

 , Ilaria Meynet 2, Silvia Denti 3, Claudia Amellone 4, Giuseppe Coppola 5, Silvana De Bonis 6, Martina Nesti 7, Pier Luigi Pellegrino 8, Antonio Rossillo 9, Matteo Ziacchi 10, Giuseppe Boriani 11, Antonio D’Onofrio 12, Silvia G. Priori 13, Sakis Themistoclakis 14, Matteo Anselmino 15,16,†, Roberto De Ponti 17,*,†
, Ilaria Meynet 2, Silvia Denti 3, Claudia Amellone 4, Giuseppe Coppola 5, Silvana De Bonis 6, Martina Nesti 7, Pier Luigi Pellegrino 8, Antonio Rossillo 9, Matteo Ziacchi 10, Giuseppe Boriani 11, Antonio D’Onofrio 12, Silvia G. Priori 13, Sakis Themistoclakis 14, Matteo Anselmino 15,16,†, Roberto De Ponti 17,*,† , on behalf of the Italian Association of Arrhythmology and Cardiac Pacing (AIAC)
, on behalf of the Italian Association of Arrhythmology and Cardiac Pacing (AIAC) 1 Division of Cardiology, Umberto Parini Regional Hospital, 11100 Aosta, Italy
2 Division of Cardiology, Ospedale di Rivoli, 10098 Rivoli, Italy
3 Division of Cardiology, Giovanni Paolo II Hospital, 07026 Olbia, Italy
4 Struttura Complessa Cardiologia, Ospedale Maria Vittoria-Martini, 10153 Torino, Italy
5 Unità Operativa Semplice Terapia Intensiva Cardiologica, Azienda Ospedaliero-Universitaria Policlinico Paolo Giaccone, 90127 Palermo, Italy
6 Unità Operativa Complessa Cardiologia—Unità di Terapia Intensiva Cardiologica, Presidio Ospedaliero Rossano Calabro, 87067 Rossano Calabro, Italy
7 Division of Interventional Electrophysiology, Fondazione Toscana Gabriele Monasterio, 56124 Pisa, Italy
8 Struttura Complessa di Cardiologia Universitaria, Azienda Ospedaliero-Universitaria Policlinico Riuniti, 71122 Foggia, Italy
9 Unità Operativa Complessa di Cardiologia, Ospedale San Bortolo, 36100 Vicenza, Italy
10 Institute of Cardiology, IRCCS Azienda Ospedaliero-Universitaria di Bologna, 40138 Bologna, Italy
11 Cardiology Division, Department of Biomedical, Metabolic and Neural Sciences, University of Modena and Reggio Emilia, Policlinico di Modena, 41124 Modena, Italy
12 Cardiologia-Elettrofisiologia, Clinica Montevergine, 83040 Mercogliano (AV), Italy
13 Cardiologia Molecolare, Istituti Clinici Scientifici Maugeri, IRCCS, 27100 Pavia, Italy
14 Unità Operativa Complessa di Cardiologia, Ospedale Dell’Angelo, 30174 Mestre-Venice, Italy
15 Division of Cardiology, Cardiovascular and Thoracic Department, “Città della Salute e della Scienza” Hospital, 10126 Turin, Italy
16 Department of Medical Sciences, University of Turin, 10126 Turin, Italy
17 Department of Medicine and Surgery, University of Insubria, 21100 Varese, Italy
†These authors contributed equally.
Abstract
Catheter ablation is the mainstay of rhythm control in atrial fibrillation (AF), and its use is steadily increasing worldwide. To optimize procedural safety and efficacy, an appropriate sedation or anesthesia regimen is essential, ensuring adequate analgesia and a stable respiratory pattern while minimizing patient movement. However, the optimal sedation strategy remains a matter of debate, with approaches ranging from general anesthesia to deep or conscious sedation. Since anesthesiologists administer general anesthesia, attention focuses on hypnotics, defined as drugs that induce and/or maintain sleep by depressing the central nervous system, and analgesics. In many centers, these agents are administered by electrophysiology laboratory staff in accordance with local regulations and institutional protocols, which vary among countries. This warrants caution, as individual responses to commonly combined agents are unpredictable and may result in deeper-than-intended sedation. Therefore, respiratory or hemodynamic support may become necessary in selected patients. Notably, protocols incorporating hypnotic communication have also been proposed and implemented. The selection of sedation and analgesia strategies for AF ablation has become increasingly important for balancing patient safety, procedural effectiveness, and resource utilization. The approach should be individualized based on patient characteristics, procedural complexity, energy source, institutional resources, and the relevant national regulatory framework.
Keywords
- atrial fibrillation
- catheter ablation
- procedural sedation
- general anesthesia
- ablation techniques
Catheter ablation of atrial fibrillation (AF) is an established therapy for rhythm control in affected patients [1, 2, 3]. In the general population with symptomatic paroxysmal or persistent AF, catheter ablation reduces arrhythmia burden and improves quality of life, while in selected patients with heart failure with reduced ejection fraction, catheter ablation improves major clinical outcomes, including mortality, by significantly reducing recurrences [2]. The 2024 European Society of Cardiology guidelines [2, 3] recommend catheter ablation as a first-line treatment option, based on shared decision-making, in patients with paroxysmal AF to reduce symptoms, recurrences, and progression of the arrhythmia; consequently, the number of candidates for this procedure is increasing worldwide. Moreover, in a simulated model of the Italian and French healthcare systems, early catheter ablation potentially increases the proportion of patients with controlled AF and reduced adverse events, offsetting the modest increase in total AF-related costs [4].
