of “Emergency caesarean section” and “Spontaneous vaginal delivery”. Abbreviations: Avg., average; Min, minimum; Max, maximum; No., number; SD, standard deviation.
The characteristics of the patients, including 108 women aged 35 years (advanced age group) or older and 821 women aged 34 years or younger (young age group), are summarized in Table 2. In this analysis, there were few women with hypertensive disorders during pregnancy, probably because women who received intravenous uterotonic agents were excluded. When the data of the advanced and young maternal age groups were compared, we detected significant differences in various factors, including maternal age, infertility treatment status, blood loss volume and vacuum delivery status. These results may indicate the adverse impacts of advanced maternal age on the outcomes of labour, as in previous reports [5, 6, 7, 8, 9]. Although there was unavoidably a significant difference in the number of patients with a history of infertility treatment, there were no significant differences in the other patient characteristics, so it was possible to treat both groups equally.
| Total (Avg. |
Advanced age (Avg. |
Young age (Avg. |
p value | |
| Gestational week (weeks) | 39.2 |
39.0 |
39.2 |
0.07 |
| Maternal age (years) | 28.3 |
37.1 |
27.2 |
|
| Maternal height (cm) | 158.1 |
158.9 |
158.0 |
0.10 |
| Maternal BMI (kg/m2) | 24.8 |
25.1 |
24.8 |
0.35 |
| Infertility treatment | n = 54/929 | n = 22/108 | n = 32/821 | |
| Uterine leiomyoma | n = 12/929 | n = 4/108 | n = 8/821 | 0.06 |
| Threatened preterm delivery | n = 245/929 | n = 33/108 | n = 212/821 | 0.35 |
| PROM | n = 287/929 | n = 39/108 | n = 248/821 | 0.26 |
| GBS positivity | n = 120/929 | n = 11/108 | n = 109/821 | 0.45 |
| GDM | n = 17/929 | n = 2/108 | n = 15/821 | 1.00 |
| Blood loss amount | 266, 46–3661, n = 929 * | 292, 78–2556, n = 108 * | 262, 46–3661, n = 821 * | |
| New-born birth weight | 3017.3 |
3014.5 |
3017.7 |
0.92 |
| Apgar score (1 minute) | 8.6 |
8.6 |
8.7 |
0.33 |
| Apgar score (5 minutes) | 9.6 |
9.6 |
9.6 |
