





Retraction published on 24 Dec 2025, see Reviews in Cardiovascular Medicine 2025, 26(12).
 , Libo Yang 2,†, Meng Cao 3, Ru Yan 2, Baozhen Zhu 4, Guangzhi Cong 2, Shaobin Jia 2,*
, Libo Yang 2,†, Meng Cao 3, Ru Yan 2, Baozhen Zhu 4, Guangzhi Cong 2, Shaobin Jia 2,*
1 The First Clinical College of Ningxia Medical University, 750001 Yinchuan, Ningxia Hui Autonomous Region, China
2 Department of Cardiovascular Medicine, General Hospital of Ningxia Medical University, 750001 Yinchuan, Ningxia Hui Autonomous Region, China
3 School of Nursing, Ningxia Medical University, 750001 Yinchuan, Ningxia Hui Autonomous Region, China
4 Department of Cardiovascular Medicine, Tongxin County People's Hospital, 751300 Wuzhong, Ningxia Hui Autonomous Region, China
†These authors contributed equally.
Abstract
Stent malapposition (SM) remains a significant challenge in percutaneous coronary intervention (PCI), particularly in cases involving calcified coronary lesions. However, the predictors of SM and their relationship with clinical outcomes remains unclear. This study aims to identify the predictors of SM through optical coherence tomography (OCT) and assess its impact on clinical outcomes.
In this single-center, retrospective observational study, we analyzed 384 patients who underwent PCI with OCT imaging for calcified coronary lesions between January 2019 and December 2023. Patients were divided into two groups based on post-PCI OCT findings: the SM group (n = 142) and non-SM group (n = 242). We compared calcium characteristics, procedural parameters, and clinical outcomes between the two groups.
The SM group exhibited more severe calcium characteristics, including a larger calcium arc (295.8° ± 58.4° vs 248.6° ± 62.3°, p < 0.001), greater thickness (1.12 ± 0.31 mm vs 0.89 ± 0.28 mm, p < 0.001), and longer length (18.6 ± 7.2 mm vs 12.8 ± 6.4 mm, p < 0.001). Multivariate analysis identified calcium arc >270° (odds ratio (OR) 2.84, 95% CI 1.86–4.32, p < 0.001), calcium thickness >1.0 mm (OR 2.16, 95% CI 1.42–3.28, p = 0.001), and diabetes mellitus (OR 1.68, 95% CI 1.12–2.52, p = 0.012) as independent predictors of SM. Over a median follow-up of 18.6 months, the SM group had higher rates of major adverse cardiovascular events (15.5% vs 8.7%, p = 0.04), primarily driven by increased target lesion revascularization (8.5% vs 4.1%, p = 0.03).
Specific calcium characteristics and diabetes mellitus are strong predictors of stent malapposition in calcified coronary lesions. The presence of stent malapposition is associated with worse clinical outcomes, highlighting the importance of optimal lesion preparation and stent deployment strategies in high-risk lesions.
Keywords
- calcified coronary lesions
- optical coherence tomography
- percutaneous coronary intervention
- stent malapposition
- calcium characteristics
- clinical outcomes
Coronary artery calcification (CAC) represents a common obstacle in modern percutaneous coronary intervention (PCI), encountered in around 20–30% of cases [1]. The presence of severe calcification not only complicates procedural aspects but also significantly impacts both immediate and long-term outcomes. Recent evidence from large-scale clinical trials has shown that calcified lesions are associated with higher rates of procedural complications, stent failure, and suboptimal clinical outcomes compared to non-calcified lesions [2].
The pathophysiology of coronary calcification is complex and multifaceted. Recent single-cell meta-analyses have revealed distinct vascular cell states and markers specifically associated with atherosclerotic calcification, including that the process involves multiple cellular mechanisms and inflammatory pathways [2]. These molecular insights have enhanced our understanding of why traditional interventional approaches may have limited success in severely calcified lesions.
Stent malapposition (SM), where the stent struts fail to fully adhere to the vessel wall, has been recognized as a key contributor to post-implantation complications, especially in the presence of calcification [3]. Achieving optimal stent deployment in calcified vessels is compounded by factors such as reduced vessel compliance, irregular surface geometry, and the risk of calcium fracture during lesion preparation. Current preparation strategies, including rotational atherectomy, have shown variable success in modifying calcium to facilitate optimal stent deployment. However, the recent introduction of intravascular lithotripsy (IVL) has shown promising results in severely calcified lesions, with clinical trials showing significant improvements in procedural success rates and a reduction in complications [1].
Optical Coherence Tomography (OCT) has revolutionized our understanding of stent-vessel wall interactions by providing high-resolution (10–20 µm) intravascular imaging. This advanced technology enables precise evaluation of calcium characteristics, such as arc, thickness, and length, as well as detailed assessment of stent expansion and apposition [4]. The superior resolution of OCT, compared to traditional intravascular imaging modalities, has made it particularly valuable in evaluating complex calcified lesions, where the detailed assessment of calcium morphology and distribution is crucial for effective procedural planning and optimization [5].
The concept of lifetime management has recently emerged as a critical consideration in the field of PCI for severely calcified lesions [6]. This approach recognizes that the long-term clinical outcomes following drug-eluting stent implantation are notably worse in calcified compared to non-calcified lesions [7]. Studies have shown that calcified lesions are associated with higher rates of in-stent restenosis, late stent failure, and major adverse cardiovascular events [7]. The treatment of in-stent restenosis or stent underexpansion in calcified lesions presents unique challenges, necessitating a careful balance between immediate procedural success and long-term outcomes [8].
