


 , Kyusup Lee 2, Ki-Dong Yoo 1, Keon-Woong Moon 1, Donggyu Moon 1, Su Nam Lee 1, Won Young Jang 1, Ik Jun Choi 3, Jae-Hwan Lee 4, Jang Hoon Lee 5, Sang Rok Lee 6, Seung-Whan Lee 7, Kyeong Ho Yun 8, Hyun-Jong Lee 9
, Kyusup Lee 2, Ki-Dong Yoo 1, Keon-Woong Moon 1, Donggyu Moon 1, Su Nam Lee 1, Won Young Jang 1, Ik Jun Choi 3, Jae-Hwan Lee 4, Jang Hoon Lee 5, Sang Rok Lee 6, Seung-Whan Lee 7, Kyeong Ho Yun 8, Hyun-Jong Lee 91 Department of Cardiology, St. Vincent’s Hospital, College of Medicine, The Catholic University of Korea, 16247 Seoul, Republic of Korea
2 Department of Cardiology, Daejeon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 34943 Seoul, Republic of Korea
3 Department of Cardiology, Incheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 21431 Incheon, Republic of Korea
4 Department of Cardiology in Internal Medicine, Chungnam National University School of Medicine, Chungnam National University Sejong Hospital, 30099 Sejong, Republic of Korea
5 Department of Internal Medicine, Kyungpook National University Hospital, School of Medicine, Kyungpook National University, 41944 Daegu, Republic of Korea
6 Department of Cardiology, Chonbuk National University Hospital, 54907 Jeonju, Republic of Korea
7 Department of Cardiology, Asan Medical Center, University of Ulsan College of Medicine, 05505 Seoul, Republic of Korea
8 Department of Cardiovascular Medicine, Regional Cardiocerebrovascular Center, Wonkwang University Hospital, 54538 Iksan, Republic of Korea
9 Department of Internal Medicine, Sejong General Hospital, 14754 Bucheon, Republic of Korea
Abstract
Background: Periprocedural myocardial infarction (PMI) occurs more
frequently in patients with heavily calcified lesion and undergoing rotational
atherectomy (RA). However, there are limited studies addressing prognostic impact
of PMI in patients requiring RA due to severe coronary artery calcification
(CAC). Therefore, the objective of this study was to determine the prognostic
impact of PMI in patients who underwent percutaneous coronary intervention (PCI)
using RA. Methods: A total of 540 patients (583 lesions) who received
PCI using RA were enrolled between January 2010 and October 2019. PMI was defined
as elevations of creatine kinase-myocardial band (CK-MB)
Keywords
- periprocedural myocardial infarction
- coronary artery calcification
- rotational atherectomy
- clinical outcome
Technological advances in coronary intervention over the past four decades have made safer percutaneous coronary intervention (PCI) possible, with both clinical outcomes and procedural complications showing significant improvement. Although the incidence of periprocedural myocardial infarction (PMI) widely varies according to the definition, biomarker, biomarker threshold, and clinical presentation, it still remains one of the most common complication [1, 2].
PMI, referred to as myocardial injury that occurs during revascularization procedures [3], occurs more frequently in patients with heavily calcified lesion [4] and those who undergo rotational atherectomy (RA) for modifying that lesion [5, 6, 7]. Therefore, PMI is an important issue in patients requiring RA due to severe coronary artery calcification (CAC).
Although several previous studies have investigated the prognostic impact of PMI in patients undergoing PCI, results are still under debate [1, 6, 8, 9, 10, 11, 12, 13]. As mentioned above, although PMI is a major problem in patients requiring RA due to severe CAC, few studies have reported the prognostic impact of PMI in those patients. Therefore, the objective of the present study was to determine the prognostic impact of PMI on clinical outcomes of patients who underwent PCI using RA.