0.63 |
| Vacuum delivery | n = 128/929 | n = 26/108 | n = 102/821 |
The representative patient characteristics obtained from medical records are
summarized in this table. For each item, we calculated averages and standard
deviations and minimum and maximum values and obtained count data from medical
records. Abbreviations: BMI, body mass index; GBS, Group B Streptococcus; GDM,
gestational diabetes mellitus; PROM, premature rupture of membranes. The p values were
compared via Student’s t test or the Yates Chi-square test. p
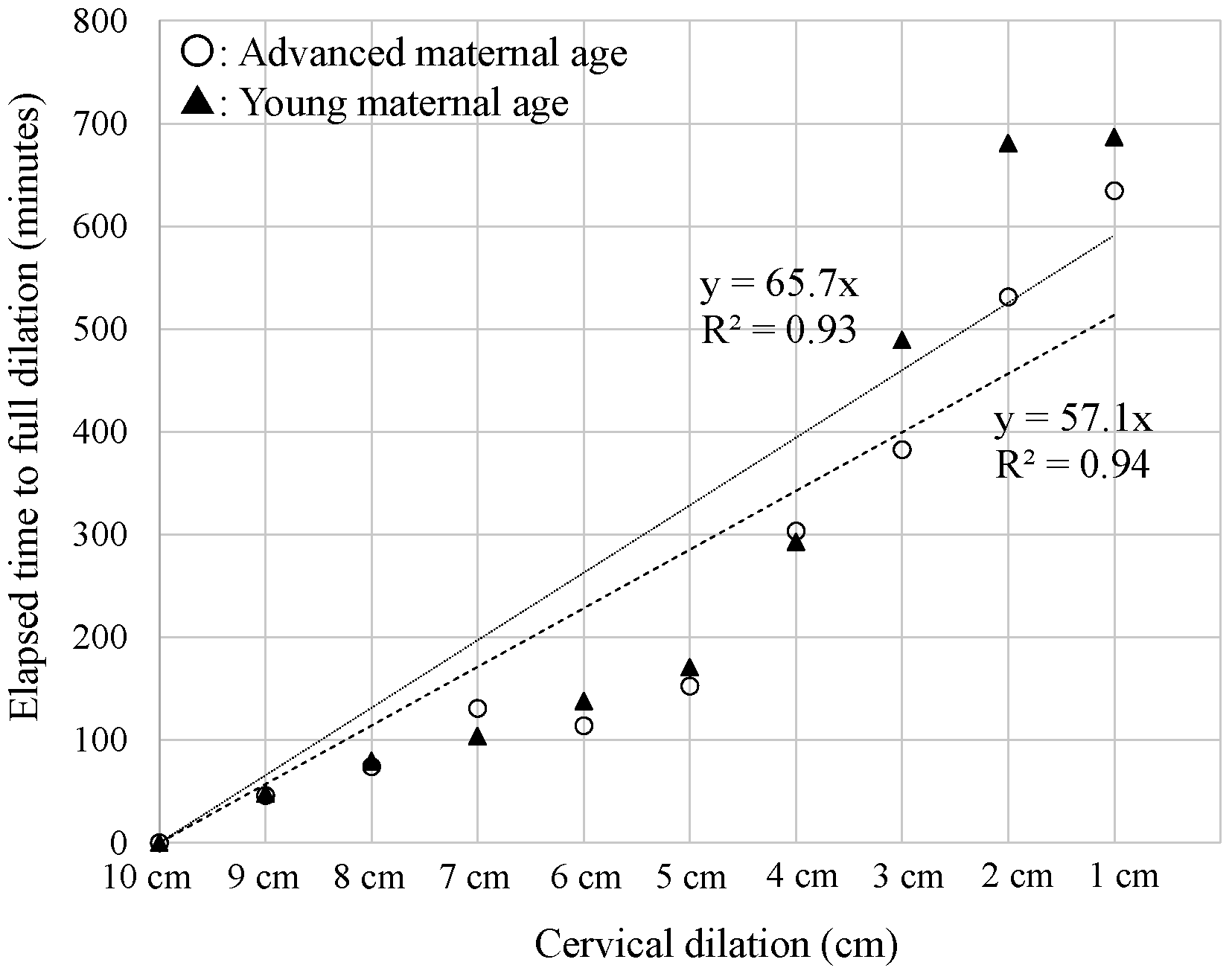
As shown in Table 3 and Fig. 1, when the elapsed time among the respective subgroups classified by cervical dilation was compared, though a significant difference was detected in the subgroup with a cervical dilation of 6 cm, no significant differences were observed in the other subgroups (Table 3), and we visually observed the same trend (Fig. 1).
| Cervical dilation | Total (Median, Min–Max, No.) | Advanced age (Median, Min–Max, No.) | Young age (Median, Min–Max, No.) | p value |
| 1 | 610, 125–2460, n = 155 | 565, 145–1680, n = 22 | 615, 125–2460, n = 133 | 0.54 |
| 2 | 565, 63–2145, n = 141 | 305, 70–1430, n = 15 | 580, 63–2145, n = 126 | 0.12 |
| 3 | 335, 30–2565, n = 312 | 270, 50–1460, n = 39 | 345, 30–2565, n = 273 | 0.09 |
| 4 | 185, 18–1300, n = 287 | 160, 18–915, n = 31 | 185, 20–1300, n = 256 | 0.68 |
| 5 | 130, 20–1480, n = 231 | 90, 20–860, n = 23 | 130, 25–1480, n = 208 | 0.18 |
| 6 | 108.5, 5–1555, n = 262 | 67, 15–825, n = 22 | 113.5, 5–1555, n = 240 | |
| 7 | 85.5, 5–1400, n = 293 | 48.5, 5–1400, n = 30 | 85, 5–757, n = 263 | 0.08 |
| 8 | 60, 3–1170, n = 356 | 65, 5–205, n = 37 | 60, 3–1170, n = 319 | 0.72 |
| 9 | 35, 1–290, n = 562 | 25, 2–185, n = 60 | 35, 1–290, n = 502 | 0.45 |
The elapsed times (minutes) among the respective subgroups classified by cervical dilation were compared. For each subgroup, we calculated median, minimum and maximum values and obtained count data from medical records. The p values were compared via the Wilcoxon rank-sum test.