Contemporary antiplatelet strategies play a crucial role in the management of patients with calcified coronary lesions undergoing PCI [8]. The optimal duration and intensity of dual antiplatelet therapy must be carefully balanced with the risk of bleeding, particularly in this often elderly and comorbid patient population [9]. Recent studies have highlighted the importance of individualized approaches to antithrombotic therapy, taking into account both patient-specific factors and lesion characteristics to optimize outcomes and minimize complications.
The relationship between specific calcium patterns and subsequent stent behavior has become a focal point of intense research [10]. Factors such as calcium arc, thickness, and distribution patterns play crucial roles in determining stent expansion and apposition, though the precise mechanisms linking these characteristics to clinical outcomes are not yet fully understood. Recent analyses using advanced imaging techniques have shown that the three-dimensional distribution of calcium within the vessel wall may be more predictive of procedural success and long-term outcomes than traditional measures of calcium burden [5].
Therefore, this study aims to identify predictive factors for stent malapposition in calcified coronary lesions using OCT assessment and to evaluate their relationship with clinical outcomes through a retrospective observational design. By leveraging the high-resolution imaging capabilities of OCT and conducting detailed analyses of calcium characteristics, we aim to develop a more comprehensive understanding of the factors contributing to stent malapposition in calcified lesions and their impact on clinical outcomes.
We performed a retrospective case-control study at General Hospital of Ningxia Medical University, covering the period from January 2019 to December 2023. The study protocol was reviewed and approved by the institutional ethics committee in April 2025 (approval number: KYLL-2025-1256). Although patient data collected between 2019 and 2023, written informed consent for data use in research was obtained from all participants at the time of their procedures, and data analysis was conducted only after ethics approval had been formally granted. All procedures complied with institutional guidelines and the principles of the Declaration of Helsinki.
Eligible cases were identified from the hospital database based on PCI procedures guided by OCT for calcified coronary lesions. Calcification was determined by angiographic and OCT criteria, specifically as lesions showing calcium arcs exceeding 90° or lengths greater than 5 mm. Patients were divided into SM and non-SM groups according to post-procedural OCT assessments of stent apposition. The analysis included only lesions managed with drug-eluting stent (DES) implantation. Cases treated solely with drug-coated balloons (DCBs) were excluded due to the inability to assess stent malapposition in the absence of stent deployment.
Inclusion required patients to be
A frequency-domain OCT system (ILUMIEN OPTIS, cat. no. C408650, Abbott Vascular, Santa Clara, CA, USA) was used to acquire intravascular images following intracoronary administration of 100–200 µg nitroglycerin (Nitrostst®, cat. no. NDC0071-0418-13, Pfizer lnc., New York, NY, USA). Iodinated contrast medium (lohexol, Omnipaque 350, cat. no. NDC00407141491, GE Healthcare, Chicago, IL, USA) was injected through the guiding catheter to clear blood during OCT image capture. Images were collected via automated pullback at a speed of 20 mm/s and a frame rate of 180 frames per second. Contrast medium was injected through the guiding catheter to clear blood during OCT image capture. Imaging measurements were conducted before and after intervention, adhering to standardized OCT analysis protocols.
A dedicated OCT analysis core laboratory evaluated all OCT recordings. Two experienced analysts independently performed the OCT analysis, blinded to clinical data and outcomes. In cases of disagreement, a third senior analyst reviewed and adjudicated the findings to reach consensus. OCT images were analyzed at 1-mm intervals throughout the stented segment and in the 5-mm proximal and distal reference segments to ensure comprehensive assessment.
Calcium characteristics were quantified, including arc (measured in degrees),
thickness (measured in millimeters), and length (measured in millimeters). Stent
malapposition was defined as the separation of at least one stent strut from the
vessel wall by a distance exceeding the combined thickness of the strut and
polymer coating. Although stent malapposition was defined according to standard
OCT criteria, previous studies suggest that only cases with a maximum
malapposition distance
Stent underexpansion was defined as a minimum stent area (MSA)
All patients received standard pre-procedural dual antiplatelet therapy,
consisting of a 300 mg loading dose of aspirin followed by 100 mg daily, in
combination with a Purinergic receptor P2Y12 (P2Y12) inhibitor as per current
guidelines. The selection of the lesion preparation strategy, including
conventional balloon pre-dilatation, cutting/scoring balloon, rotational
atherectomy (RA), or IVL, was left to the operator’s discretion, based on OCT and
angiographic assessment. Specifically, RA was generally preferred for lesions
with concentric, thick calcification and tight stenosis, where device crossing or
balloon expansion was anticipated to be difficult. IVL was often selected for
lesions with deep calcium or eccentric plaques with limited response to balloon
dilation, particularly when calcium thickness exceeded 0.5–0.7 mm but crossing
was feasible. Cutting/scoring balloons were used for focal calcification,
especially when calcium arc was
PCI procedures were performed using standard techniques via either the radial or
femoral approach. The selection of stent type and size was based on vessel
reference dimensions determined by both angiographic and OCT measurements.