Pulmonary vein isolation (PVI) remains the cornerstone of AF ablation [1]. Over time, advances in knowledge, operator experience, and technology have reduced both procedure duration and ablation time [5, 6]. Conversely, significant structural heart disease, concomitant arrhythmias such as atrial flutter or atrial tachycardia [7, 8], and/or the need for additional ablation beyond PVI in patients with persistent AF [9] are associated with longer procedures. Therefore, appropriate periprocedural management is essential, particularly because pain, respiratory variability, and body movement may influence clinical outcomes, catheter stability, and the accuracy of three-dimensional mapping. Specifically, as in several centers, three-dimensional mapping is used to support AF ablation and decrease radiation exposure [5]. The adoption of appropriate sedation strategies is crucial, as patient movement compromises the reliability of catheter visualization during electroanatomic mapping and disrupts procedural workflow.
In this context, sedation and anesthesia strategies during AF ablation have never been strictly standardized, and the optimal modality remains debated. A recent international consensus document [1] states that the procedure can be performed under general anesthesia, deep sedation, or conscious sedation, depending on patient and procedural characteristics, operator experience, anesthesia availability, and institutional protocols, and recommends a multidisciplinary approach. Accordingly, worldwide practice is heterogeneous and influenced by patient characteristics, regulatory constraints, availability of dedicated personnel, and monitoring technologies. A global survey promoted by the European Heart Rhythm Association [10] showed that, in 2019, general anesthesia was the most frequently used strategy (40.5%), followed by conscious sedation (32.0%) and deep sedation (27.5%), with marked geographical and volume-related variability. General anesthesia predominated in North and South America, whereas conscious or deep sedation was more common in Europe, although variability among European countries persisted. Between 2010 and 2019, low-volume centers increased the use of deep sedation and decreased the use of conscious sedation, while high-volume centers increased the use of general anesthesia and decreased the use of conscious sedation. Propofol and midazolam were the most commonly used hypnotic agents, and remifentanil and fentanyl were the most frequently used analgesics. In 2021, the Italian Association of Arrhythmology and Cardiac Pacing reported the results of a national survey on anesthesiology practice in interventional electrophysiology and cardiac pacing [11]. During AF ablation, approximately half of the centers used deep sedation or general anesthesia with an anesthesiologist, 40% administered sedation without an anesthesiologist, and 10% used local anesthesia alone.
The most critical phase of AF ablation is energy delivery, as different energy sources are associated with varying degrees of pain perception. When radiofrequency (RF) or cryothermal energy is used, similar sedation protocols are adopted in most centers [10]. However, the recent introduction and increasing use of pulse-field ablation (PFA), which is expected to be less well tolerated due to procedure-related pain [12], have added another variable. This energy source is associated with increased requirements for sedative and analgesic agents [13]. Although in a large international registry, the most common strategy for PFA was general anesthesia or deep sedation with continuous propofol infusion [14], smaller series of younger patients have demonstrated satisfactory results using alternative regimens combining hypnotics and opioids while avoiding propofol because of the risk of respiratory depression, without the need for noninvasive ventilation or orotracheal intubation [15, 16].
Therefore, anesthetic management requires a careful balance among analgesia, prolonged immobility, respiratory depression, and hemodynamic effects. Deeper sedation improves catheter stability and lesion formation and durability, and invasive airway management stabilizes respiratory cycles by preventing alternating apnea and deep breathing. Conversely, invasive airway management prolongs laboratory occupancy time and may increase complications in selected patients. Robust evidence identifying the optimal strategy remains lacking. However, a meta-analysis of randomized and observational studies of RF ablation demonstrated a trend toward lower AF recurrence with general anesthesia or deep sedation, without significant differences in procedural parameters or overall complications; most complications in the general anesthesia/deep sedation group were related to intubation or anesthesia [17]. Nonetheless, due to heterogeneity across studies, definitive conclusions could not be drawn. A more recent meta- analysis including 15 observational studies and 6 randomized trials found no significant differences in post-ablation recurrence between general anesthesia and sedation [18]. Although RF was the predominant energy source, studies using PFA and cryoballoon ablation were also included.
This review aims to describe the pharmacologic characteristics of commonly used agents, summarize the available literature on sedation protocols, and provide an overview of regulatory requirements for sedation and general anesthesia, which are crucial in this multidisciplinary setting.
In 1999, the American Society of Anesthesiologists defined levels of sedation and analgesia as distinct from general anesthesia, emphasizing that sedation exists on a continuum and that individual patient responses cannot always be predicted. Consequently, the depth of sedation may fluctuate at any point during a procedure, requiring prompt recognition and appropriate corrective measures. The most recent update of this document was published in October 2024 [19]. Excluding minimal sedation, which essentially provides anxiolysis and is generally inadequate for AF ablation procedures, interventions are usually performed under conscious sedation, deep sedation, or general anesthesia. Both conscious and deep sedation are typically achieved through titrated intravenous administration of sedative and/or analgesic agents throughout the procedure. However, during deep sedation, individual variability and the use of drug combinations may impair the ability of the patient to maintain spontaneous ventilation. Thus, ventilatory function may become inadequate, and airway support may be required to maintain airway patency. For this reason, practitioners administering any level of sedation must be able to promptly rescue patients who inadvertently progress to a deeper level of sedation or general anesthesia, using effective airway management and advanced life support measures [19].