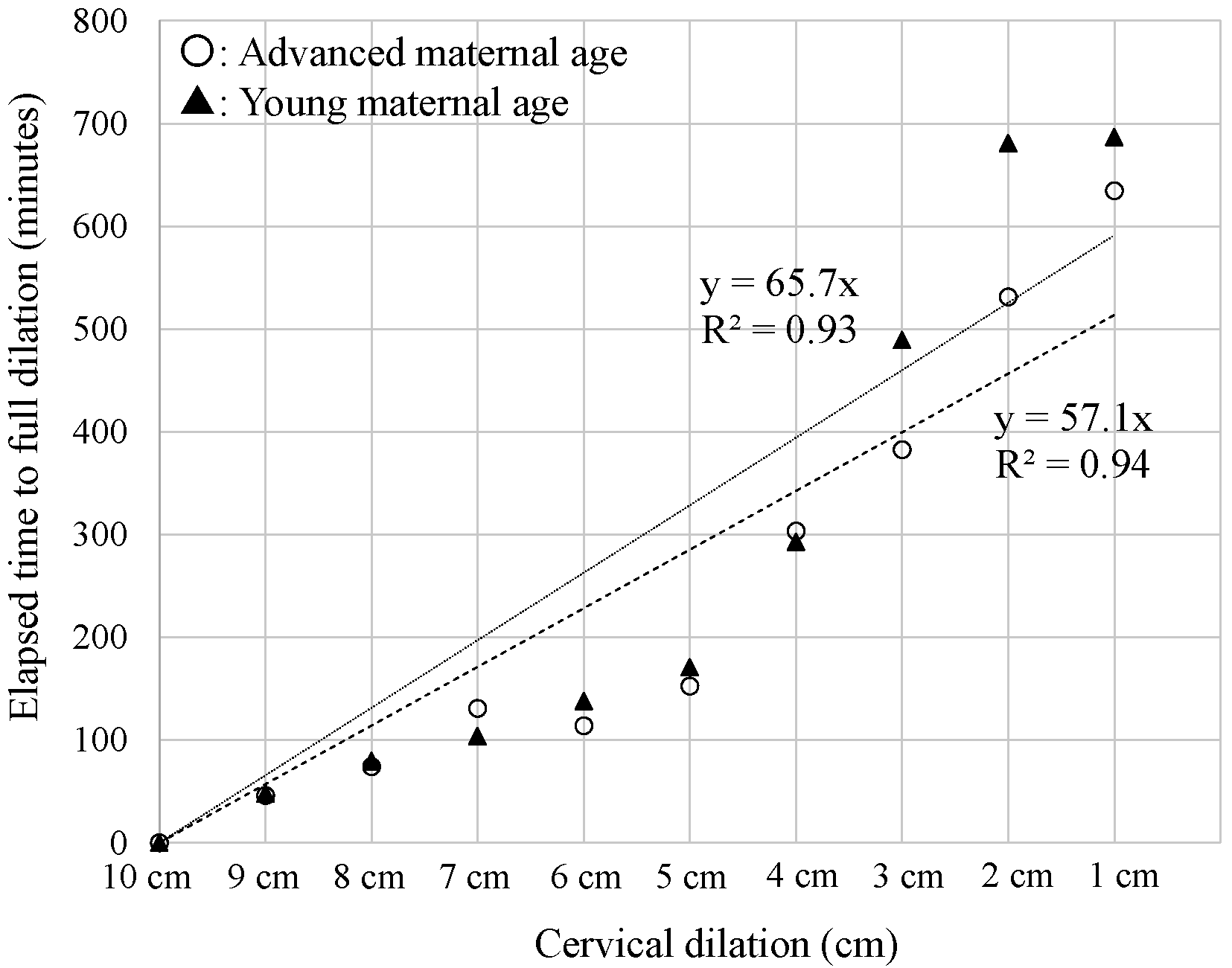 Fig. 1.
Fig. 1.
Comparison of labour progression (cervical dilation).The labour progression of nulliparous women of advanced (white circles) and young (black triangles) maternal age are shown with regression lines and R2 values. X-axis: each step of cervical dilation. Y-axis: elapsed time (minutes) to cervical dilation of 10 cm. Dashed line: young maternal age; Dotted line: advanced maternal age.