Post-dilatation was routinely with non-compliant balloons at high pressure (
Baseline demographic characteristics, cardiovascular risk factors, and procedural details were collected from electronic medical records. Laboratory data, including lipid profiles, high-sensitivity C-reactive protein (hs-CRP), and N-terminal pro-brain natriuretic peptide (NT-proBNP) levels, were obtained within 24 hours prior to the procedure. Procedural characteristics including lesion preparation techniques, stent parameters, and technical details were recorded from procedural reports. The specific type of drug-eluting stents used [Biodegradable Polymer Drug-eluting Stents (BP-DES) vs. Drug-Eluting Stent with Durable Polymer (DP-DES)] was not consistently documented in the procedural records, and therefore was not included in the present analysis.
Clinical follow-up was conducted through outpatient visits or telephone contacts at 1, 3, 6, and 12 months post-procedure, and annually thereafter. Major adverse cardiovascular events (MACE) were defined as a composite of cardiac death, target vessel myocardial infarction, and target lesion revascularization. All events were adjudicated by an independent clinical events committee that was blinded to the OCT findings.
The primary endpoint was to identify independent predictors of stent malapposition in calcified coronary lesions. Secondary endpoints included evaluating the correlation between clinical and imaging parameters, identifying factors associated with treatment success (defined as the absence of residual angina and freedom from MACE), and assessing the prognostic implications of stent malapposition based on MACE rates during follow-up.
Based on previous studies reporting a 20% incidence of stent malapposition and assuming a 70% success rate in achieving optimal stent expansion, a sample size of 120 patients per group was calculated to provide 80% power to detect significant differences between groups at a two-sided alpha level of 0.05.
Continuous variables were expressed as mean
Multivariable logistic regression analysis was performed to identify independent
predictors of stent malapposition, including variables with p
Survival analysis was performed using Kaplan-Meier curves, with the log-rank
test applied for group comparison. Cox proportional hazards regression analysis
was used to assess the relationship between stent malapposition and clinical
outcomes. All statistical analyses were performed using SPSS version 26.0 (IBM
Corp., Armonk, NY, USA). A two-sided p
We acknowledge the potential for multicollinearity, particularly between diabetes and calcium severity. However, due to the retrospective design and limited sample size, formal assessment of Variance inflation factors (VIFs) or interaction terms was not performed. This is considered a limitation of the study.
Between January 2019 and December 2023, a total of 428 patients with calcified coronary lesions underwent PCI with OCT imaging at our institution. After applying the inclusion and exclusion criteria, 384 patients were included in the final analysis. Of these, 142 patients (37.0%) were categorized into the SM group, while 242 patients (63.0%) were assigned to the non-SM group (Fig. 1).
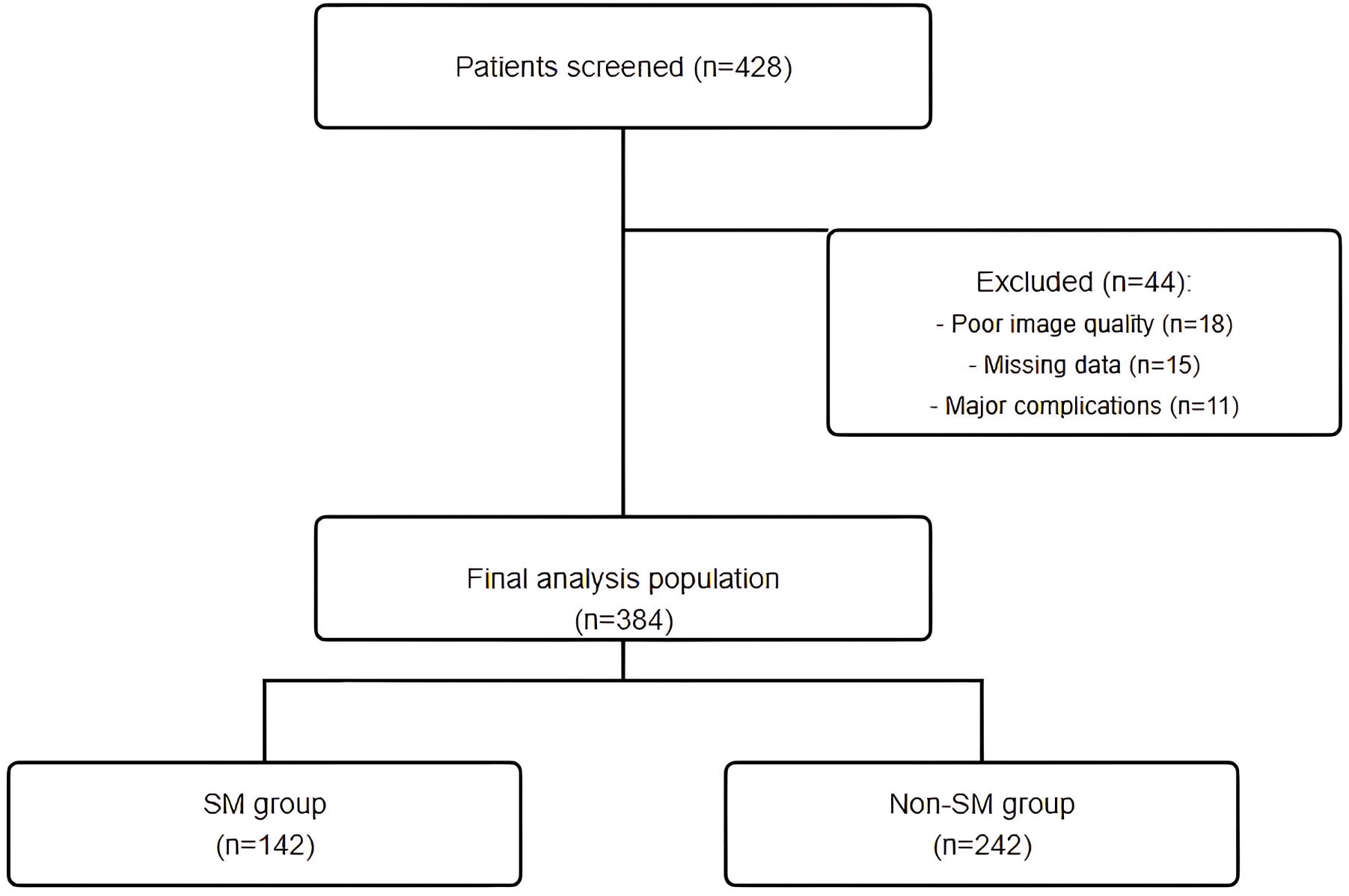 Fig. 1.