The study population consisted of 540 patients (583 lesions) with severely calcified coronary artery disease (CAD) who underwent PCI using RA from January 2010 to October 2019 at nine tertiary centers in Korea. Patients were included within the ‘ROtational atherectomy in Calcified lesions in Korea (ROCK)’ registry. This registry was approved by the Institutional Review Board (IRB) of each hospital. Data were collected at each center using a standardized case report form to record clinical and demographic characteristics, procedure related data, and follow-up data. Follow-up data were obtained up to 12 months retrospectively based on patients’ medical records and/or telephone interviews conducted by research nurses.
Patients were divided into two subgroups based on the presence or absence of PMI. The flow chart is displayed in Fig. 1. Baseline characteristics and clinical outcomes were compared between the two groups.
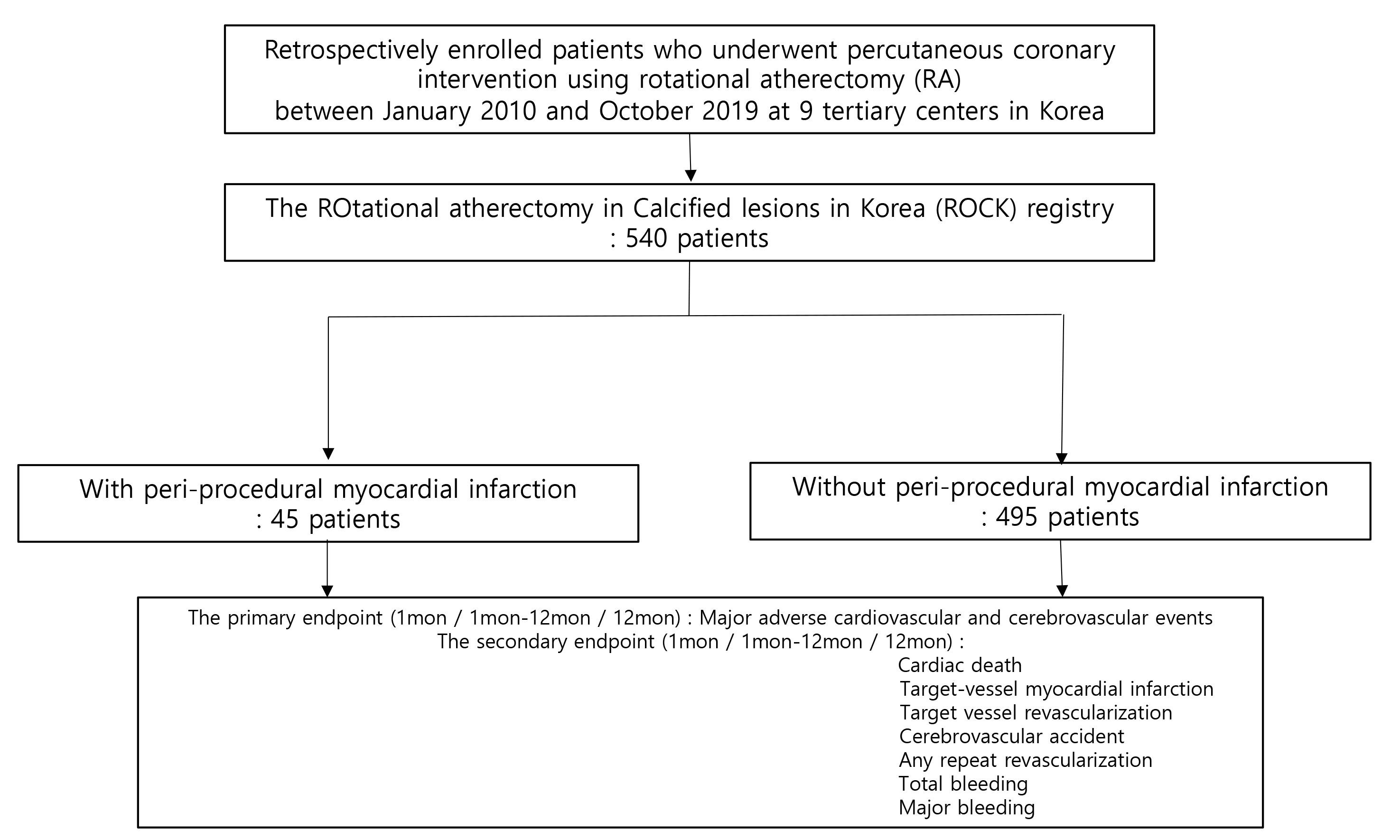 Fig. 1.