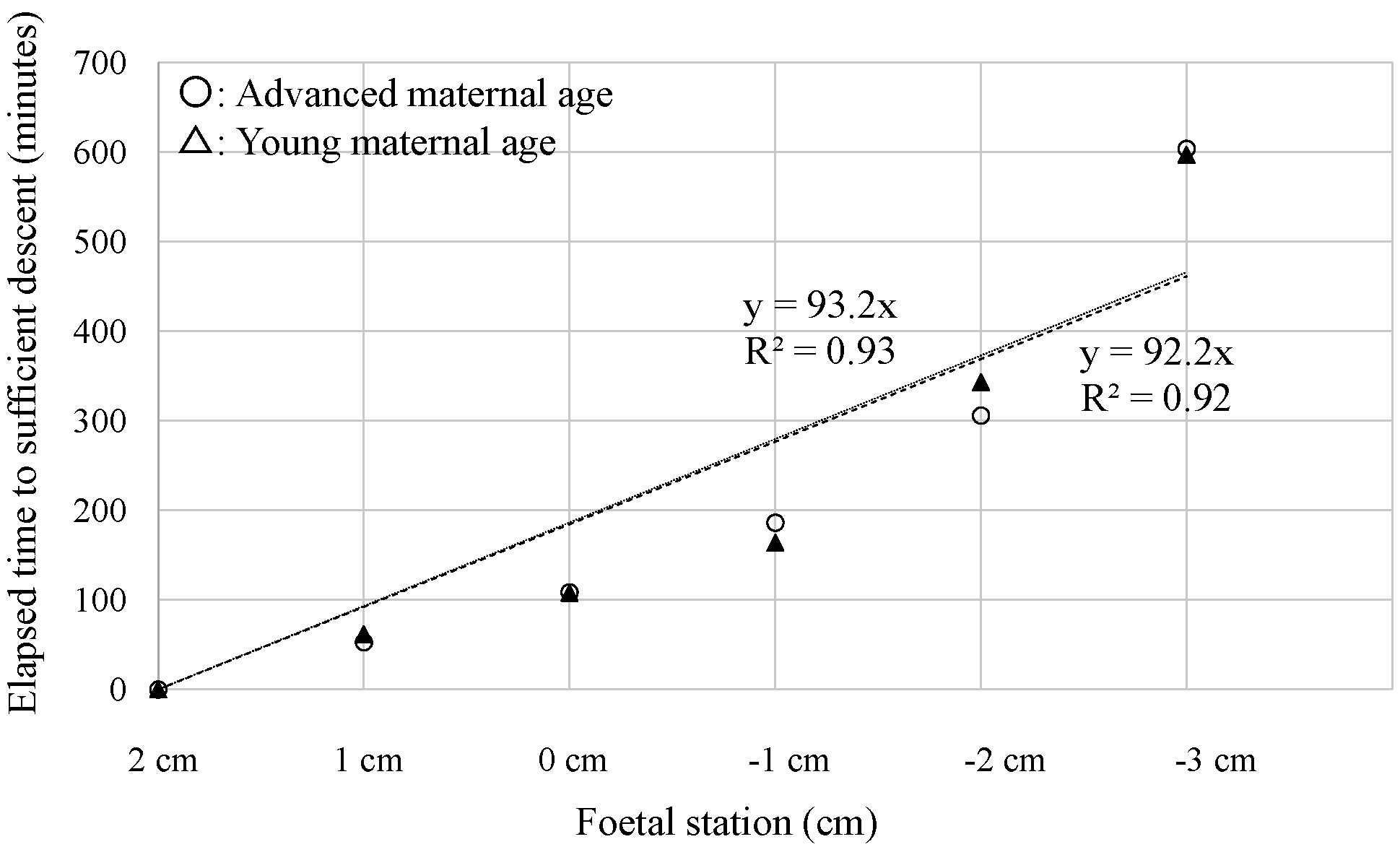
Similar to the analysis of cervical dilation, as shown in Table 4 and Fig. 2, we detected no difference in the respective subgroups classified by foetal station. Therefore, we confirmed that among nulliparous women who underwent spontaneous vaginal delivery, there was not adverse effect of advanced maternal age on labour progression. Additionally, considering the aforementioned results concerning cervical dilation, the data revealed that the goal was reached within approximately 10 hours if the labour progression was smooth.
| Foetal head station | Total (Avg. |
Advanced age (Avg. |
Young age (Avg. |
p value |
| −3 | 465, 10–2585, n = 244 | 498.5, 70–1680, n = 30 | 449, 10–2585, n = 214 | 0.62 |
| −2 | 205, 10–2215, n = 886 | 182.5, 22–1460, n = 104 | 209.5, 10–2215, n = 782 | 0.24 |
| −1 | 110, 4–1735, n = 794 | 100, 5–1600, n = 73 | 110, 4–1735, n = 721 | 0.72 |
| 0 | 65.5, 0–1425, n = 616 | 65.5, 5–600, n = 73 | 82, 0–1425, n = 543 | 0.34 |
| 1 | 35, 1–720, n = 548 | 37.5, 5–290, n = 74 | 35, 1–720, n = 474 | 0.80 |
The elapsed time (minutes) among the respective subgroups classified by foetal station was compared. For each subgroup, we calculated median, minimum and maximum values and obtained count data from medical records. The p values were compared via the Wilcoxon rank-sum test.