Fig. 1.
Study flow chart. A total of 428 patients who underwent PCI with OCT imaging for calcified coronary lesions were screened. After applying inclusion and exclusion criteria, 384 patients were included in the final analysis (142 in the SM group and 242 in the non-SM group). Main exclusion reasons were poor OCT image quality (n = 18), missing clinical data or insufficient follow-up (n = 15), and major periprocedural complications (n = 11). PCI, percutaneous coronary intervention; OCT, optical coherence tomography; SM, stent malapposition.
Baseline clinical characteristics were generally comparable between the two
groups (Table 1). However, patients in the SM group were older (68.5
| Characteristics | SM Group (n = 142) | Non-SM Group (n = 242) | p | ||
| Clinical Characteristics | |||||
| Age, years | 68.5 |
65.3 |
0.002 | ||
| Male sex | 98 (69.0) | 174 (71.9) | 0.548 | ||
| Body mass index, kg/m² | 25.8 |
25.4 |
0.312 | ||
| Hypertension | 112 (78.9) | 182 (75.2) | 0.413 | ||
| Diabetes mellitus | 60 (42.3) | 80 (33.1) | 0.071 | ||
| Dyslipidemia | 94 (66.2) | 152 (62.8) | 0.504 | ||
| Current smoker | 38 (26.8) | 72 (29.8) | 0.531 | ||
| Prior MI | 32 (22.5) | 48 (19.8) | 0.529 | ||
| Prior PCI | 45 (31.7) | 68 (28.1) | 0.456 | ||
| Laboratory Data | |||||
| LDL-C, mg/dL | 98.5 |
94.8 |
0.257 | ||
| hs-CRP, mg/L | 2.8 (1.2–5.9) | 2.4 (1.0–5.2) | 0.148 | ||
| NT-proBNP, pg/mL | 425 (186–982) | 386 (165–876) | 0.213 | ||
| Procedural Characteristics | |||||
| Target vessel | 0.681 | ||||
| - LAD | 82 (57.7) | 148 (61.2) | |||
| - LCX | 24 (16.9) | 42 (17.4) | |||
| - RCA | 36 (25.4) | 52 (21.5) | |||
| Lesion length, mm | 28.6 |
25.8 |
0.023 | ||
| Reference vessel diameter, mm | 3.1 |
3.2 |
0.058 | ||
| Lesion preparation | |||||
| - Rotational atherectomy | 40 (28.2) | 45 (18.6) | 0.029 | ||
| - Cutting/scoring balloon | 35 (24.6) | 52 (21.5) | 0.475 | ||
| - Intravascular lithotripsy | 22 (15.5) | 21 (8.7) | 0.041 | ||
| Stent characteristics | |||||
| - Number of stents per lesion | 1.8 |
1.6 |
0.012 | ||
| - Total stent length, mm | 41.2 |
36.8 |
0.021 | ||
| - Maximum deployment pressure, atm | 16.8 |
16.5 |
0.237 | ||
Values are mean
Lesion preparation strategies differed significantly between the two groups. The