Fig. 1.Study population flow chart.
All RA procedures were performed using a Rotablator
PMI was defined with reference to Society for Cardiovascular Angiography and
Interventions (SCAI) definition [15]. In patients with normal baseline creatine
kinase-myocardial band (CK-MB), PMI was defined as peak elevation of CK-MB
Continuous variables are presented as median and interquartile range or mean
Patients were divided into a PMI group and a non-PMI group according to the
occurrence of PMI. Among a total of 540 patients, 45 patients were classified
into the PMI group and the remaining 495 patients were classified into the
non-PMI group. Baseline characteristics of patients with and without PMI are
presented in Table 1 and Table 2, respectively. Procedural details are also
presented in Table 2. There was no significant difference in baseline
characteristics between the two groups except for BMI, clinical diagnosis, and
LVEF. Especially, left main (LM) disease, mean stent diameter, total number of
stents, and stent length did not show any significant difference between non-PMI
and PMI groups in this study (LM disease, 68 [13.7%] vs. 6 [13.3%], p
= 0.940; mean stent diameter, 3.0
| Non-PMI (n = 495) | PMI (n = 45) | p-value | ||
|---|---|---|---|---|
| Age, years | 71.2 |
73.6 |
0.129 | |
| Sex | 0.979 | |||
| Male | 296 (59.8) | 27 (60.0) | ||
| Female | 199 (40.2) | 18 (40.0) | ||
| Smoking | 93 (18.8) | 10 (22.2) | 0.575 | |
| BMI | 24.3 |
22.8 |
0.009 | |
| HTN | 380 (76.8) | 35 (77.8) | 0.878 | |
| Hyperlipidemia | 215 (43.4) | 20 (44.4) | 0.896 | |
| DM | 285 (57.6) | 20 (44.4) | 0.089 | |
| CKD | 88 (17.8) | 8 (17.8) | ||
| Dialysis | 46 (9.3) | 3 (6.7) | 0.787 | |
| Previous PCI | 129 (26.1) | 10 (22.2) | 0.573 | |
| Previous CABG | 22 (4.4) | 2 (4.4) | ||
| Previous MI | 63 (12.7) | 3 (6.7) | 0.235 | |
| CVA | 66 (13.3) | 9 (20.0) | 0.216 | |
| PVD | 37 (7.5) | 2 (4.4) | 0.761 | |
| Chronic lung disease | 33 (6.7) | 4 (8.9) | 0.536 | |
| Heart failure | 67 (13.5) | 10 (22.2) | 0.111 | |
| Atrial fibrillation | 43 (8.7) | 6 (13.3) | 0.281 | |
| Clinical diagnosis | 0.002 | |||
| Stable angina | 204 (41.2) | 8 (17.8) | ||
| ACS | 291 (58.8) | 37 (82.2) | ||
| HbA1C | 6.7 |
6.2 |
0.084 | |
| Total cholesterol | 143.2 |
148.3 |
0.419 | |
| LDL cholesterol | 84.6 |
86.4 |
0.798 | |
| HDL cholesterol | 46.0 |
46.7 |
0.791 | |
| Triglyceride | 121.2 |
100.1 |
0.110 | |
Data are shown as mean
PMI, periprocedural myocardial infarction; BMI, body mass index; HTN, hypertension; CKD, chronic kidney disease; DM, diabetes mellitus; PCI, percutaneous coronary intervention; CABG, coronary artery bypass graft; MI, myocardial infarction; CVA, cerebrovascular accident; PVD, peripheral vascular disease; ACS, acute coronary syndrome; HbA1c, glycated hemoglobin; LDL, low density lipoprotein cholesterol; HDL, high density lipoprotein cholesterol.