During AF ablation, general anesthesia requires airway control with an
endotracheal tube or a laryngeal mask [20], which, in certain organizational
settings, may prolong the overall procedural duration. A recent retrospective
single-center study reported a 42.2% incidence of respiratory complications in
patients undergoing AF ablation with RF or cryoablation under sedation/analgesia
[21]. When subdivided into mild, intermediate, or severe according to the
Tracking and Reporting Outcomes of Procedural Sedation tool, complications
occurred in 0.4%, 35%, and 15.1% of cases, respectively. Longer procedure
duration, age
The main pharmacological properties of drugs commonly used during AF ablation are summarized in Table 1.
| Agents | Hypnotic properties | Analgesic properties | Effect onset | Effect duration | Main side effects | Antagonist |
| Midazolam (intravenous administration) | +++ | + | Respiratory depression | Yes, flumazenil | ||
| Propofol | +++ | no | 30–40 seconds | 5–10 minutes | Respiratory depression | No |
| Hypotension | ||||||
| Negative inotropic effect | ||||||
| Dexmedetomidine | +++ | + | 2–3 hours | Hypotension | No | |
| Bradycardia | ||||||
| Vasoconstriction | ||||||
| Fentanyl/Remifentanil | No | +++ | Fentanyl: 5 minutes | Fentanyl: 30–60 minutes | Respiratory depression | Yes, naloxone |
| Remifentanil: 1–2 minutes | Remifentanil: 3–10 minutes | Increased vagal tone (bradycardia, hypotension) | ||||
| Ketamine | ++ | ++ | 30–60 seconds | 2–3 hours | Dissociation and hallucinations | No |
| Increase sympathetic tone (tachycardia, hypertension) | ||||||
| Paracetamol/Acetaminophen | No | + | 30 minutes | 4–6 hours | No major side effects | No |
Midazolam is a benzodiazepine hypnotic that induces and maintains sleep through central nervous system depression. Benzodiazepine-based conscious sedation reduces anxiety and provides amnesia and mild analgesia during minor procedures. The pharmacologic effects of midazolam are similar to those of other benzodiazepines and include sedation, anxiolysis, sleep induction, and amnesia; however, this medication has a faster onset and shorter duration of action due to the associated high lipophilicity. The onset of action occurs approximately 3 minutes after intravenous administration and 9–26 minutes after oral administration [22]. Midazolam has been associated with respiratory depression, cardiac arrest, and death, particularly when combined with opioids, although the incidence of severe adverse events is low. Flumazenil effectively reverses benzodiazepine-induced sedation; however, respiratory depression may persist and only rarely requires assisted ventilation [22]. Conscious sedation with midazolam, followed by flumazenil and administered by a cardiologist during electrical cardioversion of AF, is safe, effective, and well tolerated, facilitating the procedure and shortening its duration [23]. This approach has been extrapolated to AF ablation, typically in combination with opioids to optimize analgesia and maintain patient immobility [24]. Administration is usually performed using repeated intravenous boluses [25], although continuous infusion has also been described [26].
Propofol is an intravenous anesthetic agent that primarily acts as a positive allosteric modulator of the GABA receptor. Propofol is highly lipophilic, has rapid tissue distribution, and undergoes fast metabolic clearance, which facilitates rapid penetration of the blood–brain barrier and results in an onset of action within 30–40 seconds and rapid recovery [27]. Propofol may be administered as intermittent boluses, continuous infusion, or a combination of both. In prolonged procedures such as AF ablation, continuous infusion helps maintain more stable levels of sedation and reduces fluctuations in arousal [27]. Propofol produces significant hypotension and, particularly in patients with heart failure, exerts negative inotropic effects that may necessitate the supervision of an anesthesiologist in selected high-risk patients [28]. Increased body mass index (BMI), higher propofol dose, persistent AF, longer procedural duration, and obstructive sleep apnea have all been identified as predictors of the need for non-invasive ventilation during propofol sedation [29, 30]. Moreover, because propofol lacks intrinsic analgesic properties, concomitant administration of analgesics is generally required [27].
Propofol is listed among drugs that should possibly be avoided in patients with Brugada syndrome, a population not infrequently undergoing AF ablation, as AF is part of the clinical manifestations of the syndrome. Although the evidence remains conflicting, available data suggest a possible proarrhythmic effect [31].
Dexmedetomidine is a highly selective
Fentanyl is a synthetic piperidine µ-opioid receptor agonist with a rapid onset, achieving maximal analgesia within approximately 5 minutes, and a short duration of action of 30–60 minutes [35]. Fentanyl is metabolized by CYP3A4 and cleared by the kidneys; therefore, dose adjustment is required in patients with hepatic or renal impairment.
Remifentanil is a selective µ-opioid receptor agonist with a rapid onset and an ultra-short duration of action, characterized by an effective biological half-life of 3–10 minutes. Remifentanil is rapidly hydrolyzed by plasma and tissue esterases. Moreover, since remifentanil may inhibit sinus and atrioventricular nodal activity, bradycardia may occur [35]. Particularly in older patients, remifentanil may induce chest wall rigidity (the so-called “wooden chest syndrome”), resulting in ineffective ventilation, hypoxemia, hypercarbia, and desaturation [36]. Pretreatment with hypnotics mitigates this risk [36]. Both fentanyl and remifentanil produce significant respiratory depression and increase vagal tone; the effects of these agents can be antagonized with specific opioid antagonists, such as naloxone. However, abrupt reversal may provoke marked sympathetic activation and increase the risk of ventricular arrhythmias, including sustained ventricular tachycardia or ventricular fibrillation [37].