SM group had a higher rate of complex lesion preparation, including rotational
atherectomy (28.2% vs 18.6%, p = 0.029) and intravascular lithotripsy
(15.5% vs 8.7%, p = 0.041). Pre-procedural OCT analysis revealed more
severe calcium characteristics in the SM group, with a greater calcium arc
(295.8°
Post-intervention OCT analysis demonstrated significant differences in stent
expansion and apposition parameters between the groups. The minimum stent area
was smaller in the SM group (5.8
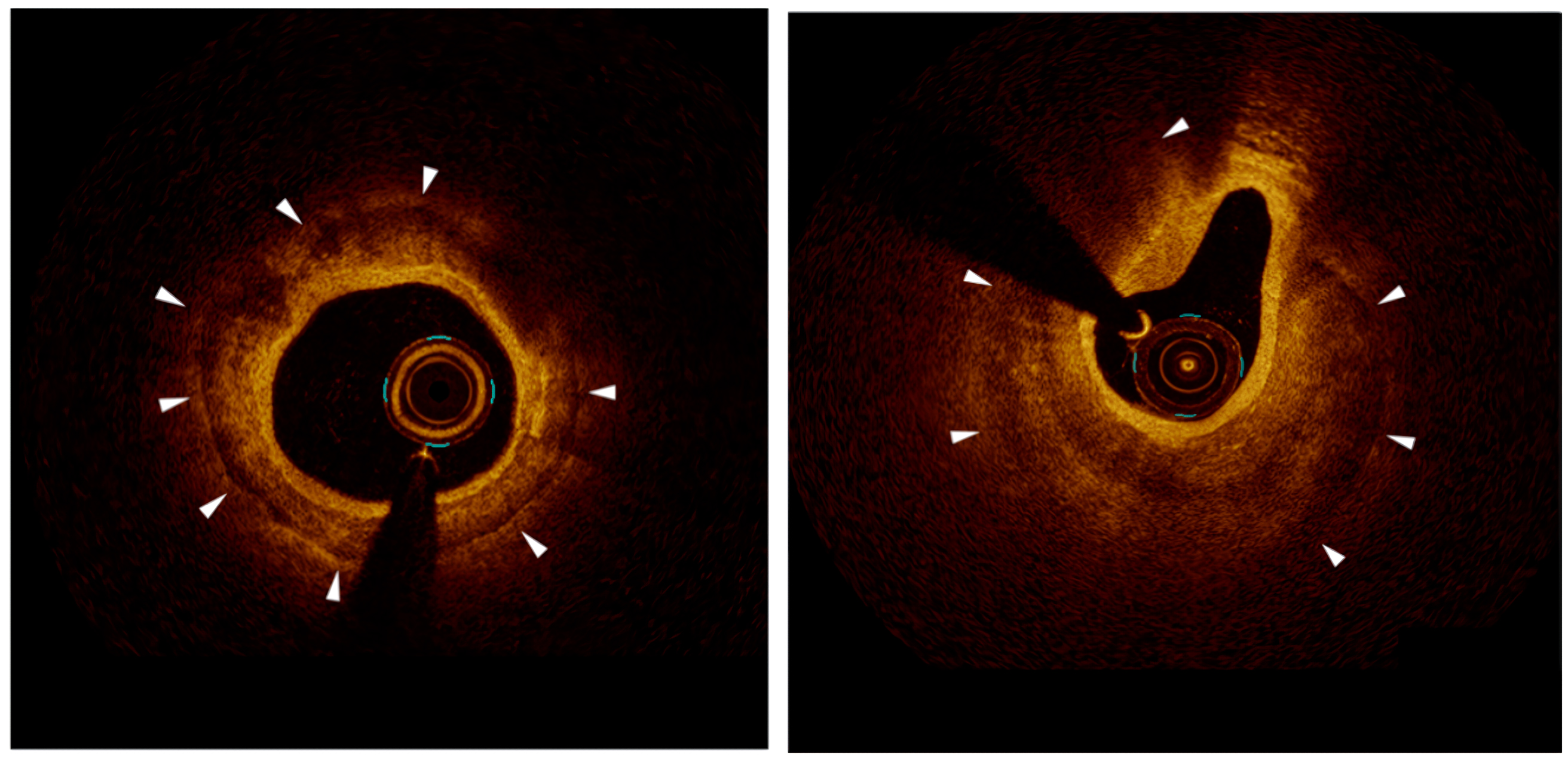 Fig. 2.
Fig. 2.
Representative OCT images. The left picture, optimal stent
apposition in a calcified lesion after successful lesion preparation and stent
deployment. The calcium arc is
Lesions with a calcium arc
Univariate analysis identified several potential predictors of SM, including
age, diabetes mellitus, calcium arc
| Variable | Univariate analysis | Multivariate analysis | |||
| OR (95% CI) | p | OR (95% CI) | p | ||
| Age |
1.62 (1.08–2.43) | 0.021 | 1.38 (0.86–2.21) | 0.182 | |
| Diabetes mellitus | 1.84 (1.26–2.68) | 0.008 | 1.68 (1.12–2.52) | 0.012 | |
| Calcium characteristics | |||||
| - Arc |
3.26 (2.18–4.86) | 2.84 (1.86–4.32) | |||
| - Thickness |
2.48 (1.68–3.66) | 2.16 (1.42–3.28) | 0.001 | ||
| - Length |
1.92 (1.32–2.80) | 0.002 | 1.45 (0.94–2.24) | 0.089 | |
| Lesion length |
1.58 (1.06–2.36) | 0.024 | 1.32 (0.85–2.06) | 0.218 | |
| Reference vessel diameter |
1.46 (0.98–2.18) | 0.062 | - | - | |
| Pre-dilatation pressure |
1.54 (1.04–2.28) | 0.032 | 1.28 (0.82–1.98) | 0.276 | |
| Multiple stents | 1.68 (1.14–2.48) | 0.009 | 1.42 (0.92–2.18) | 0.112 | |
| LAD location | 0.86 (0.58–1.28) | 0.458 | - | - | |
OR, odds ratio; CI, confidence interval. Variables with p
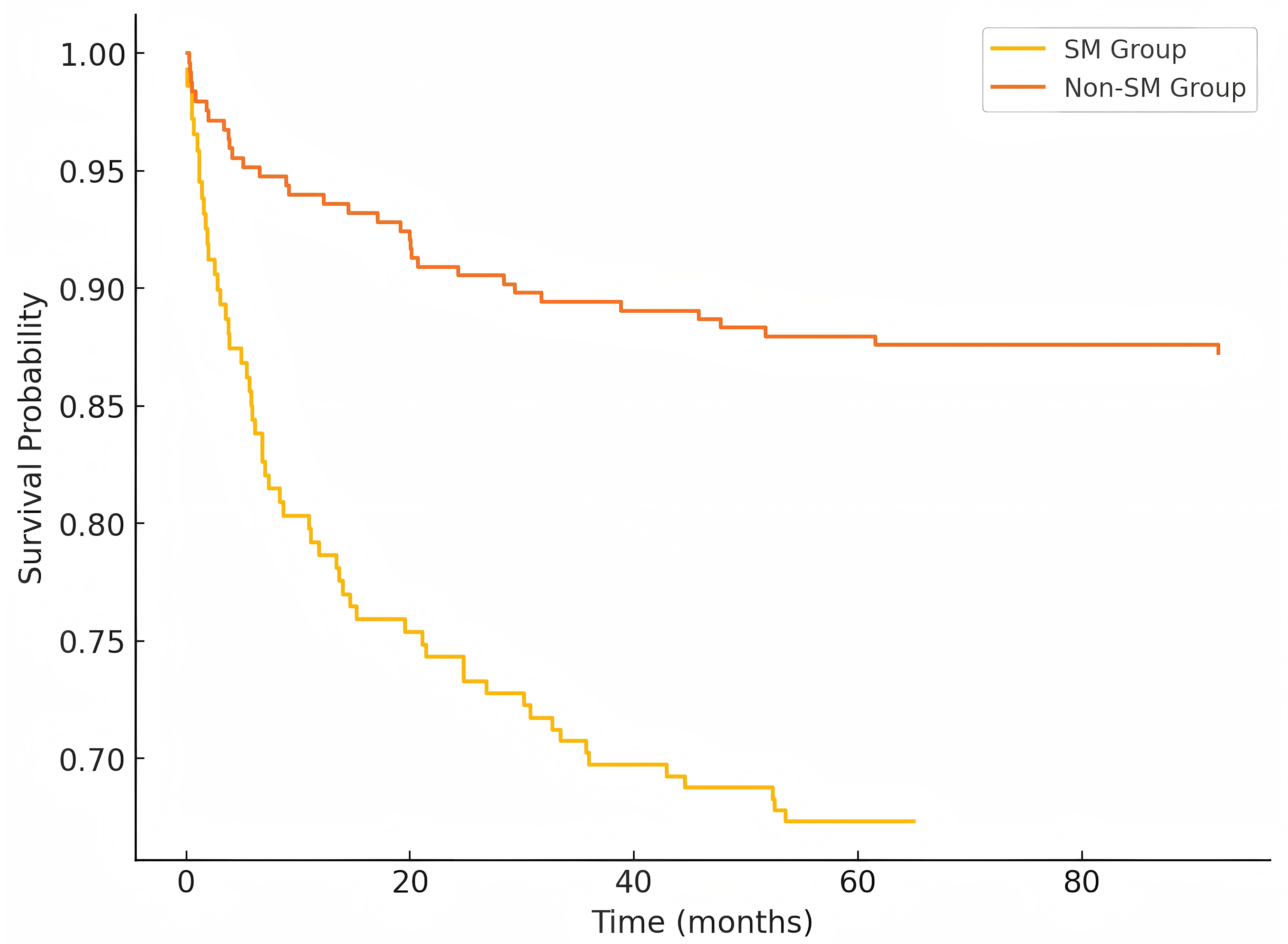 Fig. 3.
Fig. 3.
Receiver operating characteristic (ROC) curve analysis for
prediction of stent malapposition. ROC curve analysis of the prediction model
incorporating calcium characteristics (arc
During a median follow-up of 18.6 months (IQR: 12.4–24.8 months), MACE occurred more frequently in the SM group compared to the non-SM group (15.5% vs 8.7%, p = 0.04). This difference was primarily driven by higher rates of target lesion revascularization (8.5% vs 4.1%, p = 0.03) and target vessel myocardial infarction (4.9% vs 2.1%, p = 0.04).