| Non-PMI (n = 495) | PMI (n = 45) | p-value | ||
|---|---|---|---|---|
| ACC/AHA classification | 0.670 | |||
| A | 3 (0.6) | 0 (0.0) | ||
| B1 | 38 (7.3) | 2 (4.4) | ||
| B2 | 49 (9.9) | 3 (6.7) | ||
| C | 405 (81.8) | 40 (88.9) | ||
| Left main disease | 68 (13.7) | 6 (13.3) | 0.940 | |
| MVD | 385 (77.8) | 39 (86.7) | 0.195 | |
| IVUS | 231 (46.7) | 18 (40.0) | 0.390 | |
| Arc of calficication |
91/150 (60.7) | 10/18 (55.6) | 0.676 | |
| LVEF, % | 53.5 |
47.5 |
0.004 | |
| Mean stent diameter, mm | 3.0 |
3.0 |
0.895 | |
| Total number of stent | 2.3 |
2.5 |
0.370 | |
| Total stent length, mm | 66.6 |
66.7 |
0.990 | |
| Procedure time, min | 79.0 |
81.8 |
0.728 | |
Data are shown as mean
PMI, periprocedural myocardial infarction; ACC/AHA, American College of Cardiology/American Heart Association; MVD, multivessel disease; IVUS, intravascular ultrasound; LVEF, left ventricle ejection fraction.
Compared with the non-PMI group, the PMI group showed more frequent in-hospital events (6 [13.3%] vs. 15 [3.0%], p = 0.005), coronary dissection (8 [17.8%] vs. 38 [7.7%], p = 0.043), and coronary perforation (3 [6.7%] vs. 7 [1.4%], p = 0.043) (Table 3). Coronary dissection and coronary perforation are among mechanisms of PMI.
| Non-PMI (n = 495) | PMI (n = 45) | p-value | ||
|---|---|---|---|---|
| In-hospital events | 15 (3.0) | 6 (13.3) | 0.005 | |
| In-hospital death | 8 (1.6) | 3 (6.7) | 0.056 | |
| Urgent CABG | 2 (0.4) | 0 (0.0) | ||
| Urgent PCI | 5 (1.0) | 2 (4.4) | 0.109 | |
| In-hospital CVA | 1 (0.2) | 1 (2.2) | 0.160 | |
| Procedural outcomes | ||||
| Coronary dissection* | 38 (7.7) | 8 (17.8) | 0.043 | |
| Temporary pacemaker during procedure | 15 (3.0) | 1 (2.2) | ||
| Coronary perforation | 7 (1.4) | 3 (6.7) | 0.043 | |
| In-hospital bleeding | 22 (4.4) | 5 (11.1) | 0.064 | |
| Procedure success | 483 (97.6) | 37 (82.2) | ||
Data are shown as mean
*Coronary dissection from defined from The National Heart, Lung, and Blood Institute (NHLBI) classification system.
PMI, periprocedural myocardial infarction; CABG, coronary artery bypass grafting; PCI, percutaneous coronary intervention; CVA, cerebrovascular accident.
The incidence of MACCE, the primary endpoint, showed no significant difference between the two groups at 1 month, 1–12 months, or 12 months. There was no significant difference in secondary endpoints such as cardiac death, target-vessel MI, TVR, or CVA. Only total bleeding at 1 month showed a tendency to occur more frequently in the PMI group (Fig. 2) (Table 4).