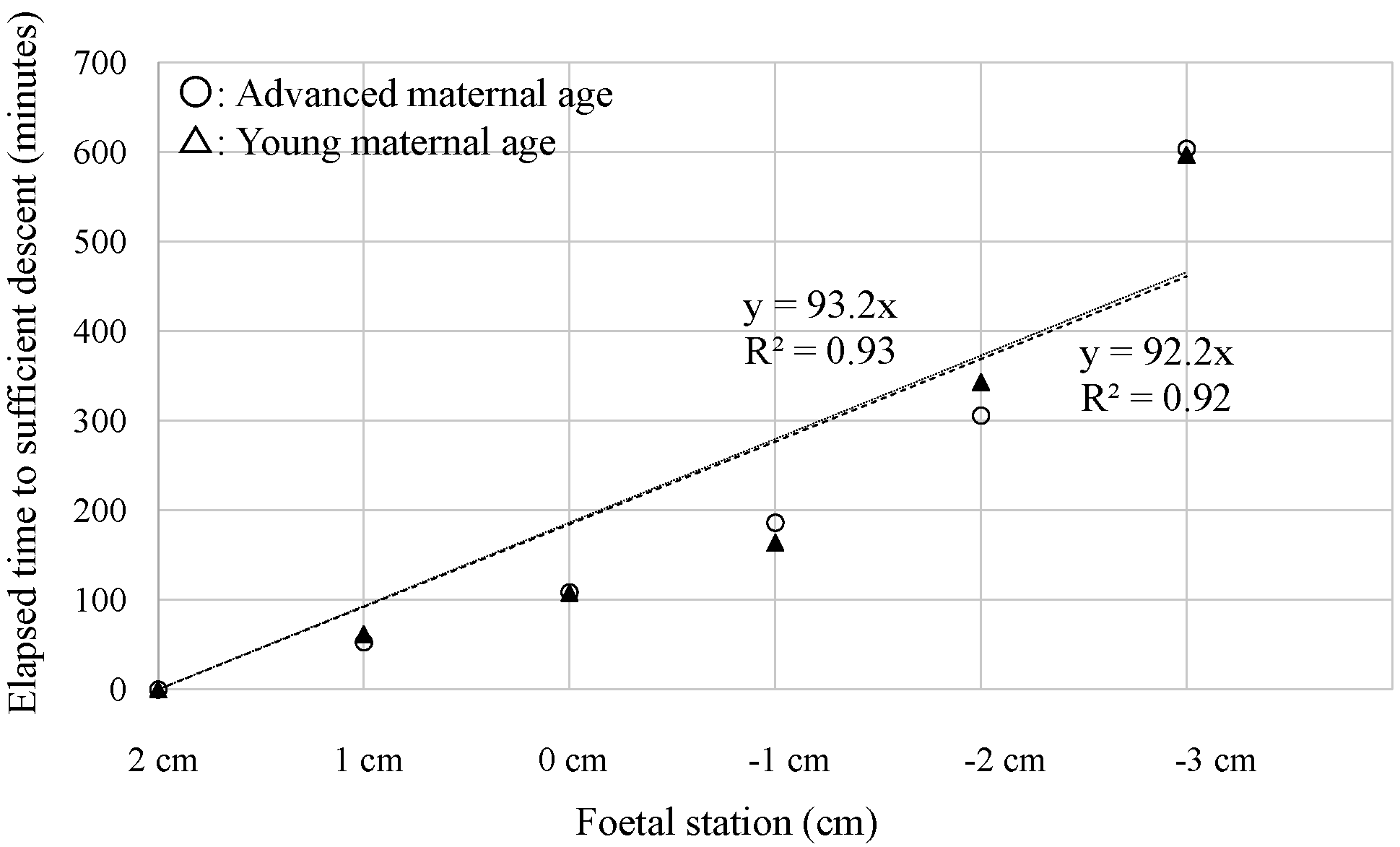 Fig. 2.