Kaplan-Meier analysis showed significantly lower MACE-free survival in the SM group (log-rank p = 0.025). Cox regression analysis identified SM as an independent predictor of MACE (adjusted HR 1.86, 95% CI 1.14–3.02, p = 0.013) after adjusting for conventional risk factors (Fig. 4).
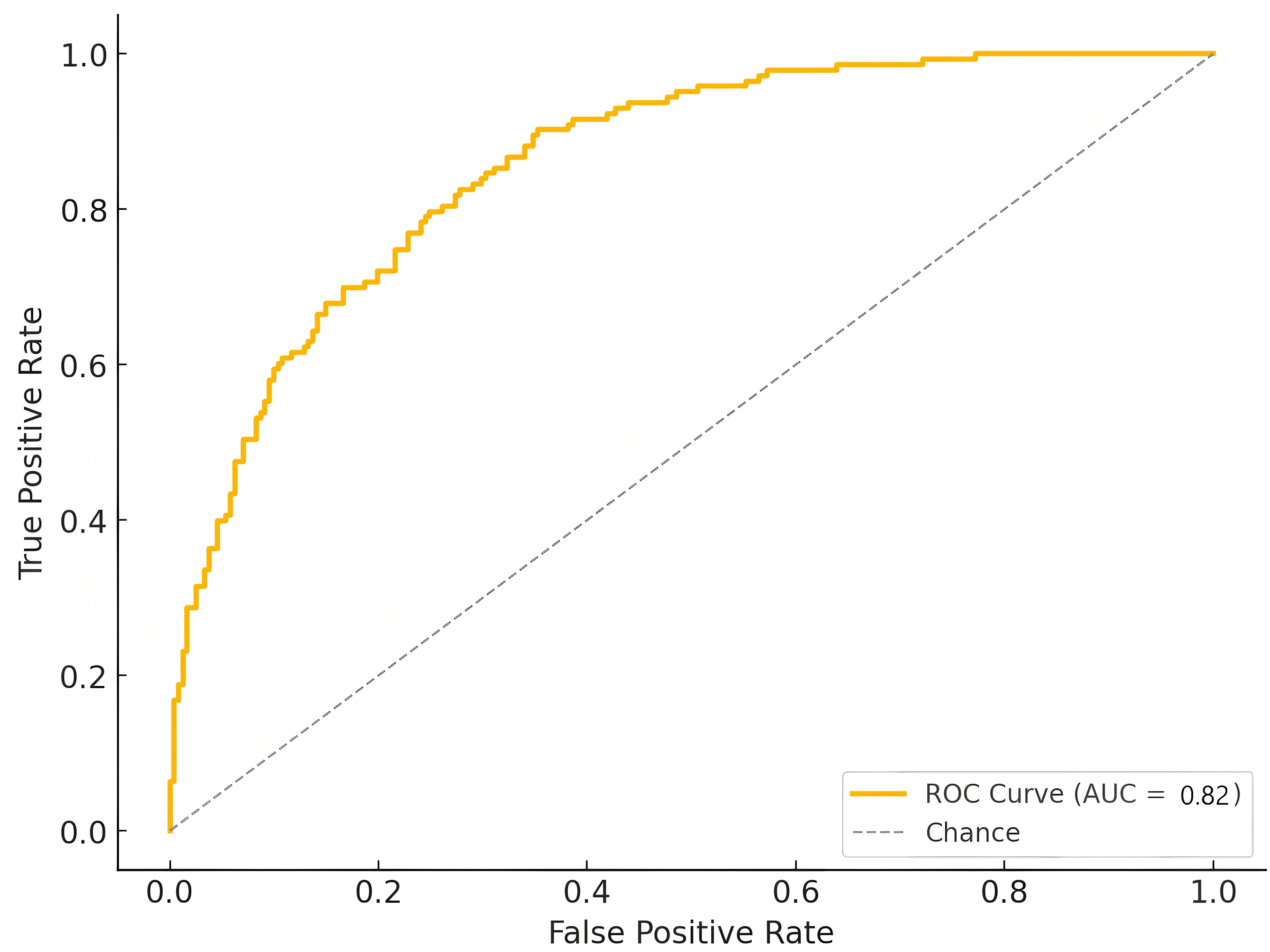 Fig. 4.
Fig. 4.
Kaplan-meier curves for MACE-free survival. Kaplan-Meier analysis demonstrating significantly lower MACE-free survival in the SM group compared to the non-SM group during follow-up (log-rank p = 0.025). MACE, major adverse cardiovascular events.
In this retrospective observational study examining predictive factors and clinical outcomes of stent malapposition in calcified coronary lesions, we identified several key findings that merit detailed discussion.
The relatively high prevalence of SM (37.0%) observed in our study is
consistent with recent evidence from the OPTIVUS-Complex PCI study, which
identified calcified lesions as independent predictors of adverse outcomes, even
in contemporary IVUS-guided PCI practice [12]. Our findings extend these
observations by providing detailed OCT-based analyses of calcium characteristics
that predict malapposition risk. We identified calcium arc
The relationship between diabetes mellitus and stent malapposition deserves particular attention. Recent molecular studies have shown that diabetes accelerates vascular calcification through multiple pathways [13]. Shen et al. [14] showed that diabetes-related vascular calcification involves complex interactions between advanced glycation end products and glucose transporters, suggesting that the metabolic disorder creates a unique microenvironment that may affect stent deployment. These findings help explain our observation of diabetes as showing a trend toward association with stent malapposition, and its identification as an independent predictor in the multivariable model.