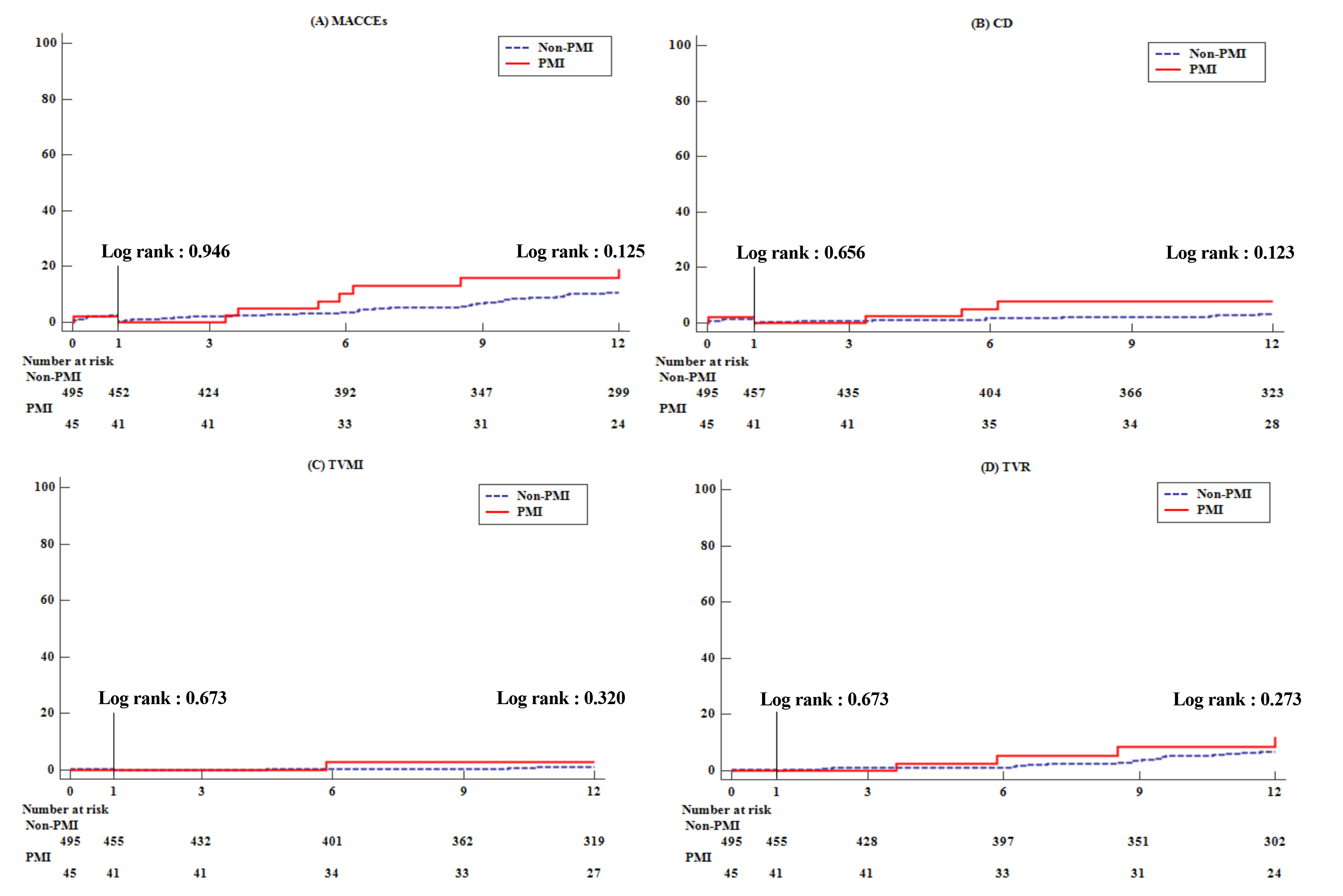 Fig. 2.