Sufentanil is a synthetic opioid, structurally related to fentanyl but more potent due to stronger affinity for the µ-opioid receptors and higher lipophilicity, which facilitates rapid central nervous system penetration and onset of action [38].
Morphine is a hydrophilic natural opioid with slower central nervous system penetration due to the blood–brain barrier, and an onset of action within a few minutes. Similar to other opioids, sufentanil and morphine may cause respiratory depression, even in the postoperative phase [38], as well as nausea and vomiting [39]. Both agents are infrequently used during AF ablation [16, 24].
Proactive management of post-procedural pain is integral to the AF ablation procedure, as moderate-to-severe pain within the first 24 hours after ablation is frequently reported [40]. Nonetheless, optimal strategies for post-procedural analgesia remain undefined. N-acetyl-para-aminophenol, known as paracetamol in Europe and acetaminophen in the United States, was first synthesized in 1878 [41]. The antipyretic and analgesic effects of N-acetyl-para-aminophenol were initially attributed to inhibition of prostaglandin synthesis via the cyclooxygenase pathway. However, more recent evidence suggests that active metabolites interact with cannabinoid receptors, elevating endogenous cannabinoid levels and thereby contributing to analgesia [41, 42]. Unlike other non-steroidal anti-inflammatory drugs, paracetamol has limited anti-inflammatory activity, minimal gastrointestinal or cardio-renal toxicity, and no respiratory depressant effects [42], making this medication suitable for post-procedural pain management. In fact, paracetamol has demonstrated significant analgesic efficacy and opioid-sparing effects after both cardiac and non-cardiac surgery, and enhanced recovery protocols recommend scheduled rather than as-needed administration [43]. In adults, typical oral doses range from 650 to 1000 mg every 6–8 hours, with a maximum daily dose of 3 g. Onset of analgesia occurs approximately 30 minutes after oral administration in fasting subjects, with a duration of about 4 hours [42]. Nevertheless, because paracetamol is hepatically metabolized, caution is warranted in patients with liver insufficiency [43].
Ketamine is an N-methyl-D-aspartic acid (NMDA) receptor antagonist with combined sedative and analgesic properties [44]. Analgesia is achieved by inhibiting NMDA receptors, resulting in central nervous system depression and dissociation. Following intravenous administration, peak plasma concentrations are reached within 2–4 minutes, and high lipid solubility enables rapid penetration of the blood–brain barrier. Ketamine has a half-life of 2–3 hours, and the clearance of this drug is largely independent of renal function. Ketamine uniquely provides both sedation and analgesia while preserving hemodynamic and respiratory reflexes.
Ketamine also has sympathomimetic effects, mediated by the release of endogenous catecholamines, inhibition of vagal activity, and inhibition of norepinephrine reuptake, resulting in increased heart rate and blood pressure, as well as potential arrhythmogenicity. A well-known adverse effect is the emergence reaction, which occurs in up to 30% of patients and is characterized by psychomotor disturbances during recovery; this may lead to detrimental patient movement during procedures [44].
Experience with ketamine in AF ablation is limited [16, 45]. Intravenous ketamine, administered after premedication with midazolam and fentanyl approximately 5 minutes before PFA, with titration to a total dose of 3 mg/kg, has been reported without major procedural or anesthesia-related complications [45].
Hypnosis is increasingly recognized as an effective approach for managing acute and chronic pain. Hypnosis involves a modified state of consciousness characterized by reduced self-awareness and increased responsiveness to suggestions [46]. Multiple studies have demonstrated the effectiveness of hypnosis in chronic pain management [47, 48] and in reducing procedural pain [49, 50]. Indeed, when used as an adjunct to conventional analgesia, hypnosis can enhance analgesic effectiveness and decrease sedative and opioid requirements. In 2019, Scaglione et al. [51] conducted an observational study comparing hypnotic communication with conventional analgesia in two cohorts of 70 patients undergoing RF ablation of AF. Hypnosis induction was successfully achieved in 97% of cases. Compared with conventional analgesia, the hypnosis group experienced significant reductions in procedural anxiety and perceived procedural duration. Procedural pain was reported as absent in 78% of patients, and no patient required invasive or non-invasive ventilatory support or additional major sedatives (midazolam or propofol). Fentanyl doses were similar in both groups, whereas higher doses of paracetamol were required in the hypnosis cohort. No differences were observed in procedural safety, acute success rates, or total RF and fluoroscopy times. These findings are promising, although replication in larger cohorts is required. Visualization, a technique in which patients are guided to modify associated subjective experience, thoughts, or behavior, has also been reported to reduce procedural pain and analgesic requirements during AF ablation [52].
A thorough pre-procedural assessment of chronic medication use is essential to minimize drug–drug interactions during anesthesia, particularly with psychotropic agents. Antidepressants (tricyclics, selective serotonin reuptake inhibitors, serotonin–norepinephrine reuptake inhibitors), antipsychotics, anxiolytics, and stimulants can modify anesthetic effects, either enhancing or, more commonly, reducing efficacy, and may precipitate serious side effects [53].