While diabetes mellitus was identified as an independent predictor of stent malapposition in our multivariable model, it is important to acknowledge the well-established link between diabetes and increased vascular calcification. This raises the possibility of multicollinearity or interaction between diabetes and calcium severity, which may influence model stability and interpretation. Although we did not perform formal VIF testing due to sample size constraints, this potential overlap should be considered when interpreting the observed associations. Future studies with larger cohorts may be able to better delineate these relationships using interaction terms or stratified analysis.
The impact of lesion preparation strategy on malapposition risk is particularly noteworthy. Despite more aggressive lesion preparation in the SM group, including higher rates of rotational atherectomy, achieving optimal stent deployment remained challenging. Recent data from Koike et al. [15] showed that even with orbital atherectomy, severely calcified lesions still pose significant technical challenges, with a procedural success rate of 96.3% but persistent risk of complications. This observation suggests that current calcium modification techniques may have limitations in certain calcium patterns [16].
The correlation between SM and adverse clinical outcomes observed in our study reinforces findings from recent research. Lee et al. [17] reported that in severely calcified lesions treated with rotational atherectomy, target vessel failure rates reached 16.0% at 1.5 years. Fan et al. [16] emphasized that adequate lesion preparation through calcium modification is crucial for ensuring procedural success and reducing adverse cardiovascular outcomes. Our OCT-based findings regarding calcium characteristics align with recent advances in intravascular imaging. The high resolution of OCT enables precise evaluation of calcium characteristics and stent-vessel wall interactions, providing crucial information for procedural planning [18].
Recent studies have highlighted the potential role of novel therapeutic approaches in addressing the challenges posed by SM. Wei et al. [18] used OCT-based patient-specific modeling to show that SM significantly affects intracoronary flow dynamics, potentially contributing to adverse outcomes. Additionally, Talanas et al. [19] reported that acute stent thrombosis in malapposed stents may be compounded by insufficient platelet inhibition, emphasizing the importance of optimal antithrombotic therapy to mitigrate advance imaging.