Fig. 2.Kaplan-meier curve for clinical outcomes during follow-up. (A) Major cardiovascular and cerebrovascular events. (B) Cardiac death. (C) Target vessel myocardial infarction. (D) Target vessel revascularization.
| Non-PMI (n = 495) | PMI (n = 45) | p-value | Univariate HR (95% CI) | p-value | Multivariate HR** (95% CI) | p-value | ||
|---|---|---|---|---|---|---|---|---|
| Endpoints at 1 month | ||||||||
| MACCEs | 10 (2.0) | 1 (2.2) | 0.933 (0.121–7.172) | 0.947 | 0.298 (0.029–3.015) | 0.305 | ||
| Cardiac death | 7 (1.4) | 1 (2.2) | 0.504 | 1.602 (0.197–13.023) | 0.659 | 0.794 (0.062–10.148) | 0.859 | |
| Target-vessel MI | 2 (0.4) | 0 (0.0) | - | - | - | - | ||
| TVR | 2 (0.4) | 0 (0.0) | - | - | - | - | ||
| CVA | 2 (0.4) | 0 (0.0) | - | - | - | - | ||
| Any repeat revascularization | 2 (0.4) | 0 (0.0) | - | - | - | - | ||
| Total bleeding | 3 (0.6) | 4 (8.9) | 0.001 | 15.037 (3.365–67.193) | 0.000 | 8.464 (1.350–53.043) | 0.023 | |
| Major bleeding | 1 (0.2) | 1 (2.2) | 0.160 | 11.121 (0.696–177.807) | 0.089 | 41.075 (0.042–40365) | 0.291 | |
| Endpoints at 1 month–12 month | ||||||||
| MACCEs | 39 (7.9) | 7 (15.6) | 0.091 | 1.852 (0.833–4.117) | 0.131 | 1.714 (0.727–4.039) | 0.218 | |
| Cardiac death | 13 (2.6) | 3 (6.7) | 0.141 | 2.591 (0.738–9.092) | 0.137 | 1.349 (0.345–5.272) | 0.667 | |
| Target-vessel MI | 4 (0.8) | 1 (2.2) | 0.354 | 2.890 (0.323–25.864) | 0.343 | 1.441 (0.138–15.080) | 0.760 | |
| TVR | 26 (5.3) | 4 (8.9) | 0.302 | 1.787 (0.624–5.121) | 0.280 | 1.785 (0.568–5.612) | 0.322 | |
| CVA | 7 (1.4) | 0 (0.0) | - | - | - | - | ||
| Any repeat revascularization | 30 (6.1) | 4 (8.9) | 0.514 | 1.532 (0.540–4.349) | 0.423 | 1.302 (0.417–4.067) | 0.650 | |
| Total bleeding | 17 (3.4) | 1 (2.2) | 0.679 (0.090–5.103) | 0.707 | 0.491 (0.047–5.186) | 0.554 | ||
| Major bleeding | 5 (1.0) | 1 (2.2) | 0.408 | 2.294 (0.268–19.659) | 0.448 | 23.083(0.928–574.0) | 0.056 | |
| Endpoints at 12 month | ||||||||
| MACCEs | 49 (9.9) | 8 (17.8) | 0.123 | 1.680 (0.800–3.531) | 0.171 | 1.314 (0.592–2.913) | 0.502 | |
| Cardiac death | 20 (4.0) | 4 (8.9) | 0.130 | 2.245 (0.767–6.568) | 0.140 | 1.277 (0.398–4.099) | 0.681 | |
| Target-vessel MI | 6 (1.2) | 1 (2.2) | 0.458 | 1.911 (0.230–15.875) | 0.549 | 1.078 (0.115–10.109) | 0.947 | |
| TVR | 28 (5.7) | 4 (8.9) | 0.329 | 1.656 (0.581–4.721) | 0.345 | 1.465 (0.471–4.558) | 0.510 | |
| CVA | 9 (1.8) | 0 (0.0) | - | - | - | - | ||
| Any repeat revascularization | 32 (6.5) | 4 (8.9) | 0.528 | 1.435 (0.507–4.057) | 0.496 | 1.103 (0.357–3.405) | 0.865 | |
| Total bleeding | 20 (4.0) | 5 (11.1) | 0.048 | 2.867 (1.076–7.640) | 0.035 | 2.681 (0.869–8.276) | 0.086 | |
| Major bleeding | 6 (1.2) | 2 (4.4) | 0.138 | 3.797 (0.766–18.814) | 0.102 | 18.956(1.542–233.1) | 0.022 | |