Patients with chronic alcohol use disorder should be identified pre-procedurally, and analgesic and sedative regimens adjusted accordingly, including opioid dose reduction and careful benzodiazepine titration [54]. These patients have an increased risk of postoperative complications such as bleeding and delirium and require close monitoring [54].
Postoperative nausea and vomiting are common after anesthesia. Current guidelines recommend pre-procedural risk assessment and prophylactic pharmacologic interventions, including ondansetron, droperidol, and dexamethasone [55].
PFA may stimulate the phrenic nerve and bronchus, leading to diaphragmatic contraction and dry cough, particularly during left superior PVI [56]. These events can induce patient movement and compromise the accuracy of three-dimensional mapping. Delivering PFA at the end of expiration can reduce diaphragmatic contraction and suppress dry cough during procedures performed under conscious sedation [57]. Although no studies have specifically evaluated intravenous lidocaine to prevent cough during PFA, many anesthesiologists advocate the use of intravenous lidocaine based on evidence supporting postoperative cough reduction [58]. Finally, vagal responses may also occur during PFA; prophylactic atropine administration has been shown to mitigate this effect [56].
While general anesthesia is strictly protocolized and administered by anesthesiologists, the pharmacological agents previously described have been employed in heterogeneous combinations, either as continuous intravenous infusions or as intermittent boluses, to achieve deep or conscious sedation. A dedicated scoping review providing a structured overview of anesthetic strategies for cardiac ablation, particularly AF, is currently underway [59]. Meanwhile, Table 2 (Ref. [13, 15, 16, 27, 30, 33, 60, 61]) and Table 3 (Ref. [20, 25, 26, 60, 62]) summarize the principal protocols used for deep and conscious sedation, respectively.
| Author and year | Number of patients | Energy source | Inclusion/exclusion criteria | Drug | Need for NIV or OTI | Sedation-related side effects |
| Salukhe et al. 2012 [27] | 1000 | RF | All consecutive patients | Propofol (2%) | None | Persistent hypotension (13.6%) |
| Fentanyl | Respiratory depression (1.9%) | |||||
| Hypersalivation (0.1%) | ||||||
| Cho et al. 2014 [60] | 45 | RF | Excluded patients with ASA score |
Dexmedetomidine + remifentanil | None | Hypotension (11.1%) |
| Foerschner et al. 2022 [30] | 3211 | RF | All consecutive patients | Midazolam | NIV (1.5%) | Persistent hypotension (12.3%) |
| Propofol (1%) | OTI (0.03%) | |||||
| Fentanyl | ||||||
| Servatius et al. 2022 [33] | 160 | RF (50%) | Excluded patients with severe HF, BMI |
Dexmedetomidine + fentanyl vs. propofol + fentanyl | None | Prolonged hypotension (8%) |
| Cryo (50%) | ||||||
| Grimaldi et al. 2023 [15] | 29 | PFA | All consecutive patients | Midazolam | None | None |
| Dexmedetomidine | ||||||
| Remifentanil | ||||||
| (premedication with ondansetron and dexamethasone) | ||||||
| Iacopino et al. 2023 [16] | 66 | PFA | All consecutive patients | Midazolam | None | Vomit after fentanyl (1.5%) |
| Fentanyl | ||||||
| Ketamine | ||||||
| Wahedi et al. 2024 [13] | 100 | Cryo (50%) | Redo‐ablation procedures excluded | Midazolam | None | Aspiration resulting in mild pneumonia (2%) |
| PFA (50%) | Propofol (1%) | |||||
| Sufentanil | ||||||
| Rillig et al. 2024 [61] | 63 | PFA | Redo‐ablation procedures excluded | Fentanyl | Larynx mask (2.5%) | None |
| Propofol (1%) |
Abbreviations: NIV, non-invasive ventilation; OTI, orotracheal intubation; RF, radiofrequency energy ablation; Cryo, cryoablation; PFA, pulsed-field ablation; HF, heart failure; BMI, body mass index; ASA, American Society of Anesthesiologists.
| Author and year | Number of patients | Energy source | Inclusion/exclusion criteria | Drug | Need for NIV/OTI | Sedation-related side effects |
| Cho et al. 2014 [60] | 45 | RF | Excluded patients with ASA score |
Midazolam Remifentanil | None | Oxygen saturation |
| Moravec et al. 2021 [26] | 73 | RF | Excluded patients with persistent AF, LVEF |
Midazolam Fentanyl | None | None |
| Calvert et al. 2025 [25] | 8 | PFA | Excluded patients with BMI |
Midazolam Fentanyl | None | None |
| Poggi et al. 2025 [62] | 58 | RF with vHPSD protocol | Excluded redo‐ablation procedures | Midazolam Fentanyl | None | None |
| Massalha et al. 2025 [20] | 399 | Cryo 88% | N/A | Midazolam Fentanyl | None | None |
| RF 12% |
Abbreviations: LVEF, left ventricular ejection fraction; vHPSD, very-high-power, short duration; N/A, not available; other abbreviations as in Table 2.
Deep sedation is generally achieved by combining hypnotic and analgesic agents (e.g., propofol with fentanyl or dexmedetomidine with remifentanil), titrated individually to the desired level of sedation.