Recent studies have further highlighted that vascular healing responses after DES implantation may vary depending on both the polymer type and the lesion modification strategy. In particular, comparisons between BP-DES and DP-DES in heavily calcified lesions treated with atherectomy have shown differential healing behaviors, especially in regions with modified versus non-modified calcium. Histopathologic and imaging evidence suggests that malapposed struts over non-modified calcium may demonstrate delayed neointimal coverage compared to those in modified zones, potentially influencing clinical outcomes. These findings underscore the importance of considering local plaque morphology and stent design when interpreting OCT-based healing patterns in calcified lesions [20, 21].
The relationship between specific calcium patterns and subsequent stent behavior has become a focal point of intense research. Sakakura et al. [22] recently proposed that the concept of “lifetime management” to severely calcified lesions, similar to the approach used in aortic stenosis, given their impact on long-term outcomes. This aligns with our observation that calcium characteristics significantly influence both immediate procedural success and long-term clinical outcomes.
From a therapeutic perspective, our findings suggest that detailed pre-procedural calcium assessment using OCT may help identify high-risk lesions requiring more aggressive preparation strategies. This is particularly relevant given recent evidence from Zhao et al. [7]. This evidence highlights the limitations of traditional drug-eluting stents in certain calcified lesion subsets [22]. The emergence of novel calcium modification techniques and specialized drug-delivery platforms may offer promising alternatives for addressing these challenging cases [7]. Furthermore, although diabetes mellitus emerged as an independent predictor of stent malapposition in our model, its close association with vascular calcification raises the possibility of residual confounding or multicollinearity. This potential interaction warrants further investigation in larger prospective studies.
In addition, the type of DES platform, specifically, whether it employs a DP-DES or BP-DES may significantly influence vascular healing and clinical outcomes, particularly in calcified lesions. Although our dataset did not consistently record this information, it is well established that BP-DES are associated with reduced chronic inflammation, improved endothelialization, and potentially lower long-term rates of adverse events, including stent malapposition. In contrast, DP-DES has been implicated in delayed arterial healing, which may exacerbate the clinical consequences of even minor malapposition in high-risk lesions. Therefore, future studies should consider stratifying SM-related outcomes by stent polymer type to better understand these interactions and guide device selection in heavily calcified vessels.
The importance of achieving optimal stent expansion and apposition in calcified lesions is further emphasized by recent data from Yamamoto et al. [5], which demonstrates that stent underexpansion and malapposition are associated with higher rates of target lesion revascularization. These findings reinforce the need for careful attention to technical aspects of stent deployment in calcified lesions.
Several limitations of this study should be acknowledged. First, detailed information on the type and generation of drug-eluting stents (BP-DES vs. DP-DES) was not available, which may influence stent apposition and clinical outcomes, particularly in calcified lesions. Although we attempted to retrieve stent type data from cath lab records and billing systems, these details were not consistently documented throughout the study period, and incomplete data would have introduced additional bias. Second, data on antiplatelet therapy regimens and duration were not systematically collected, limiting our ability to evaluate their potential impact on stent-related adverse events. Third, subgroup analyses (e.g., based on diabetes status or use of rotational atherectomy) were not performed due to sample size limitations. It remains possible that certain predictors of stent malapposition exert differential effects across patient subgroups, which warrants further investigation in larger, prospective cohorts. Future studies should also explore the potential interaction between stent platforms, calcium modification techniques, and antithrombotic strategies to optimize procedural and long-term outcomes. In addition, although our median follow-up duration of 18.6 months is adequate for midterm outcome assessment, the long-term clinical implications of stent malapposition remain uncertain. Ongoing follow-up and future studies with extended observation periods are warranted to validate these findings. Moreover, the use of relative expansion metrics such as %MSA was not feasible in this study due to inconsistencies in reference segment measurements; future studies should incorporate such parameters to enhance individualized lesion assessment and outcome prediction.
In this retrospective observational study using OCT assessment, we identified
specific calcium characteristics, particularly calcium arc
SM, Stent malapposition; PCI, percutaneous coronary intervention; OCT, optical coherence tomography; CAC, Coronary artery calcification; IVL, intravascular lithotripsy; DES, drug-eluting stent; DCB, drug-coated balloons; TCFA, thin-cap fibroatheroma; MSA, minimum stent area; RA, rotational atherectomy; ROC, receiver operating characteristic; AUC, area under the curve.
All data relevant to the study are included in the article or uploaded. The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Conceptualization: SBJ, GZC; Methodology: GZC, RY, LBY; Formal analysis and investigation: QNZ, BZZ; Data curation: MC; Writing-original draft preparation: QNZ, LBY; Writing-review and editing: QNZ, GZC, SBJ; Supervision: SBJ. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. All authors contributed to editorial changes in the manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Approval from the Medical Research Ethics Review Committee of the General Hospital of Ningxia Medical University (KYLL-2025-1256). Participants have signed the informed consent form. All procedures complied with institutional guidelines and the principles of the Declaration of Helsinki.
Not applicable.
The 2022 National Natural Science Foundation of China (82260086); The 2022 Special Fund for Central Government Guiding Local Science and Technology Development (2022FRD05046); Open competition mechanism to select the best candidates for key research projects of Ningxia Medical University (XJKF230205); The Ningxia Natural Science Foundation (2022AAC03478); National Key R&D Program of China (2018YFC1311505).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.