Fig. 2.
Comparison of labour progression (foetal station).The labour progression of nulliparous women of advanced (white circles) or young (black triangles) maternal age is indicated by respective regression lines and R2 values. X-axis: each stage of the foetal period. Y-axis: elapsed time (minutes) to a foetal station of 2 cm. Dashed line: young maternal age; Dotted line: advanced maternal age.
In this study, we compared labour progression between nulliparous women of advanced maternal age and young nulliparous women by defining advanced maternal age as 35 years or older, similar to past reports [19]. For simple analysis of labour progression itself, more than one-third of the 1573 women were excluded because of the performance of emergency caesarean section (272 women) or the administration of an intravenous uterotonic agent (372 women). Since this was a retrospective study, we were unable to control the sample size. Furthermore, since it was difficult to establish clear exclusion criteria based on the progression of labor or patient characteristics without introducing arbitrary standards, all the data from a total of 929 nulliparous women for seven years were inevitably included. This point was considered an important issue for future research. However, it was ultimately possible to roughly compare the progression of labor. In addition, by setting the goals of labour progression to cervical dilation of 10 cm (full dilation) and a foetal station of 2 cm (sufficient descent) with reference to past reports [18], we were able to include 128 women who underwent vacuum-assisted vaginal delivery. Even following vacuum-assisted vaginal delivery, multiparous women have a high probability of smooth labour progression [20, 21]. Therefore, women with vacuum-assisted vaginal delivery were treated as equivalent to women with spontaneous vaginal delivery. Unlike previous studies [12, 14, 22] in which labour progression was evaluated without classification by maternal age, the impact of maternal age on labour progression was assessed in this study.
However, unexpectedly, almost no difference was detected in the analysis of either cervical dilation or foetal station. Moreover, in all steps, similar trends were observed both digitally and visually (Tables 3,4 and Figs. 1,2). These detailed analyses led to the conclusion that advanced maternal age did not directly affect labour progression. In addition to advanced maternal age, there may be individual differences in uterine function during labour [23], which could become a novel future research topic, including in the field of basic science. These results also show that labour progression could be evaluated without considering maternal age, only when women who underwent emergency caesarean section or intravenous uterotonic agent administration were excluded. However, in doing so, the sample size may inevitably decrease, and as a result, it ultimately led to the extraction of a nulliparous women group with smooth progression of labour. As shown in Table 1, more than half of the 261 nulliparous women of advanced maternal age were excluded because of the performance of emergency caesarean section (81 women) or the administration of an intravenous uterotonic agent (72 women), although in the group of young nulliparous women, approximately two-thirds of the 1312 women were included in the analyses. Nulliparous women in good condition might be meet these criteria, but compared with the sample size of young nulliparous pregnant women (821 women), that of nulliparous pregnant women of advanced maternal age was small. The number and timing of vaginal examinations varied across women because this was a retrospective study. Since large-scale samples may be needed to perform sufficient analyses and confirm this hypothesis, further studies are needed.
We did not detect a clear impact of maternal age on labour progression in the group of nulliparous women who had spontaneous vaginal delivery after women who underwent emergency caesarean section or intravenous uterotonic agent administration were excluded. However, since the sample size of the group of nulliparous women of advanced maternal age was relatively small, further large-scale studies with sophisticated analytical methods may be needed in the future.
Avg., average; BMI, body mass index; CI, confidence interval; GBS, Group B Streptococcus; GDM, gestational diabetes mellitus; Min, minimum; Max, maximum; No., number; OR, odds ratio; PROM, premature rupture of membranes; SD, standard deviation.
The datasets used and analysed during the current study are available from the corresponding author upon reasonable request. However, due to data processing within the hospital’s closed system, there are limitations in providing raw data.
RA and WI collected and analysed the data and wrote the manuscript. WI supervised the entire study. SH, RA, WI, HF, JT and AM provided medical care for the participants. SH determined the medical interventions and supervised all medical procedures. All the authors read and approved the final manuscript. All authors contributed to editorial changes in the manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study was conducted in accordance with the Declaration of Helsinki, and approved by the Human Ethical Committee of Kinan Hospital (approval number 288). Informed consent was obtained from all patients.
This research was supported by Kinan Hospital, which provided the participants’ medical information.
The authors disclose the receipt of financial support from the Wakayama Prefecture Obstetrician Secure Fund for the preparation and publication of this article.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.