** adjusted by age, sex, BMI, clinical diagnosis, coronary perforation, coronary dissection, LVEF, procedural success.
Data are shown as mean
HR, hazard ratio; CI, confidence interval; PMI, periprocedural myocardial infarction; MACCEs, major adverse cardiovascular and cerebrovascular events; MI, myocardial infarction; TVR, target vessel revascularization; CVA, cerebrovascular accident.
Main findings of this study were as follows: (1) stent diameter, number, length,
and LM disease in patients who underwent RA showed no significant difference
regardless of PMI. (2) PMI was associated with the occurrence of more in-hospital
events. (3) There was no significant difference in MACCE during 1 year follow-up
between non-PMI and PMI groups though events trended higher in the PMI group. As
patients aged and complex PCI increased, patients with severe coronary
calcification also increased. Accordingly, procedures requiring RA was
increasing. In the present study, there were many patients in both groups with
arc of calficication
The reason why PMI was a major problem in patients undergoing PCI using RA was related to its mechanism. Mechanisms of PMI include side branch occlusion (SBO), distal embolization, coronary dissection, and coronary perforation [20]. During RA, an additional protection wire for preventing SBO cannot be used. Disrupted calcified plaque can release micro-debris that can induce microembolization and slow/no reflow, thus increasing the risk of coronary dissection and perforation. All these factors can lead to SBO or distal embolization, resulting in PMI during RA [2, 20]. Therefore, it is important to determine whether PMI affects clinical outcome because interventional cardiologists would hesitate to select RA for heavily calcified lesions if PMI affects clinical outcome considerably.
In previous studies, the prognostic impact of PMI was variable depending on
biomarkers and biomarker thresholds applied to the definition of PMI [1, 8, 10, 11, 21]. In our study, CK-MB instead of cardiac troponin (cTn) was used as a
biomarker. Its threshold was
Our study had several limitations. First, this was a non-randomized,
observational, and retrospective study with a possibility of selection bias.
Second, when defining PMI, clinical sign and ECG corresponding to ancillary
criteria were not considered. We only considered biomarker elevation. Howerever,
when ancillary criteria are applied, the CK-MB threshold is lowered to
This study shows that PMI after RA in patients with severe CAC was associated with more frequent in-hospital events and a nonsignificant trend for more events during 1 year follow-up. These findings require confirmation in larger studies with longer follow-up.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Conceptualization—JJ, SHH; Methodology—SHH; Validation—JJ, SHH and KL; Formal analysis—SHH; Investigation—JJ; Resources—KDY, KWM and DM; Data curation—SHH, KL, SNL, WYJ, IJC, JHL (Jae-Hwan Lee), JHL (Jang-Hoon Lee), SWL, KHY, SRL and HJL; Writing-original draft preparation—JJ; Writing—review and editing—SHH; Supervision—SHH. All authors have read and agreed to the published version of the manuscript.
This study was approved by the regional ethics committee for each participating hospital, and all patients provided their written informed consent to the use of medical data for the registry study (Ethic Committee Name: Institutional Review Board (IRB) of Daejeon St. Mary’s Hospital, Approval Code: DC19REDI0066, Approval Date: 30 July 2019).
Thanks to everyone who helped us during the writing of this manuscript and all peer reviewers for their comments and suggestions.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.