In a large study by Salukhe et al. [27], 1000 consecutive patients underwent AF ablation under deep sedation without assisted ventilation using 2% propofol and fentanyl. Sedation was administered, monitored, and controlled entirely by electrophysiologists. Sedation-related adverse effects requiring discontinuation of propofol and conversion to midazolam boluses occurred in 15.6% of patients (13.6% due to persistent hypotension, 1.9% due to respiratory depression, and 0.1% due to hypersalivation). Only one patient required brief (4 minutes) mechanical bag-mask ventilation, and no procedures were aborted because of sedation-related complications.
In a randomized controlled trial by Cho et al. [60], 45 patients receiving dexmedetomidine plus remifentanil were compared with those receiving midazolam plus remifentanil. Patients in the dexmedetomidine group achieved a median Ramsay sedation score of 3 and a bispectral index of 70, consistent with deep sedation. Dexmedetomidine was administered at 0.2–0.7 µg/kg/h following a loading dose of 1.0 µg/kg over 10 minutes, and remifentanil was infused at 1.2–2.4 µg/kg/h. No invasive airway management was required; five patients experienced isolated hypotensive episodes, which were corrected by adjusting infusion rates. Compared with the midazolam group, dexmedetomidine was associated with less respiratory depression, deeper sedation, improved analgesia, and lower remifentanil requirements.
In 2022, Foerschner et al. [30] retrospectively analyzed 3211
consecutive AF ablations performed under deep sedation. Sedation was initiated
with midazolam and propofol boluses, followed by a continuous infusion of 1%
propofol administered by an electrophysiology nurse under physician supervision,
with supplemental fentanyl boluses for discomfort or pain. Hypotension occurred
in 12.3% of patients and was treated with norepinephrine. Only one patient
(0.03%) required intubation, while 47 patients (1.5%) required non-invasive
ventilation due to oxygen saturation
In a single-center randomized trial, Servatius et al. [33] enrolled 160 patients undergoing initial AF ablation (RF or cryoablation) and randomized the patients to receive either dexmedetomidine or propofol. Deep sedation was administered by a trained nurse under the operator’s supervision. Propofol was delivered via target-controlled infusion (a technique that uses a computer-controlled infusion pump that delivers the drug based on patient-specific parameters to achieve a predicted plasma concentration). In contrast, dexmedetomidine was infused continuously (0.2–0.7 µg/kg/h) following a loading dose (0.5–1 µg/kg over 10 minutes), with adjunctive fentanyl boluses. Hypercapnia was more frequent with propofol (29% vs. 10%; p = 0.003), whereas the incidence of prolonged hypotension did not differ significantly between groups (3% vs. 8%; p = 0.147). Patient satisfaction was higher in the propofol group.
More recently, deep sedation has also been investigated for PFA. In a study by
Grimaldi et al. [15], patients received pre-procedural intravenous
midazolam 2 mg, ondansetron 4 mg, and dexamethasone 4 mg. The degree of sedation
was subsequently assessed using the Richmond agitation–sedation scale, the
visual analog scale, and the patient state index. During ablation,
dexmedetomidine (0.5–1.4 µg/kg/h) and remifentanil
(target-controlled infusion 0.5–2 ng/mL) were administered by
electrophysiology-trained staff and titrated to achieve a patient state index
score
Iacopino et al. [16] described a ketamine-based deep sedation protocol
with spontaneous respiration for PFA, managed by an anesthesiologist and an
operating room nurse. Patients received midazolam (2 mg) and fentanyl (1.5
µg/kg), followed by local anesthesia. An additional midazolam bolus
(2 mg) was administered after transseptal puncture, followed by ketamine (1
mg/kg) administered 5 minutes before energy delivery and titrated to the
condition, response, vital signs, and cough of the patient. Maintenance ketamine
boluses of 10 mg were administered once the effective anesthetic level was
reached. Mean sedation time was 56.4
Wahedi et al. [13] compared a sedation regimen that included midazolam, a propofol bolus and infusion, and sufentanil boluses between patients undergoing PFA and cryoablation. Sedative drug requirements were significantly higher in the PFA group, whereas complication rates were similar, with only one mild case of aspiration pneumonia in the PFA group.
Rillig et al. [61] compared deep sedation with general anesthesia for
PFA. Deep sedation was managed by trained electrophysiology laboratory staff and
consisted of fentanyl (25 µg) and propofol (3–5 mg) boluses,
followed by a propofol infusion (5 mg/kg/h), with additional boluses given before
ablation onset and as required thereafter. Only one patient with BMI
Respiratory depression represents the most common adverse event during deep sedation. Capnography enables monitoring of airway patency, respiratory rate and pattern, and pulmonary perfusion. Both the European and American Societies of Anesthesiology recommend using capnography, in addition to visual observation and pulse oximetry, for the early detection of ventilatory impairment [63, 64]. Capnography uses infrared spectroscopy to measure end-tidal CO2 (ETCO2); changes in ETCO2 values or waveform morphology enable early detection of hypoventilation or apnea, which typically precede hypoxemia.
In the midazolam–remifentanil arm of the study by Cho et al. [60], patients achieved a median Ramsay score of 2 and a bispectral index score of 90, consistent with conscious sedation. Sedation was provided using midazolam 0.02–0.05 mg/kg as a bolus and remifentanil infusion (3.6–7.2 µg/kg/h). Desaturation occurred in 33% of patients and was managed with supplemental oxygen via a face mask and airway maneuvers (head elevation, chin lift, jaw thrust); no invasive airway support was required.
Moravec et al. [26] compared 73 patients undergoing RF ablation under conscious sedation with 73 patients undergoing RF ablation under general anesthesia. Conscious sedation consisted of fentanyl 100 µg as an intravenous bolus and a continuous midazolam infusion (initiated at 0.03–0.2 mg/kg/h and titrated to achieve the target level of sedation according to the Richmond agitation–sedation scale: –2 to –3). No sedation-related complications were observed. Clinical outcomes were comparable to those under general anesthesia, although procedure duration and fluoroscopy time were longer in the conscious sedation group.
In a small PFA series, Calvert et al. [25] administered midazolam (1–2 mg) and fentanyl (50 µg) as boluses at the beginning of the procedure, before the first ablation delivery, with additional doses administered at the discretion of the operator. One patient required conversion to general anesthesia due to pain. No respiratory depression or hypotension requiring intervention was reported.
Poggi et al. [62] evaluated conscious sedation during very-high-power, short-duration RF ablation (90 W, 4 s lesions, temperature-controlled protocol). Midazolam 1–2 mg, followed by fentanyl 50–100 µg, was administered upon request to achieve pain control. Only 7% of patients required fentanyl, and approximately 40% underwent ablation without any anesthetic drugs.
Finally, the Israeli Catheter Ablation Registry, analyzed by Massalha et al. [20], included 1002 patients: 53% received general anesthesia, 6.3% deep sedation, and 40% conscious sedation (midazolam and fentanyl administered by electrophysiologists or trained cardiology nursing staff). In this registry, rates of PVI achievement, complications, and AF recurrence at 2-year follow-up did not differ between general anesthesia and conscious sedation. Predictors of general anesthesia use included RF energy, high-volume centers, persistent AF, and prior cerebrovascular events.
In several studies, drug administration and monitoring were performed by specially trained electrophysiology staff. However, drug administration may still be associated with respiratory depression and persistent hypotension [13, 27, 30, 33, 60], especially when deep sedation is achieved (Table 2), and occasionally requires non-invasive ventilation, a laryngeal mask airway, or endotracheal intubation [30, 61]. Therefore, as recommended by the American Society of Anesthesiologists [19], practitioners administering sedation must be able to rescue patients whose level of sedation becomes deeper than intended.
In the European Heart Rhythm Association survey [10], national legislation governing procedural sedation was reported to vary considerably across European countries. In some jurisdictions, including France, Spain, and Italy, deep sedation with specific agents cannot legally be performed without an anesthesiologist present in the operating room/interventional laboratory [65]. Conversely, in countries such as Germany, standardized protocols allow deep sedation with propofol during AF ablation without an anesthesiologist in attendance. In the same survey, 60% of centers reported that an anesthesiologist was required in the electrophysiology laboratory. Another 29% indicated that deep sedation could be administered in the presence of a specifically trained nurse or a second physician, whereas 11% reported that electrophysiologists could independently administer deep sedation. Similarly, in an Italian survey on deep sedation practices in electrophysiology and cardiac pacing laboratories [11], AF ablation was most commonly performed with anesthesiology assistance or with benzodiazepine-based sedation alone. However, in a minority of centers (19%), propofol was administered without anesthesiology support, presumably within predefined and institutionally approved protocols. These findings likely reflect the organizational structure of the participating institutions, as only 27% were high-volume centers performing more than 100 procedures annually. This scenario may evolve with increasing procedural volumes and the progressive implementation of structured organizational models, as observed worldwide [10]. Furthermore, the Italian consensus document on quality and performance in cardiac pacing and electrophysiology, issued by the Italian Association of Arrhythmology and Cardiac Pacing together with the Italian Federation of Cardiology, requires that an anesthesiologist be available at tertiary centers performing left-heart ablation procedures [66]. Notably, the literature on AF catheter ablation lacks recent, comprehensive, and standardized training protocols for the administration of conscious or deep sedation by nurses or non-anesthesiologist physicians, representing an important area for future investigation.
Within this framework, sedation strategies should be tailored according to patient characteristics, energy source, expected procedural duration, and anticipated pain burden [67]. Optimal patient management requires predefined, shared protocols between electrophysiologists and anesthesiologists, supported by an appropriate organizational model. As illustrated in Fig. 1, the choice among general anesthesia, deep sedation, and conscious sedation should be based on multidisciplinary decision-making that incorporates patient profile, procedural complexity, and institutional expertise, with important implications for clinical outcomes, costs, and resource utilization.
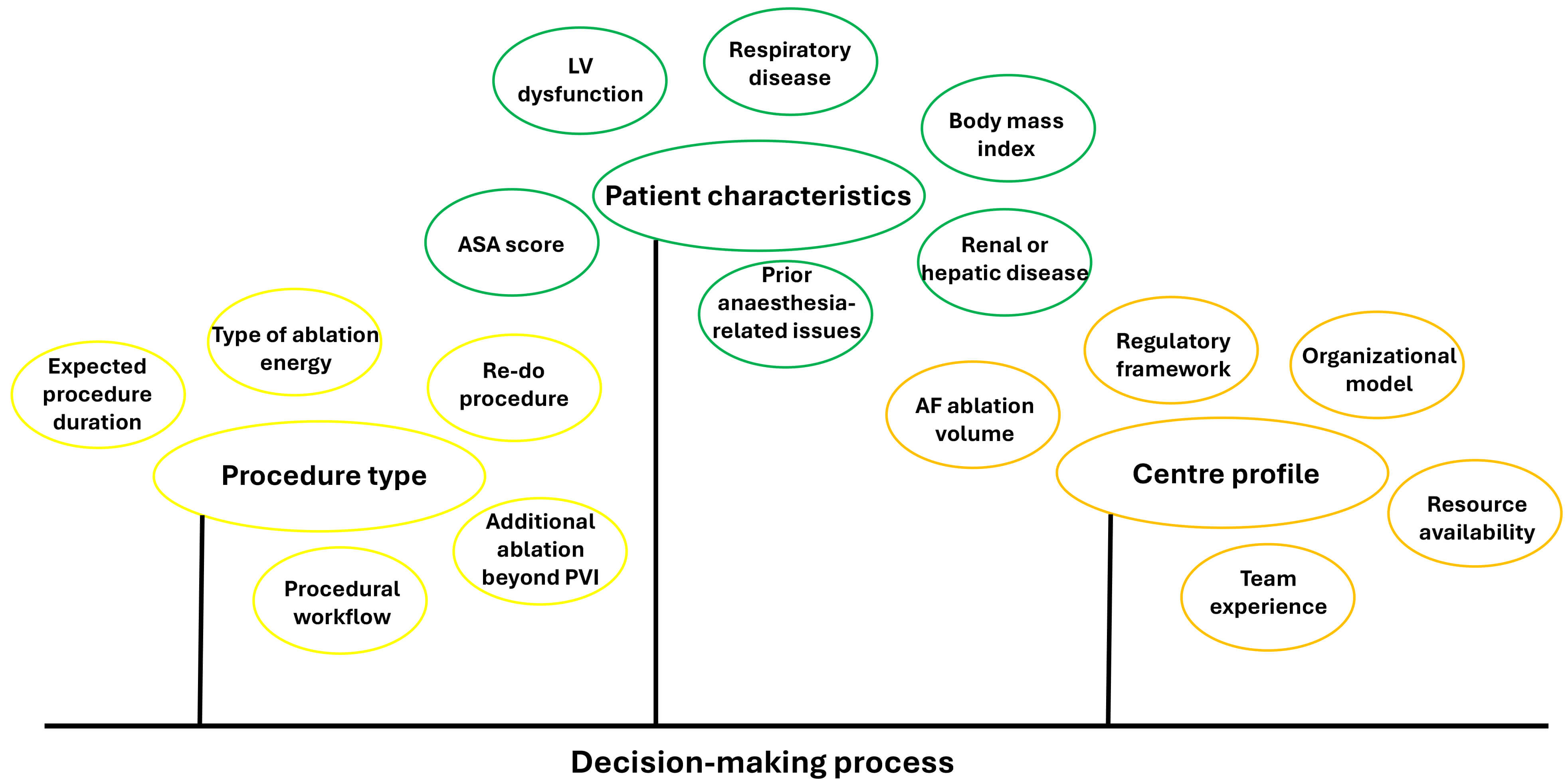 Fig. 1.
Fig. 1.
Factors to consider in the selection of a sedation and analgesia strategy for patients undergoing atrial fibrillation ablation. Abbreviations: AF, atrial fibrillation; ASA, American Society of Anesthesiologists; LV, left ventricular; PVI, pulmonary vein isolation.
The number of AF ablation procedures is increasing worldwide as clinical indications expand. Accordingly, the choice of sedation–analgesia strategy has become a key determinant of patient safety and comfort, procedural efficacy, and resource utilization. The available literature demonstrates substantial heterogeneity in both pharmacological regimens and depth of sedation, and no consensus has been reached regarding the optimal anesthetic approach for AF ablation.
This review summarizes the pharmacological characteristics of the principal agents and the protocols used for deep and conscious sedation. Ultimately, the sedation strategy should be individualized according to patient characteristics, the regulatory framework, the energy source, and center-specific organizational factors.
Conceptualization: BC, IM, SD, CA, ADO, MA, RDP; investigation: BC, IM, SD, AR, MA, RDP; data interpretation: GC, SDB, MN, PLP, AR, MZ, GB, SGP, ST; writing-initial draft preparation: BC, IM, SD, CA, MA, RDP; initial critical review and editing: GC, SDB, MN, PLP, AR, MZ, GB, ADO, SGP, ST, MA, RDP; project administration: BC, CA, RDP; supervision: GC, SDB, MN, PLP, MZ, GB, ADO, SGP, ST. All authors contributed to the final critical revision of the manuscript. All authors read, revised, and approved the final version of the paper. All authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Not applicable.
The authors are very grateful to Prof. Paolo Severgnini, from the Department of Biotechnologies and Life Science—University of Insubria, for his advice and his assistance in reviewing the manuscript. The authors are also deeply grateful to Carola Griffith Brookles, MD, for her assistance in English language editing.
This research received no external funding.
The authors declare no conflicts of interest. Giuseppe Boriani is serving as one of the Editorial Board members of this journal. Matteo Anselmino and Roberto De Ponti are serving as Guest Editors of this journal. We declare that Giuseppe Boriani, Matteo Anselmino, and Roberto De Ponti had no involvement in the peer review of this article and have no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Karol E. Watson.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.